
Abstract
We describe a modified surgical technique developed to enhance the classical irrigation and debridement procedure to improve the possibilities of retaining an infected total knee arthroplasty. This technique, debridement antibiotic pearls and retention of the implant (DAPRI), aims to remove the intra-articular biofilm allowing a higher and prolonged local antibiotic concentration using calcium sulfate beads. The combination of three different surgical techniques (methylene blue staining, argon beam electrical stimulation, and chlorhexidine gluconate brushing) might enhance the identification, disruption, and finally removal of the bacterial biofilm, which is the main responsible of antibiotics and antibodies resistance. The DAPRI technique might represent a safe and more conservative treatment for acute and early hematogenous periprosthetic joint infection.
Introduction
Total knee arthroplasty (TKA) is one of the most successful procedures in orthopedic surgery, yet nearly 20% of patients remain unsatisfied by their clinical outcomes. Principal causes of TKA failures include periprosthetic joint infection (PJI), instability, failure of osteointegration, and polyethylene wear. 1 TKA failures can occur early (<2 years) or late (>2 years), and PJI represents one of the main causes of an early complication. 2 PJI can have a devastating effect locally as well as on the general health of the patient, often leading to a decrease in daily activity level and an increase in mortality. While the incidence of PJI following primary TKA may only be approximately 1–2% over the lifetime of a prosthetic joint, 3 nearly 25% of all TKA failures today are due to infection. 2
PJI represents a significant economic burden. The annual incidence of PJIs in the United States is predicted to be between 38,000 and 270,000 by 2030. 4 The average cost per hospitalization of a PJI has been estimated to be US$24,200. 5 In the United States, US$566 million was spent treating PJI in 2006, and this is projected to increase to US$1.62 billion by 2020. 5
The current evidence supports several surgical treatments depending on timing. 6,7 Exchange arthroplasty is indicated in chronic and delayed PJI; whether this occurs best as an immediate or staged replant may depend on the identification and virulence of the microorganism and patient factors. 8 –11 However, in the case of an acute or early hematogenous infection (within 4–6 weeks from the original surgery or 7 days from symptom onset), debridement, antibiotics, and implant retention (DAIR) procedure is often employed as a reasonable treatment choice.
The current authors here describe a novel surgical technique developed to enhance the classical DAIR procedure to improve the possibilities of retaining an infected implant. The following surgical technique, debridement, antibiotic pearls, and retention of the implant (DAPRI), aggressively improves upon the conservative DAIR procedure in several aspects. First, by incorporating bioabsorbable antibiotic pearls, we believe that we can prolong the local antibiotic concentration. In addition, we describe a targeted and focused removal of biofilm on implant and soft tissue surfaces by incorporating an initial intra-articular staining injection.
Surgical technique
At present, we applied DAPRI procedure in settings that would otherwise be amenable to DAIR—that is, with acute (within 4–6 weeks from the original surgery) or early hematogenous (within 7 days from clinical onset) infections with a known microorganism. At our institution, we have not performed the DAPRI procedure outside of these indications.
The DAPRI procedure has a stepwise approach. Following the administration of regional and neuraxial anesthesia, (an adductor canal block and spinal anesthesia at our institution), 12 preoperative antibiotic therapy is intentionally held to improve the sensitivity of intraoperative cultures.
Methylene blue-guided debridement
Prior to skin incision and arthrotomy, a large bore needle is introduced into the knee and as much fluid as possible is aspirated from the knee joint. This is sent for culture. Fifty milliliters of dilute 0.1% methylene blue (40 cc normal saline and 10 cc of 0.5% methylene blue solution) is then injected into the knee joint. This technique varies from the technique described by Shaw et al. 13 as it allows for range of motion of the knee while the dilute methylene blue is in the joint. Methylene blue is known to stain bacterial biofilm. We have observed that this method provides a reliable and complete staining of all tissues in the effective joint space with minimal spill of dye outside of the effective joint space. After injection, the knee undergoes at least 1 min of flexion and extension to allow for intra-articular distribution of the staining dye. An arthrocentesis is performed under sterile conditions to aspirate as much dye as possible from the joint prior to arthrotomy, and then immediately after arthrotomy, suction is used to aspirate the remaining dye from the joint. This prevents overflow of dye to the surrounding tissues.
Following a standard medial parapatellar approach and capsulotomy, blue staining of all intra-articular surfaces is noted (Figure 1). Five soft tissue culture samples are obtained from different stained intra-articular areas for standard microbiological studies (aerobic, anaerobic, and fungal exams). The suprapatellar pouch and the patellar tendon are then freed of scar and adhesions, the knee is exposed, and the polyethylene insert is removed.
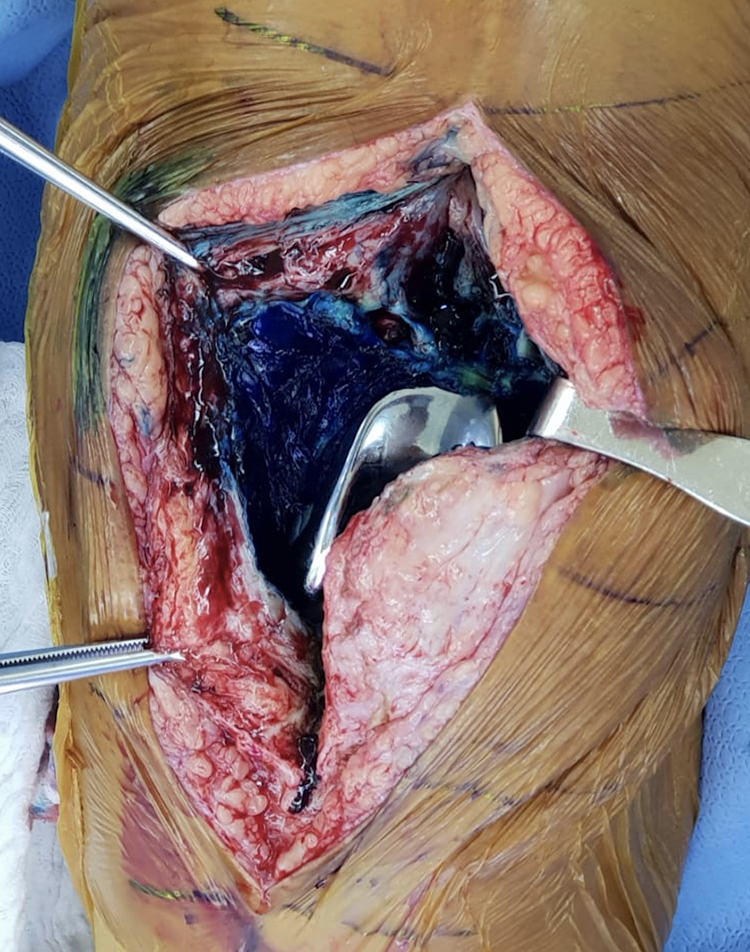
Left knee: Dyed intra-articular space.
After obtaining wide exposure, an aggressive and radical “tumor-like” synovectomy is performed including the synovial layer on the posterior capsule. The objective is to remove all stained soft tissue. These tissues had been in contact with the infected intra-articular space.
Argon beam
Next, the biofilm on retained surfaces is addressed by mechanical disruption with an argon beam coagulator, (ConMED, USA), as electrical stimulation has been shown to enhance detachment of biofilm from orthopedic implant surfaces. 14 The argon beam coagulator is set to 120 watts and had a probe that applied the beam in a painting brush-like fashion for all visible surfaces on the femoral and tibial components (Figure 2). This technique seems to work best on conductive metal surfaces, but more recently we have approached this step with caution as it is still unclear whether this part of the procedure can alter the surface of the metal. 15
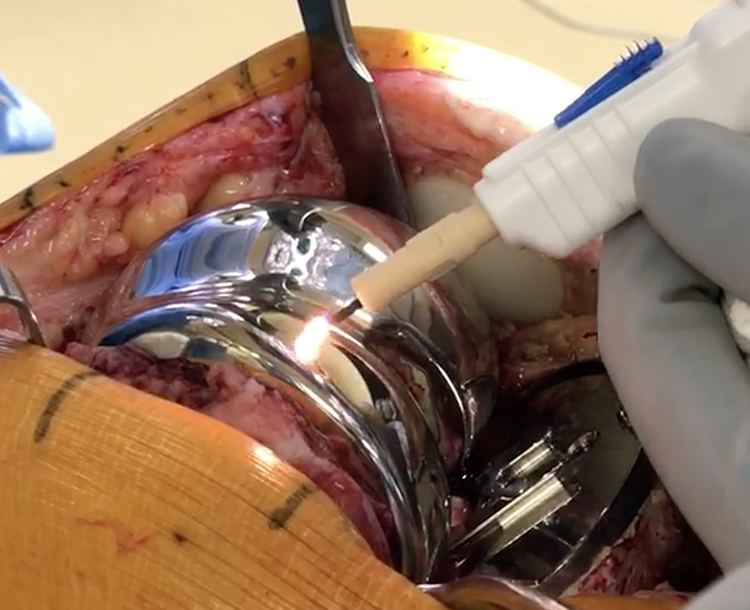
Argon bean application on the femoral component.
Chlorhexidine gluconate scrub
At this point, a 4% chlorhexadine gluconate-added brush is used to scrub all visible surfaces of the femoral, tibial, and patellar components: this is performed to mechanically remove biofilm as suggested by Tria et al. 16
Last, abundant pulse irrigation with 9 L of bacitracin-added saline is performed.
At this point, we place a povidone-iodine-soaked gauze within the wound and an antimicrobial incision drape is placed on the wound. The surgical team removes their used gowns and gloves and the back table with contaminated instruments is no longer used. The patient is then re-draped with clean drapes, the surgical team uses new gowns and gloves, and a new back table with new instruments is used. The gauze is removed from the wound. A further irrigation of the joint is undertaken using 1 L of bacitracin-added 0.9% sodium chloride prior to inserting the new, implant specific, polyethylene insert.
Calcium sulfate antibiotic-added beads application
Calcium sulfate antibiotic-impregnated beads are then prepared. A 10-mL kit of PG-CSH (Stimulan; Biocomposites Ltd, UK) is mixed with 1000 mg of vancomycin hydrochloride powder, 6 mL of a 40 mg/mL tobramycin solution, and a third antibiotic powder according to the preoperative antibiogram. A smooth paste is formed by mixing all components for 60 s and is pressed into 4.8-mm diameter hemispherical cavities in a flexible mold. 11 The beads harden and are ready for implantation after resting for at least 15 min. These calcium sulfate beads are a biocompatible and resorbable antibiotic-loaded intra-articular delivery system, which allow for a continuous local elution of the appropriate antibiotic. The hydrophilic crystalline structure is normally reabsorbed over 4–6 weeks, and their presence is visible on radiographs.
Ordinarily, the antibiotic beads are inserted in the suprapatellar pouch (Figure 3) and in proximity of the proximal tibia and distal femur to allow for a high concentration of antibiotics in the intra-articular space. After placing an intra-articular drain, the capsule is closed with Stratafix size-1 (Ethicon, Johnson & Johnson, Bridgewater, New Jersey, USA) suture, the subcutaneous tissue with 2-0 PDS suture, and the skin with staples.

Right knee: Calcium sulfate beads applied in the suprapatellar pouches at the end of the procedure.
All patients follow an identical, standard postoperative rehabilitation protocol, including weight-bearing as tolerated with crutches on the first postoperative day. Discharge from the hospital occurs when the patient achieves independence in activities of daily living, including walking 20 steps, climbing and descending stairs, and independent toileting.
Postoperative antibiotic treatment is routinely established in accordance with our institutional infectious disease service based on preoperative and intraoperative findings. A DAPRI procedure is usually followed by a 6-week course of intravenous antibiotic therapy: after this, another 6-week course of oral antibiotic therapy follows. The procedure is usually considered successful when clinical presentation and serologic tests (erythrocyte sedimentation rate, C-reactive protein, and D-dimer) normalize.
Results
The authors were able to report the initial outcome of 10 patients treated with DAPRI following a PJI in the knee joint. The original procedure was primary TKA in all patients.
Most patients undergoing DAPRI were male in our series (90%). The mean age of the patients was 69 years (range 63–92 years) and the mean BMI was 35 (min 30–max 48).
No patient was lost to follow-up at a minimum of 24 months (range 24–31 months): all the infections were classified as acute (within 6 weeks from the original surgery) or early hematogenous (within 7 days from clinical onset) infections with a known microorganism. All DAPRI procedures were performed on average 2 days after onset of symptoms (range 1–4 days). At the final follow-up, the procedure was considered a failure in 2 of 10 (20%) patients who underwent resection arthroplasty at 2 and 3 months, respectively, from the DAPRI procedure and a two-stage revision TKA afterward.
Most infections were caused by Staphylococcus aureus species (60%) and 20% of them were methicillin-resistant S. aureus (MRSA). The rest of the patients developed streptococcal infection (30%) and Granulicatella adiacens infection (10%). The procedures considered a failure after DAPRI were in two patients with MRSA infection. Overall infection could be controlled in eight patients, thus the success rate of infection eradication was 80%. The current data did not have sufficient power for statistical analysis.
Discussion
DAPRI augments the standard DAIR technique in several respects. Added interventions include intra-articular use of methylene blue to stain the intra-articular tissues, use of an argon beam coagulator as a biofilm disrupter, use of chlorhexidine gluconate brush as a biofilm remover, and use of calcium sulfate antibiotic-impregnated beads to prolong the intra-articular antibiotic concentration. 17 Combined, these techniques may lead to an increase in the overall success rate in implant-retention revision surgery.
This article presents a novel surgical technique DAPRI with the objective of improving the results of the standard DAIR procedure by allowing for a high and prolonged local antibiotic concentration using a calcium sulfate beads and eradicating the bacterial biofilm both on the intra-articular soft tissues and on the implant surfaces through the use of a multimodal approach. The goal of these added steps to DAIR is to disrupt the bacterial biofilm, which is the main culprit of antibiotic resistance and immune evasion.
Historically, the DAIR procedure showed a reasonable infection eradication rate between 50% and 80% when used in appropriately selected patients. Several factors have been associated with treatment failure: patient’s own immune deficiency and a high ASA score, MRSA, and Pseudomonas aeruginosa species, poor local tissues viability, the presence of rheumatic disease, delayed presentation from the original surgery (i.e. more than 4 weeks after TKA at the authors Institution), and erythrocyte sedimentation rate above 60 mm/h at presentation. 18,19 Success rates between 28% and 62% have been shown in a review article when DAIR is applied to chronic infections, as compared between 31% and 100% for acute infections. 20 Furthermore, DAIR has shown a higher success rate for acute postoperative infections when compared to a hematogenous spread in the late postoperative setting. 18,21,22 These reports highlight the importance of performing any implant retention technique in a timely fashion to achieve clinical success.
We believe that, in combination with timely intervention, our technique of targeted antibiotics mixed in calcium sulfate beads should provide a better outcome.
The calcium sulfate antibiotic-impregnated beads have the peculiar characteristic of being able to reach a prolonged and appropriate intra-articular minimal inhibitory concentration without reaching toxic systemic levels, even at their maximal local concentrations. 23 Furthermore, they are usually absorbed over 6 weeks from insertion, leaving no foreign body substrate (“nidus”) for successive bacteria adhesion. 23
Polymethylmethacrylate (PMMA) antibiotic-added beads have been historically used for local antibiotic delivery in the treatment of PJI, as shown by Buchholz and Engelbrecht. 24 However, the use of nonabsorbable PMMA beads has several limitations, including the need for a subsequent surgery to remove them from the articular space, and the risk of acting as a potential foreign body for bacterial colonization. Furthermore, when compared, to PMMA, calcium sulfate beads have showed a better “in vitro” elution profile 17 especially when cefazolin was used as a mixed antibiotic and a better “in vitro” inhibition of bacterial growth. 25 –28
The use of calcium sulfate beads is not free from complications. McPherson et al. 25 reported the presence of a copious exudate from the wound requiring surgical intervention in 3.2% of patients following the use of calcium sulfate beads to treat PJI. The formation of heterotopic ossifications is another complication reported in 1.2% of patients following calcium sulfate beads use.
Several studies have shown that the biofilm is the main culprit responsible for antibiotic resistance 29 in a PJI scenario. Biofilm is composed of an exopolysaccharide matrix produced by the microorganism when in contact with an implanted foreign material. It protects bacteria from harmful conditions in the host, sequesters in a nutrient-rich area, and provides an environment for the exchange of genetic material between cells. 29 Biofilm removal is mandatory for success with any implant retention procedure 30 : the current authors suggest the combination of three surgical techniques to identify, disrupt, and remove as much biofilm as possible. The current authors performed a methylene blue guided debridement technique, modified from Shaw et al. 13 : this approach allows the surgeon to adequately perform a “tumor-like” synovectomy, removing the proper amount of nonviable, infected tissue while avoiding healthy tissue. Another advantage of methylene blue is its antibacterial activity which might enhance the effectiveness of the DAPRI procedure itself. 31
The use of argon beam coagulation is well-described in the general and gynecologic surgery literature 32 but its use as an adjuvant in biofilm eradication is currently evolving. This device delivers unipolar electrical current of inert argon gas that may disrupt bacterial biofilm. The use of 4% chlorhexidine gluconate has been previously reported as effective to treat MRSA biofilm. 33 The current authors use the chlorhexidine gluconate brush on the femoral, tibial, and patellar component once the argon beam phase has been completed to mechanically remove the thermally disrupted biofilm: it must kept into consideration the potential cytotoxicity secondary to the use of chlorhexidine. 34
The DAPRI technique proposed in this article has several major limitations. First, inclusion criteria are very strict and the authors do not suggest applying this surgical approach outside of those criteria, as preoperative microorganism identification and accurate timing are fundamental. Second, this technique is the step-wise synthesis of several surgical techniques previously reported by different authors. Third, clinical outcomes are not reported here: the authors are following their consecutive series and intend to present their results at 2 years minimum follow-up.
Conclusion
The DAPRI is a standard DAIR technique augmented by the intra-articular use of methylene blue to stain biofilm, the use of the argon beam coagulator to burn and disrupt the biofilm, the chlorhexidine gluconate brush to further kill and remove biofilm, and calcium sulfate antibiotic-impregnated beads to prolong and elevate the intra-articular antibiotic concentration in the setting of TKA PJI.
We believe that the DAPRI technique might represent a reasonable treatment for acute and early hematogenous PJI. We expect that this approach will improve upon the DAIR success rate, although more studies are necessary to evaluate the clinical efficacy of this surgical procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study complies with the Declaration of Helsinki: however, no patient data are included in this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.