
Abstract
Purpose
Worldwide, spinal cord injuries are associated with diminished participation in the labor market. Inconclusive reporting and differences between workplace settings for individuals with spinal cord injury (SCI) make conceptualizing return to work rates among this population inherently challenging. The objectives of this study are to explore factors associated with return to work (RTW) following an SCI. Moreover, the factors were classified according to the work disability prevention framework. Finally, we conducted a meta-analysis of the prevalence of RTW following an SCI.
Methods
Original articles were identified through a literature search in four health databases. The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines for the mapping and identification of records. Included studies contained primary studies that included the nature of the injury, antecedent factors associated with the injury, and study characteristics and RTW outcomes. Exclusion criteria for the studies included if there was no discussion of RTW outcomes, systematic reviews, and meta-analyses.
Results
A total of 461 full-text articles were assessed for eligibility, and eight studies were included and assessed using the Critical Appraisal Skills Programme checklist, Risk of Bias, and Newcastle–Ottawa Scale. Four studies identified personal system factors, four identified healthcare system factors, two identified compensation system factors, and one identified workplace system factors.
Conclusions
Attempts to optimize RTW among persons with SCI are inherently difficult due to the diversity of this client population. Findings from the studies included in this systematic review support the utility of interventions for facilitating RTW, such as vocational rehabilitation and workplace accommodations, while simultaneously acknowledging the limitations in identifying specific interventions as facilitatory or inhibitory throughout the process.
Introduction
Globally, between 250,000 and 500,000 individuals suffer a spinal cord injury (SCI) each year. 1 Inconclusive reporting and differences between workplace settings for individuals with SCI make conceptualizing return to work rates among this population inherently challenging. In spite of these challenges, it has been reported that only 12% of SCI patients return to their pre-injury professions, with an average rate of employment of 35%. 2 Those who returned to work after an SCI experienced a variety of beneficial outcomes including mental stimulation, social contact, a sense of purpose, and personal growth via a “spread effect.” 2 Return to work (RTW), as measured by the obtainment of competitive employment, is often used to understand one’s quality of life after SCI.3,4
Work is central in peoples’ lives as it positively impacts their physical, mental, and social well-being.5–8 Employment also facilitates financial independence and is considered a source of personal growth, 9 life satisfaction, and social integration and is linked to improved health.10,11
Barriers and challenges to RTW and sustaining employment are exacerbated with diminished availability of supports. 12 Several systematic reviews have indicated that RTW after SCI involves the complex interplay of the person, environment, and injury-related factors.4,13–16 A limited number of studies measure quality of life outcomes or the utility of vocational rehabilitation (VR) services for RTW among post-SCI populations. Given that the post-SCI population is highly diverse, it is difficult to conclude how financial, cultural, and other demographic factors impact access to, and success with, VR services post-SCI. Nevertheless, some studies used in this meta-analysis provide insight into this ongoing research endeavor.
Certain studies define the success of VR services by the attainment of employment, while others use hours of employment post-SCI as criteria for determination. Individuals receive extensive VR with the goal of maximizing functioning and RTW. 16 Employment is regarded as a key indicator of social well-being of the population. 17 However, data suggest that rates of employment among people with SCI is approximately 35–37%,18–20 with higher rates in Europe (51%) compared to North America (30%).19,21
Preventing work disability supports RTW and promotes functional independence. 22 The work-disability prevention (WDP) framework is anchored by the worker. The central location of the worker emphasizes the importance of his/her place within the WDP paradigm. The conceptual model emphasizes the different facets, and their various levels, from the person (physical and psychosocial), the workplace, the compensation system, and healthcare system that may influence WDP. 22 Additionally, the model demonstrates the challenges and opportunities of the return to work process in the workplace, from the worker’s job position to the whole workplace organization and even possibly to the external environment in which the firm functions. 22
The objectives of this study were to explore factors associated with RTW following SCI. Moreover, the factors were classified according to the work disability prevention framework. Furthermore, we conducted a meta-analysis of the prevalence of RTW following an SCI.
Methods
Inclusion and exclusion criteria for studies following the PICO framework.
Note: SCI: spinal cord injury; PICO: population, intervention, comparison, and outcome; RTW: return to work; SCI: spinal cord injury.
Search strategy and study selection
The search criteria were finalized with assistance from a health research librarian, and all articles included in the study were published in English. Our process complied with each database’s requirements used (full search strategy available as online Supplementary Material). The selection of articles was retrieved on April 10, 2020, and updated March 29, 2021. The studies chosen for this review contained information regarding SCI, the antecedent factors that led to the injury, and RTW outcomes. The inclusion and exclusion criteria are listed in Table 1.
Two reviewers took part by independently examining, collecting, and reporting the data of each article. All the included studies were stored in Rayyan, 24 a free web application that permitted the screening of abstracts and titles. The research team reviewed the disagreements and consensus achieved.
Critical appraisal of included studies
The Critical Appraisal Skills Programme (CASP) cohort review checklist was used by two reviewers to assess all the included studies 25 to evaluate their relevance, validity, and quality against 10 questions (Online Supplementary Material) to generate an overall score for each study. Risk of bias for observational studies was examined using the Newcastle–Ottawa Scale (NOS), 26 which appraised studies across three domains (selection, comparability, and outcome), and for randomized control trials, the “risk of bias” assessment tool was used across six domains (selection bias, performance bias, detection bias, attrition bias, reporting bias, and other bias). 27 An overall summary of the risk of bias was calculated for RCT studies. A study was deemed low risk if attrition bias due to missing data was unlikely to be related to RTW and SCI (e.g., for survival analysis data, censoring was unlikely to introduce bias). A study was designated unclear if there was insufficient information to determine its risk of bias.
Statistical analyses
A meta-analysis of proportions was computed using the data from the selected articles and employed a random-effects model to test the prevalence proportion of return to work following an SCI. The I2 statistic was also computed as an evaluation of the proportion of the overall variation in the proportion that was attributable to between-study heterogeneity. All analyses were conducted in R 4.02, and “metafor” (version 2.4–0) package was used for the meta-analysis of proportions.28–30 The underlying assumption of the meta-analytic procedures assumed the findings were independent. We used a random-effects model including considerations of heterogeneity in the effect estimate. 31
Classification of RTW predictors
This systematic review used the work disability framework (WDF) presented by Loisel et al. to categorize RTW predictors following an SCI. This framework recognizes that RTW and independent living is contingent on meeting workers’ needs across the personal, health care, compensation, and workplace systems. 32
Data collection
Data regarding the nature of the injury, antecedent factors associated with the injury, and study characteristics (e.g., sample size, study design, and type of injury) were collected.
Results
The study identified a total of 146,523 articles across seven databases (Figure 1) from which eight articles were suitable for full text review that explored RTW predictors among individuals post-SCI12,18,33–38; the mean CASP score was 9/10 (standard deviation of 0.57). Five studies were from the United States, two from the Netherlands, and one from Taiwan; there was one prospective RCT that used the obtainment of competitive employment (CE) as the primary outcome measure
37
and the rest were observational studies. PRISMA flow diagram of the inclusion process. *References included per database before removing duplicates: Medline (33,984), Embase (52,662), PsycINFO (4607), CINAHL (45,738), Cochrane (1437), AMED (5994), and ASSIA (2101). **Studies excluded with reason include those that met the exclusion criteria listed in Table 1.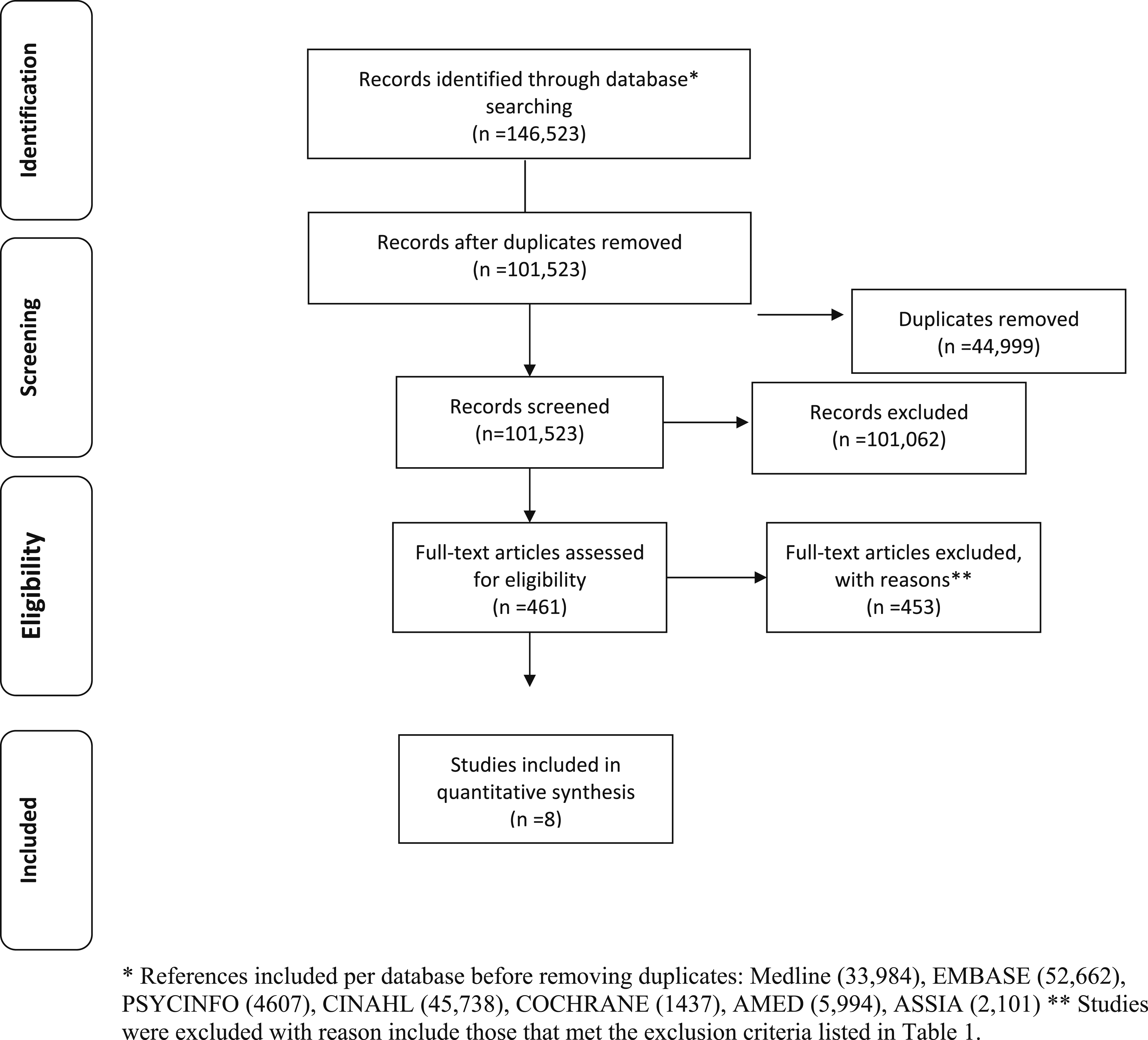
Characteristics and antecedent factors of individuals with spinal cord injuries returning to work.
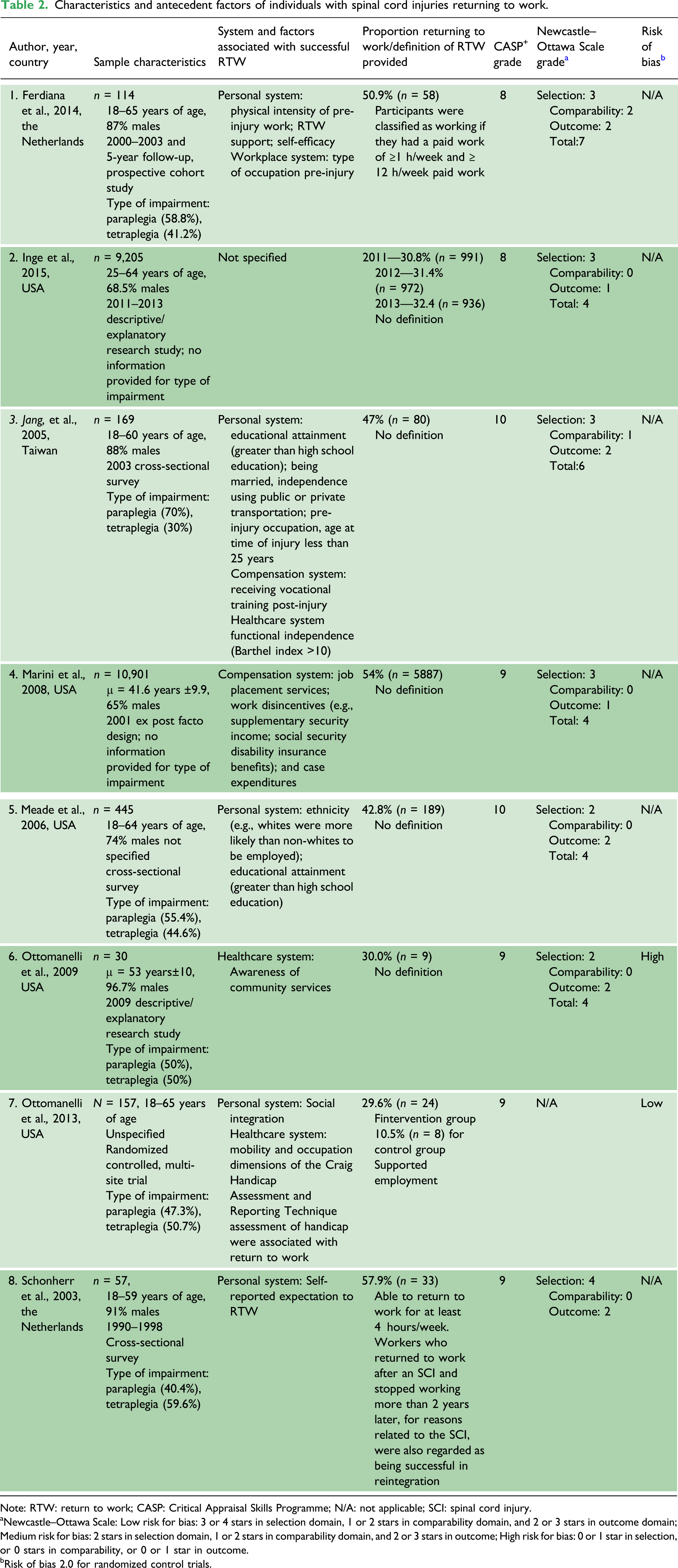
Note: RTW: return to work; CASP: Critical Appraisal Skills Programme; N/A: not applicable; SCI: spinal cord injury.
aNewcastle–Ottawa Scale: Low risk for bias: 3 or 4 stars in selection domain, 1 or 2 stars in comparability domain, and 2 or 3 stars in outcome domain; Medium risk for bias: 2 stars in selection domain, 1 or 2 stars in comparability domain, and 2 or 3 stars in outcome; High risk for bias: 0 or 1 star in selection, or 0 stars in comparability, or 0 or 1 star in outcome.
bRisk of bias 2.0 for randomized control trials.
Summary of factors associated with successful RTW with individuals with a spinal cord injury.
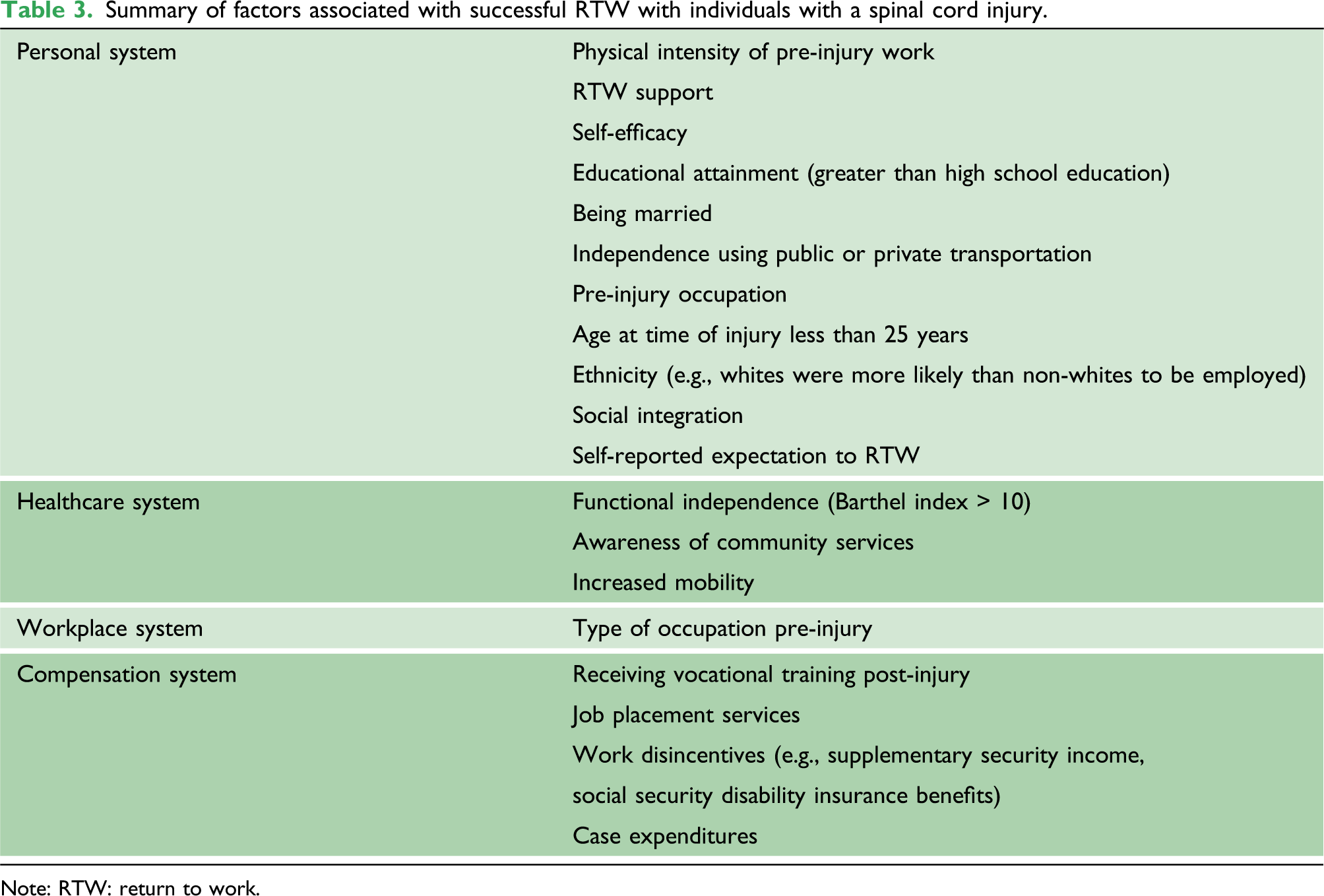
Note: RTW: return to work.
A meta-analysis of the prevalence of RTW following an SCI was performed (Figure 2). The overall prevalence of RTW following an SCI from the results reported in eight of the studies was 45.8% (95% CI, 0.35–0.57) (I2 = 99%, p < 0.01). A random-effect model was employed for all the factors.
40
Prevalence of return to work following a spinal cord injury.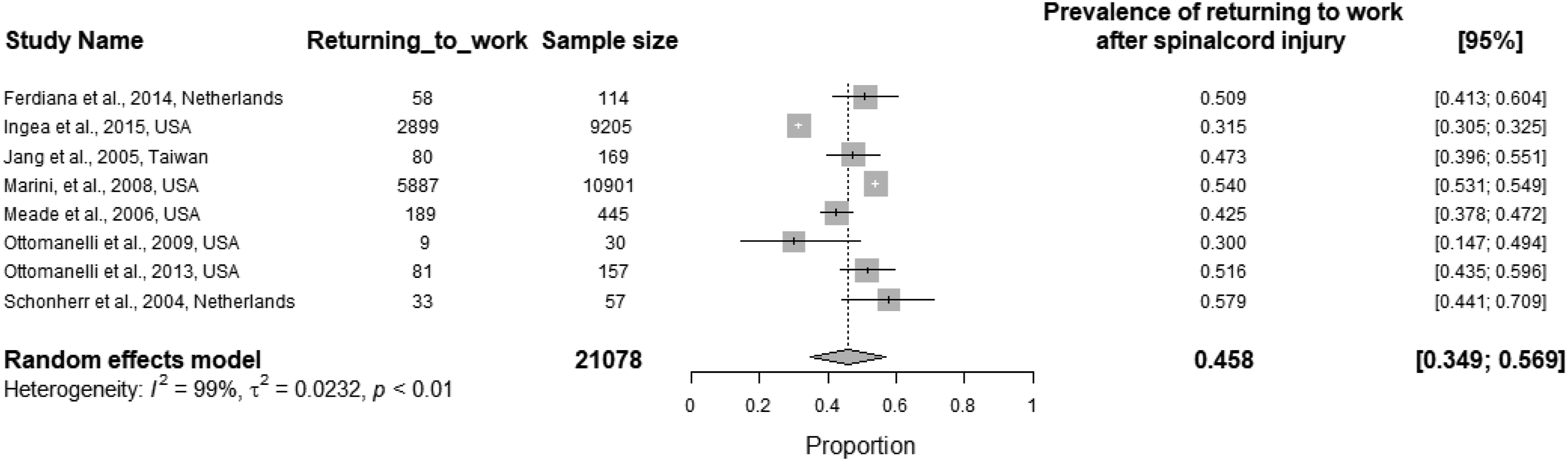
Discussion
The objective of this study was to determine factors associated with RTW following an SCI. Moreover, the factors were classified according to the work disability prevention framework. Rehabilitative efforts for persons with SCI strive to maximize independence and quality of life, with RTW frequently used as an indicator of rehabilitative success.3,4 Understanding factors that influence RTW among persons with SCI is a valued research endeavor as RTW percentages remain low for this population despite efforts to re-integrate these patients into gainful employment.2,4,20 This systematic review and meta-analysis synthesized findings from studies that explored factors, including demographics and features of rehabilitative programs, that may influence the RTW process among patients with an SCI.
Personal system
The finding that CE post-SCI did not elicit significant increases in health-related quality of life among veterans demonstrates the limitations of using CE to account for subjective experiences. Obtaining CE does not capture the sustainability of the work, a patient’s enjoyment, or if financial stability is provided by the job—factors that are likely to influence viewpoints regarding employment post-SCI and its impact on quality of life outcomes. 37 Several studies included in this systematic review examined the effect that demographic factors, financial assistance, and support services have on gaining CE for patients post-SCI.12,36 While the paucity of high-quality studies regarding RTW outcomes among persons with SCI is discouraging, the review of these articles did support findings in other literature.4,18 Studies produced evidence in support of educational attainment and age at onset of injury as primary indicators of RTW outcomes and are consistent with existing literature.14,41,42 For example, persons with SCI who gained employment post-injury were consistently found to have attained higher levels of education (e.g., undergraduate and masters) and a mean age of 33 years.12,38 These demographic variables bring attention to the importance of modifiable and non-modifiable factors when anticipating RTW outcomes. 14 For instance, though patients post-SCI were more likely to obtain CE when they had higher educational attainment and were younger at the time of injury, these may be worthwhile upstream targets of change to enhance CE among the SCI population. 3
Health care
The systematic review identified RTW outcomes such as education level, cultural background, supplementary income, and specific VR interventions.12,36 VR services provided to Hispanic Americans focused primarily on eliminating environmental barriers impeding RTW outcomes post-SCI, such as lack of access to transportation. 41 Comparatively, European Americans accessed job placement and on-the-job-training more frequently when using VR services. 41 These studies highlighted the benefit of specific VR services, such as job placement and assistive technology, on RTW outcomes, but were unable to articulate these services’ features that could explain the findings (i.e., types of assistive technology used and frequency of job support provided).
Compensation system
For clinicians, this review examined factors associated with RTW following a SCI and demonstrates the need to work closely with stakeholders in the compensation system. Such a collaboration ensures individuals with an SCI receive vocational training post-injury, 35 job placement services, social security income, disability benefits, and case expenditures. 36 There is a dearth of evidence regarding the inclusion and role of the compensation system in supporting RTW among individuals with SCI. 43 The limited available evidence suggests that they may play a supportive role in promoting functioning. 43
Workplace system
The intrinsic differences that exist among persons with SCI and the quality of service delivery of various VR programs are essential to note. It is unrealistic to expect VR interventions to be delivered the same person to person or country to country. Conversely, individualizing VR services to facilitate successful RTW outcomes is necessary to understand which interventions provide optimal support for a highly diverse SCI population. As VR offers a breadth of different services to facilitate the RTW process, the combinations or intensities of specific interventions seem to serve as more robust predictors of CE obtainment than simply considering whether VR services were accessed or not by persons with SCI.12,36,44
Limitations
The search criteria used for this systematic review only included literature published in English, which may have limited the discovery of potential predictors of RTW outcomes among persons post-SCI. Most of the included studies implemented retrospective analyses and cross-sectional experimental designs, which do not allow for causative factors of successful or unsuccessful RTW outcomes to be concluded with certainty. Moreover, the studies were predominantly from North America and Europe and limited the external validity of the findings. RTW outcomes may be more or less responsive to VR services, demographic factors, or supplementary income from a cultural standpoint, but these findings could not be captured based on the literature search used. Operationalizations of RTW also varied amongst studies. Some studies deemed RTW successful when CE was obtained post-SCI, even if employment was not retained due to SCI-related barriers. Alternatively, others defined RTW based on the number of hours of employment per week. The absence of an objective definition of what constitutes returning to work among persons after SCI makes concluding RTW outcomes as successful or unsuccessful inherently challenging. Objective efforts to define RTW also overshadow the subjective values placed on RTW outcomes. Specifically, for persons with SCI, successful RTW outcomes may be defined by job stability over time and personal satisfaction with their work instead of financial earnings, hours worked, or simply being employed.
A commonality of each study used in this systematic review was the propensity that sample populations contained more men than women. While the inclination for SCI to occur is higher among men than women, 18 our understanding of RTW post-SCI is narrowed as findings may be more reflective of the male experience. Conversely, potential predictors of RTW among persons with SCI may have been masked due to the disparity present between sexes in the sample populations used. Qualitative study designs related to RTW amongst individuals post-SCI are a valued undertaking as understanding the experience of RTW outcomes for women post-SCI remains largely unexplored.
Future research
Future research should strive to account for personal experiences of persons with SCI and the VR services that optimized their RTW outcomes. Subjective factors such as motivation and the belief that RTW is possible have been instrumental in facilitating successful RTW outcomes among persons with SCI. 20 The majority of research completed to date that explores predictors of RTW outcomes for patients post-SCI is quantitative and cross-sectional by design. While useful for aggregating objective data such as the relationship between VR service access and CE obtained among patients post-SCI, providing explanations for what worked and why it was effective is impossible without the voice of the primary consumer of the services.
Attempts to optimize RTW among persons with SCI are inherently challenging due to the diversity of this client population. Findings from the studies included in this systematic review support the utility of interventions for facilitating RTW, while simultaneously acknowledging the limitations in identifying specific interventions as facilitatory or inhibitory throughout the process. Assessing the role that VR services have in RTW outcomes requires a focused understanding of interventions that meet the specific needs of the patient as individualized services consistently demonstrated promising results despite small sample sizes. The endeavor to identify RTW predictors among persons with SCI continues to be a necessary first step toward enabling favorable employment outcomes, such as job security, maintenance, and financial stability post-SCI.
For researchers, this system review identifies factors associated with RTW that may serve as a starting point for future exploration. These systems provide opportunities for future intervention studies to explore the factors associated with RTW in greater depth. For instance, what types of occupations are more likely to be associated with timely RTW among individuals with SCI?
For rehabilitation clinicians and learners, the findings provide a holistic framework to situate RTW interventions with individuals with an SCI. Targeted interventions should consider the WDP framework and place the individual at the center of care and use a multidisciplinary care approach during VR and RTW journey.
Supplemental Material
sj-pdf-1-tra-10.1177_14604086211033083 – Supplemental Material for Prevalence and predictors of return to work following a spinal cord injury using a work disability prevention approach: A systematic review and meta-analysis
Supplemental Material, sj-pdf-1-tra-10.1177_14604086211033083 for Prevalence and predictors of return to work following a spinal cord injury using a work disability prevention approach: A systematic review and meta-analysis by Behdin Nowrouzi-Kia, Nirusa Nadesar, Yingji Sun, Markus Ott, Gobika Sithamparanathan and Priya Thakkar in Trauma
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
BN.
Provenance and peer review
Not commissioned, externally peer reviewed.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.