
Abstract
Purposes:
Over 80% of patients with primary ileocolic Crohn’s disease have a surgical resection within 10 years of diagnosis, and 40%–50% of them need further surgery within 15 years. Laparoscopic surgery can be challenging due to a thickened mesentery and the potential for fistulas, abscesses, and phlegmons. Aim of this study is to analyze the short-term outcomes of laparoscopic redo ileocolic resections for Crohn’s disease in patients with previous multiple laparotomies.
Methods:
All patients undergoing laparoscopic surgery for ileocolic Crohn’s disease from March 2006 to February 2017 were prospectively evaluated. Short term outcomes of laparoscopic ileocolic resection were compared between patients with previous multiple major surgeries and recurrent Crohn’s disease, and patients undergoing surgery for the first presentation of Crohn’s disease and no history of previous surgery. Conversion rate and 30-day morbidity were the primary outcomes. Reoperations, readmissions, operating time and length of stay were the secondary outcomes.
Results:
29 patients with recurrent Crohn’s disease and previous multiple laparotomies were included: the number of laparotomies these patients previously underwent was 2 in 19 cases (65.5%), 3 in 9 (31%), and 4 in 1 (3.5%). In total, 90 patients with no history of any previous abdominal surgery, who underwent laparoscopic ileocecal resection for Crohn’s disease, represented the control group. No differences were found in morbidity and conversion rate. Operating time was longer in patients with history of previous abdominal surgery.
Conclusion:
Laparoscopic redo ileocolic resection for Crohn’s disease is feasible and safe in patients with previous multiple laparotomies at the expense of longer operating time.
Introduction
Despite many advances in the medical management of Crohn’s disease (CD), there is still a significant risk of surgical resection for failure of medical management or complications during the lifetime of a patient (1).
Although the patterns of disease within the gastrointestinal tract are varied, the most commonly affected areas are the terminal ileum and cecum (55%). Other areas include small bowel disease only (11%–48%), colon disease only (19%–51%), and combined small and large intestine (26%–48%) (2).
Over 80% of patients diagnosed with primary ileocolic CD, who are typically young adults, have a surgical resection within 10 years of their diagnosis (3). Of these, 30%–50% will have symptomatic recurrence of disease during the first 5 years and 50%–80% by 10 years after surgery (4). Approximately, 40%–50% of patients undergoing surgery for CD are likely to need further operations within 10–15 years (5).
The advent of laparoscopic surgery has dramatically changed the landscape of colorectal surgery for both benign and malignant disease. When compared with traditional open surgery, laparoscopy offers well-described benefits (6) such as decreased pain, lower wound complication rates, improved pulmonary function, earlier resumption of diet and bowel function, better cosmesis, and shorter hospital stays (7). However, widespread use of laparoscopy in inflammatory bowel disease has been more limited due to technical constraints: the inflammation encountered in CD is often multifocal and makes a minimally invasive approach challenging due to a thickened mesentery, as well as the potential for fistulas, abscesses, and large phlegmons (8, 9); moreover, the lack of tactile feedback potentially limits the identification of occult disease.
As a consequence, a substantial number of patients with complicated CD have been traditionally denied an initial laparoscopic approach until recently. Similarly, the feasibility and safety of laparoscopy surgery for recurrent CD, particularly at the ileocolic anastomosis, has been debated: arguments for this approach include both the inherent technical challenge and the higher incidence of postoperative septic complications that can reach 50% in patients with multiple additive risk factors such as chronic steroid use, low albumin level, and presence of abscesses and fistulas (10). The aim of this prospective observational study is to analyze the short-term outcomes of laparoscopic redo ileocolic resections for CD in patients with previous multiple laparotomies, addressing the question on the feasibility of laparoscopic surgery in the hostile abdomen, which has traditionally been considered a relative contraindication to a minimally invasive approach.
Methods
Study Objectives
To compare the short-term outcomes of laparoscopic ileocolic resection in (1) patients with recurrent CD of the distal ileum and previous multiple laparotomies (MPL—group A) versus (2) patients with first presentation of ileocolic CD and no previous abdominal surgery (NPS—group B).
Study Design
All patients undergoing laparoscopic surgery for ileocolic CD from 1 March 2006 to 28 February 2017 were included in this prospective observational study. All patients undergoing open, single-incision, robotic or hand-assisted surgery for ileocolic CD were excluded as were patients undergoing emergency operations.
In order to assess the feasibility of a laparoscopic approach even in complex recurrent CD, patients with previous multiple major surgeries were compared with patients undergoing surgery for CD for the first time and with no history of any previous abdominal operation.
Group A—MPL included patients with recurrent ileocolic CD and history of two or more previous laparotomies. A previous laparotomy was defined as an open surgical procedure which required a midline abdominal incision. Laparoscopic procedures such as appendectomies, cholecystectomies, and diagnostic laparoscopies were not counted as previous surgery as was an appendectomy performed via a McBurney incision or a cesarean section via a Pfannenstiel incision.
The MPL cases were compared to a control group represented by all patients who underwent surgery for first presentation of ileocolic CD and no history of any previous abdominal surgery (group B—NPS). Strict criteria were decided for inclusion in the control group, and patients were excluded even if they only had minor laparoscopic procedures, such a diagnostic laparoscopy or a laparoscopic appendectomy.
The indication for surgical resection was discussed at a dedicated inflammatory bowel disease (IBD) multidisciplinary team (MDT) meeting involving gastroenterologists, colorectal surgeons, radiologists, and pathologists. Preoperative assessment included colonoscopy, magnetic resonance imaging (MRI) enterography, and intestinal ultrasound.
Data Collection
Preoperative, operative, and postoperative data were prospectively recorded for each patient in both groups. Preoperative parameters included age, sex, body mass index (BMI), comorbidities, American Society of Anesthesiologists (ASA) status, albumin and hemoglobin concentration, smoking status, weight loss, indication for surgery, and preoperative medical therapy.
Operative data included duration of surgery, intra-operative complications, estimated operative blood loss, type of incision for specimen retrieval, conversion rate, reason for conversion, and use of temporary ileostomy. Postoperative data included length of hospital stay (LOS), time to tolerate oral fluids and oral diet, and time to resolution of ileus and postoperative complications according to the Dindo–Clavien classification (11).
Primary and Secondary Outcomes
As we did not expect a difference in mortality, data on morbidity and feasibility of the laparoscopic approach have been the key outcome measures in the comparison. Conversion rate and 30-day morbidity were the primary outcomes.
The secondary outcomes were operating time, LOS, reoperations, and rehospitalization within 30 days and were recorded prospectively.
Surgical Technique
In reoperative surgery the sites of previous abdominal incisions are marked and the first trocar is inserted via an open Hassan technique away from the midline, alternatively an optical trocar access in the left upper quadrant may be utilised. The abdominal cavity is inspected and preliminary division of adhesions is often necessary and performed with cold sharp dissection. This is followed by a complete mobilization of the terminal ileum and right colon and hepatic flexure and mobilization of the small bowel mesentery up to the duodenum. The recurrence is usually at the ileocolic anastomosis and that area is approached last. Hepatic flexure and terminal ileum are mobilized first. Placing a 5-mm camera through the suprapubic port can usually give a very good view of the phlegmon and retroperitoneal structures allowing a safer dissection. When adequate mobilization has been obtained, the bowel is exteriorized through a 4- to 5-cm midline incision that may need to be extended to exteriorize larger terminal ileal phlegmons. This provides excellent exposure of the usually thickened mesentery, which is systematically divided using an overlapping Kocher clamp technique. In our experience vessel, sealing devices are not adequate to control the large blood vessels of the friable mesentery of patients with CD; therefore, we routinely use transfixion sutures. After bowel transection, a side-to-side ileocolic anastomosis is usually fashioned and the bowel is pushed back into the abdominal cavity. The staple lines are routinely over sewn.
We consider the procedure to be “converted” when the abdominal incision is used for any lateral or medial mobilization of the right colon or terminal ileum. Patients receive a single dose of prophylactic antibiotics and are routinely enrolled in an enhanced recovery pathway after surgery.
Definitions
Steroid use was defined as corticosteroids administered within 1 month prior to surgery, while immunosuppressive use was defined as azathioprine or 6-mercaptopurine used within 2 weeks prior to surgery. Anti-Tumor Necrosis Factor (TNF) monoclonal antibody use was defined as the last infusion of infliximab 4 weeks prior to surgery. Active smoking status was defined as smoking within 4 weeks before surgery, and weight loss was defined as more than 5 kg in the previous 6 months. Duration of the operation was defined as time from skin incision to wound closure.
Mortality was defined as death occurring in the hospital or within 30 days from discharge, while postoperative morbidity was defined as complications occurring in the hospital or within 30 days after surgery.
Statistical Analysis
Categorical variables are presented as frequency or percentage and were compared with the use of the chi-square test or Fisher’s exact test, as appropriate. Continuous variables are presented as mean (±standard deviation) or median (range) and were compared with the use of Student’s t-test. The Mann–Whitney U test was used for continuous, not normally distributed outcomes.
To test the presence of potential confounding factors, we analyzed the impact of the history of two or more previous multiple laparotomies (MPL vs NPS) on postoperative morbidity in multivariable logistic regression model, considering also age, sex, ASA grade, BMI, conversion, and operating time.
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS version 16.0; SPSS, Chicago, IL, USA). All reported p-values were two-tailed, and p-values of less than 0.05 were considered to indicate statistical significance.
Ethics
The study is conducted in accordance with the principles of the Declaration of Helsinki and “good clinical practice” guidelines. Informed consent has been obtained from the patients.
Results
Patient Characteristics
In total, 35 patients with history of two or more previous abdominal surgeries underwent laparoscopic ileocolic resection in the study period. Six patients were excluded because one of the two previous surgeries was represented by cesarean section in two cases, laparoscopic appendectomy in two cases, laparoscopic cholecystectomy in one case, and diagnostic laparoscopy in one case.
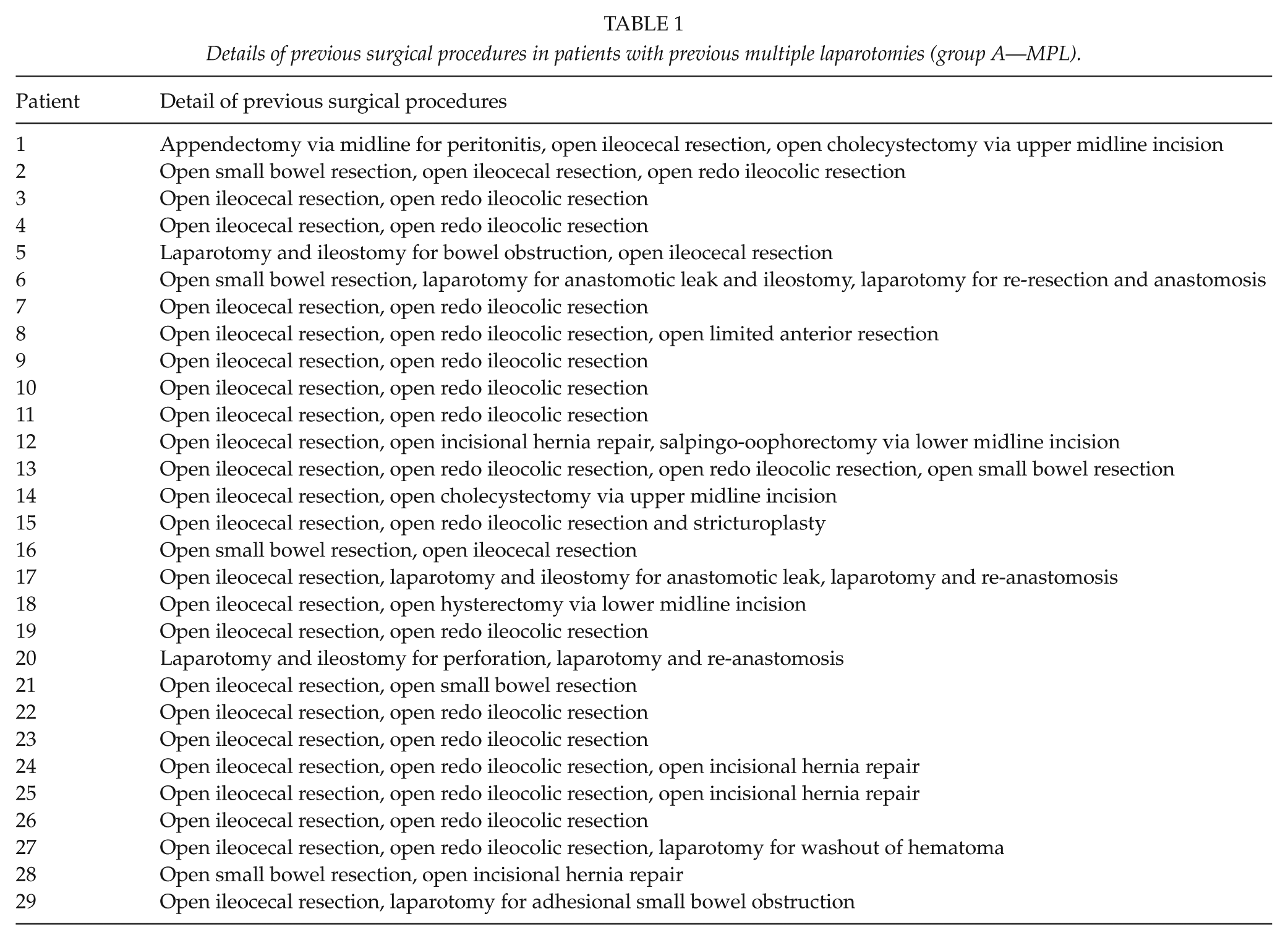
In total, 29 patients were finally included in the group A—MPL: the number of laparotomies these patients previously underwent was 2 in 19 cases (65.5%), 3 in 9 (31%), and 4 in 1 (3.5%) as detailed in Table 1.
Details of previous surgical procedures in patients with previous multiple laparotomies (group A—MPL).
In total, 90 patients with no history of any previous abdominal surgery underwent laparoscopic ileocecal resection for CD in the same study period, representing Group B—NPS.
Baseline patient characteristics are detailed in Table 2. We do not routinely perform ureteric stenting in redo surgery for CD: this was only planned in one patient in the MPL group after review of the imaging at the inflammatory bowel disease multidisciplinary meeting.
Patient characteristics.
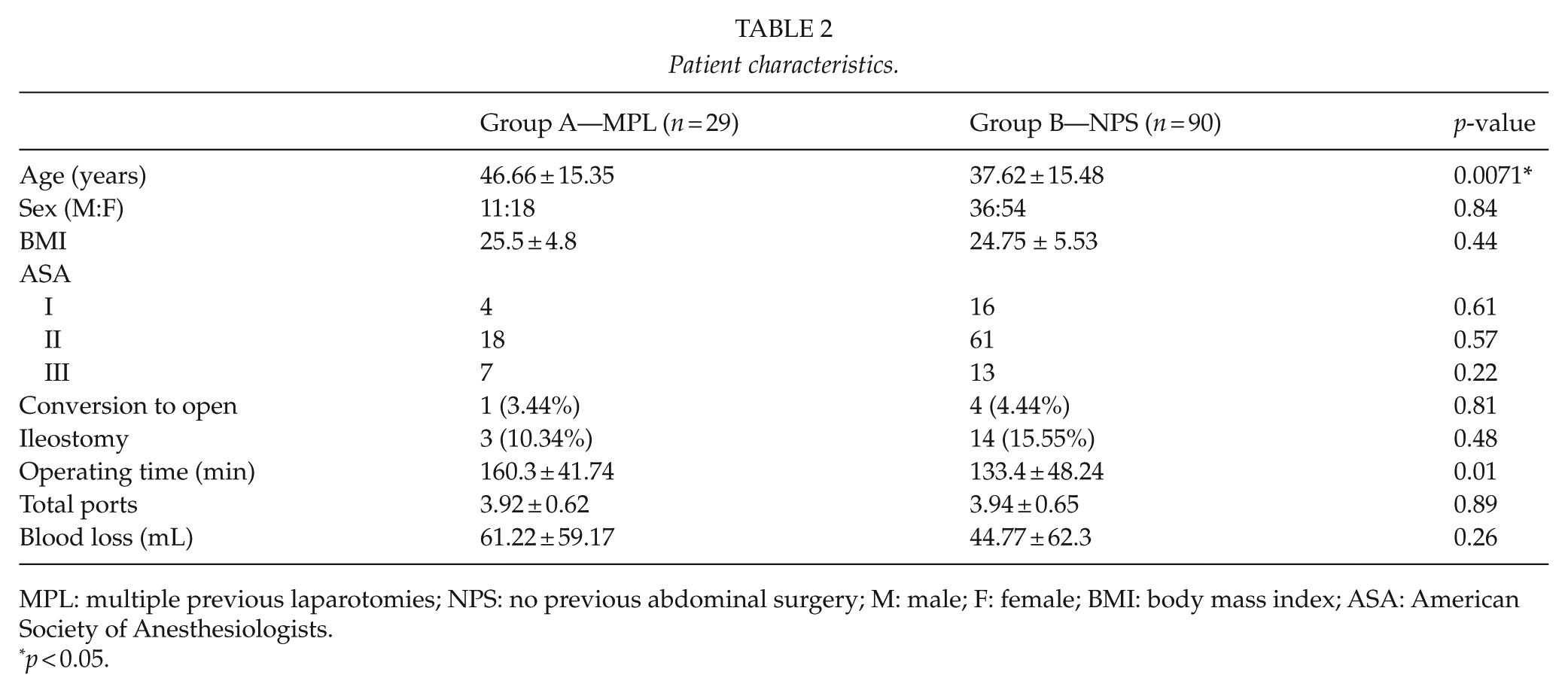
MPL: multiple previous laparotomies; NPS: no previous abdominal surgery; M: male; F: female; BMI: body mass index; ASA: American Society of Anesthesiologists.
p < 0.05.
Conversions to Open Surgery
There was one conversion to open surgery (3.44%) in the MPL group and four (4.44%) in the NPS group (p = 0.81). Reason for conversion in MPL was adhesions and suspected bowel injury, while the three conversions in the NPS group were justified by suspected bowel injury in one case and need to extend the extraction site to complete colonic mobilization in other two cases.
Morbidity and Mortality
No mortality was recorded. The 30-day morbidity is detailed in Table 3.
Postoperative outcomes.
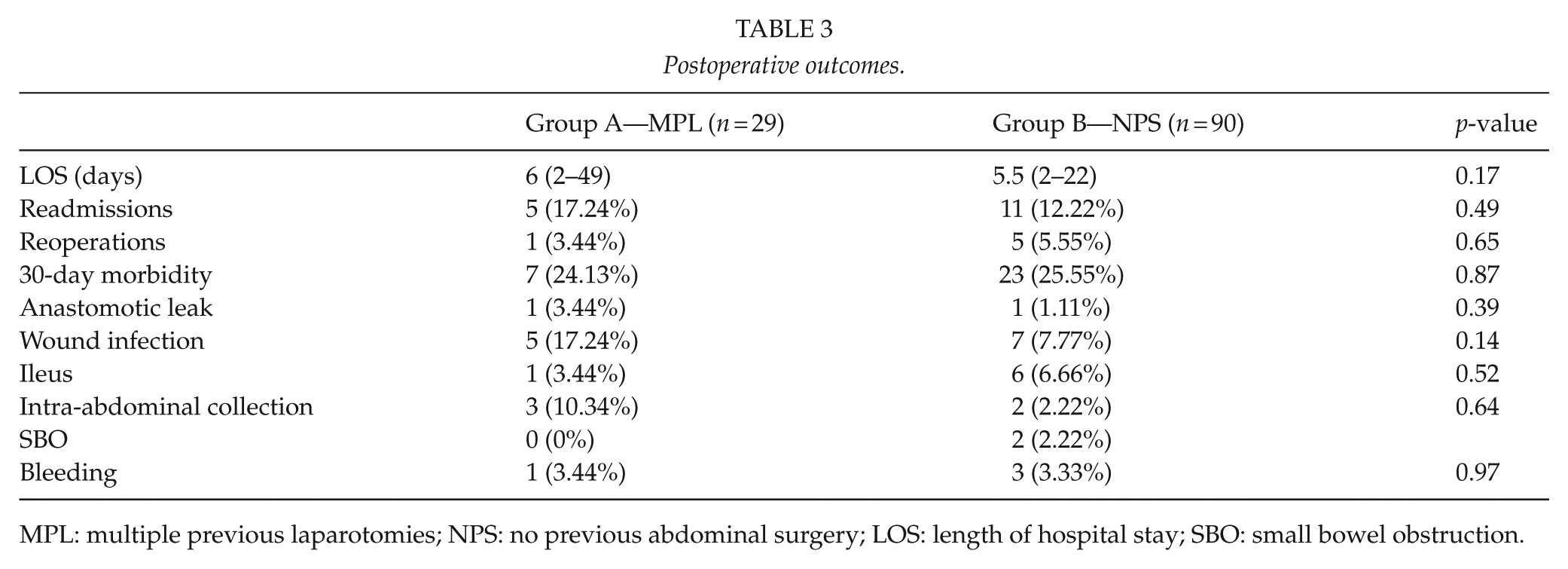
MPL: multiple previous laparotomies; NPS: no previous abdominal surgery; LOS: length of hospital stay; SBO: small bowel obstruction.
The 30-day morbidity was 24.1% and 25.5% in group MPL and NPS, respectively (p = 0.87). No differences were found in anastomotic leak, wound infection, and postoperative ileus between the two groups. One patient in MPL and three patients in NPS required postoperative blood transfusions.
In total, 11 complications were recorded in 7 patients in group MPL: 4, grade 1; 3, grade 2; and 4, grade 3 according to Dindo–Clavien classification. In total, 25 complications were recorded in NPS group: 9, grade 1; 10, grade 2; and 5, grade 3.
Readmissions and Reoperations
Within 30 days from hospital discharge five patients (17.24%) were readmitted in group MPL and 11 (12.22%) in group NPS, with no difference between the two groups. Reasons for readmission are detailed in Table 4.
Reasons for readmission within 30 days from hospital discharge.
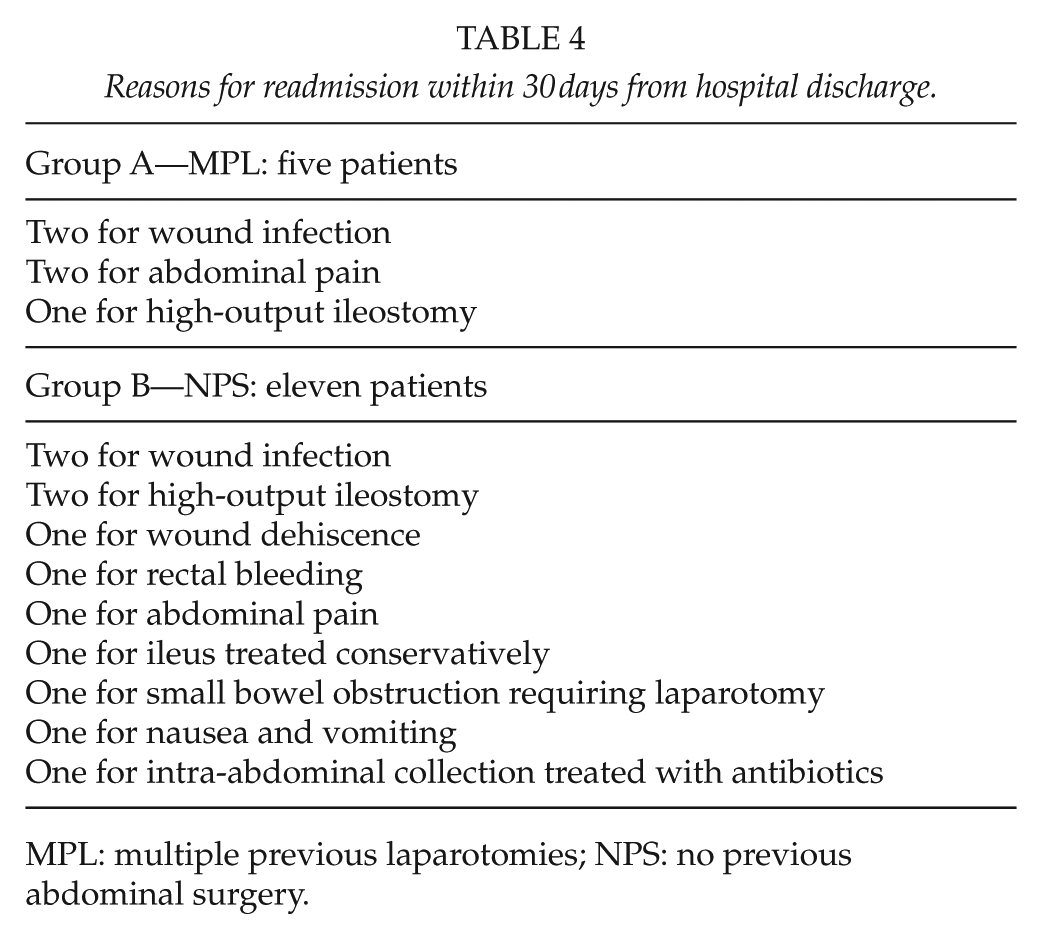
MPL: multiple previous laparotomies; NPS: no previous abdominal surgery.
Reoperations did not differ significantly between the two groups. One patient (3.44%) was reoperated in MPL and indication for surgery was anastomotic leak requiring laparotomy and ileostomy formation. Five patients (5.55%) were reoperated in NPS group, and indication was small bowel obstruction in two cases, bleeding in two cases, and anastomotic leak in one case.
Operating Time and Los
Operating time was 160.3 ± 41.74 min in MPL group and 133.4 ± 48.24 min in NPS (Fig. 1). As expected, operating time was slightly longer in the MPL group where adhesiolysis was often needed; however, this difference did not reach statistical significance (p = 0.01).
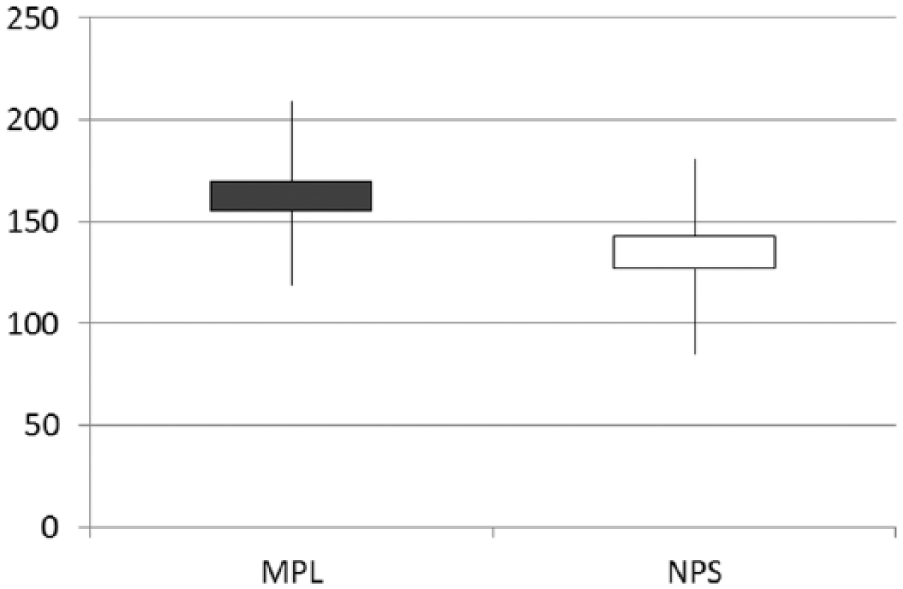
Mean operating time (min).
Patients in the MPL group spent on average half a day longer in hospital compared to the NPS group (6 and 5.5 days, respectively, p = 0.17).
Discussion
This study demonstrates that laparoscopic surgery is feasible even in the hostile abdomens of patients with recurrent CD and previous multiple laparotomies. Despite the benefits of laparoscopic surgery (12), a considerable number of CD patients may be a formidable challenge even for the most-experienced laparoscopic surgeon (13).
In addition, the surgeon has to be prepared to deal with unexpected findings that may require additional surgery. These include proximal strictures, fistulas, abscesses, or phlegmons, which can be identified in about 20% of patients (14). This is one of the reasons why these patients benefit particularly from MDT discussion, where not only the indication for surgery is discussed but also the surgical strategy, with careful review of the imaging to plan the surgical approach and the need for adjuncts such as ureteric stents.
Relatively high rates of mortality and septic complications have been reported in patients who undergo resections for CD, with a rate of intra-abdominal sepsis and anastomotic leak of 14% and 17%, respectively (10)
These challenges explain the concerns on feasibility and safety of the laparoscopic approach in redo ileocolic resection for CD; nevertheless, growing evidence is demonstrating a trend toward inclusion of difficult and complex laparoscopic colorectal cases in highly specialized units without compromising results (15, 16).
We routinely offer elective minimally invasive surgery to patients with recurrent ileocolic CD who failed medical therapy; however, this study pushes the boundaries of laparoscopic surgery in a highly selected group of patients with two or more previous laparotomies, in whom complex and technically challenging surgery is expected.
We found a conversion rate of 3.4%, in patients with two or more previous multiple laparotomies, which is significantly less compared to rates of 6.7%, 25%, and 32% of previously published series, where moderate to severe adhesions was the primary indication of conversion to open surgery (6, 17, 18). A standardized approach to adhesiolysis, with the first trocar inserted away from the previous midline scar, the use of a 5-mm camera that can easily be moved in different ports, and careful cold sharp dissection, may explain these results in our unit.
Not surprisingly, we found that redo ileocolic resection for CD in patients with previous multiple abdominal surgeries requires 30 min longer than patients who undergo surgery for the first time. However, it is important to note that this does not reflect in increased rate of complications, which was indeed not different in our study populations.
Our study found a slightly longer postoperative hospital stay in patients who underwent redo surgery. Despite being equally enrolled in an enhanced recovery program, patients with multiple previous abdominal surgeries spent an average of 6 days in hospital compared to 5.5 days of the primary resection group: this difference did not reach statistical significance, and a trend toward older patients with more comorbidities was noted in the redo surgery group.
As outlined in the review of previous studies, there is ample data to support the safety and feasibility of laparoscopic surgery in redo ileocolic resections for CD; however, our study has some limitations. First of all, as the group of patients with two or more multiple laparotomies is a highly selected one, we only enrolled 29 cases in our main intervention group and larger numbers are needed to provide more robust evidence. Nevertheless, no statistical differences were found in baseline patient characteristics between the two study groups. Moreover, the aim of our study was to assess the feasibility of the laparoscopic approach in the extreme setting of ileocolic resection in patients where severe adhesions are common, and technically challenging surgery is expected. Our study, therefore, wants to add new and different evidence to the already available literature on laparoscopic surgery for redo ileocolic resection, and this is manifested by the exclusion of minor laparoscopic procedures from the count of the previous surgeries.
Secondly, our patients have been recruited within a study period of 11 years, and concerns about cases being performed at different stages of the learning curve might be raised, particularly with relation to conversion to open surgery. A cumulative conversion rate of 3.87% (5 cases out of 119) was found in our study, and it is important to note that three of the five conversions happened in the last 3 years of the study period.
Finally, our study did not include an open surgery group, which would have allowed a comparison between the results of laparoscopic surgery and the most commonly alternative approach for redo ileocolic resection for CD. However, open surgery is now rarely offered in our minimally invasive unit in the elective setting, and due to widespread adoption of laparoscopic surgery, we expect that the only way of addressing this question is represented by a multicentre randomized controlled trial, which we are currently designing.
Conclusion
Laparoscopic redo ileocolic resection for CD is feasible and safe in specialized laparoscopic Units even in patients with previous multiple laparotomies, at the expense of longer operating time. Randomized controlled trials are needed to produce more robust evidence and compare with open surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.