
Abstract
Background:
Distal pancreatic resection is associated with a high frequency of postoperative complications. The aim of this study was to characterize the effect of diabetes mellitus (DM) on short-term complications after distal pancreatectomy.
Methods:
Patients who underwent distal pancreatectomy between 1 January 2010 and 31 December 2020 were identified from the Swedish National Pancreatic and Periampullary Cancer Registry, and the data were cross-linked with the National Diabetes Registry. The complication rates were compared between patients with and without diabetes.
Results:
In total, 1297 patients underwent distal pancreatectomy, and 247 (19%) of these patients had DM. Postoperative complications occurred in 697/1297 (54%) patients. There was no difference observed in the risk of overall complications (odds ratio (OR) = 0.76, 95% confidence interval [CI]: 0.58–1.00; p = 0.052), general surgical complications (p = 0.053), medical complications (p = 0.872), or postoperative pancreatic fistula rates (p = 0.603) according to the univariable analysis. In the multivariable analysis, patients with DM demonstrated a lower risk of overall complications (OR = 0.72, 95% CI = 0.54–0.96; p = 0.025). In the subgroup analysis, patients with high mean HbA1c levels (p = 0.041), high last measurement (p = 0.032), or DM duration >10 years (p = 0.022) exhibited lower risks of complications in the multivariable analysis.
Conclusion:
This study revealed a lower overall complication risk in patients with DM compared to patients without DM after distal pancreatectomy; however, no difference in the pancreatic fistula rate or medical complications was observed.
Keywords
Introduction
Distal pancreatic resection is a major surgical procedure with a high frequency of postoperative complications. 1 There is a complex interplay between surgically treated pancreatic diseases and diabetes mellitus (DM). DM is a well-known risk factor for postoperative complications in numerous types of surgical procedures, and DM is a common comorbidity observed in patients evaluated for pancreatic resection.2,3 However, DM has also been associated with the development of pancreatic fibrosis; therefore, it could be associated with a reduced risk of the most feared complication after pancreatic resection involving postoperative pancreatic fistula.4,5 Furthermore, obesity (which is more common in patients with DM) is associated with pancreatic steatosis and a soft pancreas, which may play a role in the pathogenesis of postoperative pancreatic fistula, thereby potentially increasing the risk of postoperative pancreatic fistula in obese patients with diabetes.6–10
Previous studies have reported conflicting results concerning the impact of DM on postoperative complications after pancreatic surgery, with some studies demonstrating that DM is associated with an increase in the complication rate.11,12 Conversely, other studies have reported a decreased risk of complications or no association whatsoever between the risk of complications and DM.13–16 Furthermore, metabolic syndrome (involving the combination of DM, hypertension, and obesity) has been associated with an increased risk of complications after pancreatic surgery. 17 Moreover, several studies have not specifically reported outcomes after distal pancreatectomy, and most studies have not reported data on antidiabetic treatments or glycemic control.
The aim of this study was to characterize the associations between preoperatively diagnosed DM and short-term outcomes after distal pancreatectomy, with a focus on diabetes as a risk factor for postoperative pancreatic fistula. Furthermore, a secondary aim was to examine whether glucose control, coexisting obesity, and duration of diabetes would alter the risk of complications.
Methods
Data source
The Swedish National Pancreatic and Periampullary Cancer Registry was founded in 2010 and included all patients diagnosed with pancreatic or periampullary cancer. Patients undergoing surgery due to benign or premalignant lesions are also included in the registry. The registry collects data on tumor characteristics, patient comorbidities, operative technical details, short- and long-term follow-ups, and oncological treatments. Surgeons are also prompted to enter data concerning the specific complications that the patient has experienced into the registry. Moreover, the registry coverage rate exceeds 90%. 18
The Swedish National Diabetes Register (NDR) was founded in 1996 and includes data obtained from visits regarding DM at primary care departments, as well as specialized endocrinology departments. The registry collects various types of patient data, including year of onset, type of diabetes, treatment, metabolic control (measured via HbA1c levels), blood pressure, and diabetic complications. The registry coverage in the NDR is close to 100%.
Study design
The design and reporting of this study were conducted in accordance with the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines for the reporting of observational studies. 19 Data on patients who underwent distal pancreatectomy between 1 January 2010 and 31 December 2020 were obtained from the pancreatic registry and were cross-linked with the Swedish NDR. Patients who had missing data on the occurrence of postoperative complications were excluded from the study (n = 78). Short-term glycemic control was assessed by using the HbA1c levels measured at the most recent visit for DM before surgery. Long-term glycemic control was assessed by calculating mean HbA1c levels for all of the visits entered into the Swedish NDR throughout the duration of DM until the last preoperative visit. Patients with DM were divided into quartiles according to their most recent HbA1c levels (quartile 1: < 47 mmol/mol/< 6.5% Diabetes control and complications trial (DCCT); quartile 2: 47–53 mmol/mol/6.5–7.0% DCCT; quartile 3: 54–63 mmol/mol/7.1–7.9% DCCT; and quartile 4: > 63 mmol/mol/7.9% DCCT), as well as their mean HbA1c levels (quartile 1: < 46.2 mmol/mol/< 6.4% DCCT; quartile 2: 46.2–53.2 mmol/mol/6.4–7.0% DCCT; quartile 3: 53.3–60 mmol/mol/7.1–7.6% DCCT; and quartile 4: > 60 mmol/mol/7.6% DCCT). Patients with diabetes were also subgrouped according to the duration of diabetes (< 5 years, 5–10 years, > 10 years, and unknown duration). Major complications were defined as Clavien-Dindo grade ⩾ 3a. Postoperative pancreatic fistula was defined as clinically relevant postoperative pancreatic fistula, consisting of grade B or C postoperative pancreatic fistula according to the International Study Group of Pancreatic Surgery (ISGPS). 20 Postoperative pancreatic fistula grading data according to the ISGPS grading system have been entered into the registry by the surgeon since 2018. For patients who underwent surgery before this date and who were entered into the registry as having had a postoperative pancreatic fistula (i.e. with no grading specified in the registry), a modified fistula grading system was employed. A postoperative pancreatic fistula was considered to be a clinically relevant fistula (such as an ISGPS B- or C-grade fistula) if patients were registered as having both a pancreatic fistula and a complication according to a Clavien-Dindo grade ⩾2, as well as a surgical infection. 21 Patients who did not meet these criteria were considered to have biochemical leakage; thus, they were not considered to have postoperative pancreatic fistula in this study. The modified grading system was validated against patients who underwent surgery after 2018 to ensure acceptable precision. The Swedish Authority for Ethics in Clinical Research approved the study protocol. Patients are included in the registries in an opt-out manner; therefore, the need for informed consent was waived by the ethics authority. The study protocol was not preregistered. Furthermore, patients were anonymized by the registries after cross-linking.
Statistical analysis
Parametric data are presented as the means with standard deviations; moreover, nonparametric continuous data are presented as medians and interquartile ranges, and categorical data are presented as frequencies with relative frequencies. Student’s t-test was used for hypothesis testing of the parametric data; moreover, the Wilcoxon test was used for the assessment of nonparametric data, and the chi-square test was used for the assessment of the categorical variables. Univariable and multivariable logistic regressions were conducted to identify variables associated with the primary outcome, and separate regressions were conducted for each of the secondary outcomes. Covariates for the multivariable regression were included via purposeful selection of variables considered to be clinically relevant. 22 The model consisted of the following six covariates: laparoscopic approach, body mass index (BMI, which was categorized as underweight: BMI < 18.5, normal or overweight: BMI 18.5–30 and obese: BMI > 30, according to the World Health Organization (WHO) definition, 23 sex and age at operation as the continuous variables). As the data were mostly complete (incomplete cases: n = 43, 3.3%), missing BMI data were handled by the imputation of the mode value before the multivariable regression analysis was performed, and univariable analysis was performed by complete case analysis. A sensitivity analysis was conducted by including patients with missing data regarding postoperative complications (n = 78) and by considering these patients as having no postoperative complications.
Results
A total of 1297 patients were included in this study, of whom 247 (19%) patients had preoperatively diagnosed DM. A detailed account of the inclusions and exclusions is shown in Fig. 1. A majority of the patients (701, 54%) were female. The most common pancreatic pathology involved a malignant lesion (39%), followed by benign pancreatic tumors (29%). The full distribution of the pathologies, as well as the clinical characteristics of the patients with and without DM, is shown in Table 1. Compared with patients without diabetes, patients with diabetes were older, and a greater proportion of the patients with diabetes required surgery due to pancreatic malignancy, demonstrated a WHO performance status of 1 or 2, exhibited an American Society of Anesthesiology (ASA) classification score of 3 or 4 and were more likely to be obese. Surgery was performed by the laparoscopic approach in 294 (23%) patients, and spleen-preserving surgery was performed in 103 (8%) patients. Patients with DM were less likely to have received spleen-preserving surgery and exhibited a somewhat greater amount of intraoperative bleeding (the intraoperative characteristics of the patients with and without diabetes are shown in Supplemental Table S1). In terms of the DM classification, the vast majority of the patients were classified as having type 2 DM (n = 215, 87%), whereas only 10 patients (4%) were classified as having type 1 DM, 16 patients (6%) were classified as having other specified types of DM, and 6 patients (2%) were unclassified. The diabetes type, antidiabetic treatment, and HbA1c levels of the patients with and without complications are shown in Table 2. When comparing patients grouped according to HbA1c levels and duration of diabetes, patients exhibiting higher HbA1c levels and longer durations of diabetes were more likely to receive treatment with insulin, either alone or in combination with other antidiabetic medications (an overview of the antidiabetic medication treatment according to HbA1c levels and disease duration is shown in Supplemental Tables S2 to S4). No association between HbA1c levels and creatinine levels was observed (p = 0.418).
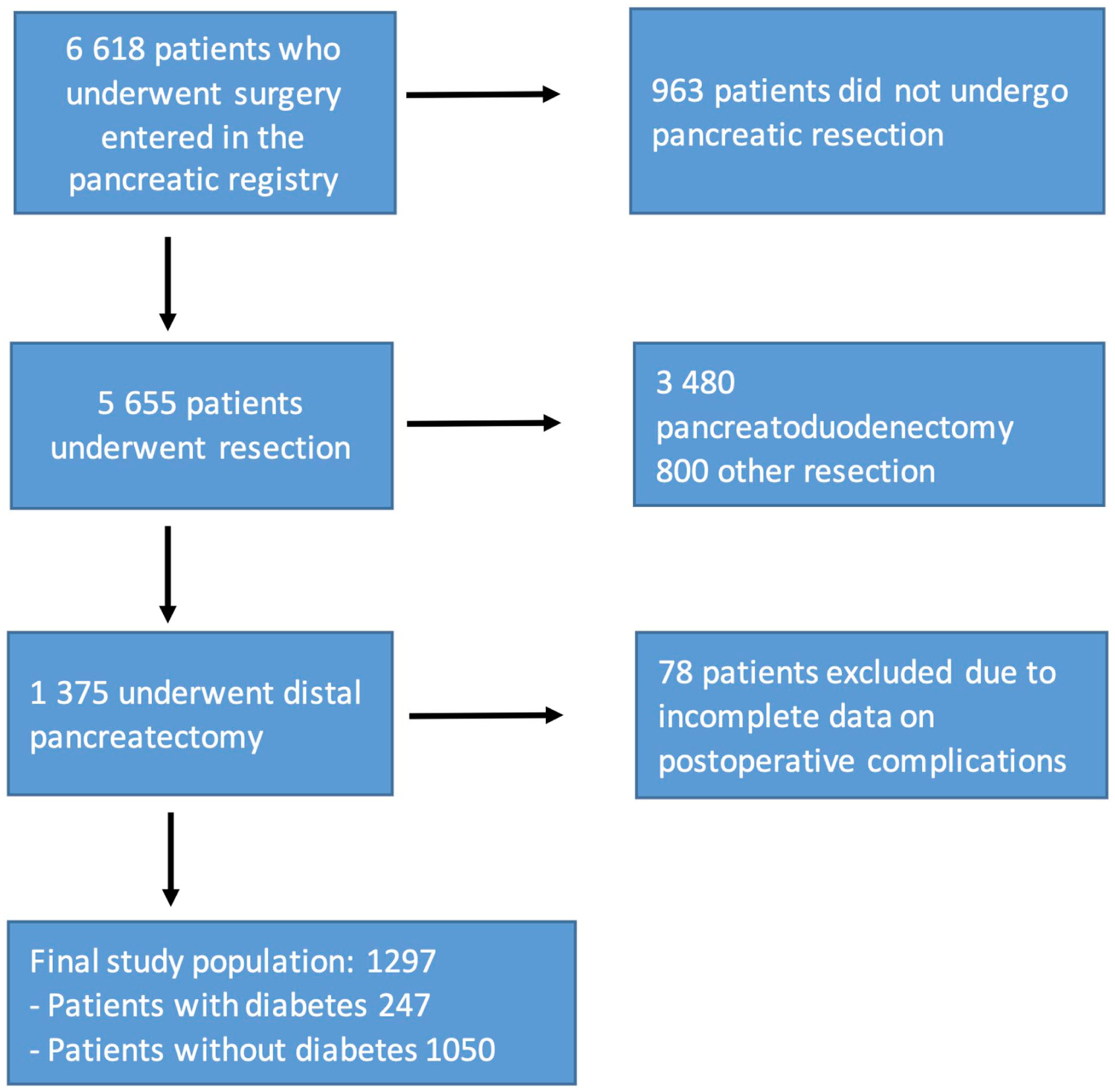
Flowchart describing the event pathway of patients identified in the Swedish Pancreatic and Periampullary Cancer registry.
Preoperative characteristics for patients with and without diabetes.
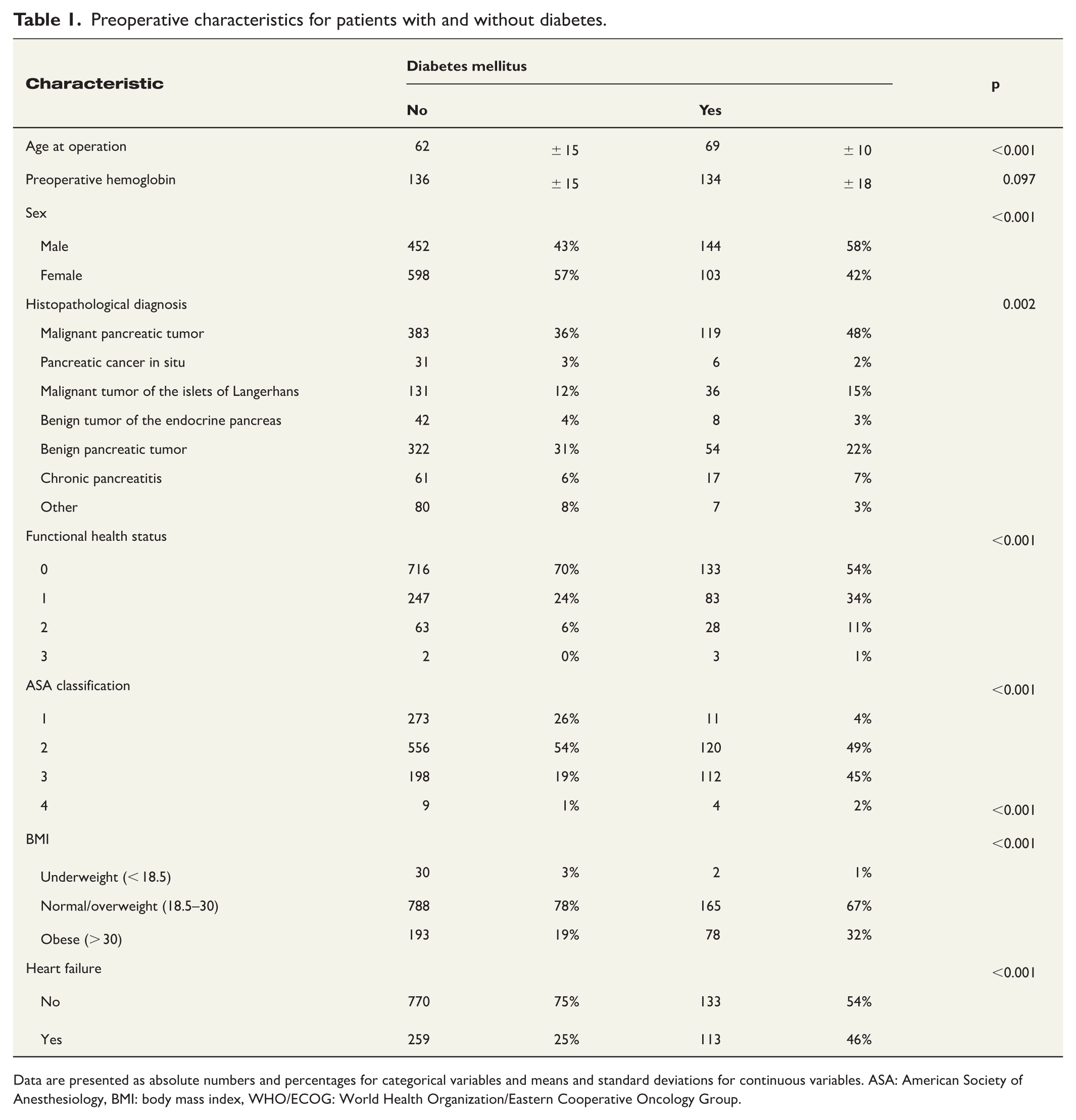
Data are presented as absolute numbers and percentages for categorical variables and means and standard deviations for continuous variables. ASA: American Society of Anesthesiology, BMI: body mass index, WHO/ECOG: World Health Organization/Eastern Cooperative Oncology Group.
Diabetic characteristics for patients with and without postoperative complications.
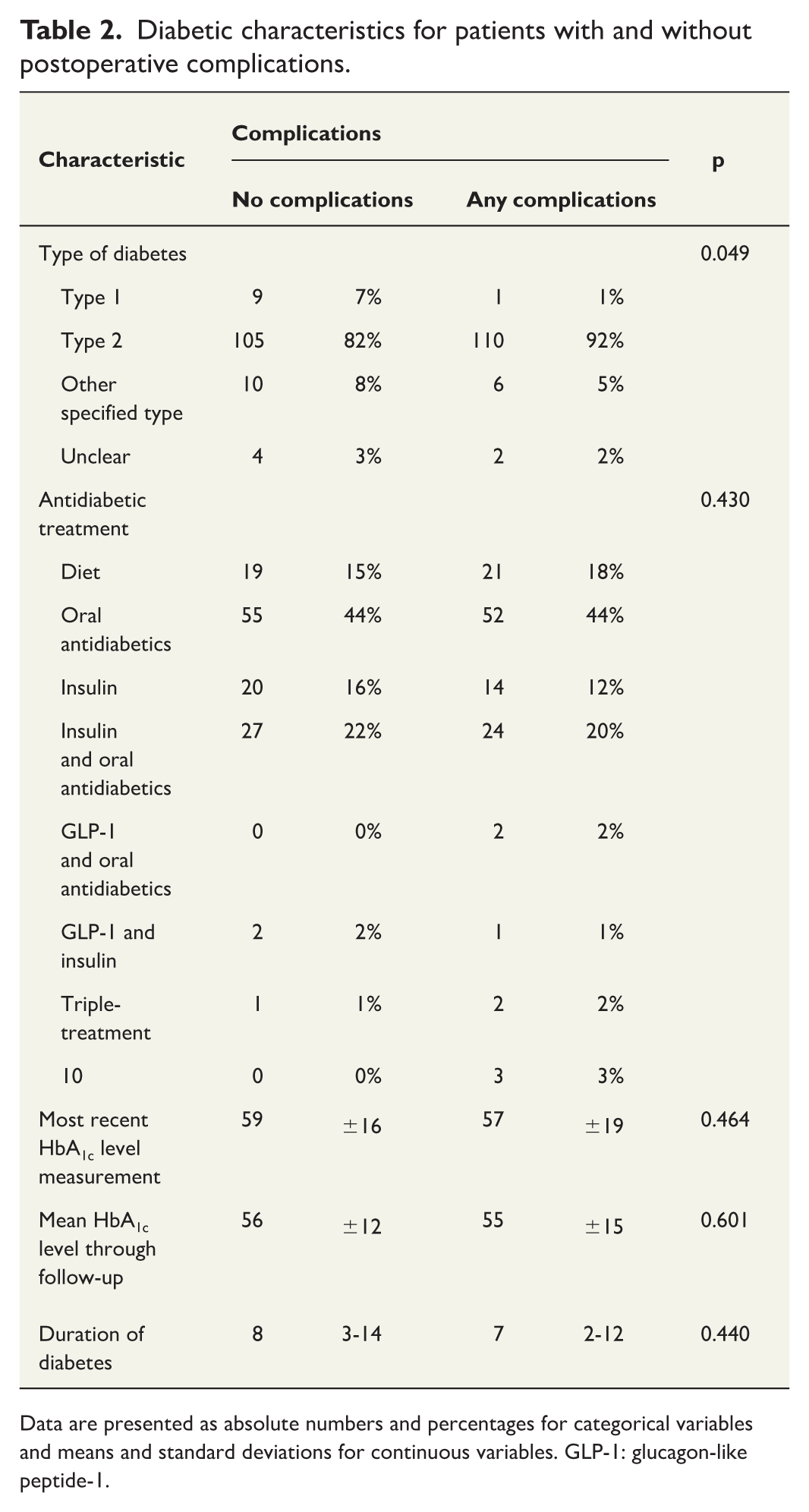
Data are presented as absolute numbers and percentages for categorical variables and means and standard deviations for continuous variables. GLP-1: glucagon-like peptide-1.
Postoperative complications occurred in 697 (54%) patients; specifically, 565 patients (44%) experienced surgical complications, and 263 patients (20%) experienced medical complications. Details of the complications are shown in Fig. 2. The most common type of complication was surgical site infection, which afflicted 174 patients (13%). As shown in Fig. 3, patients with DM did not demonstrate a significantly different risk for overall complications (odds ratio (OR) = 0.76, 95% confidence interval (CI) = 0.58–1.00; p = 0.052) compared to patients without diabetes, according to the univariable logistic regression. Furthermore, there were no differences observed in surgical complications (OR = 0.76, 95% CI = 0.57–1.00; p = 0.053), medical complications (OR = 1.03, 95% CI = 0.73–1.45; p = 0.872), or postoperative pancreatic fistula (OR = 0.79, 95% CI = 0.50–1.24; p = 0.603) between patients with and without DM.
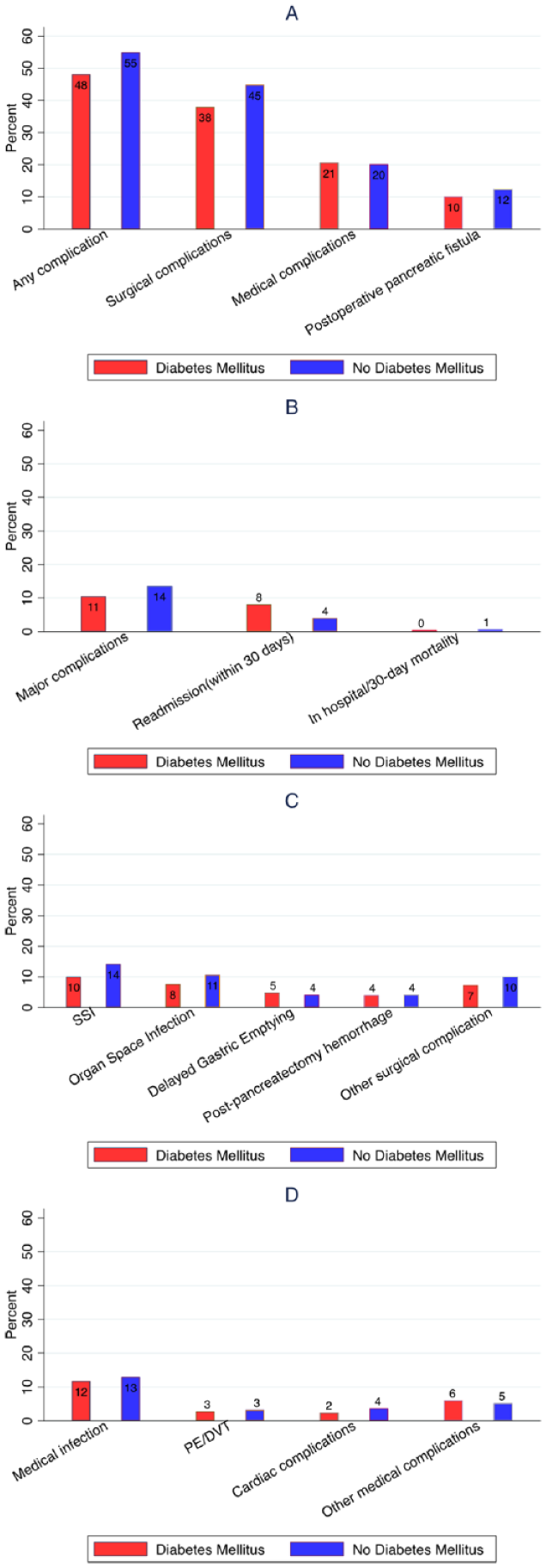
Bar charts of postoperative outcomes: (A) percentage of patients suffering from any complication, surgical complications, medical complications, or postoperative pancreatic fistula; (B) percentage of patients suffering from major complications, readmission within 30 days of index admission, in-hospital mortality, or 30-day mortality; (C) percentage of patients suffering from surgical site infection (SSI), organ space infection, delayed gastric emptying, postpancreatectomy hemorrhage, or other surgical complications; and (D) percentage of patients suffering from medical infection, pulmonary embolism or deep vein thrombosis (PE/DVT), cardiac complications, or other medical complications.
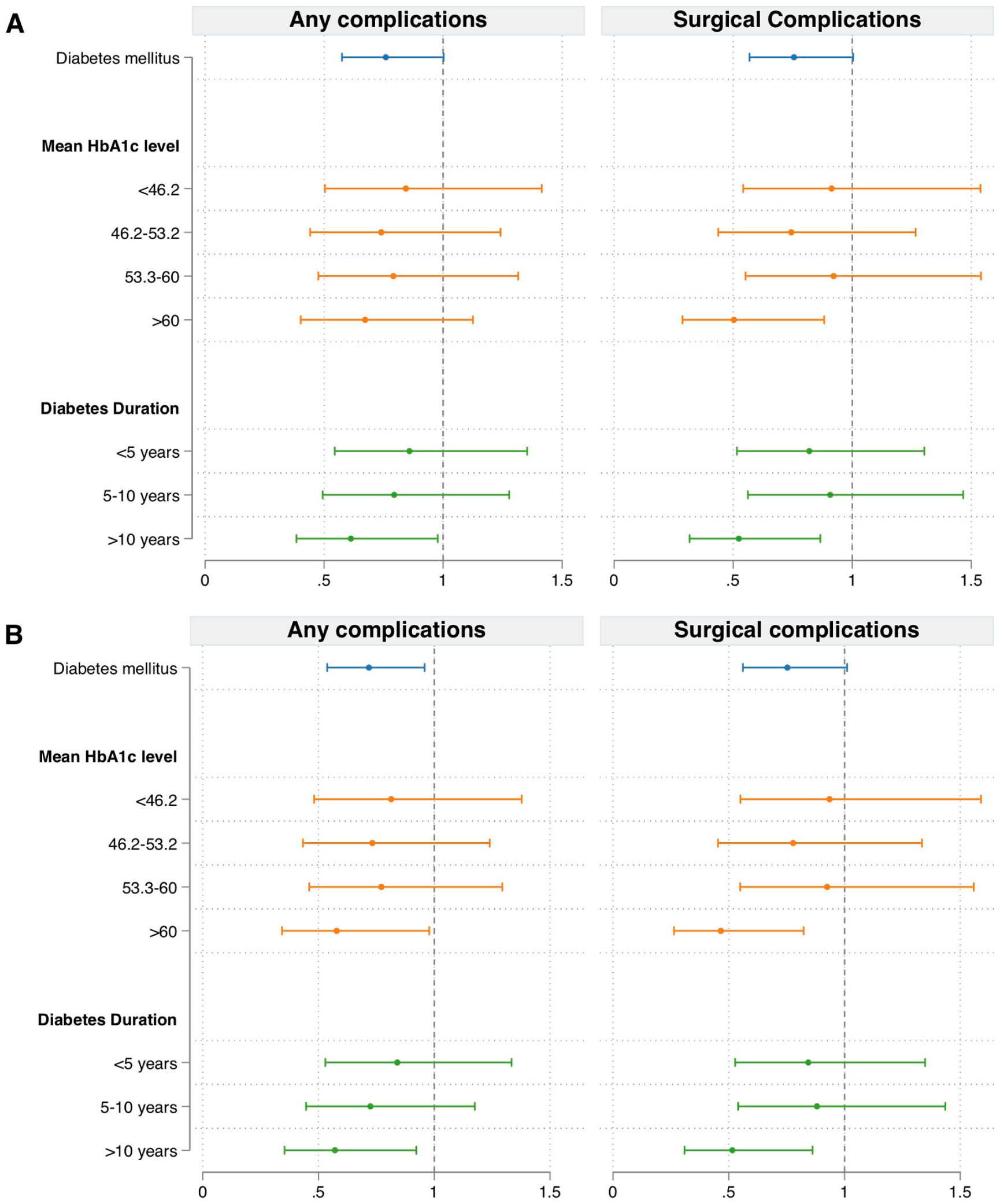
Univariable (A) and multivariable (B) logistic regressions of the risk of all postoperative complications, surgical complications, medical complications, and postoperative pancreatic fistula according to diabetes status, mean HbA1c level, most recent HbA1c measurement, and diabetes duration, respectively. The multivariable regression was adjusted for sex, age at operation, American Society of Anesthesiologists (ASA) score, laparoscopic surgery, and underweight status (BMI < 18.5) or obesity status (BMI > 30).
When patients were subgrouped by HbA1c levels, patients with a mean HbA1c level in the highest quartile (HbA1c ⩾ 60 mmol/mol) exhibited a lower risk of surgical complications (OR = 0.50, 95% CI = 0.29–0.88; p = 0.016). However, no differences were observed in overall complications (OR = 0.67, 95% CI = 0.40–1.13; p = 0.131), medical complications (OR = 1.26, 95% CI = 0.69–2.30; p = 0.448), or postoperative pancreatic fistula (OR = 0.36, 95% CI = 0.11–1.15; p = 0.085) compared to patients without diabetes in the univariable analysis. When HbA1c levels obtained at the most recent measurement were examined, patients in the highest quartile (HbA1c > 63 mmol/mol) exhibited a decreased risk of surgical complications (OR = 0.39, 95% CI = 0.22–0.71; p = 0.002); however, no differences were observed in overall complications (OR = 0.63, 95% CI = 0.38–1.06; p = 0.080), medical complications (OR = 1.26, 95% CI = 0.92–2.86; p = 0.098), or postoperative pancreatic fistula (OR = 0.48, 95% CI = 0.17–1.35; p = 0.167) compared with patients without diabetes. When examining the risk of complications for patients subgrouped according to duration of diabetes, patients with a duration of diabetes > 10 years demonstrated lower risks of overall complications (OR = 0.61, 95% CI = 0.38–0.98; p = 0.040) and surgical complications (OR = 0.52, 95% CI = 0.32–0.87; p = 0.012) but not medical complications (OR = 0.96, 95% CI = 0.53–1.71; p = 0.881), or postoperative pancreatic fistula (OR = 0.81, 95% CI = 0.38–1.73; p = 0.592) compared to patients without DM.
In the multivariable analysis (as shown in Table 3), patients with diabetes demonstrated a lower risk of overall complications compared to patients without diabetes (OR = 0.72, 95% CI = 0.54–0.96; p = 0.025). However, as shown in Fig. 3, there were no differences observed in surgical complications (OR = 0.75, 95% CI = 0.56–1.01; p = 0.059), medical complications (OR = 0.85, 95% CI = 0.59–1.21; p = 0.371) or postoperative pancreatic fistula (OR = 0.76, 95% CI = 0.48–1.22; p = 0.258) when examined separately.
Adjusted logistic regression for risk of any complication for patients with diabetes compared to patients without diabetes.
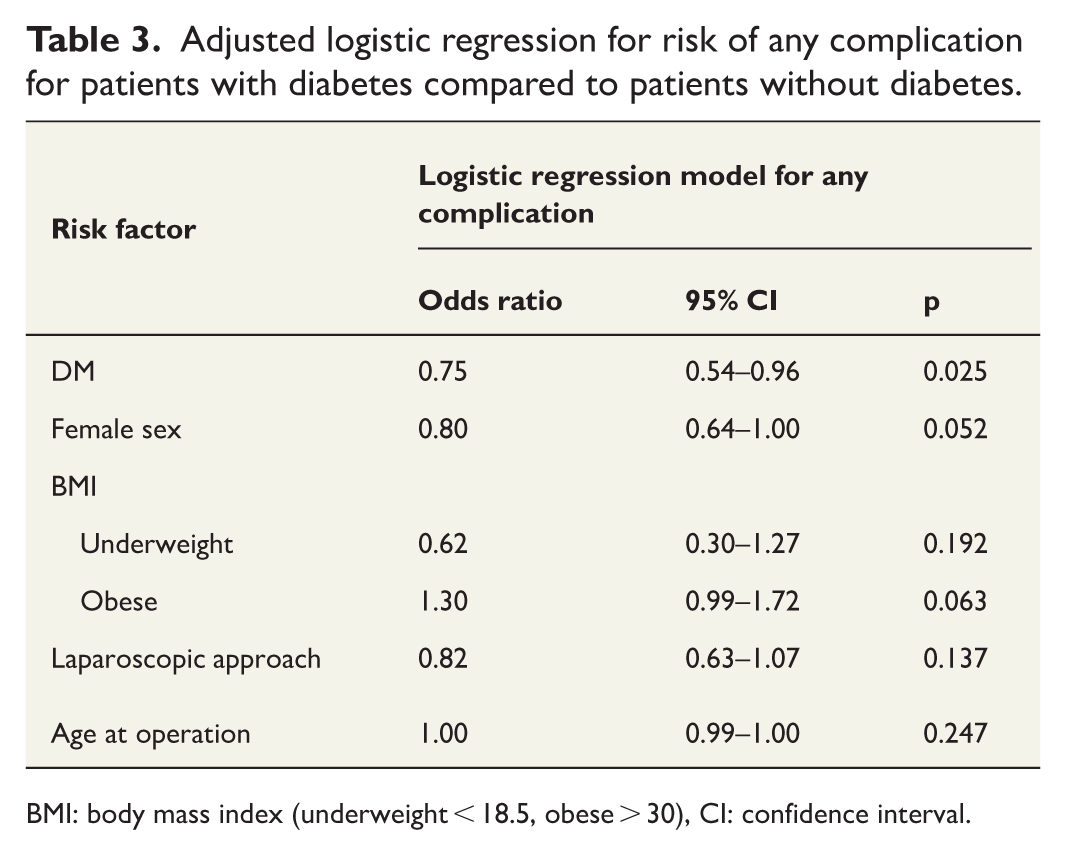
BMI: body mass index (underweight < 18.5, obese > 30), CI: confidence interval.
When examining the impact of glycemic control on the risk of complications, patients with HbA1c levels in the highest quartile at the last preoperative measurement demonstrated lower risks of overall complications (OR = 0.56, 95% CI = 0.33–0.95; p = 0.032) and surgical complications (OR = 0.37, 95% CI = 0.20–0.67; p = 0.001), whereas there was no significant association observed between HbA1c levels at the last measurement and medical complications (OR = 1.36, 95% CI = 0.76–2.44; p = 0.295) or postoperative pancreatic fistula (OR = 0.44, 95% CI = 0.16–1.24; p = 0.122) in the multivariable analysis. Moreover, there was no association observed between HbA1c levels in quartiles 1–3 at the most recent measurement and postoperative complications.
When the impact of long-term metabolic control (defined as the mean HbA1c level) was examined, patients within the highest mean HbA1c quartile demonstrated lower risks of overall complications (OR = 0.58, 95% CI = 0.34–0.98; p = 0.041) and surgical complications (OR = 0.47, 95% CI = 0.26–0.82; p = 0.009) compared to patients without DM in the multivariable analysis. There was no association observed between the mean HbA1c measurement and medical complications (OR = 1.00, 95% CI = 0.72–1.25; p = 0.991) or postoperative pancreatic fistula (OR = 0.31, 95% CI = 0.10–1.02; p = 0.054). There was no association observed between the mean HbA1c level in quartiles 1–3 and postoperative complications. In the subgroup analysis according to duration of diabetes, patients with a duration of > 10 years demonstrated lower risks of overall complications (OR = 0.57, 95% CI = 0.35–0.92; p = 0.022) and surgical complications (OR = 0.52, 95% CI = 0.31–0.86; p = 0.011) compared to patients without diabetes. There was no association observed between diabetes duration and the risk of medical complications (OR = 0.76, 95% CI = 0.42–1.39; p = 0.371) or postoperative pancreatic fistula (OR = 0.78, 95% CI = 0.36–1.69; p = 0.532).
Discussion
The present study comprehensively evaluated the associations between preoperatively diagnosed DM and the risk of postoperative complications in patients who underwent distal pancreatectomy. A decreased risk of overall complications in patients with diabetes was observed. Notably, the finding of the reduced risk of complications after distal pancreatectomy was mainly observed in patients with DM with longer disease duration and/or a higher preoperative HbA1c level (assessed both at the latest measurement before surgery and when long-term metabolic control was examined).
In contrast to our finding of lower overall complication rates for patients with DM, an American National Readmission Database study including 8401 patients who underwent pancreatic surgery (pancreatoduodenectomy, total pancreatectomy, or partial pancreatectomy) revealed that DM was associated with an increased risk of overall complications. Specifically, the risks of bleeding, as well as renal and endocrine complications, were increased, whereas there was no increase observed in the risk of pulmonary, infectious, or cardiovascular complications. However, the study included only complications treated in an inpatient setting and all types of pancreatic resections. Therefore, it is possible that the difference detected in our findings is due to differences in the patient population, as they did not specifically report the impact of DM on distal pancreatectomy. 11 In a retrospective review of 266 patients who underwent pancreatoduodenectomy for ampullary adenocarcinoma, Zhang et al. 24 reported no difference in overall complications between patients with and without diabetes.
Metabolic control is of paramount importance in managing DM to reduce the risks of microvascular and macrovascular long-term sequelae of diabetic disease, such as cardiovascular, renal, and retinal diseases.25,26 It is presumed that atherosclerotic and microangiopathic changes driven by hyperglycemia could lead to reduced microperfusion at surgical sites, thus predisposing patients with diabetes to impaired healing and increasing the risk of postoperative infections. It could also be hypothesized that diabetes-related changes to vital organs reduce the physiologic reserve of these tissues, thereby predisposing patients to medical complications such as postoperative renal or cardiac failure. This study attempted to assess whether factors associated with diabetes, such as metabolic control or diabetes duration, affect the risk of early postoperative complications after distal pancreatectomy. Surprisingly, this study revealed an association between increased HbA1c levels (i.e. worse metabolic control) and a reduced risk of complications, as well as an association between a longer duration of diabetes and a reduced risk of complications. These results indicate that the decreased risk of complications observed in patients with DM is more pronounced in patients with a higher and longer exposure to hyperglycemia, thereby suggesting that the decreased risk is indeed a result of DM rather than some confounding factor. Although caution is advised in interpreting these results, no support was demonstrated for the hypothesis that long-term preoperative hyperglycemia predisposes patients with diabetes to postoperative complications. This result contrasts with the aforementioned study of the American National Readmission Database published by Hussein et al. 11 According to the subgroup analysis conducted in their study, the risk of complications was increased in patients with type 1 DM and in patients with DM with poor glycemic control or diabetic complications, thus suggesting that long-standing, poorly controlled diabetes is a potential risk factor for postoperative complications.
DM and elevated HbA1c levels have also been observed to be associated with increased pancreatic fibrosis, thereby potentially decreasing the risk of postoperative pancreatic fistula after pancreatic resection. In a study of 29 patients who underwent pancreatic resection for pancreatic malignancy, findings indicative of fibrosis on preoperative magnetic resonance imaging (MRI) were correlated with preoperative HbA1c levels, thereby suggesting that hyperglycemia is correlated with an increased degree of pancreatic fibrosis. 5 Furthermore, in a murine model of chronic pancreatitis, DM increased fibrosis via enhanced collagen I deposition, along with increasing the proliferation of interstitial cells and stimulating the expression of α-smooth muscle actin in stellate cells. 4 These findings are indicative of a potential association between DM and favorable pancreatic consistency, which could reduce the risk of postoperative pancreatic fistula. However, previous studies have demonstrated conflicting results regarding an association between DM and the risk of postoperative pancreatic fistula, and there was no association detected between DM and postoperative pancreatic fistula after distal pancreatectomy in the present study.12,14,27
Given that the association between DM and a decreased risk of complications reported in this study contrasts with the general increase in the risk of postoperative complications observed in patients with diabetes, it is plausible that the decreased risk is conferred by some type of pancreas-specific mechanism. Postoperative hyperamylasemia and postpancreatectomy acute pancreatitis are increasingly becoming recognized as drivers of postoperative morbidity and have been observed to increase the risk of other systemic and local complications.28–30 Furthermore, postoperative hyperamylasemia was observed to be less common in patients with DM, as well as in patients with a hard pancreatic texture, in a recent study of pancreatoduodenectomy by Bannone et al. 29 DM has also been associated with a lower frequency of a soft pancreas (46% in patients with DM vs 80% in patients without DM), thereby suggesting a potential link between a lower risk of postoperative hyperamylasemia and DM. 31 Interestingly, amylase levels have been observed to be lower in patients with DM than in healthy controls.32,33 Finally, among patients with DM, longer disease durations and higher HbA1c levels have been associated with lower amylase levels.33,34 These findings, combined with the findings of the present study, suggest that the decreased frequency of soft pancreatic texture in patients with DM could reduce their risks of postoperative hyperamylasemia and/or postpancreatectomy acute pancreatitis, thereby reducing their overall risk of complications following distal pancreatectomy.
The present study is a retrospective registry study; therefore, it is limited by unknown confounding factors. Moreover, this study is limited to data available from the registry, and information parameters such as pancreatic texture, as well as data on the type and duration of antibiotic prophylaxis, would have improved the analysis. There could also be selection bias in the treatment strategies for diabetic disease, which could lead to confounding effects regarding the HbA1c values. Furthermore, it has been demonstrated that diabetes is underdiagnosed in patients undergoing pancreatic surgery. 35 Therefore, the identification of patients with diabetes via the diabetic registry may represent an underestimation of the true diabetic prevalence in our study population; such bias could lead to an underestimation of the difference between patients with and without diabetes. However, the use of the National Diabetes Registry also represents one of the strengths of the present study, as we utilized very reliable identification of patients with diagnosed diabetes and had access to long-term data that are typically not available in pancreatic registries. Notably, most of the patients included in the National Diabetes Registry are classified as having type 2 diabetes if they do not have measurable levels of antibodies; however, in the present study, some of these patients may instead have had pancreatogenic diabetes (i.e. type 3 diabetes). Finally, patients with DM were divided into quartiles, and other categorizations could lead to different results.
In conclusion, the present study revealed a lower risk of complications in patients with preoperatively diagnosed DM who underwent distal pancreatectomy after adjustments for confounders. The results of this study also suggest that worse preoperative metabolic control and longer diabetic disease duration are associated with a lower risk of postoperative complications.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969251390998 – Supplemental material for The effect of diabetes on complications after distal pancreatectomy: A population-based cross-matched registry study
Supplemental material, sj-docx-1-sjs-10.1177_14574969251390998 for The effect of diabetes on complications after distal pancreatectomy: A population-based cross-matched registry study by Henrik Bergenfeldt, Eva Ekström, Katarina Fagher, Karin Filipsson and Bodil Andersson in Scandinavian Journal of Surgery
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Ethical approval
The Swedish Authority for Ethics in Clinical Research approved the study protocol.
Clinical trial registration
The study protocol was not preregistered.
Patient confidentiality
Patients were anonymized by the registries after cross-linking. The identities of the patients were not known to the authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.