
Abstract
Background and aims:
Antibiotics for computed tomography (CT)-confirmed uncomplicated acute appendicitis is a safe and feasible treatment alternative highlighting the importance of accurate pre-interventional differentiation between uncomplicated and complicated appendicitis. CT is the gold standard in assessing appendicitis severity. The aim of this study was to assess potential prognostic CT factors for complicated acute appendicitis.
Methods:
A large prospective patient cohort was collected in concurrence with enrollment in two randomized clinical trials between April 2017 and November 2018 with CT-diagnosed acute appendicitis with both available histopathology and surgical diagnosis. The main aim was to evaluate the effect of appendiceal diameter on appendicitis severity. Other assessed CT variables included appendiceal wall enhancement defect and fluid and edema around the appendix. A subgroup analysis on patients without an appendicolith was performed.
Results:
The main analysis included 3085 patients with CT-diagnosed appendicitis, and there were 1965 patients without an appendicolith in the subgroup analysis. In both analyses, wider appendiceal diameter (p < 0.001) and appendiceal wall enhancement defect (p < 0.001) were associated with increased risk of complicated acute appendicitis. No clear cut-off point for appendiceal diameter association with complicated appendicitis could be determined. Among patients without an appendicolith, appendiceal wall enhancement defect had an odds ratio (OR) of 3.39 (95% confidence interval [CI] = 2.10 to 5.50) for complicated appendicitis.
Conclusions:
Wider appendiceal diameter and appendiceal wall enhancement defect on CT are objective imaging findings associated with an increased risk of complicated acute appendicitis. These findings and risks should be acknowledged by clinicians when selecting the optimal treatment alternative for each patient and assessing whether a patient is suitable for non-operative treatment.
Keywords
Summary
This study indicates that wider appendiceal diameter and wall enhancement defect on CT increase the risk of complicated appendicitis, which can guide clinicians in selecting optimal treatment alternatives for acute appendicitis.
Context and relevance
The safety and effectiveness of antibiotic treatment for CT-confirmed uncomplicated acute appendicitis emphasize the need for accurate pre-treatment differentiation between uncomplicated and complicated acute appendicitis. There is still a large population of patients with acute appendicitis who appear to have a higher risk for appendectomy and non-responsiveness to non-operative treatment. There is a major knowledge gap regarding the pre-interventional factors associating with a higher risk of a more complicated course of the disease. In this study, a larger appendix diameter was associated with complicated acute appendicitis (p < 0.001) with no specific cut-off point. Appendiceal wall enhancement defect had an OR of 2.21 (95% CI = 1.55 to 3.16) for complicated acute appendicitis. Clinicians should acknowledge these findings and risks when selecting the optimal treatment alternative for each patient and assessing whether a patient is suitable for non-operative treatment.
Introduction
The over century-long paradigm of appendectomy as standard treatment for all patients with acute appendicitis has been challenged by the effectiveness and safety of non-operative treatment of computed tomography (CT) confirmed uncomplicated acute appendicitis.1–5 With epidemiological and clinical data supporting the hypothesis that uncomplicated and complicated acute appendicitis are two different diseases,6–8 pre-intervention differential diagnosis of acute appendicitis severity is crucial for optimal treatment selection.9,10 In order to optimize all appendicitis treatment alternatives, clinically the most important issue is to rule out complicated acute appendicitis by identifying potential findings associated with a more complicated course of the disease. Uncomplicated acute appendicitis can be treated with antibiotics2,11–13 and perhaps even with symptomatic therapy,14–16 while complicated acute appendicitis most often requires emergency surgery excluding patients with periappendicular abscess. 17 However, between these two forms of appendicitis severity lies a gray area in acute appendicitis, where some could benefit from non-operative treatment and others from emergency appendectomy. Findings associated with non-responsiveness to antibiotics are not yet uniformly defined.
The presence of an appendicolith on pre-operative imaging and enhancement defect of the appendiceal wall, as well as periappendiceal fluid, have all been reported to predict non-responsiveness to non-operative treatment.1,18–21 Another finding associated with a more complicated course of the disease is appendiceal diameter. 22 Haijanen et al. 23 found that appendiceal diameter greater than or equal to 15 mm on CT was associated with primary non-responsiveness to antibiotic therapy in a secondary analysis of the APPendicitis ACuta II Randomized Controlled Trial (APPAC II RCT). 12 Kim et al. 21 performed a systematic review and meta-analysis in 2018 concerning CT features for differentiating complicated and uncomplicated acute appendicitis. They identified ten CT features associated with complicated acute appendicitis: extra- and intraluminal appendicolith, periappendicular abscess, appendiceal wall enhancement defect, extraluminal air, ileus, periappendicular fluid collection, ascites, periappendiceal fat stranding, and intraluminal air.
The main aim of this study was to assess whether appendiceal diameter is associated with appendicitis severity. The secondary aim was to identify other CT characteristics associated with complicated acute appendicitis. Identification of potential prognostic pre-intervention CT findings could enable further improvement in patient selection for optimal treatment of acute appendicitis.
Methods
Study design
This study was a secondary analysis of a prospectively collected patient data of patients evaluated for enrollment in two concurrent multicentre randomized controlled trials (RCTs).12,15 Briefly, APPAC II (NCT03236961) was a multicentre noninferiority RCT comparing oral antibiotics with intravenous followed by oral antibiotics in the treatment of CT-confirmed uncomplicated acute appendicitis.12,24 APPAC III (NCT03234296) was a multicentre, superiority double-blind RCT comparing antibiotic therapy with placebo in the treatment of CT-confirmed uncomplicated acute appendicitis. 15 The trial protocol for the RCTs was approved by the ethics committee of the Hospital District of Southwest Finland, the Finnish Medicines Agency, and by institutional boards at each participating hospital. All patients gave written informed consent. The medical records of all patients assessed for eligibility in APPAC II or APPAC III due to suspected acute appendicitis were reviewed for this study. This study included only patients with both CT-confirmed appendicitis and available histopathology for reference standard diagnosis after surgery. The study population was collected from nine different hospitals. All study patients were imaged and treated with normal protocols of each hospital, and no standardized study protocol for intravenous enhanced CT imaging was used. Nevertheless, a standardized CT imaging report was used for all evaluated patients. The final clinical diagnosis was determined by two researchers already for the APPAC II 12 and APPAC III 15 RCTs based on both surgical and histopathological findings. The finding of intramural neutrophil invasion of the removed appendix was required for the histopathological diagnosis of acute appendicitis. The surgical finding of perforation, appendiceal neoplasm, and/or periappendicular abscess was evaluated as complicated acute appendicitis as well as gangrene of the appendix, if supported by both surgery and histopathology. The presence of an appendicolith, whether found on CT or during surgery, was also classified as complicated acute appendicitis.
Outcome measures
Evaluated CT characteristics included appendiceal diameter, fluid and edema around the appendix, and appendiceal wall enhancement defect. Patients were first divided into three groups—normal appendix, uncomplicated acute appendicitis, and complicated acute appendicitis—based on both surgical and histopathological findings. In the analysis of CT variables, patients were categorized into two: those with complicated acute appendicitis and those with uncomplicated acute appendicitis or a normal uninflamed appendix. The primary CT variable was the diameter of appendix also aiming to identify a potential cut-off value predicting complicated acute appendicitis. Secondary CT variables included appendiceal wall enhancement defect and accumulated fluid and edema around the appendix. A subgroup analysis for the same CT characteristics was performed for patients with no appendicolith on CT to eliminate the effect of appendicolith as a possible contributing factor for complicated acute appendicitis.
Statistical methods
Categorical variables were characterized using frequencies and percentages, and continuous variables were described using medians with range or quartiles. Differences between groups were evaluated using Pearson’s Chi-square test for categorical variables and non-parametric Kruskall–Wallis test for continuous variables. Univariate binomial logistic regression was used to analyze associations of explanatory variables (appendiceal diameter, fluid, and edema around the appendix, and the appendix wall enhancement defect) to complicated appendicitis and results were quantified using odds ratios (ORs) with 95% confidence intervals (CIs). In addition, a multivariable binomial logistic regression analysis was conducted in further analyses of complicated appendicitis. The model included CT variables (appendiceal diameter, fluid, and edema around the appendix, and the appendix wall enhancement defect) and baseline characteristics (sex, age, body mass index, temperature, white blood cell count, and C-reactive protein). Receiver operating characteristic (ROC) curve was used to evaluate a possible cut-off point value for appendix diameter to predict complicated appendicitis and area under the ROC-curve (AUC) with 95% CIs was presented as a result. Sensitivity and specificity of possible cut-off points with 95% CIs were also presented. In the subgroup analysis among patients without an appendicolith, CT characteristics (appendiceal diameter, fluid, and edema around the appendix, and the appendix wall enhancement defect) were analyzed for possible association for complicated acute appendicitis similarly to the main analysis. Two-sided tests were used, and p-values less than 0.05 were considered statistically significant. Statistical analyses were performed using SAS System for Windows, Version 9.4 (SAS Institute Inc, Cary, NC, USA).
Results
There were 3512 patients with clinical suspicion of acute appendicitis. Of these, 3085 had CT-confirmed acute appendicitis with a final diagnosis based on histopathology and surgical finding, collected between April 1, 2017, and November 27, 2018. Out of these 3085 patients analyzed for potential predictive CT findings of complicated acute appendicitis, 1531 (49.6%) had complicated acute appendicitis, 1495 (48.5%) had uncomplicated acute appendicitis, and 59 (1.9%) had normal appendix with no inflammation (Fig. 1). Patient demographics and baseline characteristics are shown in Table 1.
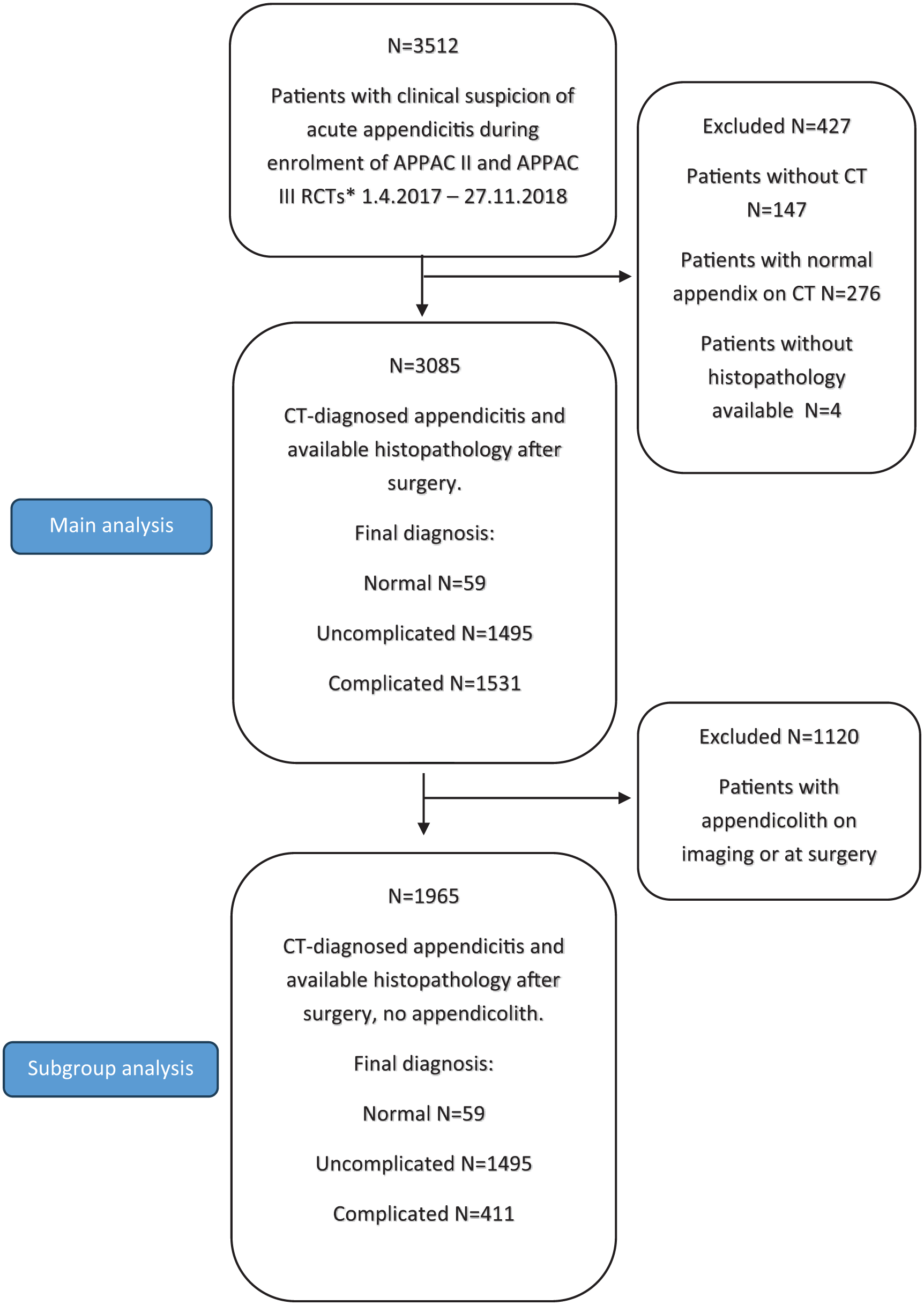
Patient flowchart.
Patient demographics and baseline characteristics.
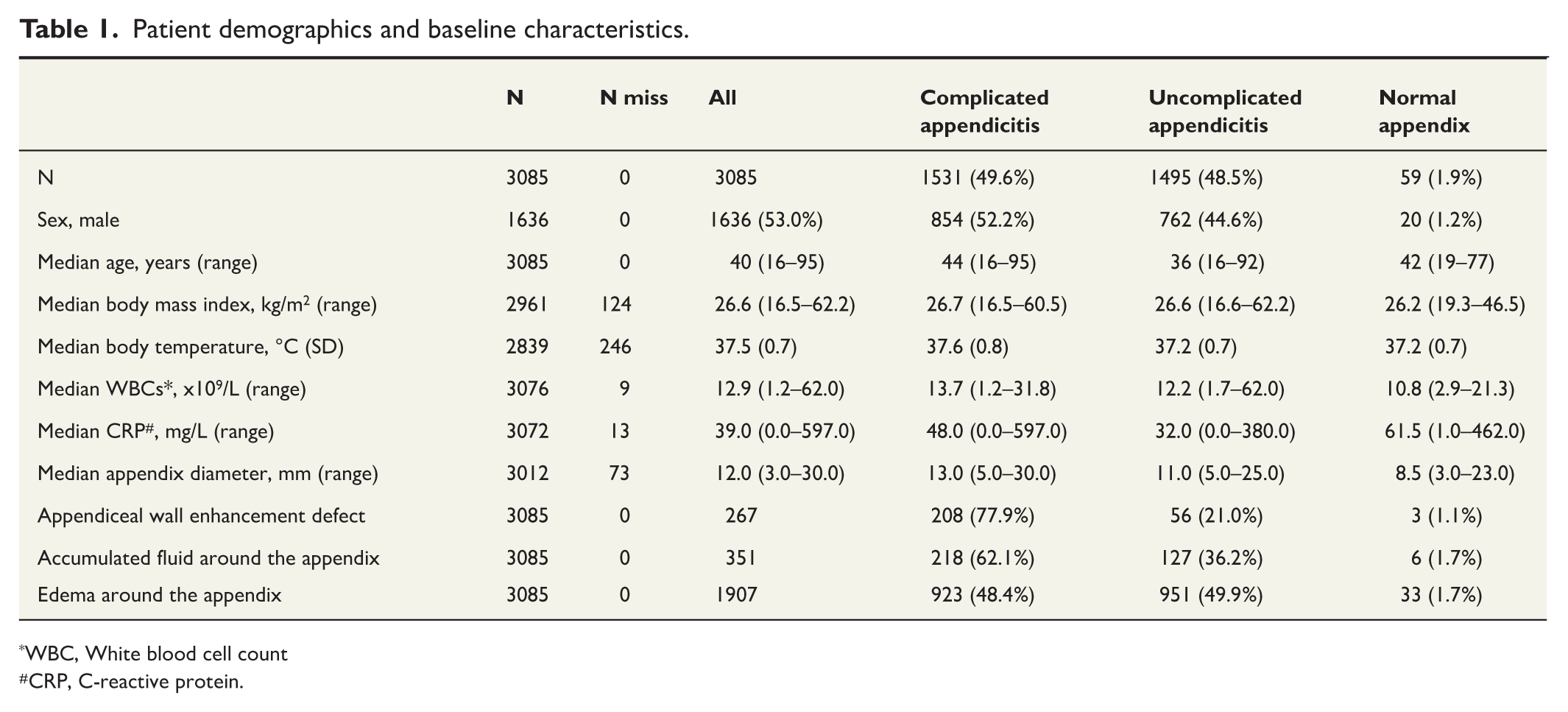
WBC, White blood cell count
CRP, C-reactive protein.
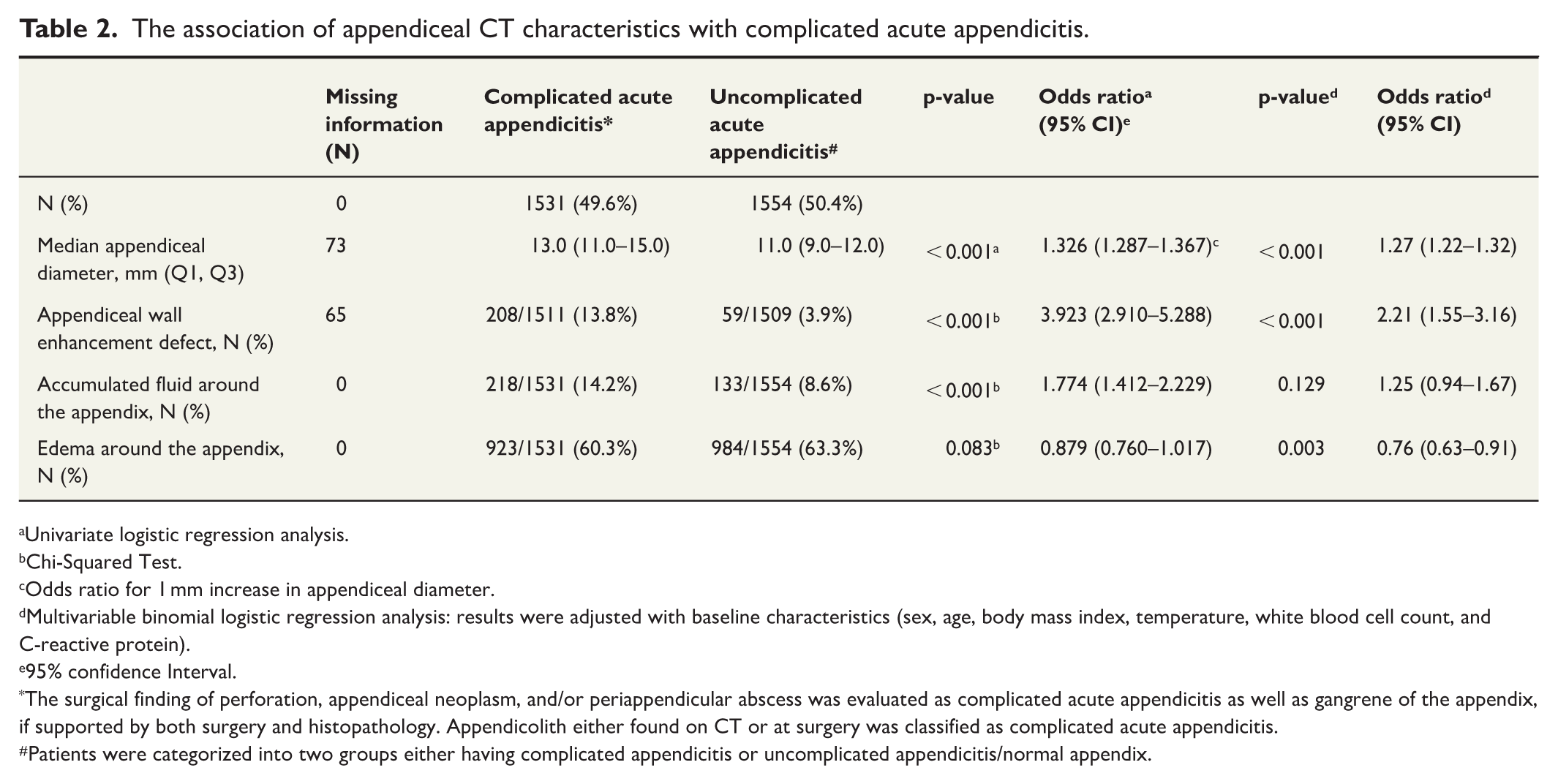
In the univariate analysis, a larger appendiceal diameter was associated with complicated acute appendicitis (p < 0.001), but no clear cut-off point could be established (Table 2). AUC was 0.713 (95% CI = 0.695 to 0.731). Different variations of possible cut-off points for appendiceal diameter are presented in Supplementary Tables 1 and 2. Of the other assessed CT variables, appendiceal wall enhancement defect (p < 0.001) and accumulated fluid around the appendix (p < 0.001) were associated with complicated acute appendicitis (Table 2). The appendiceal wall enhancement defect had an OR of 3.92 (95% CI = 2.91 to 5.28) for complicated acute appendicitis.
The association of appendiceal CT characteristics with complicated acute appendicitis.
Univariate logistic regression analysis.
Chi-Squared Test.
Odds ratio for 1 mm increase in appendiceal diameter.
Multivariable binomial logistic regression analysis: results were adjusted with baseline characteristics (sex, age, body mass index, temperature, white blood cell count, and C-reactive protein).
95% confidence Interval.
The surgical finding of perforation, appendiceal neoplasm, and/or periappendicular abscess was evaluated as complicated acute appendicitis as well as gangrene of the appendix, if supported by both surgery and histopathology. Appendicolith either found on CT or at surgery was classified as complicated acute appendicitis.
Patients were categorized into two groups either having complicated appendicitis or uncomplicated appendicitis/normal appendix.
In the multivariable analysis adjusted with baseline characteristics, a larger appendiceal diameter was associated with complicated acute appendicitis (p < 0.001) and the OR for 1 mm increase in appendiceal diameter for complicated acute appendicitis was 1.27 (95% CI = 1.23 to 1.32). The appendiceal wall enhancement defect had an OR of 2.21 (95% CI = 13.55 to 3.16; p < 0.001) for complicated acute appendicitis. In the multivariable analysis, accumulated fluid around the appendix was not statistically significantly associated with complicated acute appendicitis (p = 0.129, OR = 1.25 (95% CI = 0.94 to 1.67)).
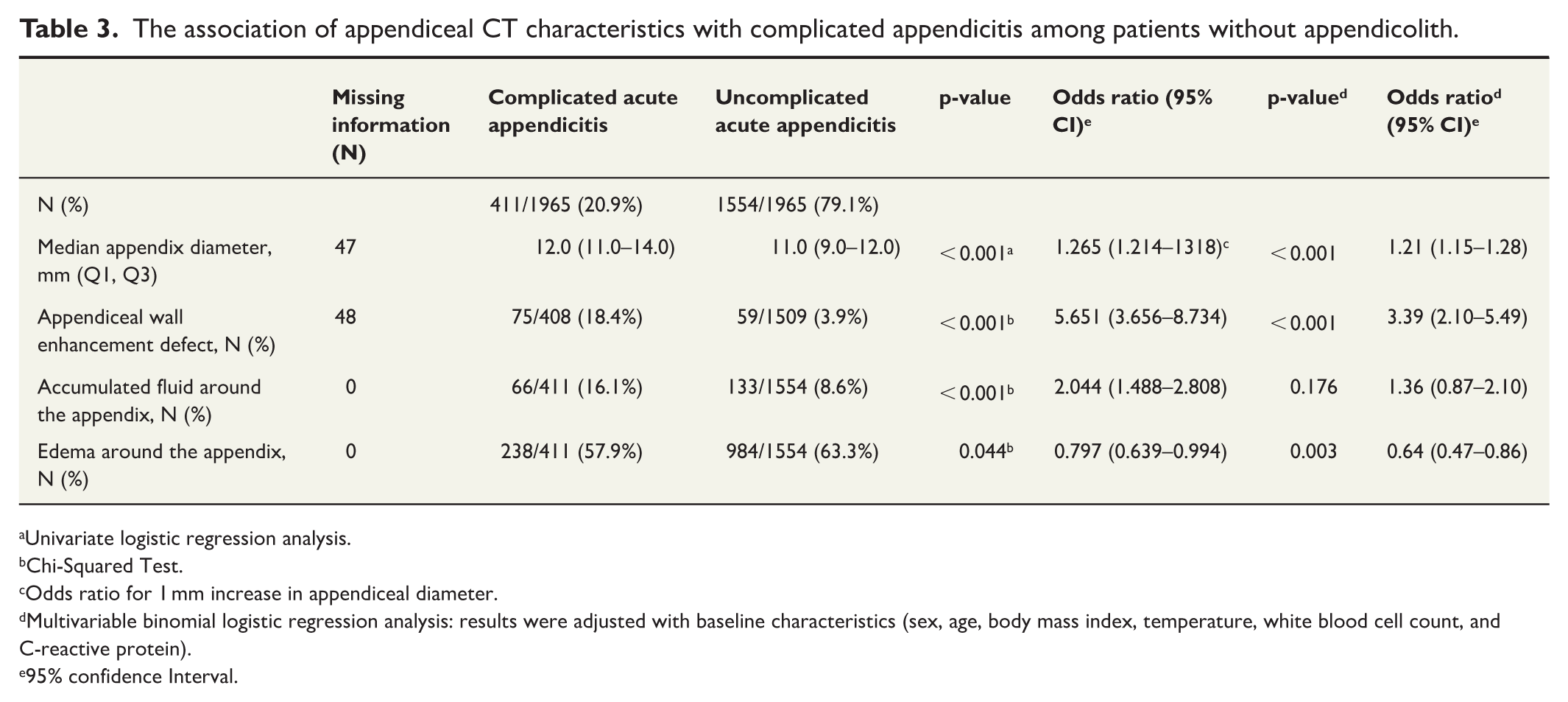
In the subgroup analysis of patients presenting without an appendicolith, there were 1965 patients (Fig. 1). Out of these 1965 patients, 411 (20.9%, n = 411/1965) had complicated acute appendicitis, 1495 (76.1%, n = 1495/1965) had uncomplicated acute appendicitis, and 59 (3.0%, n = 59/1965) patients had a normal appendix. In this subgroup analysis, the appendiceal diameter (p < 0.001), appendiceal wall enhancement defect (p < 0.001), accumulated fluid around the appendix (p < 0.001), and edema around the appendix (p = 0.044) were all associated with complicated acute appendicitis (Table 3). The appendiceal wall enhancement defect had an OR of 5.65 (95% CI = 3.65 to 8.73) for complicated appendicitis.
The association of appendiceal CT characteristics with complicated appendicitis among patients without appendicolith.
Univariate logistic regression analysis.
Chi-Squared Test.
Odds ratio for 1 mm increase in appendiceal diameter.
Multivariable binomial logistic regression analysis: results were adjusted with baseline characteristics (sex, age, body mass index, temperature, white blood cell count, and C-reactive protein).
95% confidence Interval.
In the multivariable subgroup analysis excluding patients with appendicoliths, larger appendiceal diameter had an OR of 1.21 (95% CI = 1.15 to 1.28; p < 0.001) for complicated acute appendicitis, while appendiceal wall enhancement defect had an OR of 3.39 (95% CI = 2.10 to 5.49; p < 0.001). Accumulated fluid around the appendix had no association with complicated acute appendicitis (p = 0.129). As in the main analysis, edema around the appendix showed the opposite effect for complicated acute appendicitis, with an OR of 0.64 (95% CI = 0.47 to 0.86; p = 0.003).
Discussion
This study demonstrated a statistically significant association between a wider appendiceal diameter on CT and complicated acute appendicitis. Even though a clear cut-off point could not be determined, this study showed that appendiceal diameter is an important factor associated with appendicitis severity. Furthermore, in patients without an appendicolith, an appendiceal wall enhancement defect increases the probability of complicated appendicitis to 3.4-fold compared to a finding of even enhancement of the appendiceal wall. In clinical practice, these findings may support clinical decision-making and patient information when assessing optimal treatment options for patients with acute appendicitis.
Like many other surgical diseases, the treatment of acute appendicitis has been shifting more toward a non-operative approach in recent years based on robust data from RCTs.2,3,11–13 It is nowadays generally acknowledged that most patients with imaging-confirmed uncomplicated acute appendicitis without an appendicolith can be treated with antibiotics.11,25 However, no standardized definitions of appendicitis severity exist, and this knowledge gap must be addressed to optimize all treatment options. Optimization of antibiotic treatment of acute appendicitis requires identifying factors associated with non-responsiveness to antibiotics. With this in mind, we evaluated potential prognostic factors associated with complicated acute appendicitis visible on pre-intervention CT imaging. In addition, the role of antibiotics in the treatment of uncomplicated acute appendicitis still needs to be defined 14 as even symptomatic therapy alone has shown promising results.15,16,26
The appendiceal diameter of 7 mm or wider on CT is commonly accepted as criteria for uncomplicated acute appendicitis. 27 Haijanen et al. 23 reported that appendiceal diameter of greater than or equal to 15 mm was associated with the risk of primary antibiotic non-responsiveness. This study aimed to find more accurate cut-off point for clinical use, but no clear cut-off point could be determined. The chosen cut-off point depends on balancing sensitivity and specificity, as well as the level of risk acceptable to the patient and clinician when choosing between non-operative and surgical management. The findings of this study also corroborate with the findings from the CODA trial reporting OR of 1.09 (95% CI = 1.00% to 1.18) for complicated appendicitis for every 1 mm increase in the appendiceal diameter. 22
For the other CT characteristics assessed in this study, similar outcomes have been shown in other studies.21,28 For example, Hong et al. 29 showed that appendiceal wall enhancement defect was statistically significant in antibiotic treatment failure in patients with appendicitis and appendiceal diameter less than 12 mm. In this study, appendiceal wall enhancement defect was associated with complicated acute appendicitis indicating that emergency appendectomy may be a better option for patients with acute appendicitis and appendiceal wall enhancement defect. The problem with these secondary outcome CT characteristics (enhancement defect, fluid, edema) is their subjectivity compared to the objective nature of appendiceal diameter. Thus, internationally standardized definitions and criteria for these outcomes are needed to enable consistency between different trials and clinical guidelines. Fluid and edema are commonly seen around the appendix in acute appendicitis. This study showed statistical significance in both fluid around the appendix and in edema around the appendix associated with complicated appendicitis in patients without appendicolith. However, this statistical significance does not relate to any clinical significance in the differential diagnosis of appendicitis severity, as in patients with complicated acute appendicitis 57.8% (238/411) had edema around the appendix, while in patients with uncomplicated acute appendicitis, the corresponding number was 63.3% (984/1554), respectively.
This study had several limitations. The first limitation of this study is that the assessed variables, such as appendiceal wall enhancement defect and edema around appendix, are naturally subjective and potentially radiologist dependent. However, with the current gold standard diagnosis of acute appendicitis with CT, we need to assess all identifiable CT markers. The second limitation is that even though CT characteristics were associated with complicated acute appendicitis, the influence of patient-related factors, such as fever and inflammatory markers, cannot be eliminated. Third limitation is that this study did not evaluate non-operatively treated patients. However, in order to have the most reliable reference standard, that is, histopathology and surgical finding of the appendix, only patients undergoing appendectomy could be included. In addition to the large prospective cohort, this reference standard of as accurate as possible clinical diagnosis of acute appendicitis severity is the main strengths of this study.
In conclusion, appendiceal diameter seems to be an independent risk factor of complicated acute appendicitis. The risk of complicated acute appendicitis was also increased with appendiceal wall enhancement defect on CT. In patients with no appendicolith, an appendiceal wall enhancement defect increases the probability of complicated appendicitis to 3.4-fold compared with even appendiceal wall enhancement. These findings and risks should be acknowledged by clinicians when selecting the optimal treatment alternative for each patient and assessing whether a patient is suitable for non-operative treatment.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969251386556 – Supplemental material for Prognostic CT-imaging findings for complicated acute appendicitis
Supplemental material, sj-docx-1-sjs-10.1177_14574969251386556 for Prognostic CT-imaging findings for complicated acute appendicitis by Sami Sula, Miska Kujala, Ville Tammilehto, Saija Hurme, Tero Rautio, Pia Nordström, Tuomo Rantanen, Tarja Pinta, Anne Mattila, Juha Grönroos, Suvi Sippola, Jussi Haijanen and Paulina Salminen in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
We would like to thank all APPAC II and APPAC III trial researchers (Ari Leppäniemi, Eeva-Liisa Sävelä, Elisa Mäkäräinen, Eliisa Löyttyniemi, Hannu Paajanen, Harri Marttila, Heini Savolainen, Imre Ilves, Johanna Laukkarinen, Jukka Rintala, Markku Aarnio, Sanna Meriläinen, Tomi Sippola) and the whole APPAC study group for their contribution in patient recruitment. We also thank the Academy of Finland (Paulina Salminen), the Sigrid Jusélius Foundation (Paulina Salminen), the Finnish Medical Foundation (Sami Sula), and the Orion Research Foundation (Sami Sula) for providing research grants.
Author contributions
S.S. and P.S. accessed and verified the data. P.S., S.S., and J.H. conceived of the study. S.H. did the analysis. P.S. led all the APPAC randomized trials. S.S. wrote the first manuscript. All authors gave critical input into interpretation and manuscript writing and revision.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Academy of Finland, the Sigrid Jusélius Foundation, the Finnish Medical Foundation, the Mary and Georg C. Ehrnrooth Foundation, and the Orion Research Foundation sr. The funders had no role in the design and conduct of the study.
Data sharing
A completely de-identified patient data set will be made available to researchers on reasonable collaboration request addressed to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.