
Abstract
Background: Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are no longer considered inpatient-only procedures. Qualifying for inpatient status reimbursement requires additional, unreimbursed administrative effort, and may limit care to these patients. Purpose: We sought to evaluate and compare the overall health status of patients receiving THA and TKA. Methods: We conducted a retrospective review evaluating 2207 patients undergoing primary THA and TKA from 2015 to 2018 at a single institution. Clinical parameters, surgical procedure, medical history, laboratory values, length of stay (LOS), and discharge location were recorded and compared between the 2 groups. Results: In 2202 patients, we observed differences for body mass index (THA = 29.4 ± 0.4, TKA = 32.1 ± 0.3), low-density lipoprotein cholesterol levels (THA = 105.8 ± 13.5 mg/dL; TKA = 128.6 ± 13.7 mg/dL), and blood glucose levels (THA = 98.2 ± 1.7 mg/dL; TKA = 101.4 ± 1.3 mg/dL), indicating that TKA patients were more likely than THA patients to be classified as obese, hypercholesterolemic, and hyperglycemic. We observed longer LOS in THA patients (51.25 hours, 95% CI ± 3.87 hours) than in TKA patients (36.93 hours, 95% CI ± 1.17 hours). A greater proportion of TKA patients were discharged home (81.97%, N = 1155) rather than to additional care facilities compared with THA patients (71.84%, N = 539). Conclusion: In this retrospective study, we observed that TKA patients had higher rates of comorbidities than did THA patients, but TKA patients spent less time in the hospital and were more likely to be discharged home. Future studies should evaluate reasons for poor clinical outcomes for patients undergoing total joint arthroplasty with an outpatient designation.
Introduction
There are approximately 1 million total hip arthroplasty (THA) and total knee arthroplasty (TKA) procedures performed annually in the United States, and this number is expected to surpass 1.5 million per year by 2030 [15]. In 2018, the Centers for Medicare and Medicaid Services (CMS) updated guidelines on evaluation of TKA patients for appropriate hospital stay classification; updated guidelines for THA followed in 2020 [11]. However, inappropriately assigning an outpatient designation to a total joint arthroplasty (TJA) procedure can translate into worse outcomes, more readmissions, and decreased rates of satisfaction [3,10]. Although the outpatient designation presents a clear financial benefit for CMS, the classification of either inpatient or outpatient creates an administrative burden on surgeons [17]. Inpatient designation may place increased burden on value-based care systems [11]. As well, more medically complex patients who require a hospital admission spanning more than 2 midnights may have limited access to centers that provide the higher level of care required for inpatient status.
The purpose of our study was to evaluate the overall health status of patients undergoing primary THA and TKA. We sought to determine whether THA patients possess the same number of medical comorbidities and criteria for inpatient status as TKA patients. Another aim of this investigation was to evaluate if an increase in hospital length of stay (LOS) or a non-home discharge are associated with increased medical comorbidities. We hypothesized that for both issues listed above, there would be no differences between THA and TKA patients. Finally, we considered how outpatient TJA may affect access to care.
Methods
We performed a retrospective chart review of primary THA and TKA procedures that took place at a single institution from January 2015 to December 2018. Institutional review board approval was obtained. All patients were identified via current procedural terminology (CPT) billing codes for primary THA or TKA. Exclusion criteria were revision surgery, conversion of unicompartmental knee arthroplasty to TKA, surgery for trauma (ie, hip fracture), incomplete medical records, or age < 18 years.
Medical records were reviewed to obtain the following parameters: clinical—age, gender, body mass index (BMI), and blood pressure; surgical—TKA or THA, American Society of Anesthesia (ASA) score, and estimated blood loss (EBL); fasting laboratory values—low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL), cholesterol, glucose, hematocrit, hemoglobin, vitamin D2, sodium, potassium, chloride, bicarbonate, creatinine, glucose, calcium, albumin, total bilirubin, direct bilirubin, alkaline phosphatase, total protein, lactate dehydrogenase, phosphate, uric acid, thyroxine, thyroid-stimulating hormone, white blood cell count, red blood cell count, neutrophil %, lymphocyte %, monocyte %, and eosinophil %; past medical history—number of previous orthopedic surgeries, pain medication use, osteoarthritis, previous falls, heart disease, peripheral vascular disease, stroke, and cancer; hospital LOS; and discharge location.
Statistical Analysis
Pairwise comparisons of each parameter were performed using an independent samples t-test for all patients as well as male and female patients separately. In addition, pairwise comparisons between TKA and THA patients for frequency of previous history of osteoarthritis, heart disease, peripheral vascular disease, stroke, and cancer as well as frequency of obesity (BMI > 30 kg/m2), and abnormal labs were examined using χ2 analysis. Type I error was set at α = 0.05 for all analyses. For all significant comparisons, effect size was calculated using either a Cohen’s d (t-test) or phi (χ2) statistic and was interpreted as follows: 0 to 0.1 (negligible, N), 0.1 to 0.3 (small, S), 0.3 to 0.5 (moderate, M), 0.5 to 0.7 (large, L), > 0.7 (very large, VL) [9].
Results
There were 2207 patients eligible for evaluation. After application of exclusion criteria, 2202 (THA: 349 male, 412 female; TKA: 623 male, 818 female) charts were available for final evaluation (Table 1). No pairwise differences between groups were detected for previous history of disease (Table 2) or preoperative vital statistics (Table 3). Significant differences between groups were observed for the following parameters: BMI (Table 1), LDL cholesterol (Table 4), and blood glucose levels (Table 4) resulting in a greater frequency of TKA patients classified as obese, hypercholesterolemic, and hyperglycemic compared with THA patients (Supplemental Fig. 1) (P < .05). No other variables from laboratory values, ASA score, or EBL were different between groups.
Patient demographics.
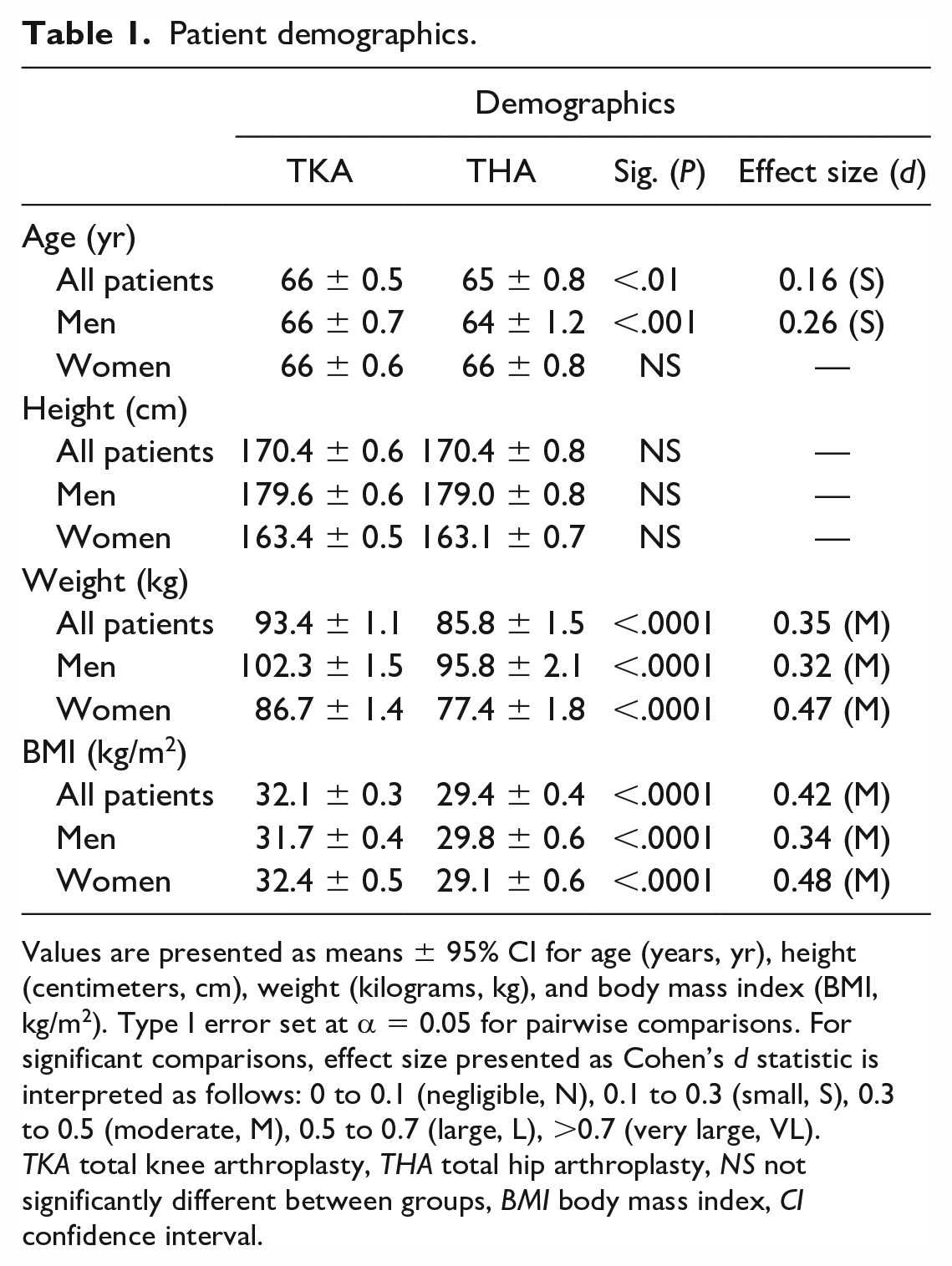
Values are presented as means ± 95% CI for age (years, yr), height (centimeters, cm), weight (kilograms, kg), and body mass index (BMI, kg/m2). Type I error set at α = 0.05 for pairwise comparisons. For significant comparisons, effect size presented as Cohen’s d statistic is interpreted as follows: 0 to 0.1 (negligible, N), 0.1 to 0.3 (small, S), 0.3 to 0.5 (moderate, M), 0.5 to 0.7 (large, L), >0.7 (very large, VL).
TKA total knee arthroplasty, THA total hip arthroplasty, NS not significantly different between groups, BMI body mass index, CI confidence interval.
Previous medical history.
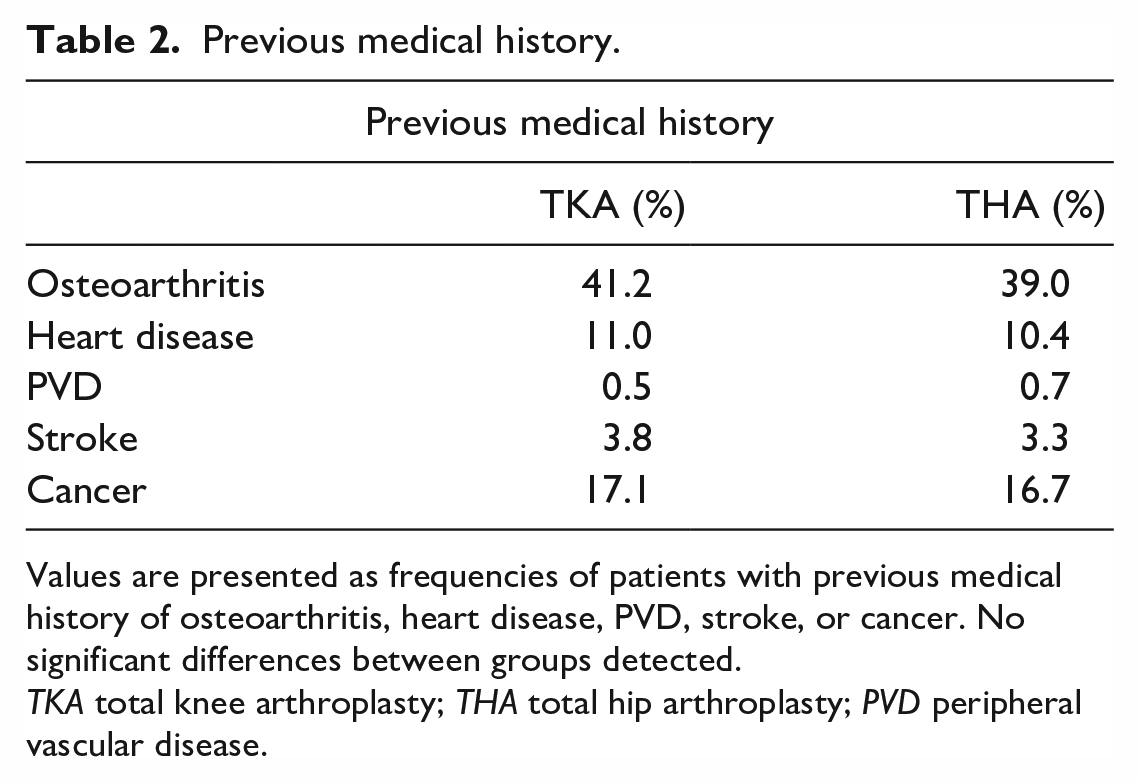
Values are presented as frequencies of patients with previous medical history of osteoarthritis, heart disease, PVD, stroke, or cancer. No significant differences between groups detected.
TKA total knee arthroplasty; THA total hip arthroplasty; PVD peripheral vascular disease.
Preoperative vitals.
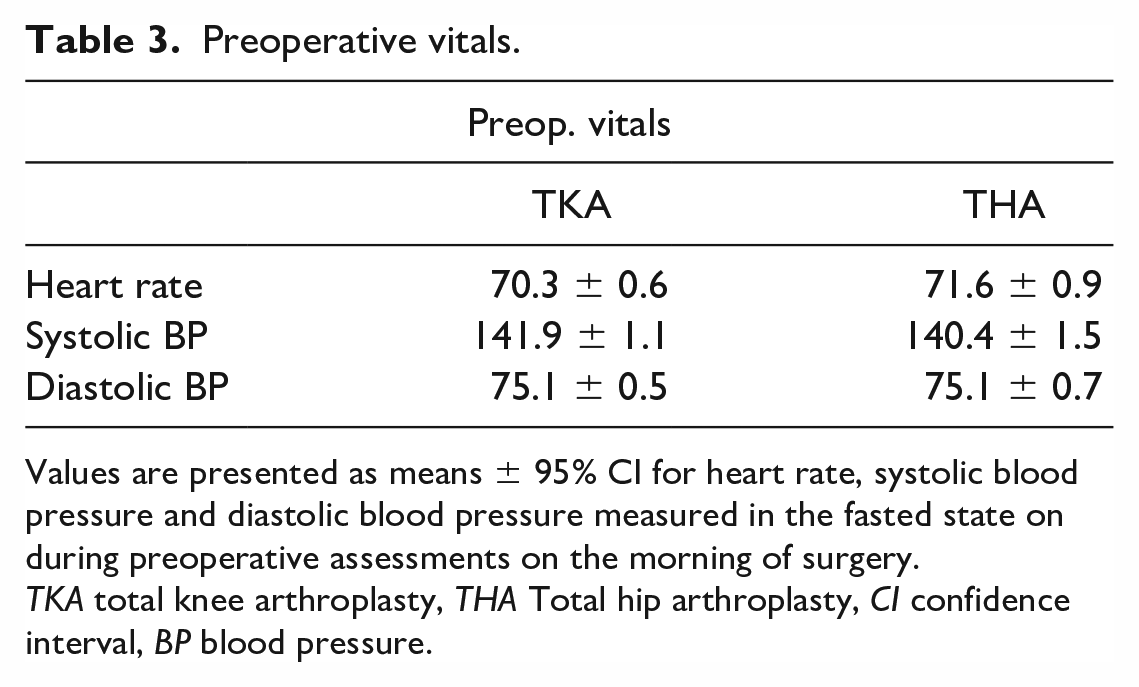
Values are presented as means ± 95% CI for heart rate, systolic blood pressure and diastolic blood pressure measured in the fasted state on during preoperative assessments on the morning of surgery.
TKA total knee arthroplasty, THA Total hip arthroplasty, CI confidence interval, BP blood pressure.
Fasted preoperative blood lipids and glucose.
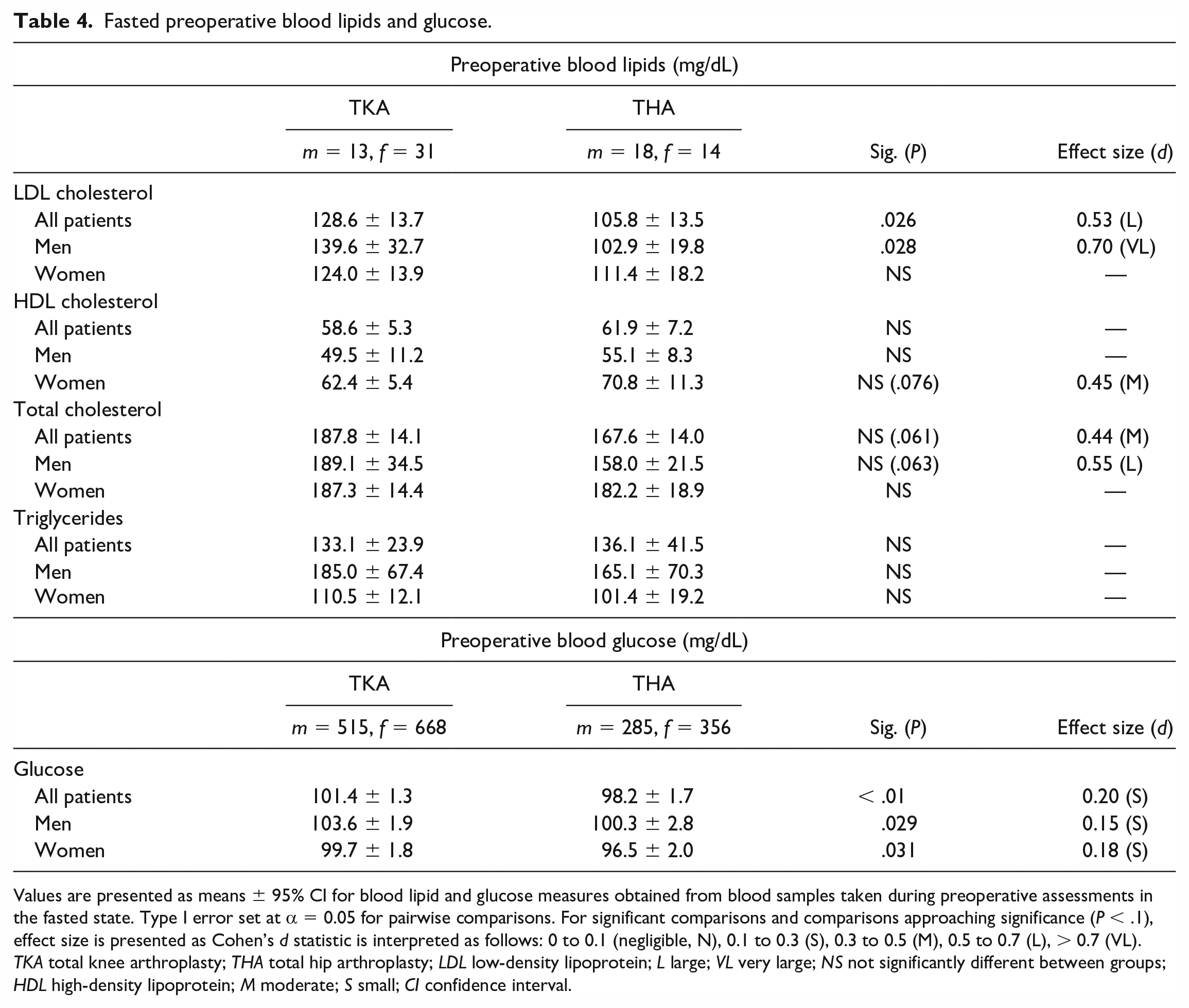
Values are presented as means ± 95% CI for blood lipid and glucose measures obtained from blood samples taken during preoperative assessments in the fasted state. Type I error set at α = 0.05 for pairwise comparisons. For significant comparisons and comparisons approaching significance (P < .1), effect size is presented as Cohen’s d statistic is interpreted as follows: 0 to 0.1 (negligible, N), 0.1 to 0.3 (S), 0.3 to 0.5 (M), 0.5 to 0.7 (L), > 0.7 (VL). TKA total knee arthroplasty; THA total hip arthroplasty; LDL low-density lipoprotein; L large; VL very large; NS not significantly different between groups; HDL high-density lipoprotein; M moderate; S small; CI confidence interval.
Obesity was recorded more often in the TKA cohort. The mean BMI in THA patients was 29.4 (95% CI ± 0.4 kg/m2), compared with 32.1 (95% CI ± 0.3 kg/m2) in TKA patients (Table 1; P < .0001; ES: 0.42 M). When examining frequency of obesity, 40% of THA patients were found to be categorized as obese compared with 58% of TKA patients (Supplemental Fig. 1a; P < .0001; ES: 0.34 M). These findings were also observed to be similar when analyzing men and women separately (P < .0001).
Levels of LDL cholesterol were found to be higher in the TKA cohort (P < .01). The mean total cholesterol value for THA patients was 167.6 mg/dL (95% CI ± 14 mg/dL) compared with 187.8 mg/dL (95% CI ± 14.1 mg/dL) for TKA patients, which approached but did not reach statistical significance (Table 4; P = .061). When comparing clinically important cutoffs, 39% of TKA patients were observed to have “high” total cholesterol (> 200 mg/dL), while only 16% of THA patients were deemed high (Supplemental Fig. 1d;P = .03; ES: 0.51 L). Notably, this difference was primarily attributed to LDL cholesterol, where THA patients had a mean LDL of 105.8 (95% CI ± 13.5 mg/dL) compared with 128.6 mg/dL (95% CI ± 13.7 mg/dL) for TKA patients (Table 4; P = .026; ES: 0.53 L). When comparing clinically important cutoffs, 43% of TKA patients were observed to have “high” LDL cholesterol (> 100 mg/dL), compared with 16% of THA patients (Supplemental Fig. 1c; P < .01; ES: 0.65 L). There was no statistically significant difference in HDL cholesterol values between the groups.
When comparing clinically important cutoffs, THA patients were more likely to have normal blood glucose (66% THA vs 58% TKA), while being less likely to be pre-diabetic (100-124 mg/dL; 26% THA vs 30% TKA) or diabetic (> 125 mg/dL; 8% THA vs 11% TKA) (Supplemental Fig. 1b; P = .01; ES: 0.17 S) The mean blood glucose value in THA patients was 98.2 mg/dL (95% CI ± 1.7 mg/dL) compared with 101.4 mg/dL (95% CI ± 1.3 mg/dL) in TKA patients (Table 4; P < .001; ES: 0.2 S).
Length of stay was observed to be longer for THA patients (51.25 hours, 95% CI ± 3.87 hours) compared with TKA patients (36.93 hours, 95% CI ± 1.17 hours) (P < .001; ES: 0.35 M). A greater proportion of TKA patients were discharged home (81.97%, N = 1155) instead of additional care facilities compared with THA patients (71.84%, N = 539) (P < .001; ES: 0.11 S).
Discussion
In this retrospective cohort study, we observed objectively worse overall health status in TKA patients compared with THA patients, with significance observed for obesity, hypercholesterolemia, and hyperglycemia. However, we also observed that TKA patients had a hospital LOS that was 14 hours less and were 10% more likely to be discharged home than THA patients, despite the greater prevalence of medical comorbidities in TKA patients.
Limitations of the study include its retrospective nature and the inclusion of data found in the electronic medical record. In addition, preoperative blood lipid levels were available only for a small fraction of our total patient population (TKA = 44; THA = 32) and therefore may be underpowered for comparison. Despite reduced patient numbers for this comparison, statistical significance paired with medium to very large effect sizes were observed, which provides a reasonable confidence in the findings. We did not perform an outcome or cost analysis on the identified medical comorbidities, which makes it difficult to determine what clinical relevance these findings may have. Finally, as a single institution study, our findings may lack generalizability.
When the CMS published guidelines for removing TKA and THA from the inpatient-only list, they made recommendations on which patients would be appropriate for inpatient admission. These included patients needing postsurgical rehabilitation or skilled nursing facility admission; patients undergoing technically challenging procedures; and those with morbid obesity (BMI > 35), diabetes (HbA1c > 7), baseline anemia (Hgb < 10 mg/dL), chronic kidney disease, coronary artery disease or uncontrolled hypertension, chronic obstructive pulmonary disease on multiple medications and/or home oxygen, baseline abnormal mental status that would require close monitoring, and other risk factors (including surgical risk, postoperative bleeding risk, and postoperative safety risk) [4]. Based on our evaluation of medical comorbidities, we believe that many patients undergoing TJA, particularly those covered by Medicare, would qualify for inpatient admission status despite these new guidelines. The criteria for inpatient admission status were more commonly achieved in TKA patients. This is before even considering social implications, which often affect where and when patients can be discharged. Prior authors have suggested that the amount of caregiver assistance available to a patient after TJA was an independent predictor of discharge location [2], which is a factor the Medicare criteria do not explicitly consider.
Much research exists on health status for TJA patients as it relates to postoperative outcomes, but studies on preoperative health status differences between THA and TKA patients is scarce. A prior study comparing retired (> 65 years) to working-age (< 65 years) patients undergoing TKA evaluated several health parameters and found that younger TKA patients were largely overweight or obese, and the majority had > 2 medical comorbidities [8], consistent with our findings. Another study sought to determine the quality of life in patients on a TJA waiting lists and found that 63% of patients had cardiovascular disease, 33% had high blood pressure, 33% had diabetes, and 33% had endocrinologic issues [16].
Financial savings were a large driver behind the CMS decision to take TJA off the inpatient-only list. Lovald et al [12] compared extended stay (3-4 days) with short stay (1-2 days) and outpatient TKA, and found outpatient procedures saved $8527 on average compared with extended stay, and short stay saved $1967 compared with extended stay. Another study, which compared outpatients with inpatients, found that outpatient procedures cost roughly $6487, compared with $9643 for inpatients, for a savings of $3155 [7]. Regardless of the patient status, the goal of a hospital stay should be early, safe discharge. A study by Sibia et al [14] showed a savings of $1814 if a patient was discharged on postoperative day 2 to a skilled nursing facility rather than on postoperative day 3 after TKA. About 23% of patients in our study required discharge to an additional care facility; discharge to a rehabilitation facility after initial admission under non-inpatient status can result in an additional day in the hospital to meet Medicare’s minimum 2-day inpatient requirement [4], at further cost to the hospital.
With removal of THA and TKA from the inpatient-only list, there has been a push toward outpatient surgery, and Medicare has finally joined the outpatient TJA trend, adding outpatient coverage to the Medicare list in 2020 [13]. It is predicted that in coming years CMS may eliminate the inpatient option altogether from elective TJA surgery, as removal from the inpatient-only list pushed a nearly 2-fold increase in TKAs to the outpatient setting. With CMS now covering outpatient surgeries, one would expect a similar trend in increasing practice migration with all joint replacements. Indeed, 15% of TJAs migrated to the outpatient setting at the time of the announcement [13], while another study projected that by 2026 more than 50% of TJAs would be performed in an outpatient ambulatory surgery center (ASC) [5]. As TJA moves to the outpatient setting, concerns arise about limited access to care, as some surgeons may be discouraged from operating on patients with medical comorbidities that make them “poor” candidates for the ASC setting. If CMS, and therefore private payer insurance, were to lower reimbursements for these surgeries, it would effectively decrease the number of health systems and surgeons willing to perform them. This would concentrate the sickest (and usually poorest) patients into a few centers, resulting in losses to those centers and incentivizing systems to not operate on these types of patients [6]. While the impetus toward outpatient surgeries is promising when evaluating costs, that must be tempered that with consideration for the ongoing need of well-reimbursed, inpatient TJA in less healthy patients. The goal would be to not further the access discrepancy, wherein those in the lowest socioeconomic brackets may be less likely to receive THA or TKA [1].
In conclusion, our retrospective study suggests that in our institution, the overall health status of TKA patients was more complex preoperatively compared with that of THA patients. On the other hand, TKA patients were hospitalized 14 fewer hours and were 10% more likely to be discharged home than THA patients. Future studies should evaluate clinical outcomes of patients mandated to earlier discharge because they do not qualify for inpatient status under CMS guidelines, to determine whether this is beneficial for both the patient and CMS.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231209308 – Supplemental material for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care
Supplemental material, sj-docx-1-hss-10.1177_15563316231209308 for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care by Katharine D. Harper, Thomas C. Sullivan, Austin Wininger, Stephen J. Incavo and Bradley S. Lambert in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231209308 – Supplemental material for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care
Supplemental material, sj-docx-2-hss-10.1177_15563316231209308 for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care by Katharine D. Harper, Thomas C. Sullivan, Austin Wininger, Stephen J. Incavo and Bradley S. Lambert in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231209308 – Supplemental material for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care
Supplemental material, sj-docx-3-hss-10.1177_15563316231209308 for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care by Katharine D. Harper, Thomas C. Sullivan, Austin Wininger, Stephen J. Incavo and Bradley S. Lambert in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231209308 – Supplemental material for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care
Supplemental material, sj-docx-4-hss-10.1177_15563316231209308 for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care by Katharine D. Harper, Thomas C. Sullivan, Austin Wininger, Stephen J. Incavo and Bradley S. Lambert in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316231209308 – Supplemental material for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care
Supplemental material, sj-docx-5-hss-10.1177_15563316231209308 for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care by Katharine D. Harper, Thomas C. Sullivan, Austin Wininger, Stephen J. Incavo and Bradley S. Lambert in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316231209308 – Supplemental material for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care
Supplemental material, sj-docx-6-hss-10.1177_15563316231209308 for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care by Katharine D. Harper, Thomas C. Sullivan, Austin Wininger, Stephen J. Incavo and Bradley S. Lambert in HSS Journal®
Supplemental Material
sj-docx-7-hss-10.1177_15563316231209308 – Supplemental material for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care
Supplemental material, sj-docx-7-hss-10.1177_15563316231209308 for Health Status of Total Hip Versus Total Knee Arthroplasty Patients and Possible Effects on Decisions Regarding Surgical Location, Cost, and Access to Care by Katharine D. Harper, Thomas C. Sullivan, Austin Wininger, Stephen J. Incavo and Bradley S. Lambert in HSS Journal®
Footnotes
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bradley S. Lambert, PhD, reports a relationship with Delfi Medical Innovations. Stephen J. Incavo, MD, declares relationships with Innomed, Kyocera, Microport Orthopedics, Osteoremedies, Smith & Nephew, Wright Medical Technology, and Zimmer Biomet. The other authors declare no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived for all patients included in this study.
Level of Evidence
Level III: Retrospective Cohort Study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.