
Abstract
Children with vulvar swelling often present to multiple physicians and face a prolonged period of ambiguity and extraneous treatments. Here, we report a case of an 8-year-old girl who presented to the dermatology clinic with a 2-month history of vulvar swelling and was ultimately diagnosed with Crohn’s disease. Although extra-intestinal manifestations are common in inflammatory bowel diseases, they rarely present before an existing diagnosis. This report highlights this potential early manifestation and demonstrates how timely diagnosis leads to improved outcomes for patients, their families, and healthcare systems.
Introduction
Crohn’s disease (CD) is a chronic inflammatory condition of the gastrointestinal tract with relapsing and remitting symptoms. 1 In patients with CD, granulomatous lesions sometimes form in tissues distant to the gastrointestinal tract and this is referred to as metastatic CD. 2 Symptoms of metastatic CD are rare and can actually precede the classic symptoms of CD.3,4 When this occurs, pediatricians and sub-specialists are often faced with diagnostic dilemmas and patients consequently suffer from prolonged symptoms and extraneous treatments. 5 In this article, we report the case of a pediatric patient who presented to dermatology for vulvar swelling and was ultimately diagnosed with metastatic CD. We also provide a brief review of the literature on similar cases and discuss the importance of maintaining a high index of suspicion for this presentation.
Case report
An 8-year-old girl presented to the dermatology clinic with a 1-year history of lip swelling and a 2-month history of painless vulvar swelling. On physical examination, the patient’s upper and lower lips were edematous and scaly, with mild fissuring and crusted erosions (Figure 1). There was also some mild perioral desquamation. The examination of the genitals revealed bilaterally enlarged erythematous labia majora with a “peau d’orange” texture in the absence of tenderness or discharge (Figure 2). In the perianal region, there were three erythematous anal tags that resembled hemorrhoids.

Lip swelling at presentation.

Genital swelling at presentation.
The patient’s medical history was significant for eczema and a brief period of anemia at 4 years of age. It was also discovered that the patient had transient episodes of abdominal pain and bloody stools in the past that were not extensively investigated. One month before presentation, the child had been seen in emergency department for an episode of pseudo-appendicitis that resolved spontaneously. In addition, the patient’s maternal grandmother was known to have ulcerative colitis. Despite there being no change in the patient’s appetite or growth, CD with extragenital manifestations was suspected. A 4 mm punch skin biopsy of the vulva was performed under deep sedation to minimize discomfort and stress for the young patient. Histopathology demonstrated non-caseating dermal granulomas with giant cells, neutrophilic exocytosis, and epidermal erosions, consistent with a diagnosis of metastatic CD. Upon formal workup by gastroenterology, the diagnosis of CD was confirmed, and the patient was started on infliximab (Remicade) weeks following her presentation to dermatology.
Concurrent with the gastroenterology workup and management, topical therapy was initiated to treat the vulvar manifestations. Clobetasol propionate 0.05% ointment was prescribed twice daily for 2 weeks which lead to a partial improvement of the vulvar skin findings while the patient was still being investigated by gastroenterology and did not have systemic treatment yet. Afterward, alternating 1-week courses of daily clobetasol with daily tacrolimus 0.1% ointment led to a significant improvement of the vulvar swelling after 4 months. At this point, the patient transitioned to topical tacrolimus daily as maintenance alone and the clobetasol ointment was instructed to be used on an as-needed basis. The patient still presented with some swelling of her lips, which would worsen as time passed after her infliximab infusions. Methotrexate was added at this time by her gastroenterologist as it is indicated to prevent the development of antibodies against infliximab. 6
The patient was reassessed 6 months later. Her gastrointestinal symptoms were completely controlled on high dose (13 mg/kg) infliximab infusion every 6 weeks and methotrexate 7.5 mg weekly. The family also reported that the lips and genital swelling had completely subsided. They had not needed to use clobetasol since their last appointment and had elected to discontinue the tacrolimus ointment considering her lack of cutaneous signs or symptoms of the disease.
Discussion
Our case is among the few existing cases describing vulvar swelling as an early manifestation of CD in the pediatric literature. This presentation is thought to be caused by granulomatous inflammation within the vulva or by granulomas obstructing lymph vessels causing lymphedema. 7
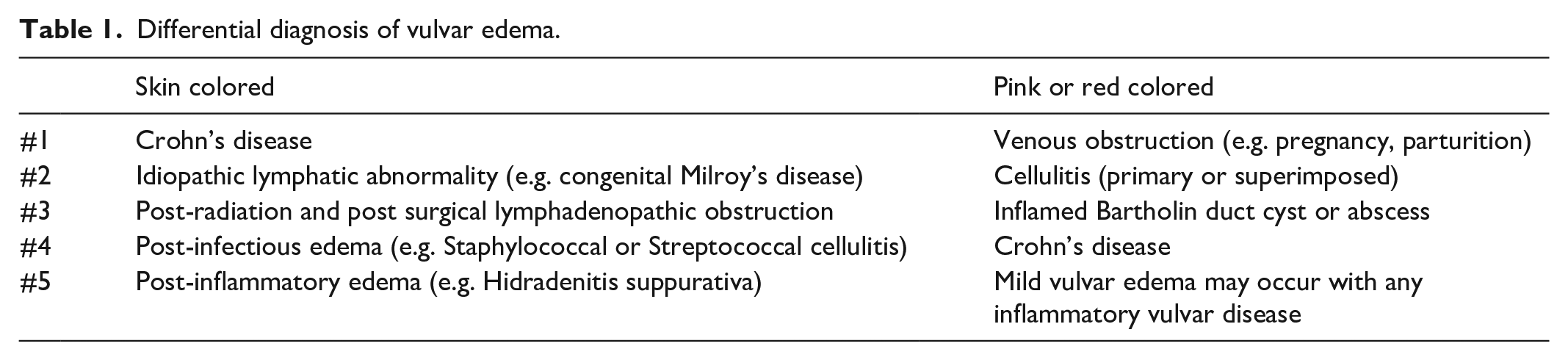
In a Medline search of the English literature, we identified 22 studies with similar presentations (Supplemental Appendix 1). The patients were between ages 3 and 15. Symptoms were present for up to 5 years before being diagnosed with CD. In the interim, they were frequently misdiagnosed and extraneously treated. The most common attributed diagnosis was cellulitis and most of the patients were prescribed courses of empiric antibiotics. Other diagnoses included sexual abuse and Bartholin’s cysts.8,9 Vulvar swelling has been described as a symptom that can involve a high number of consulting services such as primary care, gynecology, urology, dermatology, and gastroenterology. 5 Although multiple case reports have been published on this topic since 1970, the diagnosis of CD is still often missed. Particularly striking was the number of cases where child abuse was suspected. We suspect that the reason for the delay in diagnosis is related to the fact that vulvar edema as a presenting complaint appears to be relatively underrepresented in textbooks and medical literature as a whole. Crohn’s disease did not figure in the main differential diagnosis of major dermatology textbooks we consulted. However, when consulting a specific vulvar pathology textbook, 10 the main differential of vulvar edema can be divided in two categories as per Lynch et al. (Table 1). 11 It is important to note that sexual abuse does not figure in either of theses lists. Removing sexual abuse from the differential of vulvar swelling may avoid precipitating such significant psychological stress for children and their families. Moreover, CD is present on both lists, number 1 and number 4, respectively. Increasing the awareness that CD is the major and almost sole consideration in the pediatric patient without any risk factor for the other conditions that are part of the differential diagnosis of vulvar swelling is essential.
Differential diagnosis of vulvar edema.
Prompt diagnosis of CD is also beneficial as this disease leads to progressive bowel damage and disability. 1 In addition, cases exist in the literature of patients suffering from sporadic gastrointestinal symptoms for prolonged periods of time before diagnosis of the underlying inflammatory bowel disease is made. 5 In increasingly burdened healthcare systems, diagnosing inflammatory bowel diseases when the patient is younger also results in significant cost savings and decreased resource utilization. 12
Another takeaway, we would like to reinforce is the concept that there can be a delay in the response of vulvar symptoms to systemic therapy. Concomitant skin-directed therapy is thus warranted. In this case, genital CD responded rapidly to topical therapy with a potent corticosteroid while the patient was being investigated for possible CD and systemic treatment had not yet been initiated. Success using topical therapy for metastatic Crohn’s disease has been previously reported as well. 13 To reduce the risk of side effects of long-term corticosteroid use in the genital area, topical tacrolimus was used for its steroid sparing effect. We feel this treatment combination of skin-directed treatments were contributors to the improvement of the vulvar symptoms while the systemic treatments were taking effect in the deeper dermis. These treatments were well tolerated by the patient and she did not present any significant side effects to them. We suggest this combination treatment be employed in similar cases while awaiting onset of action of the systemic therapy.
Conclusion
CD should be included in the differential diagnosis, when young patients present with vulvar swelling. The timely diagnosis of metastatic CD can lead to quicker relief of symptoms, less extraneous investigations, and improved efficiency for healthcare systems. Furthermore, we feel the activity of the genital and labial CD can be used as an indirect marker of bowel inflammation allowing physicians to adjust systemic therapy. Topical therapy of the extra-digestive CD can be used to rapidly improve symptoms during the lag time between the initiation of the systemic treatments and their effect.
Supplemental Material
sj-pdf-1-sco-10.1177_2050313X211008627 – Supplemental material for Vulvar swelling and the timely diagnosis of Crohn’s disease: A case report
Supplemental material, sj-pdf-1-sco-10.1177_2050313X211008627 for Vulvar swelling and the timely diagnosis of Crohn’s disease: A case report by Arieh Gomolin, Hanieh Zargham, Ana Maria Sant’Anna and Audrey Lovett in SAGE Open Medical Case Reports
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent statement
Patient consent was obtained in writing for the publication of case details and photographs.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.