
Abstract
Background and aims:
Gangrenous appendicitis, a type of complicated appendicitis, is an indication of emergency surgery due to a high risk of perforation. However, it can be challenging to diagnose preoperatively. This study aimed to validate the predictive factors of patients with gangrenous appendicitis and develop a novel scoring model based on objective parameters.
Methods:
This retrospective single-center study included 171 of 302 consecutive patients undergoing appendectomy between April 2014 and December 2023. Patients with perforation, chronic appendicitis, and appendicitis presenting with an abscess were excluded from the analysis. In other words, the study targeted Grades 1 and 2 on the American Association for the Surgery of Trauma (AAST) severity assessment scale. Computed tomography (CT) scan value was defined as the average value of fluid in the appendix lumen on plain CT scan. Univariate and multivariate analyses were performed to identify the independent objective predictors of gangrenous appendicitis. A new scoring model was developed based on the logistic regression coefficients of the independent predictors. The scores were then classified into three categories, and the probability of gangrenous appendicitis for each category was evaluated.
Results:
Overall, 46 (27%) and 125 (73%) patients presented with gangrenous appendicitis (=AAST Grade 2) and non-gangrenous (uncomplicated) appendicitis (=AAST Grade 1), respectively. The independent predictive factors of gangrenous appendicitis included a CT value of ≥24 HU, an appendiceal diameter of ≥12 mm, the presence of cecal mucosal edema, and a C-reactive protein level of ≥5.4 mg/dL. The scoring model, based on these four independent predictors, ranged from 0 to 4. The probability values of gangrenous appendicitis were 0%, 15%, and 97% in the low (0)-, moderate (1, 2)-, and high (3, 4)-risk categories, respectively.
Conclusion:
Our scoring model may assist in decision-making concerning emergency surgery and appendicitis management.
Context and Relevance
The independent predictive factors of gangrenous appendicitis included a computed tomography value of ≥24 HU, an appendiceal diameter of ≥ 12 mm, the presence of cecal mucosal edema, and a C-reactive protein level of ≥54 mg/L. A novel scoring model was developed based on these four independent predictors, with scores ranged from 0 to 4. The probabilities of gangrenous appendicitis were 0%, 15%, and 97% in the low (0)-, moderate (1, 2)-, and high (3, 4)-risk categories, respectively. This scoring model can aid in decision-making for emergency surgery and appendicitis management.
Introduction
Acute appendicitis is one of the most common causes of lower abdominal pain resulting in emergency room visits. Further, it is the most common diagnosis in younger individuals hospitalized due to acute abdominal pain.1–3 The lifetime risk of acute appendicitis worldwide is approximately 7%–8%. 4 However, not all patients diagnosed with acute appendicitis require emergency surgery. The 2020 Update of the WSES Jerusalem guidelines on the diagnosis and treatment of acute appendicitis recommend discussing nonoperative management with antibiotics as a safe alternative to surgery in selected patients with acute appendicitis and absence of appendicolith for uncomplicated appendicitis, along with advising the patient of the risk of failure and of misdiagnosing complicated appendicitis. 5
Acute appendicitis can be classified as uncomplicated or complicated. Uncomplicated acute appendicitis is characterized by the absence of conditions such as perforation, abscess, and gangrene. In contrast, complicated acute appendicitis may be characterized by rapidly progressive gangrene, perforation, and abscess. Further, it occurs in approximately 4%–25% of all patients with acute appendicitis.6–10 Patients with complicated acute appendicitis such as those with perforated appendicitis and gangrenous appendicitis require emergency surgery as the condition may progress to acute peritonitis. Therefore, an accurate preoperative diagnosis is extremely important. Previous studies have shown that patients with appendicitis who present with an abscess can be effectively managed with conservative antibiotic treatment and abscess drainage, followed by interval appendectomy.11,12 Mällinen et al. 13 also reported that in a multicenter noninferiority randomized clinical trial (Peri-Appendicitis Acuta), the rate of neoplasia after periappendiceal abscess was higher, especially in patients over 40 years.
The preoperative diagnosis of gangrenous appendicitis is challenging. 5 Some studies have examined complicated acute appendicitis with perforation and gangrene.14–16 However, comparative studies on the specific predictors of complicated acute appendicitis without perforation and abscess are limited. This study aimed to validate the predictive factors of patients with gangrenous appendicitis and to develop a scoring model.
Methods
Patients and data collection
In total, 302 consecutive patients underwent appendectomy between April 1, 2014 and December 31, 2023. Patients with perforation (Fig. 1A) and abscess (Fig. 1B) on computed tomography (CT) scan, those with chronic appendicitis or appendiceal tumors, those with evident perforation based on specimen analysis, and those with appendicitis diagnosed via ultrasonography were excluded from the analysis. In other words, the study targeted Grades 1 and 2 on the American Association for the Surgery of Trauma (AAST) severity assessment scale. 17 Cases in which CT scan was not performed within 12 h of the start of surgery were also excluded. Surgery was performed even on children with acute appendicitis after obtaining consent from the parents. Therefore, patients aged <10 years were included in the study, and an upper age limit was not set. This study was performed in accordance with the principles of the Declaration of Helsinki and was approved by the institutional ethics committee. The need for informed consent was waived due to the retrospective nature of this study.
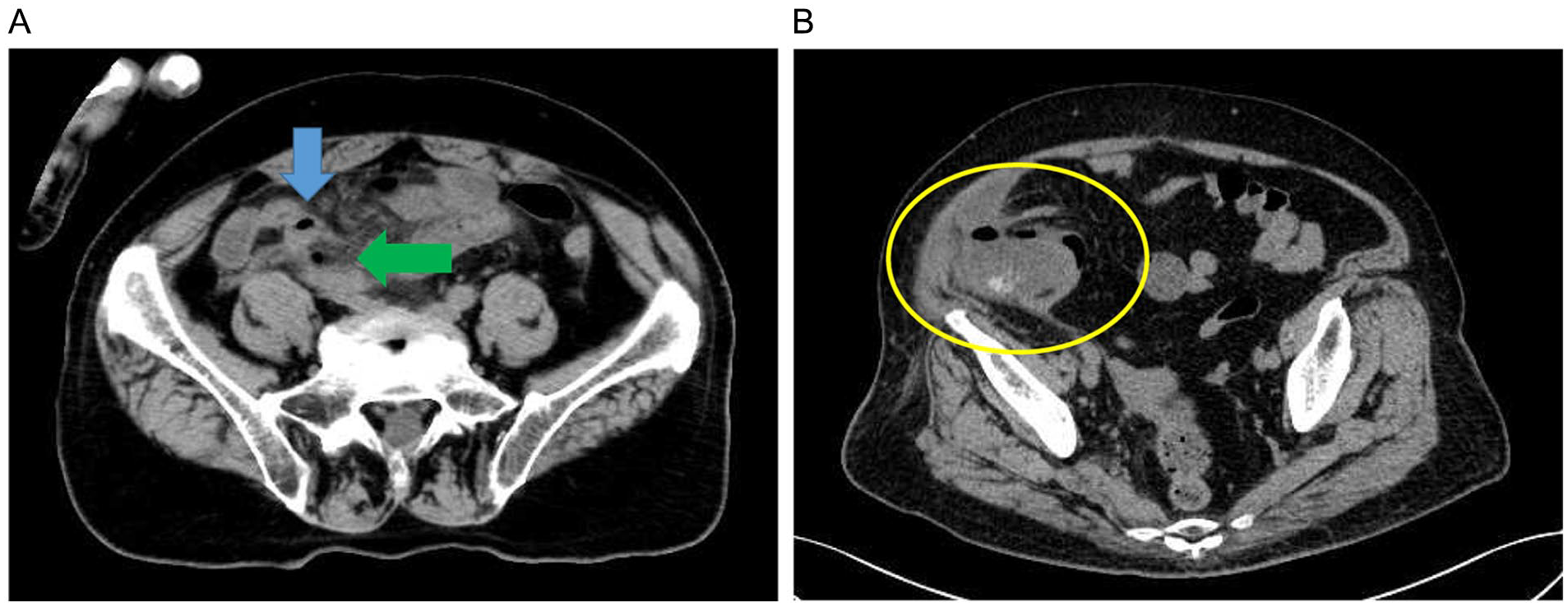
Computed tomography (CT) scan findings. (A) Appendicitis (blue arrow) with perforation. CT image shows free gas around the appendix (green arrow). (B) Appendicitis with abscess. CT scan image shows a pericecal abscess (yellow circle).
CT scan findings
CT scan value was defined as the average value of the maximum appendiceal lumen fluid on plain CT scan (Fig. 2A, B). The CT scan value of the fluid in the appendiceal lumen was calculated. The CT scan image was magnified, and caution was taken not to include the appendiceal wall. Appendix diameter was defined as the largest diameter measured on plain CT scan (Fig. 2C, D). Plain CT scan was performed to check for cecal mucosal edema. Patients with cecal mucosal edema at the root of the appendix were diagnosed with mucosal edema (+) (Fig. 2E, F). An increase in the fat concentration around the appendix was confirmed on simple CT scan, and patients with an evident increase in fat concentration were diagnosed with elevated fat concentration around the appendix (+) (Fig. 2G, H). One investigator (T.S.) performed all CT scan finding analyses under the supervision of an experienced radiologist. In addition, CT findings in all cases were obtained up to 12 h before the start of surgery. A low-dose CT protocol was used.
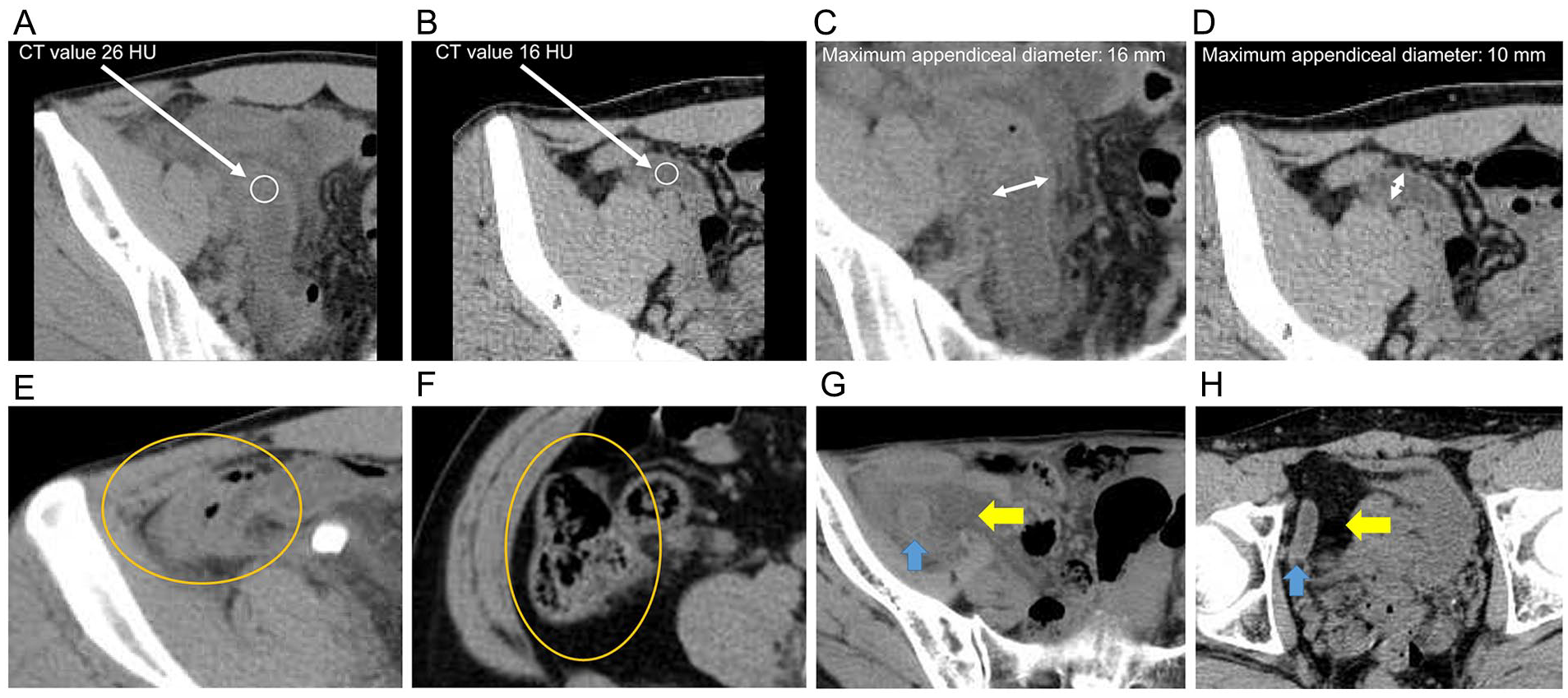
Computed tomography (CT) scan findings. (A) Gangrenous appendicitis (GA). CT scan value: 26 HU (white circle). (B) Uncomplicated appendicitis (UA). CT scan value: 16 HU (white circle). (C) GA. Appendiceal diameter: 16 mm (white arrow). (D) UA. Appendiceal diameter: 10 mm (white arrow). (E) GA. Edema in the cecal mucosal edema (+) (orange circle). (F) UA. Edema in the cecal mucosal edema (−) (orange circle). (G) GA (blue arrow). Fat concentration around the appendix (+) (yellow arrow). (H) UA (blue arrow). Fat concentration around the appendix (−) (yellow arrow).
Pathological examination
Histopathologically, catarrhal appendicitis is defined as the apparent enlargement of the lymphoid follicles in the appendix mucosa. Cellulitis appendicitis is defined as neutrophil infiltration into all layers. Gangrenous appendicitis is defined as neutrophil infiltration and muscle or full-thickness necrosis. Herein, gangrenous appendicitis and non-gangrenous appendicitis were defined as pathologically confirmed gangrenous (=AAST Grade 2) and catarrhal or cellulitis (=AAST Grade 1) appendices. Patients with perforation in the macroscopic and pathological findings of the specimen were excluded from the analysis (=AAST Grades 3,4,5).
Statistical analysis
The demographic characteristics and preoperative CT scan findings of the gangrenous appendicitis and non-gangrenous appendicitis groups were compared. Categorical variables were presented as numbers with percentages and compared using the chi-square test. Continuous variables were presented as medians with ranges and compared using the Mann–Whitney U test. Univariate and multivariate analyses of the predictive factors of gangrenous appendicitis were performed via a logistic regression analysis. Variables that were found to be significant in the univariate analysis were included in the multivariate analysis. The cutoff value for continuous variables was determined via a receiver operating characteristic (ROC) curve analysis. Finally, the scores were classified into three categories, and the probability of gangrenous appendicitis for each category was evaluated. A two-sided P value of <0.05 indicated statistically significant difference. All statistical analyses were performed using JMP version 12 (SAS Institute, Cary, NC, USA).
Results
Clinical characteristics of the participants
During the study period, 171 (56.6%) of 302 patients who underwent appendectomy were included in this analysis (Fig. 3). Patients with perforation, chronic, tumor, and appendicitis with periappendicular abscess were excluded. The sample size originally calculated based on a complicated acute appendicitis prevalence of at least 20% with 95% confidence interval (CI) and a 6% margin of error was met. In total, 46 (27%) patients presented with gangrenous appendicitis (=AAST Grade 2) and 125 (73%) presented with non-gangrenous appendicitis (=AAST Grade1). Table 1 shows the differences in terms of clinical characteristics between the gangrenous appendicitis and non-gangrenous appendicitis groups. Patients with gangrenous appendicitis had a higher body temperature (BT; 37.7 °C vs. 36.9 °C, P < 0.001) and C-reactive protein (CRP) level (6.8 vs. 0.7 mg/dL, P < 0.001) than those without gangrenous appendicitis. Regarding the CT scan findings, patients with gangrenous appendicitis had a larger appendiceal diameter (13 vs. 10 mm, P < 0.001), a higher CT scan value (28 vs. 19 HU, P < 0.001), and a greater fat concentration around the appendix (93% vs. 64%, P < 0.001) than those with non-gangrenous appendicitis. Patients with gangrenous appendicitis were more likely to present with cecal mucosal edema (65% vs. 7%, P < 0.001) than those with non-gangrenous appendicitis.
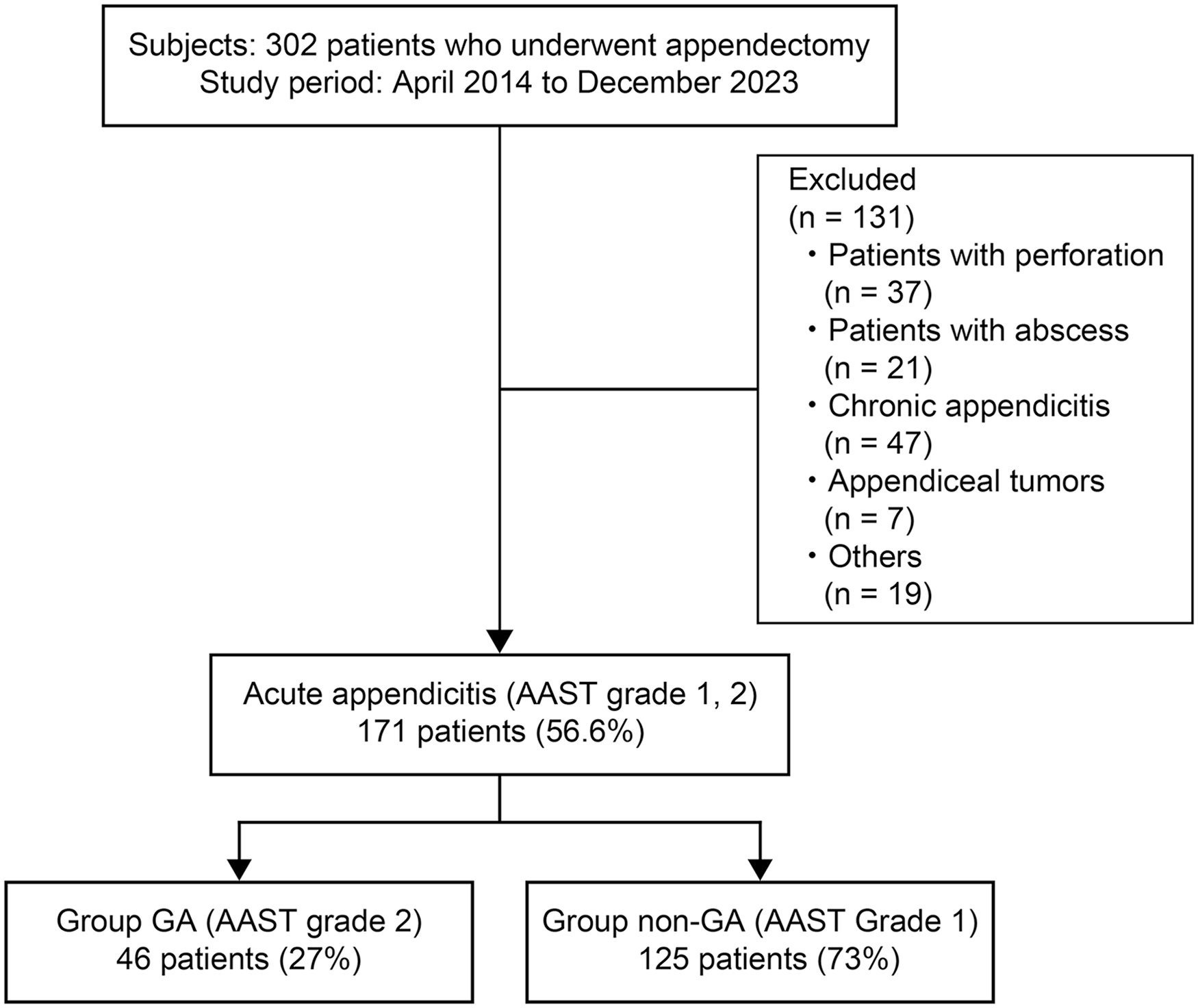
Patient flow diagram.
Comparison of clinical characteristics between gangrenous appendicitis and non-gangrenous appendicitis groups.
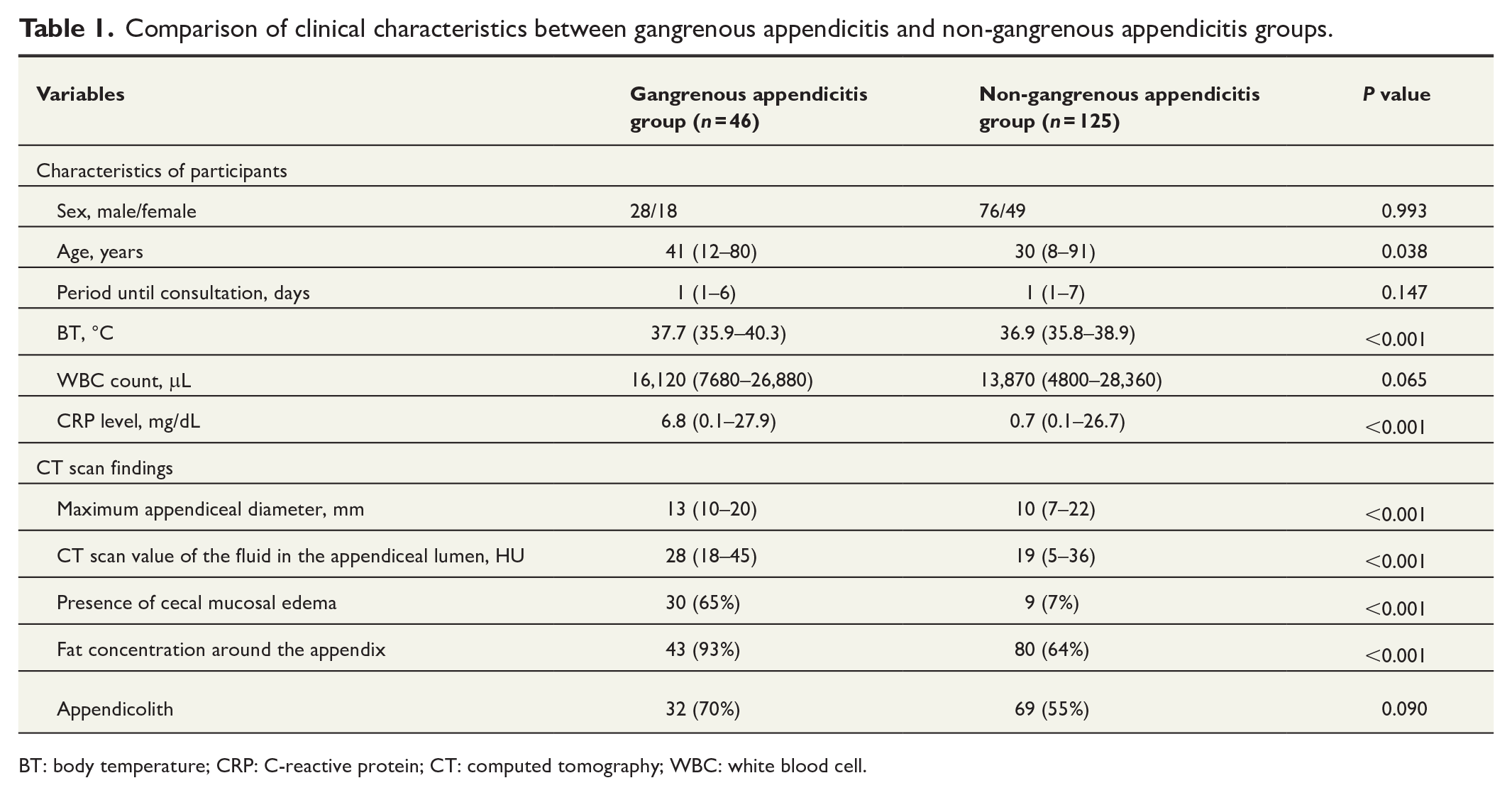
BT: body temperature; CRP: C-reactive protein; CT: computed tomography; WBC: white blood cell.
Predictive analysis of gangrenous appendicitis
For the continuous variables, according to the ROC curve analysis, the cutoff values for BT, CRP level, maximum appendiceal diameter, and CT scan value were 37.6 °C, 5.4 mg/dL, 12 mm, and 24 HU, respectively (Fig. 4). The ROC curve only for factors with P < 0.001 cutoff values was used for calculations to compare the clinical characteristics between the gangrenous appendicitis and non-gangrenous appendicitis groups. As shown in Table 2, the significant predictive factors of gangrenous appendicitis in the univariate analysis were age (relative risk [RR]: 1.02, P = 0.01), BT ≥37.6 °C (RR: 4.71, P < 0.001), CRP level ≥5.4 mg/dL (RR: 11.14, P < 0.001), maximum appendiceal diameter ≥12 mm (RR: 10.57, P < 0.001), CT value ≥24 HU (RR: 23.09, P < 0.001), presence of cecal mucosal edema (RR: 24.16, P < 0.001), and a higher fat concentration around the appendix (RR: 8.06, P < 0.001).
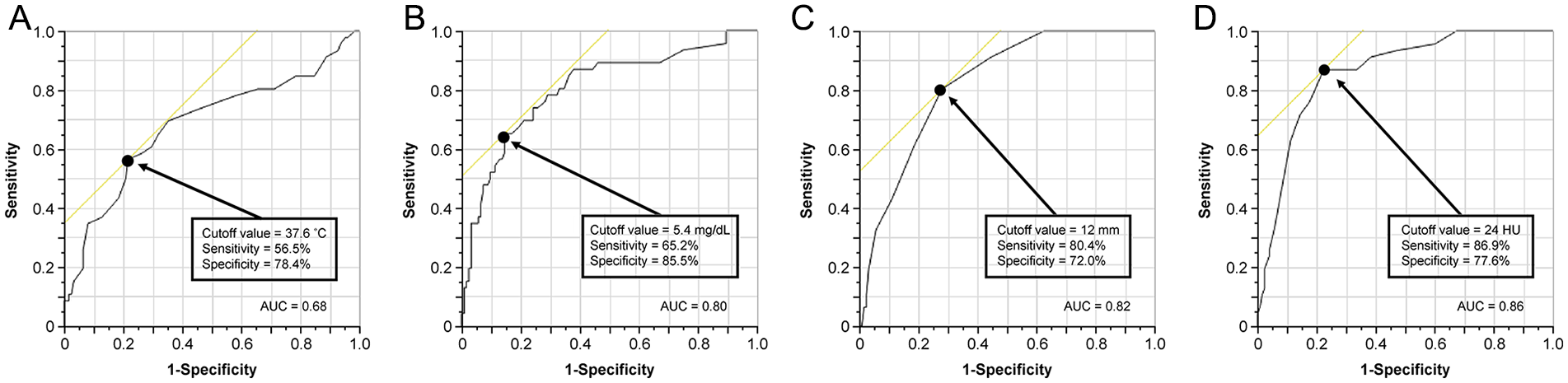
The receiver operating characteristic curve analysis. (A) Body temperature. (B) C-reactive protein. (C) Maximum appendiceal diameter. (D) CT scan value.
Gangrenous appendicitis based on a univariate predictive analysis.
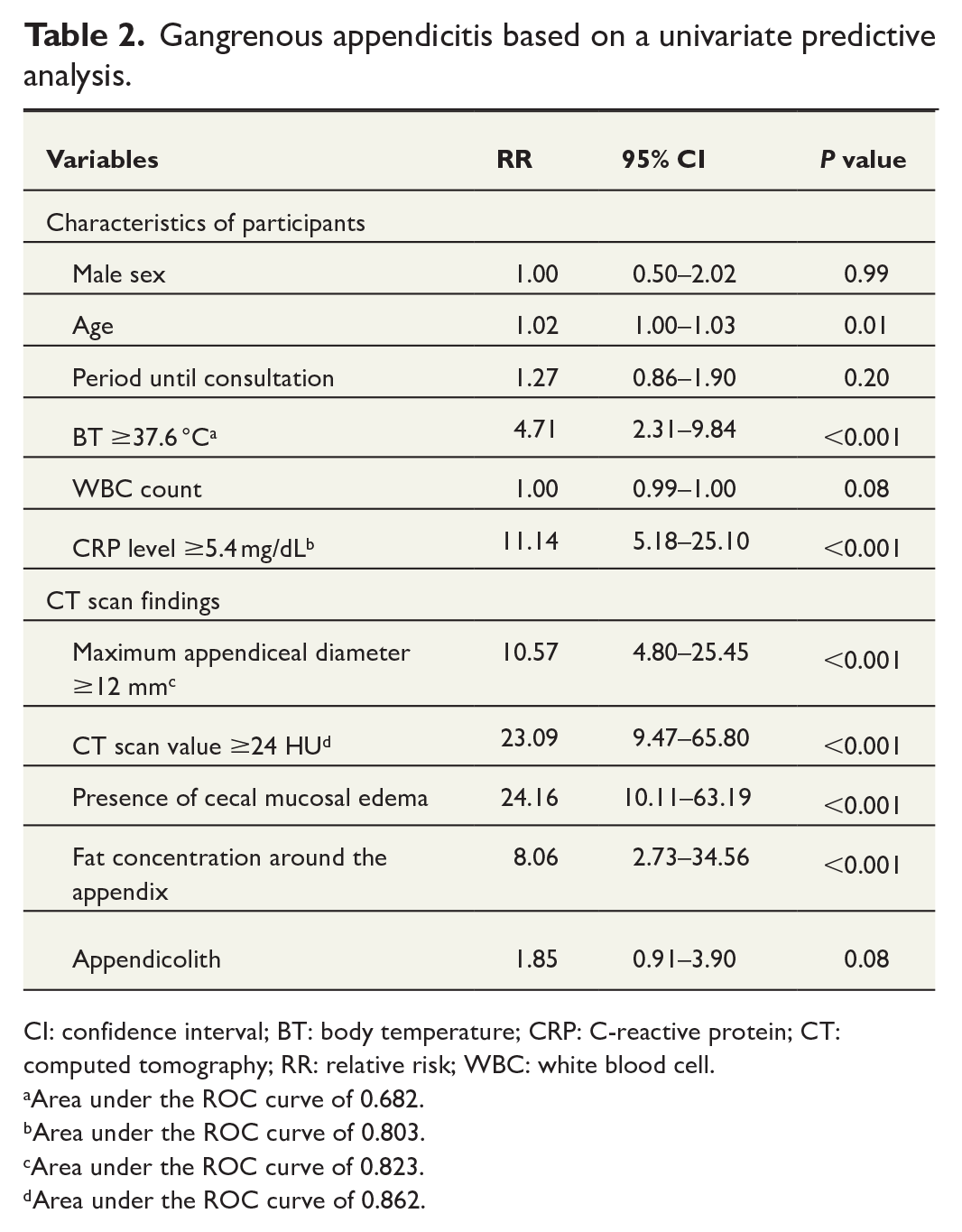
CI: confidence interval; BT: body temperature; CRP: C-reactive protein; CT: computed tomography; RR: relative risk; WBC: white blood cell.
Area under the ROC curve of 0.682.
Area under the ROC curve of 0.803.
Area under the ROC curve of 0.823.
Area under the ROC curve of 0.862.
Based on the multivariate risk analysis using these cutoff values, the independent predictive factors of gangrenous appendicitis were a CRP level ≥5.4 mg/dL (RR: 12.47, 95% CI: 3.10–67.24, P < 0.001), maximum appendiceal diameter ≥12 mm (RR: 17.49, 95% CI: 4.30–99.13, P < 0.001), CT value ≥24 HU (RR: 54.34, 95% CI: 11.14–481.56, P < 0.001), and presence of cecal mucosal edema (RR: 35.58, 95% CI: 7.31–289.41, P = 0.041; Table 3).
Gangrenous appendicitis based on a multivariate predictive analysis.
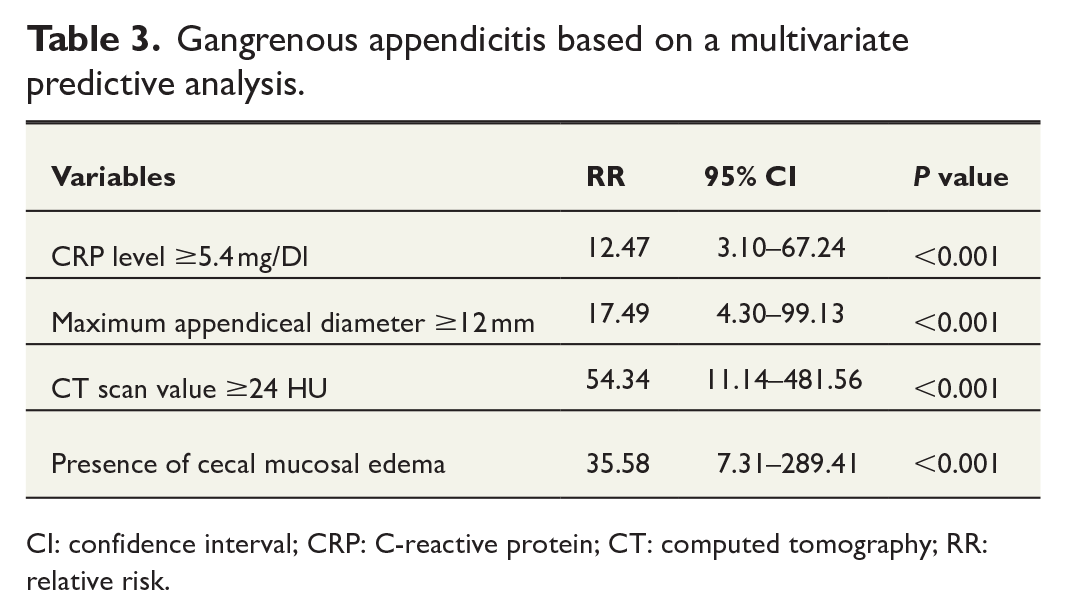
CI: confidence interval; CRP: C-reactive protein; CT: computed tomography; RR: relative risk.
The four predictive factors drawn were scored based their applicability and stratified into the low-risk group (score of 0), intermediate-risk group (score of 1, 2), and high-risk group (score of 3, 4). The probability values of gangrenous appendicitis in each category were 0%, 15%, and 97% in the low-, moderate-, and high-risk groups, respectively (Fig. 5)
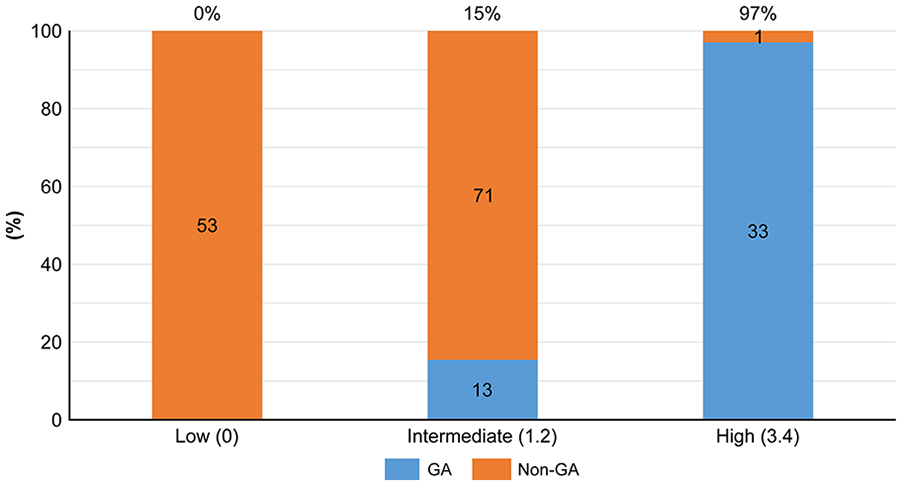
Probability-based risk categories for gangrenous appendicitis (GA).
Discussion
The incidence rate of gangreneous appendicitis was comparable between the current study and previous ones (15.2% [n = 46] vs. 4%–25%).6–10 A CT scan ≥24 HU, maximum appendiceal diameter ≥12 mm, presence of cecal mucosal edema, and CRP level ≥5.4 mg/dL were independent predictive factors of gangreneous appendicitis. Further, according to the scoring system, the risk of gangreneous appendicitis in the low-risk group was almost not significant and in such a case, conservative treatment must be actively selected. However, patients in the high-risk group were at high risk of gangreneous appendicitis and in these patients, emergency surgery should be performed. In the intermediate-risk group, most patients presented with non-gangreneous appendicitis with a low risk of gangreneous appendicitis.
The scoring system should be re-evaluated and implemented. As the clinical examination findings of acute appendicitis vary widely, CT scan is the gold standard imaging modality to reduce negative resection rates and identify complicated acute appendicitis characterized by perforation and abscess formation.11,18,19 Several studies have evaluated the use of CT scan markers to differentiate perforation from uncomplicated acute appendicitis. However, data on CT scan markers that can distinguish uncomplicated acute appendicitis from gangreneous appendicitis are limited. 20
To our knowledge, the current study is the first to show that a CT scan value ≥24 HU is an independent risk factor of gangreneous appendicitis. The CT scan values were blood-based and ≥30 HU,21,22 which was in close agreement with the results of previous studies. In gangreneous appendicitis, an increased intra-appendiceal pressure attributed to obstruction causes changes such as impaired blood flow in the appendix, insufficient blood supply to the appendiceal mucosa, and thrombus formation resulting in mucosal necrosis and bleeding in the lumen. In gangreneous appendicitis cases, blood effusion was found in the lumen of several specimens removed and could have caused the high CT values. The CT scan values of the appendicular lumen are easy to obtain and should be measured aggressively.
The normal appendiceal diameter is <6 mm,23,24 and a diameter ≥6 mm is indicative of acute appendicitis, with a sensitivity of 93% 25 and a specificity of 92%. 25 The independent risk factor of gangrenous appendicitis in this study was an appendiceal diameter ≥12 mm. A recent subgroup analysis of the APPAC II trial evaluated 583 patients with CT-confirmed uncomplicated acute appendicitis without appendicoliths. Results showed that an appendiceal diameter ≥15 mm and a BT ≥38 °C were associated with an increased risk of failed treatment with first-line antibiotics. 26 In a retrospective study of 81 patients who received nonoperative management of uncomplicated acute appendicitis, an appendiceal diameter ≥13 mm was associated with a higher risk of treatment failure with antibiotics alone in a logistic regression model adjusted for demographic characteristics, comorbidities, and admission vital signs and laboratory values (odds ratio: 17.55 [95% CI: 1.30–237]). 27 A larger appendicular diameter is associated with a more complicated illness severity where conservative therapy is not effective.
CRP is an indicator observed during the acute phase of inflammation in several diseases. Some studies have shown that elevated CRP levels are a valuable and viable marker in differentiating uncomplicated acute appendicitis from complicated acute appendicitis.28–30 In addition, Avanesov et al. 31 evaluated the use of an appendicitis severity index combined with CT scan findings and parameters such as CRP levels and white blood cell count. Results showed that the positive predictive value of the index for complicated acute appendicitis was 92%. A CRP level ≥54 g/dL was obtained as a predictor of gangrenous appendicitis in our study.
Elderly patients were more susceptible to gangreneous appendicitis, a finding consistent with those of previous studies. 32 This high risk of gangreneous appendicitis is potentially due to the developments of vascular sclerosis in the vermiform appendix and the fibrosis-related narrowing of the lumen in elderly patients. In these patients, the muscle layer is infiltrated with fat, creating a structural weakness that progresses early. 33
The presence of appendicoliths on CT was not a predictor of gangreneous appendicitis potentially because patients with perforation and abscess were excluded. Obstruction of the appendix outlet is widely recognized as the main cause of acute appendicitis. 34 Appendicoliths cause persistent obstruction of the appendix cavity, followed by increased intracavitary pressure and promotion of inflammatory process progression. These effects might lead to appendix perforation and abscess formation. 35
The current study had several limitations. First, this was a retrospective, single-center study, and there could have been potential bias in the selection of information from the medical records. We believe that further prospective multicenter investigations must be performed by dedicated associations and strict and high-volume tertiary centers to establish reliable evidence-based guidelines. Second, the sample size was relatively small. However, it met the sample size originally calculated. Third, CT scan findings were used. In some cases, ultrasonography can be utilized to diagnose appendicitis. However, CT scan is the primary imaging modality for suspected cases of acute appendicitis in clinical practice.36,37 Further, CT scan findings are an objective factor.
Conclusion
A CT scan value ≥24 HU, maximum appendiceal diameter ≥12 mm, presence of cecal mucosal edema, and CRP level ≥5.4 mg/dL were independent predictive factors of gangreneous appendicitis. Preoperative identification of patients at risk for gangreneous appendicitis in acute appendicitis may modify the treatment strategies on a case-by-case basis improving outcomes.
Footnotes
Acknowledgements
The authors thank Saki Kasuya (Medical Affairs Division Medical Information Management Office, Hanyu General Hospital Medical History Department) and Minami Kawakita (Medical Affairs Division Medical Information Management Office, Hanyu General Hospital Medical History Department) for their assistance in collecting medical data.
Author contributions
Toshiyuki Suzuki: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Writing—Original draft, Visualization, Project administration, Funding acquisition.
Akiyo Matsumoto: Data curation, Supervision.
Daisuke Sugiki: Data curation, Supervision.
Takahiko Akao: Data curation.
Hiroshi Matsumoto: Writing—Review & editing.
All authors approved the final version of the manuscript and agree to be held accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data availability statement
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study was performed in accordance with the principles of the Declaration of Helsinki and was approved by the Tokushukai Group Joint Ethics Review Committee (TGE01857-011). The need for informed consent was waived due to the retrospective nature of this study. However, an opt-out format is used.
Consent to participate
The need for informed consent was waived due to the retrospective nature of the study.
Consent to publish
The authors confirm that the research participants provided informed consent for the publication of the images in Figs 1 and ![]() .
.