
Abstract
Background and Aims:
A high body mass index (BMI) has traditionally been a strict criterion for surgical eligibility for arthroplasty based on the increased risk for periprosthetic joint infection (PJI). Individuals with obesity are two to four times more likely to undergo joint arthroplasty. There are limited data on how well BMI predicts PJI risk and whether strict BMI-based surgical criteria are justified.
Methods:
This retrospective single-center cohort study included all primary total hip arthroplasties (THAs) and total knee arthroplasties (TKAs) performed at our institution between 1 January 2008 and 28 November 2023. Survival was analyzed using the Kaplan–Meier method, with PJI as the primary outcome. The association between BMI and PJI was assessed using logistic regression and Cox proportional hazards regression.
Results:
A total of 54,879 arthroplasties (23,544 hip and 31,335 knee arthroplasties) were included. The median age was 68 years (interquartile range (IQR): 60–75), and 60.0% of patients were female. The risk for PJI was highest in patients with a BMI >45. After THA, the lowest risk for PJI was seen with a BMI <25 (1.0%) and between 25 and 30 (1.1%) after TKA. After THA, a J-shaped association between BMI and PJI was observed in logistic regression analysis, as the risk for PJI increased in patients with both low and high BMIs. A J-shaped association between BMI and PJI was also observed in Cox regression analysis after both TKA and THA. Men had a higher risk for PJI after THA than women, whereas no sex variation was observed after TKA.
Conclusion:
The risk for PJI does not increase linearly with BMI and the risk differs between women and men. When BMI exceeds 45, risk levels become notably high. Otherwise, the absolute risk differences between different BMI categories are relatively low. Emphasis should be placed on individualized risk assessment and shared decision-making rather than focusing solely on BMI.
Context and relevance
Obesity and high body mass index (BMI) are recognized risk factors for periprosthetic joint infection (PJI), and BMI has therefore often been used as a strict eligibility criterion for arthroplasty. However, BMI alone may not accurately capture infection risk, as obesity is common among arthroplasty candidates. In this large single-center cohort of nearly 55,000 primary hip and knee arthroplasties, we found that the risk of PJI was J-shaped in relation to BMI and that differences between BMI categories were smaller than previously assumed, except for markedly elevated risk at BMI above 45. These findings highlight the limitations of BMI-based thresholds and emphasize the need for individualized risk assessment and shared decision-making.
Introduction
Periprosthetic joint infection (PJI) is one of the most serious complications after total hip arthroplasty (THA) and total knee arthroplasty (TKA). 1 Obesity, commonly indicated by a high body mass index (BMI), has been identified as an important predictor of PJI following primary THA and TKA.2–4
The effect of BMI on the risk for PJI in individuals with obesity appears to be associated with a higher number of comorbidities, more challenging surgeries, and suboptimal tissue oxygenation. 5 In addition, lower serum and tissue concentrations of prophylactic antimicrobial agents,6,7 as well as the potential release of immune-weakening mediators produced by adipose tissue, 8 may play a role in the increased risk for PJI.
BMI has traditionally been a strict criterion for surgical indication.9,10 However, the evidence supporting such strict criteria is not definitive, as opposing views have also been presented.11,12 This lack of definitive evidence highlights the need for validation in larger cohorts. Moreover, as the prevalence of obesity continues to rise, it is essential that further study is conducted on the predictive effect of BMI in relation to other associated factors.13,14
We aimed to answer the following research questions: (1) What is the incidence of PJI at 90 days and 2 years after THA and TKA across different BMI groups in a large, unselected cohort of patients, and (2) how well does baseline BMI predict infection risk in relation to other preoperative variables?
Materials and methods
Data sources
This retrospective cohort study included all primary THAs and TKAs performed at a high-volume academic referral center specializing in joint arthroplasty between 1 January 2008 and 28 November 2023. Our institution is a high-volume academic referral center specializing in joint arthroplasty surgery, performing over 3900 primary TKAs and more than 2600 primary THAs annually. For patients who underwent surgery on multiple joints, each joint was analyzed as a separate procedure. Patient selection, exclusions, and follow-up are illustrated in the study flow chart (Figure 1).

Flow chart illustrating patient selection, exclusions, and follow-up. Patients were followed from the date of primary surgery until revision for prosthetic joint infection, aseptic revision, death, or end of follow-up. Analyses were performed at 90 days, 1 year, and 2 years.
Patient data were retrieved from our prospectively collected hospital database where the detailed medical histories and treatment data of patients (e.g. details of surgery, prosthesis, laboratory results, medication, comorbidities) are documented. The following clinical data were collected from the database: indication for surgery, age, sex, BMI, American Society of Anesthesiologists (ASA) risk class, presence of kidney disease, presence of liver disease, and diabetic status. Height and weight used to calculate BMI are recorded as part of a standardized preoperative assessment.
Information on kidney and liver disease was based on clinician-assigned diagnoses recorded in the electronic patient record as part of routine clinical care. Kidney disease was defined as moderate to severe renal disease, where moderate disease was defined as serum creatinine greater than 3 mg/dL (0.27 mmol/L), and severe disease included patients on dialysis, those with a history of kidney transplantation, or uremia. Liver disease was categorized as mild, moderate, or severe. Mild liver disease referred to chronic hepatitis or cirrhosis without portal hypertension; moderate disease to cirrhosis with portal hypertension without a history of variceal bleeding; and severe disease to cirrhosis with portal hypertension and a history of variceal bleeding.
Follow-up period and outcomes
The outcome in our analyses was revision surgery due to PJI. PJI was defined as a clinically established diagnosis leading to surgical treatment for infection, based on up-to-date diagnostic criteria. All surgical procedures performed for PJI were included, including debridement, antibiotics, and implant retention (DAIR) as well as revision arthroplasty. Analyses were performed at three follow-up time points: 3 months, 1 year, and 2 years after primary surgery. The follow-up period began immediately after surgery and ended when one of the following occurred: the follow-up period expired, the patient underwent revision due to PJI, the patient underwent an aseptic revision, the patient was lost to our hospital’s regular follow-up program (e.g. due to death or relocation), or if none of the above had occurred by the time of data collection, the follow-up period ended on the data collection date.
Data analyses
Means with standard deviations (SD) were presented for normally distributed variables and medians with interquartile range (IQR) for variables with non-Gaussian populations.
Kaplan–Meier analysis was used to assess PJI risks associated with different BMI categories. Logistic and Cox regression were used to examine how BMI predicts the risk for PJI in relation to other baseline variables. 15 In regression models, BMI was modeled as a continuous variable to preserve the underlying variability of the data and to avoid information loss associated with categorization. 15 In the Cox models, the proportional hazards assumption was evaluated using Schoenfeld residuals, with no violations detected in any model. Variables previously associated with risk for PJI in the literature were selected for modeling, specifically indication for surgery, age, sex, ASA class, presence of kidney disease, presence of liver disease, and diabetic status.16–20
BMI values were missing for 2733 patients (1382 THA and 1351 TKA patients) and were handled using multiple imputation, assuming the values were missing at random. The imputations were performed in R separately for the THA and TKA datasets using the aregImpute function. The number of imputations was set to 10. The means of the imputed values were then calculated and added to the original datasets. Comparisons between the imputed dataset and the original dataset, from which missing values had been removed, showed no statistically significant differences when examined with the t-test.
The analysis of the marginal residual plot indicated a violation of the linearity assumption, prompting the use of a restricted cubic spline (RCS) transformation with four knots in both the logistic and Cox regression analyses. Due to hypothesized sex-based differences in adipose tissue distribution, the impact of BMI on PJI risk by sex was analyzed using a Cox multivariable model with an RCS-transformed BMI and an interaction term for sex. 21 To evaluate the discriminative ability and explained variance of the multivariable models, the concordance index (C-index) and Nagelkerke’s R² were calculated for the Cox multivariable models with and without BMI. A C-index of 0.5 indicates random prediction, whereas a value of 1.0 indicates perfect prediction. Several sensitivity analyses were performed to assess the consistency of the findings. These included analyses excluding patients with major comorbidities (rheumatoid arthritis, vascular disease, or diabetes), stratification by year of surgery to account for changes in PJI diagnostic criteria (before 2013, 2013-2017, and ⩾2018), and analyses excluding patients who underwent arthroplasty due to fracture. Results from multivariable analyses were presented with adjusted odds ratios (aOR) and adjusted hazard ratios (aHRs) with 95% confidence intervals (CIs). All analyses were performed using R (version 4.1.1; R Foundation for Statistical Computing, Vienna, Austria).
Ethical considerations
In accordance with Finnish legislation, no formal ethics committee review was required because of the retrospective register-based study design and because the patients were not contacted.
Results
During the study period, a total of 54,879 primary joint arthroplasties were performed, comprising 23,544 hip and 31,335 knee arthroplasties. The median age of the overall cohort was 68 years (IQR: 60–75) and was identical in patients undergoing THA and TKA. Of the total cohort, 60.0% were female (57.0% in THA and 62.3% in TKA). Patient demographics are presented in Table 1.
Patient demographics, diabetic status, and preoperative data.
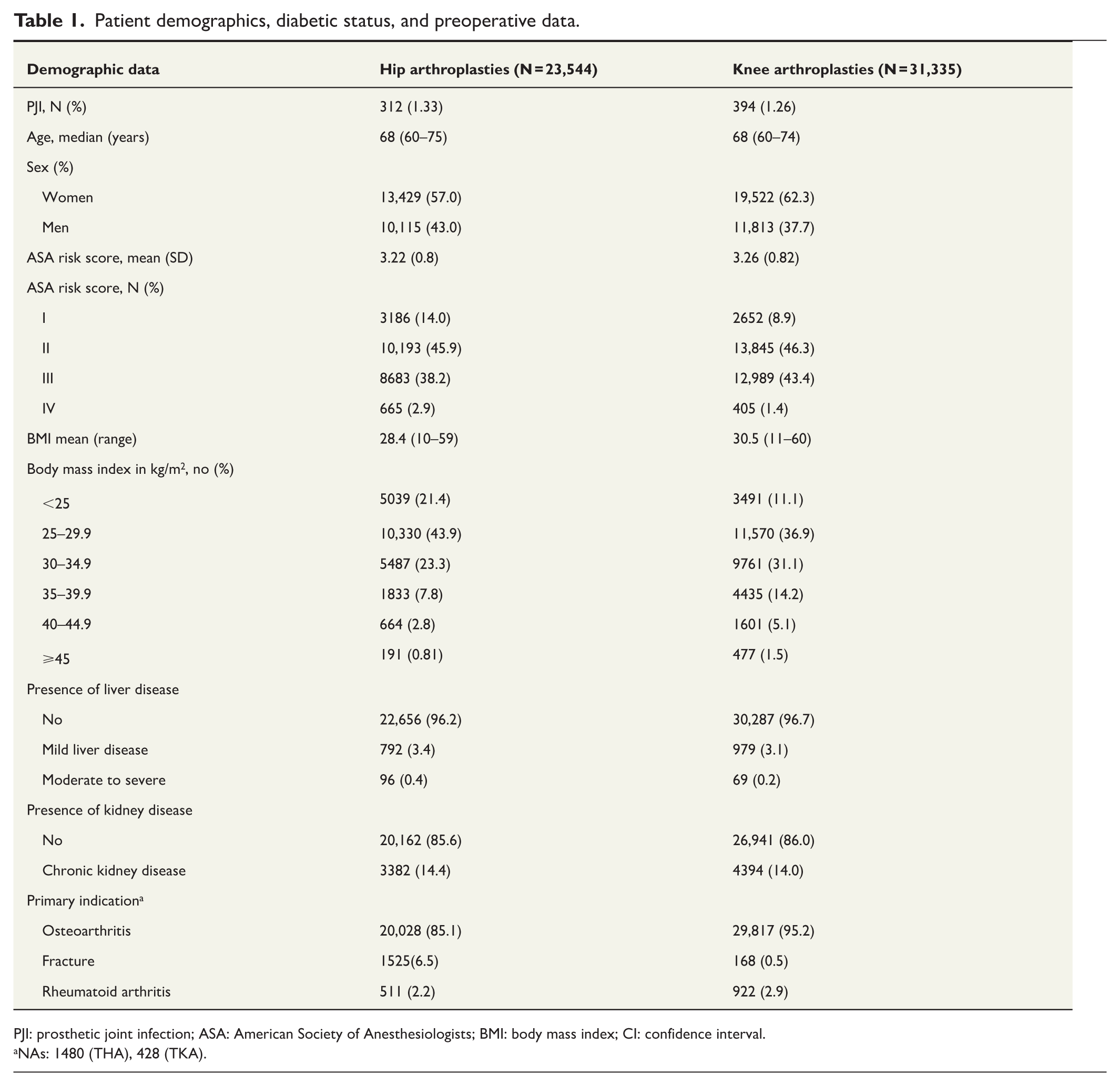
PJI: prosthetic joint infection; ASA: American Society of Anesthesiologists; BMI: body mass index; CI: confidence interval.
NAs: 1480 (THA), 428 (TKA).
The incidence of PJI within 90 days postoperatively was 1.1% (CI: 0.9%–1.2%) following THA and 0.8% (CI: 0.7%–0.9%) following TKA. The highest incidence of PJI within the 90-day follow-up period was observed in patients with a BMI >45: 6.4% (CI: 2.8%–9.9%) after THA and 3.4% (CI: 1.8%–5.1%) after TKA. The lowest incidence of PJI after THA was in patients with a BMI <25 (1.0%, CI: 0.7%–1.2%), whereas after TKA, the lowest incidence was seen in patients with a BMI of between 25 and 30 (1.01%, CI: 0.9%–1.2%). Detailed results are presented in Table 2.
Risk for PJI using Kaplan–Meier survival estimates.
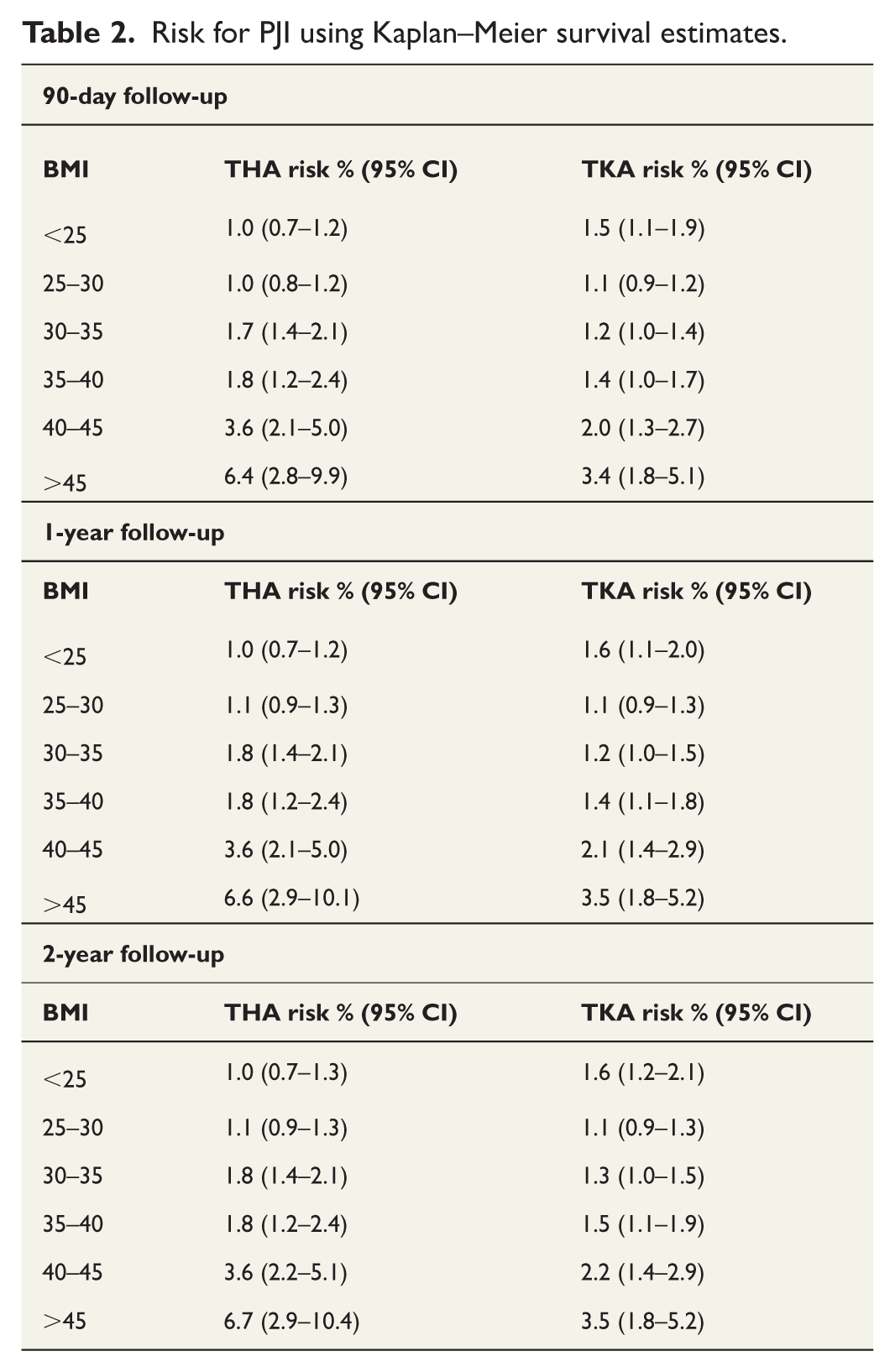
The incidence of PJI within 1 year postoperatively was 1.2% (CI: 1.1%–1.3%) following THA and 1.0% (0.9%–1.1%) following TKA. The highest incidence of PJI within 1-year follow-up was observed in patients with a BMI >45: 6.6% (CI: 2.9%–10.1%) after THA and 3.5% (CI: 1.8%–5.2%) after TKA. The lowest incidence of PJI after THA was in patients with a BMI <25 (1.0%, CI: 0.7%–1.2%), while after TKA, the lowest incidence was in patients with a BMI of between 25 and 30 (1.1%, CI: 0.9%–1.3%).
The incidence of PJI within 2 years postoperatively was 1.2% (CI: 1.1%–1.4%) following THA and 1.1% (CI: 1.0%–1.2%) following TKA. The highest incidence of PJI within 2-year follow-up was observed in patients with a BMI of >45, with incidences of 6.7% (CI: 2.9%–10.4%) after THA and 3.5% (CI: 1.8%–5.2%) after TKA. The lowest incidence of PJI was observed in patients with a BMI of <25 for THA (1.0%, CI: 0.7%–1.3%) and a BMI between 25 and 30 for TKA (1.1%, CI: 0.9%–1.3%). The incidence of PJI for all BMI categories is presented in Table 2, and Kaplan–Meier survival curves are shown in Figure 2.
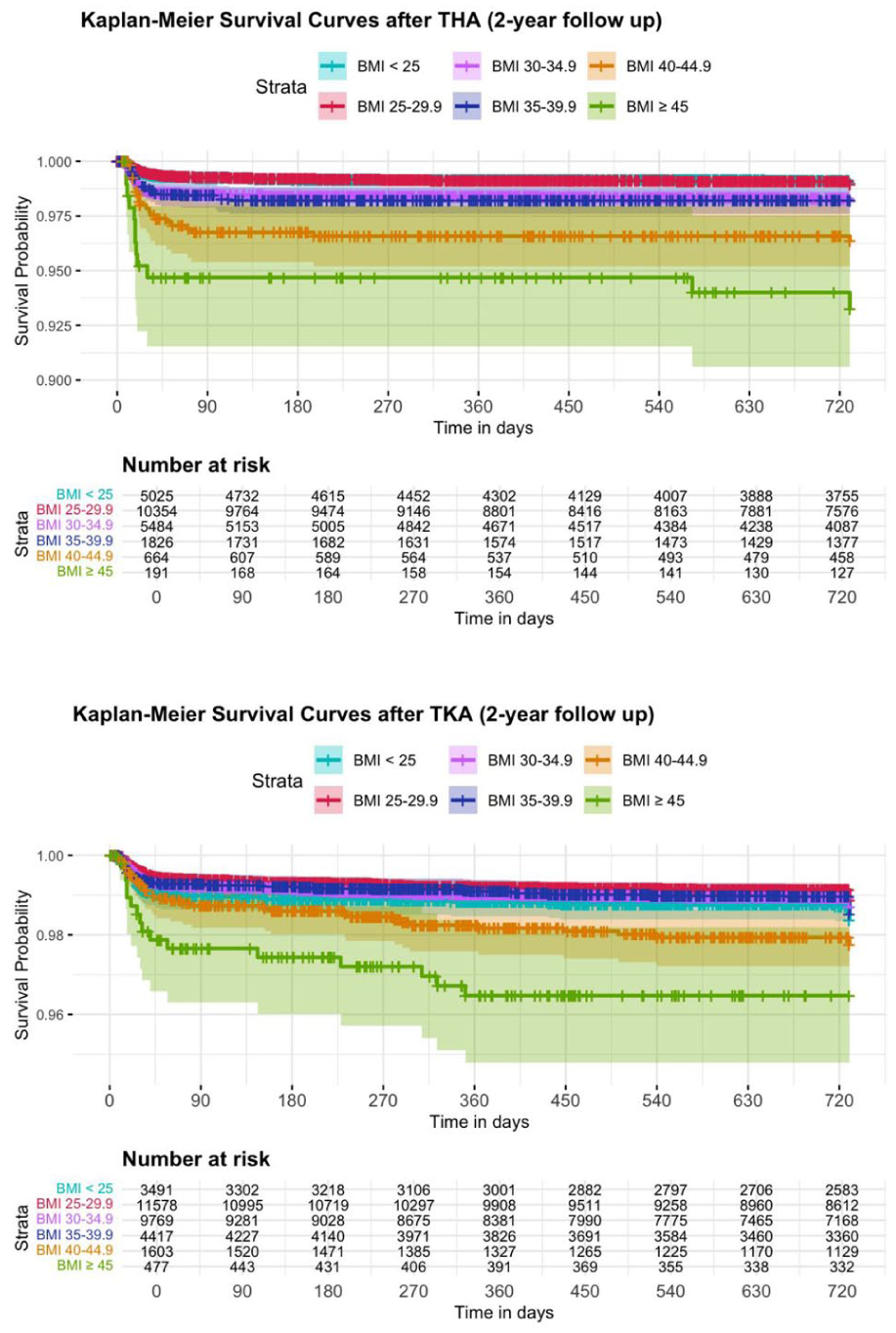
Kaplan–Meier curves.
Logistic regression analysis revealed that higher BMI was associated with an increased risk for PJI after both THA and TKA. After THA, the risk increased steadily with BMI, whereas after TKA, the association followed a J-shaped pattern, with both low and high BMI associated with a higher risk for PJI (Figure 3). In the Cox model, the association between BMI and PJI followed a J-shaped pattern after THA and TKA, with higher BMI associated with an increased risk, with both low and high BMI associated with increased risk (Figure 3). The detailed results from regression analyses are presented in the Supplementary file.
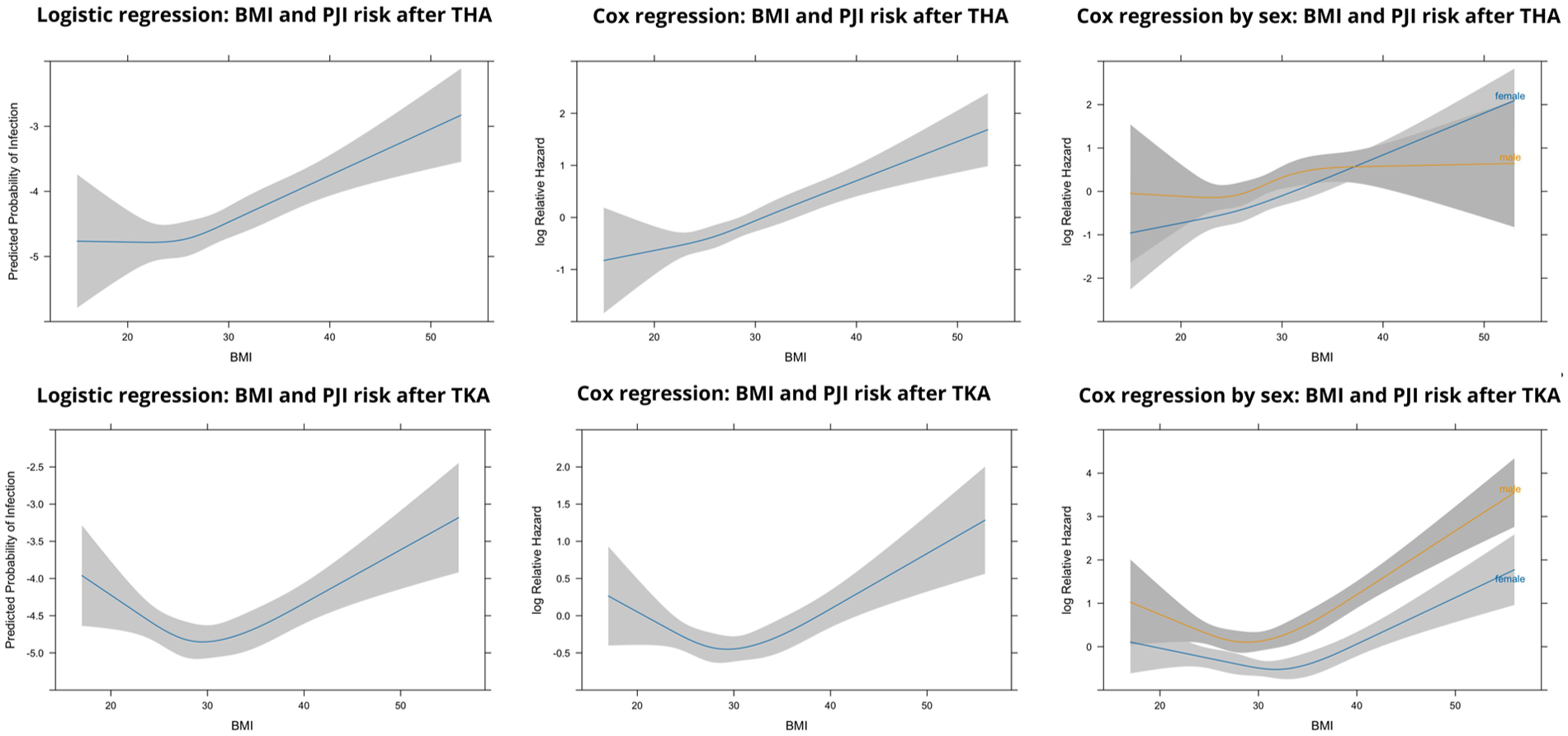
Association of BMI and PJI after primary total hip and knee arthroplasties. The figure summarizes multivariable logistic and Cox regression analyses evaluating the association between BMI and the risk of PJI. The left panels show predicted log odds of PJI derived from logistic regression models, the middle panels show estimated log relative hazards from Cox regression models, and the right panels show Cox regression analyses stratified by sex. In all panels, BMI is modeled as a continuous variable. More positive values on the y-axis indicate a higher risk of PJI.
Men had a higher risk for infection both after THA (90-day, 1-year, and 2-year aHR 1.3, CI: 1.0–1.6) and after TKA (90-day, 1-year, and 2-year aHR 2.0, CI: 1.6–2.5). Furthermore, a remarkable sex-specific difference in the association between BMI and the risk for PJI was observed among THA patients. For example, among women, the relationship exhibited a J-shaped curve, whereas in men, the J-shaped curve plateaued at higher BMI levels. Interestingly, no remarkable sex-related variation in infection risk was observed in TKA patients (Figure 3).
The C-index of the multivariable analysis with BMI was 0.68 for THA and 0.66 for TKA, whereas the C-index without BMI was 0.64 and 0.65, respectively. The R² values with BMI were 0.024 for THA and 0.020 for TKA, and 0.016 for THA and 0.015 for TKA without BMI, indicating a small improvement in model performance when BMI was included.
In the supplementary analyses limited to patients without major comorbidities, analyses excluding fracture-related arthroplasties, and analyses stratified by year of surgery according to diagnostic criteria, the association between BMI and PJI was consistent from the analyses for the whole cohort. Detailed results from these subgroup analyses are provided in the Supplementary file.
Discussion
Our findings highlight that BMI is not linearly associated with risk for PJI after THA and TKA. Instead, the relationship is more complex. The influence of BMI on infection risk varies considerably between men and women. In those patients with a BMI of >45, however, PJI risk levels become notably high.
We acknowledge a few limitations in this study. Ideally, the impact of risk factors on the rate of PJI should have been studied in a prospective setting. However, due to the low incidence of PJI, gathering sufficient data within a reasonable timeframe would have been challenging. Consequently, we opted for a retrospective approach, using our institution’s prospectively filled database, which allowed us to achieve a large sample size. As this was a single-center study conducted at a high-volume arthroplasty center, the generalizability of the findings to lower-volume hospitals may be limited; however, high procedural volume and standardized practices may have reduced random variation. A further limitation was that data on patients’ smoking status were not available. This may introduce bias, as both malnutrition and smoking are known to increase the risk of PJI.19,22 Nevertheless, given the large, prospectively collected dataset representing a broad population, the potential impact of smoking on the results was likely to be minimal. In addition, the number of underweight patients (BMI < 20 kg/m²) was small, limiting statistical power and precluding separate analyses for this subgroup.
Obesity has increased globally, with the number of overweight individuals expected to rise further.13,14 Individuals with obesity are 2–4 times more likely to undergo joint arthroplasty and may need surgery at a younger age.23–25 This could potentially lead to a notable rise in the incidence of these infections, which has already been reported from the Nordic countries. 26
Previous studies have reported that the risk for PJI increases with higher BMI.3,27 Specifically, each two-unit increase in BMI raises the risk by 10%. 27 It has also been suggested that individuals with obesity (BMI 35–40 kg/m²) have twice the risk for PJI compared to those with normal weight, while a BMI >40 increases the risk by 3 to 4 times.3,27 Conflicting results have also been reported.12,28–31 The findings of our study clearly showed that a higher BMI was associated with an increased risk for PJI after both THA and TKA. At BMI values above 40, the cumulative incidence of PJI increased, and the regression analyses demonstrated a more pronounced association between BMI and PJI risk. The impact of BMI on infection risk follows a J-shaped pattern, with infection risk rising in line with increases in BMI. Therefore, in contrast to previous studies, our study demonstrates a nonlinear association between BMI and PJI, thereby questioning the assumption that each unit increase in BMI corresponds to a consistent percentage rise in infection risk.3,27 In addition to obese patients, underweight patients have also been reported to have an increased risk for PJI following TKA surgery, 22 although contradictory results have also been reported in both TKA and THA patients. 27 Given the limited number of underweight patients, this patient group could not be separately analyzed in our study.
The literature has consistently demonstrated that obesity is more harmful to men than to women. 32 For example, abdominal obesity, which is more common in men, is more dangerous than fat distribution in the thigh and hip regions. 33 Given that trunk fat has been associated with an increased risk for cardiovascular disease, metabolic disorders, cancer, and mortality, it is reasonable to assume that similar physiological mechanisms may also contribute to a heightened risk for PJI.32,34 Chaudhry et al. 35 found that morbidly obese women had a higher risk for PJI than morbidly obese men 30 days after primary THA. In our multivariable analysis, men had a higher overall risk for PJI both after TKA and THA. After THA, however, the risk for PJI in women increased hand in hand with increasing BMI, whereas in men, the risk plateaued at around a BMI of 35. As a result, a BMI of approximately 38 or greater in women resulted in higher risk for PJI, supporting the findings of Chaudhry et al. 35 An explanation for this finding may be that women tend to accumulate more adipose tissue subcutaneously, with greater accumulation in the hip area, regardless of BMI.21,36 This could lead to suboptimal tissue oxygenation in the incision area, and lower serum and tissue concentrations of prophylactic antimicrobial agents. Adipose tissue has also been associated with impaired immune function and the secretion of pro-inflammatory cytokines, which may increase susceptibility to infection. 8
Various BMI cutoff points have been proposed. When the BMI cutoff is lowered, a growing number of patients are denied access to surgery where they would have experienced a complication-free outcome. The American Academy of Orthopaedic Surgeons (AAOS) clinical practice guidelines define obesity as meeting moderate-strength criteria for increased PJI risk and recommend considering delaying surgery when the BMI is above 40, especially if the patient has other risk factors.9,10 DeMik et al. 37 found that with a BMI cutoff of 50, nine patients must be excluded from THA surgery to prevent one complication; lowering the cutoff to 30 increases this number to 17. Giori et al. 38 reported similar findings; with a BMI cutoff of 50, four patients must be excluded from total joint arthroplasty surgery to prevent one complication, whereas lowering the cutoff to 30 increases this number to 18. Studies have also been published that challenge strict cutoff points.12,39
Our results revealed that the association between BMI and infection risk followed a J-shaped pattern, meaning that both low and high BMI increased the risk for infection. This challenges the justification for strict upper BMI limits, as underweight individuals are also at risk. Moreover, after the slope shifted from decreasing to increasing, the relationship between BMI and infection risk exhibited a steady rise rather than a sharp threshold effect, suggesting that strict BMI cutoff points are not justified. In addition, the impact of BMI on infection risk varied between men and women, suggesting that BMI does not affect all patients equally, further challenging the validity of universal BMI cutoffs.
These considerations raise the question as to whether the absolute increase in risk is significant enough to justify strict BMI criteria, or whether it would be more beneficial to focus on other risk factors when making surgical decisions. Tightening the BMI cutoff points may reduce the number of complications, but this would come at the cost of many potentially successful surgeries, especially when the cutoff points are set very low. Given that underweight patients, as well as those with obesity, face elevated risks for PJI, a more personalized approach to surgical eligibility and preoperative management may be necessary. Hence, besides solely focusing on BMI, it is important to weigh what constitutes an acceptable balance between avoiding complications and providing access to care.
Conclusion
The risk for PJI does not increase linearly with BMI. Furthermore, the risk differs between men and women. It appears, however, that once BMI is greater than 45, the risk levels become notably high. Otherwise, the absolute risk differences between different BMI categories are relatively low. Thus, rather than focusing solely on BMI, more emphasis should be placed on individualized risk assessment and shared decision-making.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969261438911 – Supplemental material for Time to move beyond BMI alone in predicting arthroplasty infections: A large single-center retrospective cohort study
Supplemental material, sj-docx-1-sjs-10.1177_14574969261438911 for Time to move beyond BMI alone in predicting arthroplasty infections: A large single-center retrospective cohort study by Elisa Kosonen, Rasmus Liukkonen, Aleksi Reito, Eerik Skyttä and Antti Eskelinen in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors would like to thank Peter Heath for the language editing of the manuscript.
Author contributions
All authors contributed to the study conception and design. Data analysis, statistical processing, visualization, and drafting of the first version of the manuscript were performed by E.K. All authors provided comments on previous versions of the manuscript and approved the final version for submission.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.K., R.L., and E.S. declare no conflicts of interest related to the subject matter or content of this article. There are no financial or personal relationships with other individuals or organizations that could inappropriately influence the research. A.R. reports other financial or material support from a company or supplier: paid course from Zimmer Biomet. He also serves on editorial/governing boards of orthopedic journals: Scandinavian Journal of Surgery (section editor) and Acta Orthopaedica (social media editor). A.E. reports speaker’s bureau/paid presentations: lecture fees from Heraeus Medical GmbH and J&J Medtech. He is also an Advisory Board Member in the Finnish Arthroplasty Register.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by personal grants to E.K. from the Orion Research Foundation and Saply (Suomen Artroplastiayhdistys). All relevant funding sources were disclosed, and the research was conducted independently of the funders.
Data availability statement
The data that support the findings of this study are derived from the patient registry of Coxa Hospital for Joint Replacement. Due to privacy and ethical restrictions under Finnish legislation, the data are not publicly available.
Social media summary
Strict BMI cut-offs may be misleading: BMI is not linearly associated with PJI. However, extremely high BMI can increase risk, and risk profiles differ between women and men. Findings from 54,879 cases support shared decision-making.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.