
Abstract
Background and objective:
Medical treatment and treatment goals for Crohn’s disease (CD) have evolved over the past 20 years. The aim of the study was to assess the cumulative risk of surgery in newly diagnosed CD patients in all age groups over this period.
Methods:
Recently diagnosed CD patients were retrieved from the registry of the Social Insurance Institution of Finland and data on surgeries from the Finnish Institute for Health and Welfare. The focus was on major intestinal surgery. Patients were stratified according to the year of diagnosis into three study periods: 2000–2006, 2007–2013, and 2014–2020.
Results:
We identified 11,329 recently diagnosed CD patients, of whom 1959 underwent surgery. The cumulative risks of surgery were 8.2%, 13.8%, and 18.7% at 1, 5, and 10 years post diagnosis, respectively. Surgical treatment was more frequent in male patients (IRR = 1.20, CI = 1.10–1.32). The pediatric group (age < 20 years) and the elderly (age ⩾ 60 years) had a higher risk of surgery (IRR = 1.24, CI = 1.10–1.39 and IRR = 1.20, CI = 1.07–1.34, respectively) compared to adults (aged 20–59 years at diagnosis). Adults had a lower risk of undergoing surgery in later periods than in the first period (IRR = 0.55, CI = 0.49–0.62). The pediatric group demonstrated reduction only in the last study period (IRR = 0.25, CI = 0.18–0.34). Elderly patients had a stable risk (IRR = 1.04, CI = 0.82–1.31) with 5-year risk increasing in the last period (IRR = 1.45, CI = 1.08–1.96).
Conclusions:
The risk of surgery among patients with newly diagnosed Crohn’s disease is declining. The risk was also decreasing in the pediatric population, whereas in the elderly it remained stable or increased.
Introduction
Crohn’s disease (CD) is a chronic immune-mediated inflammatory disease with a high risk of abdominal surgery. Historically, CD patients have had up to 90% risk of surgery in the 30 years after diagnosis. 1 The risk in children is reportedly at least as high as in adults and may reach 53% at 10 years. 2 However, the findings regarding surgical risk in the elderly are inconsistent: some studies report a lower risk than in younger patients, whereas others report a higher risk.3–7
Infliximab was the first biological treatment approved for CD in 1998. Subsequently, several biologics and small molecule agents with different modes of action have been proven beneficial in CD and numerous novel molecules are on the horizon. 8 Many studies report declining surgery rates associated with the use of biologics.9,10 On the other hand, there are reports of increased risk of needing surgery after 2010 in CD patients. 11 Our knowledge of the optimal use of biologics has grown over time. Furthermore, disease monitoring and treatment strategies have evolved, with contemporary studies supporting a top-down approach and early intervention to achieve remission.12–15
The aim of our study was to determine the cumulative risk of intestinal operation among recently diagnosed CD patients, including the pediatric population and the elderly. In addition, we aimed to study the trends in terms of calendar periods.
Methodology
Data source
All 5.6 million permanent residents of Finland are covered by the Social Insurance Institution of Finland (SII). SII provides special reimbursement for numerous medical conditions, including inflammatory bowel disease (IBD). 16 The two-step application procedure for the reimbursement and the excellent coverage and validity of the IBD reimbursement registry have been described elsewhere.17,18 We searched the SII registry with the International Classification of Diseases 10 codes K50.XX to find recently diagnosed CD patients between 1 January 2000 and 31 December 2020. Reimbursement for IBD is typically granted within a few weeks of diagnosis; therefore, we used the reimbursement date as a surrogate for the diagnosis date. Since CD may be diagnosed postoperatively following histological or other additional workup, we included reimbursements granted up to 12 months postoperatively, acknowledging that the reimbursement process may also require additional time.
The Finnish Institute for Health and Welfare (THL) as a national authority records data on surgeries from both the public and private health care sectors. We used the THL database to find operations performed on CD patients between 1 January 2000 and 11 December 2023. The procedures included were stricturoplasties and resections of any extent of the small or large intestine. Perianal procedures and second operations on stoma, such as stoma closure, were excluded. Specific codes of the NOMESCO Classification of Surgical Procedures used are listed in the Supplementary Data.
The Finnish Social and Health Data Permit Authority Findata (Findata) approved the study protocol. Patient characteristics from the SII on all diagnosed patients were analyzed anonymously as aggregate data. People with missing data or who denied permission to process their personal data under the European Union’s General Data Protection Regulation (GDPR) were excluded. Findata merged the SII and THL data and pseudonymized the records for surgically treated patients.
Stratification
We categorized patients into three groups according to the time of the diagnosis: 2000–2006, 2007–2013, and 2014–2020. During the period 2000–2006, infliximab was the only available biological medicine. The European Medicines Agency approved adalimumab for CD in 2007. Vedolizumab was approved in 2014, and ustekinumab followed in 2016. Hence, in 2007–2013 two tumor necrosis factor (TNF) inhibitors and in 2014–2020 multiple biologics were available for CD. However, pediatric indications for CD were accepted later; infliximab in 2007 and adalimumab in 2012.
Patients diagnosed in 2000–2017 were included in 5-year risk analyses and patients diagnosed in 2000–2012 in 10-year risk analyses. The subgroups were defined as pediatric (aged < 20), adults (aged 20–59), and the elderly (aged ⩾ 60) at the time of diagnosis. 19 The pediatric group included children and adolescents according to the definition of the World Health Organization. 20 We assumed complete follow-up of the cohort.
Statistical analysis
Medians with interquartile range (IQR) and percentages were presented in the descriptive data. Disease duration was defined as the time between the beginning of the CD reimbursement and the date of surgery. If the date of surgery was missing, the date of admission for surgery was used as a surrogate. Incidence rates were calculated by dividing surgically treated patients by patients diagnosed in the time period. Analyses were performed using IBM SPSS Statistics 26. We calculated incidence rate ratios (IRRs) using a generalized linear model assuming a Poisson distribution. The p-values < 0.05 were considered significant and 95% confidence intervals (CIs) were reported.
Results
After excluding patients with missing data (n = 46) and those who denied permission to process their data according to the GDPR (n = 6), we identified 11,329 CD patients. Of these, 2100 were operated on. We excluded 141 of these surgical cases due to an unconfirmed surgery indication or an excessively long interval between the initial surgery and reimbursement, leaving 1959 surgically treated cases for analysis (Table 1). The assumed follow-up times were 67,274 person-years (py) for patients diagnosed in 2000–2006, 49,054 py for 2007–2013, and 27,785 py for 2014–2020.
Patient characteristics.
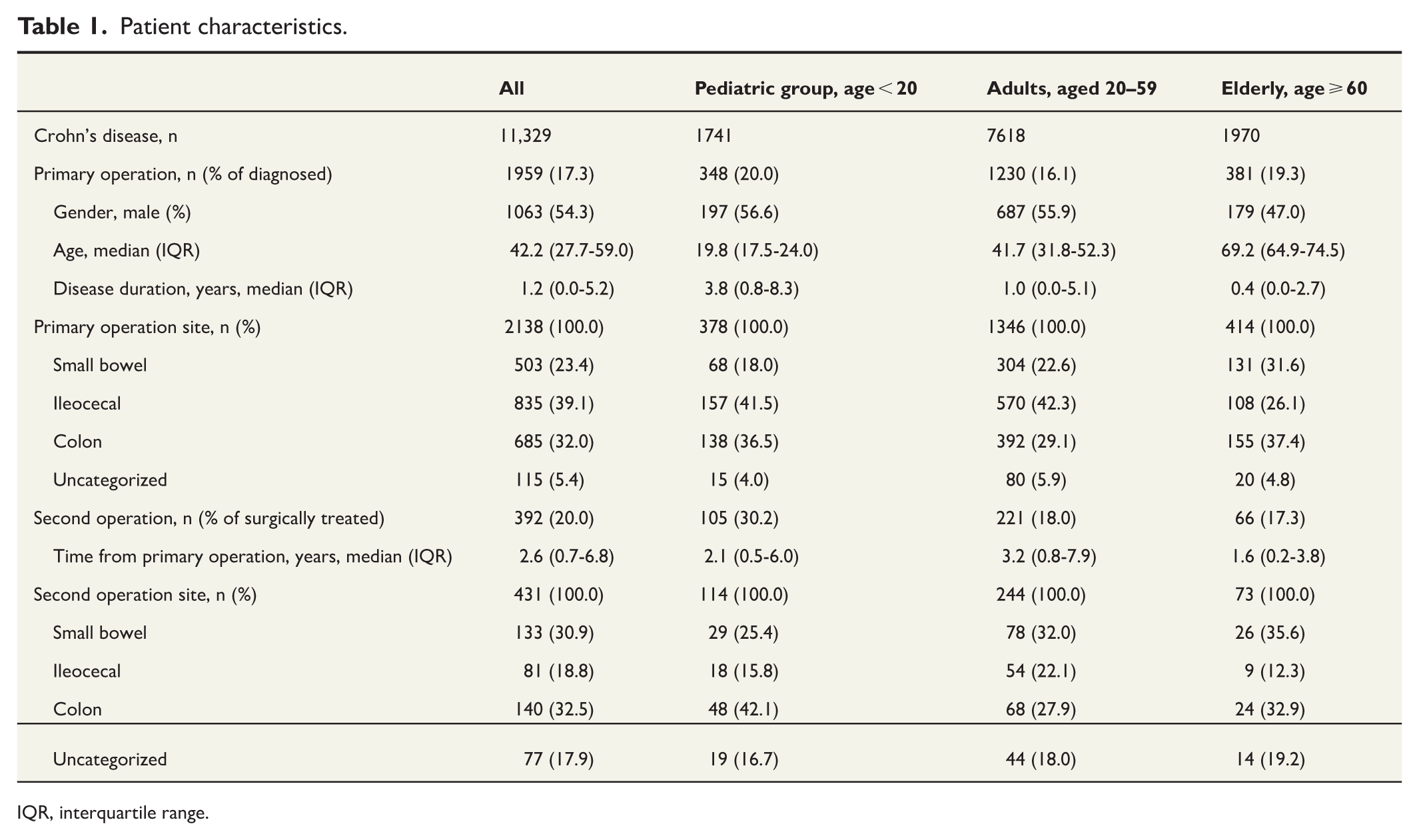
IQR, interquartile range.
Risk of surgery
The cumulative incidence of surgery was 8.2%, 13.8%, and 18.7% at 1, 5, and 10 years post diagnosis, respectively. The risks stratified by age groups are shown in Figure 1 and in the Supplementary Data.
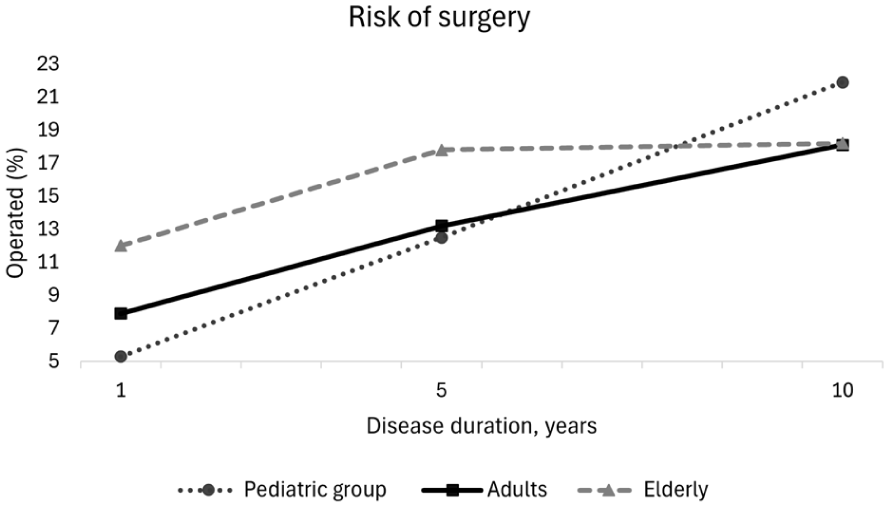
Risk of surgery by age.
The 1- and 5-year risks declined (IRR = 0.97, CI = 0.96–0.98 and IRR = 0.98, CI = 0.97–0.99), yet the 10-year risk remained constant (IRR = 0.99, CI = 0.98–1.01). Men had a higher risk of surgery (IRR = 1.20, CI = 1.10–1.32), and this elevation was evident at all time points. The most common surgery type was ileocecal resection, as shown in Table 1.
The subgroups
The pediatric group and the elderly had a higher risk of surgery (IRR = 1.24, CI = 1.10–1.39 and IRR 1.20, CI = 1.07–1.34 respectively) compared to the adults. Their cumulative risks were 5.3%, 12.5%, and 21.9% among the pediatric and 12.0%, 17.8%, and 18.2% among the elderly patients 1, 5, and 10 years after diagnosis, respectively. Consistent with the overall cohort, the 1- and 5-year risks of surgery in the pediatric group declined (IRR = 0.96, CI = 0.93–0.99 and IRR = 0.967, CI = 0.940–0.995, respectively), whereas the 10-year risk remained stable (IRR = 0.99, CI = 0.95–1.02). Conversely, in the elderly the 1- and 10-year risks of surgery were unchanged (IRR = 1.00, CI = 0.98–1.02, and IRR = 1.03, CI = 0.99–1.07, respectively), while the 5-year incidence rose (IRR = 1.028, CI = 1.004–1.052). The adolescents (aged 10–19, n = 323) had a higher risk of surgery than small children (aged < 10, n = 25) (IRR = 1.74, CI = 1.16–2.62).
Comparison of study periods
In the overall study population, the 1-year incidences of surgery were lower in 2007–2013 (IRR = 0.82, CI = 0.70–0.95) and in 2014–2020 (IRR = 0.65, CI = 0.55–0.76) than in the first period. The 5-year incidence was lower only in the latest period 2014–2020 (IRR = 0.76, CI = 0.66–0.88 versus IRR = 0.89, CI = 0.79–1.01 in 2007–2013). The 10-year incidences in the first and second periods were equal (IRR = 0.90, CI = 0.80–1.01). The relative subgroup risks are presented in Table 2 and the absolute risks in Figure 2.
Relative risk of surgery.
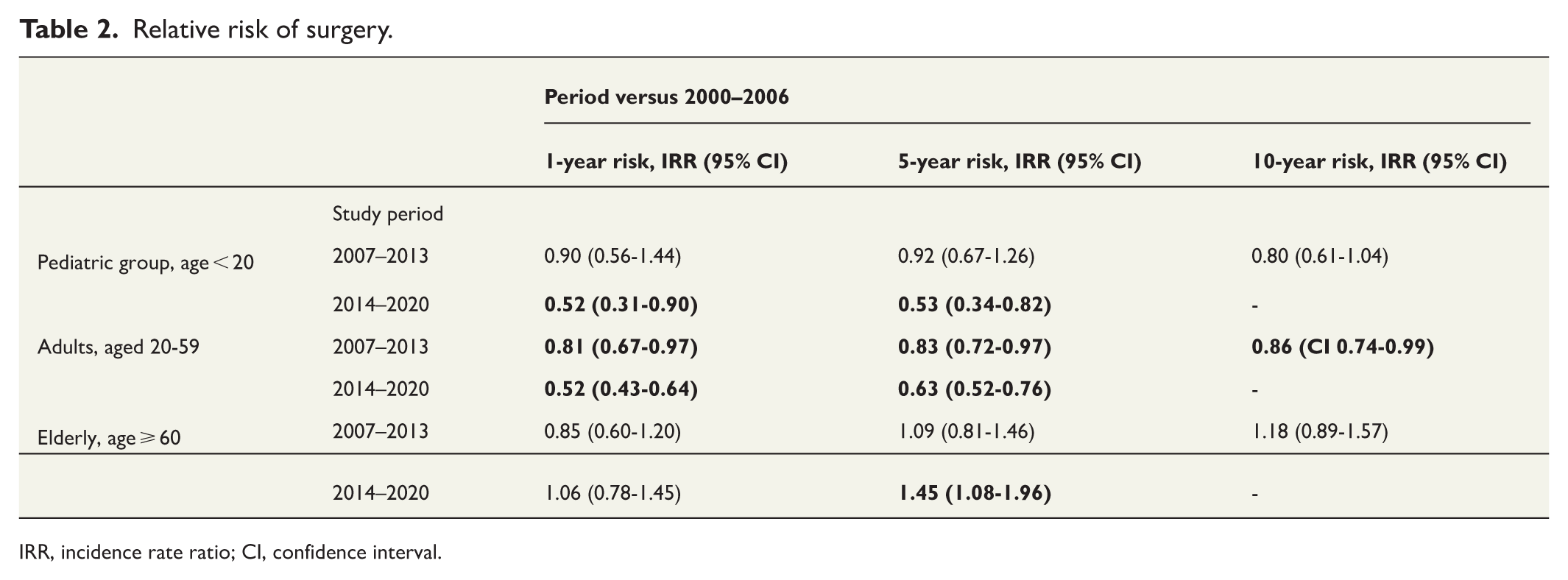
IRR, incidence rate ratio; CI, confidence interval.
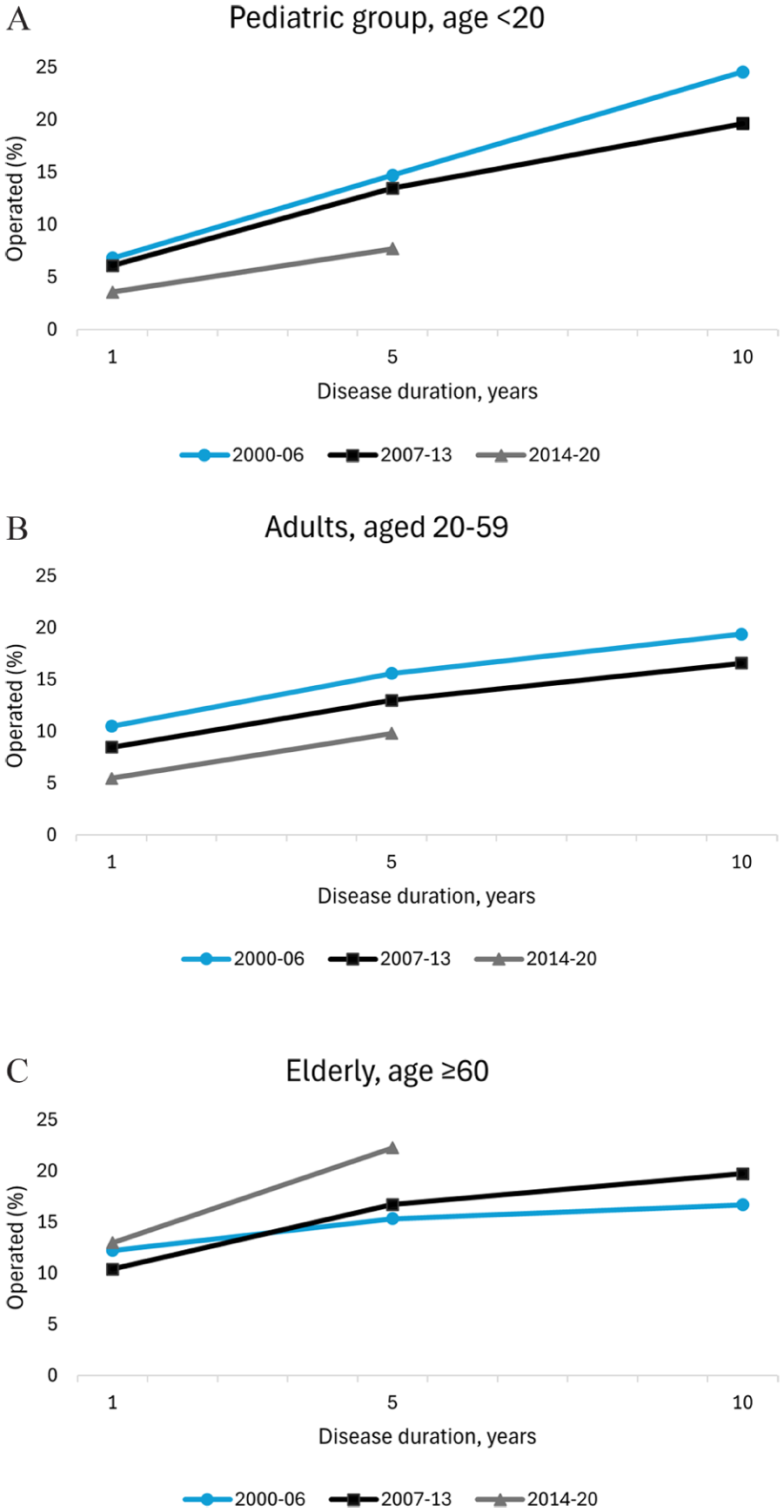
Risk of surgery stratified by period of diagnosis: (a) the pediatric group, (b) adults, and (c) the elderly.
Re-resections
A second operation was performed on 392 patients (20.0%), and 88 (4.5%) patients of those operated on had three or more abdominal operations. Details on the re-resections are presented in Table 1. The respective re-resection rates were 6.3%, 13.3%, and 17.3% at 1, 5, and 10 years after the primary operation. The pediatric group had a higher risk of re-resection (IRR = 1.68, CI = 1.33–2.12) than did the adults, with cumulative re-resection risk of 10.4%, 22.3%, and 31.5%, respectively. The risk of the elderly was similar (IRR = 0.96, CI = 0.73–1.27) to that of the adults and their respective re-resection risks were 6.4%, 14.3%, and 16.4%. Over the study period there were no statistically significant changes in 1-, 5-, and 10-year risks of re-resection in any of the subgroups nor in the overall cohort (Supplementary Data).
Discussion
Our study demonstrated respective 8%, 14%, and 19% cumulative risk of surgery at 1, 5, and 10 years after CD diagnosis. Moreover, the pediatric group and the elderly had a higher incidence of surgery, with the respective cumulative risks of 5%, 13%, and 22% in the pediatric group and 12%, 18%, and 18% in the elderly group. Over time, the risk of surgery declined overall, except among the elderly, for whom it remained constant or even rose.
A vast meta-analysis reported respective risks of surgery of 12%, 18%, and 26% after 1, 5, and 10 years of disease duration in 21st-century cohorts. A European multicenter study showed a surgery risk of 22% at 5 years post diagnosis. 21 The risks in pediatric-onset CD patients were 9%, 16%, and 44%, respectively. 22 A meta-analysis of elderly-onset CD patients reveals rates of surgery similar to those of the adults, with a 5-year risk of 22%. 23 However, a more recent Danish study showed elderly-onset patients to have a higher risk of surgery both 1 and 5 years post diagnosis compared to that among adult-onset patients. 6
The declining surgery rates in CD during the last two decades may result from several improvements. First, the decline is often associated with biological medication.9,10,24 Second, a meta-analysis suggests early introduction of biologics reduces the risk of surgery compared to late treatment. 14 However, a Nordic analysis reported stable surgery rates although the use of biologics had increased in the same period. 25 Third, several nonpharmacologic factors play a role in the outcome. In this millennium, the availability of many new technologies, such as magnetic resonance enterography, capsule endoscopy, and intestinal ultrasound, has led to earlier disease detection and improved follow-up schemas. Simultaneously, STIRDE-I in 2015 suggested treating to target, and the benefits of tighter inflammation control were established in the CALM study 2017.12,26 Still, in the LIR!C follow-up study of patients with luminal ileocecal CD randomized to laparoscopic ileocecal resection or infliximab, there was no difference between the groups in the duration of effect or in the need for additional therapy after the initial intervention. 27
Half of pediatric CD patients end up having anti-TNF treatment within 5 years of the diagnosis, which also seems to reduce surgery rates in children. 28 Our declines in pediatric surgery risks were most apparent in the last study period 2014–2020, when both infliximab and adalimumab were available and their use established in practice. Conversely, elderly CD patients start on biologics much less than do younger patients, although their perseverance in taking these drugs is reportedly similar.5,6 CD patients diagnosed in Denmark had an age-dependent frequency in the use of biologics. Within 5 years of diagnosis, biologic exposure was 39% in pediatric-onset patients, 15%–27% in adults, and 8% in elderly-onset patients. 29 The reason for this is unknown, but milder disease course, fear of side effects, comorbidities, and frailty of the elderly have been suggested. Lower biologics use, together with comorbidities that complicate management, may explain their higher surgery rates.
In Denmark, respective re-resection figures were 3%, 22%, and 32% at 1, 5, and 10 years, while a meta-analysis reported 5- and 10-year risks of 15% and 26%.22,30 A Finnish single-center cohort with 4.7 years of follow-up had a 19% reoperation rate. 31 The cumulative risks of re-resection in pediatric-onset CD was 21% at 5 years and 34% at 10 years post-diagnosis, which are comparable to our estimates. 22 Our findings are also in concordance with Swedish results indicating that the risk of re-resection has not declined since 2000 despite the increasing use of biologics. 32
The strengths of this study are its population-based study setting, the good coverage of the CD patients in the SII reimbursement registry, and the compulsory reporting to THL. The databases are also the greatest limitation. Finland unfortunately lacks a national IBD registry. Due to this, our clinical data are limited, and we are unable to correlate biologics use with surgical rates at the national level. In addition, a small subset of CD patients may never have applied for reimbursement for outpatient medications and therefore may have been missed. Not censoring deaths from follow-up is also a limitation. Nonetheless, excluding deaths would not have affected the results, as the objective was to assess cumulative risk rather than rates. 33
As CD may present with surgery-requiring complications, the effect of proactive therapy is limited. Optimized management may reduce later surgery, but the impact of emerging biologics and small molecules requires further research.
In conclusion, the risk of surgery is decreasing among newly diagnosed Finnish CD patients. The risk of surgery is also declining in pediatric patients, whereas in the elderly it is stable or even increasing.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969261423004 – Supplemental material for Crohn’s disease: Risk of surgery among newly diagnosed patients
Supplemental material, sj-docx-1-sjs-10.1177_14574969261423004 for Crohn’s disease: Risk of surgery among newly diagnosed patients by Kristi Kontola, Pia Oksanen, Heini Huhtala, Ilona Helavirta and Tuire Ilus in Scandinavian Journal of Surgery
Footnotes
Author contributions
All authors participated in the study design, review and editing, and approved the final version. K.K. conducted data management and K.K. and H.H. statistical analyses. K.K. wrote the original draft.
Data availability statement
No datasets available. Datasets can be regenerated by Findata in response to a justifiable application.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.K. has received personal fees from Pfizer, Tillotts Pharma, Celltrion Healthcare, Abbvie, Johnson & Johnson, and CSL Vifor; P.O. from Janssen-Cilag, Abbvie, Takeda, and Tillotts Pharma; I.H. from Abbvie and Medtronic; and T.I. from Celltrion Healthcare, Janssen-Cilag, Bristol Myers Squibb, Abbvie, Eli Lilly, Pfizer, and Takeda. P.O. is a board member of the Finnish Society of Internal Medicine. I.H. is a board member of the IBD subdivision of the Finnish Society of Gastroenterology and a consultant for the Nursing Research Foundation. T.I. is a national representative of ECCO, a board member of the Finnish Society of Gastroenterology and a member of the scientific advisory board of the Finnish Coeliac Society. H.H. has no conflict of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Wellbeing Services County of South Ostrobothnia (HYVAEP/1644/2025 to K.K.).
Ethical considerations
The use of data was permitted by Findata (Permission number THL/2099/14.02.00/2023). Personal pseudonymized patient data were accessible via a remote server to three researchers only. The subjects had the right to refuse permission to process their personal data. Clinical trial registration: N/A.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.