
Abstract
Background:
In recent years, as new strategies have been developed, there has been a reduction of invasive interventions for prevention or treatment of ischaemic cerebral events. Furthermore, surgical treatment has been centralized to major vascular centra.
Aim:
This study analyzed registered malpractice claims to the insurance during two decades. Treatment policies (more pharmacological treatment, less intervention for asymptomatic carotid artery disease) and claiming patterns changed (Introduction of Patient Safety Act 2011).
Material and methods:
During a 20-year period (2000–2019), 184 malpractice claims related to invasive treatment of carotid artery cerebral circulatory disorders were registered in the files of the Swedish National Insurance Company. These were analyzed in two 10-year cohorts regarding the indication for intervention, the intervention itself, and the sufferers’ reasons motivating the claims and the final decision as judged by the Insurance Company’s medical and juridical experts.
Results:
The claim rate was on a 1% level (of all carotid artery interventions), no difference between the two decades. Between the first and second decade, claims concerning intervention for asymptomatic carotid artery disease decreased with 26%. In 51% of the claims, the damage was considered avoidable and the claimants were compensated for their financial losses. Motor nerve lesions were compensated for in 78% and stroke in 40%. Thrombolysis as a claimed procedure increased from 2 to 10 between the periods.
Conclusion:
During a 20-year period, negligence claims after interventions for asymptomatic carotid artery disease or manifest carotid artery cerebral ischemia were stable at a 1% level of all interventions. The compensation rate was around 50%. Dominating injuries to be claimed and compensated for were perioperative motor cranial nerve injuries and postoperative stroke. Despite changes in treatment policy, the claim and compensation rate were stable.
Research letter
In Sweden, the Patient Insurance Act can give financial compensation to patients with avoidable treatment-related injuries. In this retrospective observational registry study, claims due to clinical negligence after carotid interventions were analyzed (Regional Ethics Committee, University of Uppsala 2018/015). Negligence claims to the Swedish National Patient Insurance Company (Löf) between years 2000 and 2019 were registered (ICD-10-SWE-codes I65.2, I65.3, I65.8, I63.0, I63.1, I63.2, and procedure codes related to these diagnoses). Background data (sex, indication, procedure, postoperative stroke/mortality) were extracted from the Swedish Vascular Registry (Swedvasc).
During period A, 8885 carotid interventions were registered, of which 18.4% were performed for asymptomatic disease. During period B, the figures were 9235 and 9.8%, respectively, showing 48% reduction for asymptomatic disease. The highest annual number of interventions, 1180, were performed in year 2009. Then, a continuous decline was observed (792 in 2019).
Altogether, 203 claims were recorded, 19 being irrelevant to carotid disease leaving 184 for the analysis. There were 90 claims in period A (2000–2009) and 94 in period B (2010–2019) (Table 1). Most patients with claims (94%) were treated in central hospitals. In all, 112 (61%) claimants were between 61 and 80 years old (mean age 64 ± 11 years). Symptomatic disease dominated as treatment indication in 147 claimants (80%). In 128 patients (70%), endarterectomy was performed, bypass in 12 (7%) and thrombolysis in 12 (7%). Two patients in period A and 10 patients in period B had undergone thrombolysis that was the reason for the negligence claim. Six patients underwent stenting (period B); none was compensated. Motor nerve lesions in 59 (35%) and stroke in 65 (39%) were the most common reasons for claiming. There was no difference between the periods. Sixty-four (39%) of the claims were considered as non-avoidable and 11 (6%) as not contributing to the consequences of negligence. In 92 (50%) of the claims, the damage was considered avoidable; no difference between the periods was observed. The claimants with avoidable damages were financially compensated. In 28 patients (7%), a delay in diagnosis and/or treatment motivated compensation. Motor nerve lesions were compensated for in 78% (46/59) and stroke in 38% (25/65). There were 4 glossopharyngeal injuries (all compensated), 9 hypoglossal (five compensated), 40 recurrent nerve injuries (35 compensated), 2 Horner’s syndrome (one compensated). The judgment of avoidability by independent experts is the explanation why all nerve injuries were not compensated. There were 17 claims for postoperative bleeding, eight with stroke. Four patients with intracerebral hemorrhage received compensation.
Patients’ reasons for filing a claim in 184 claims related to carotid artery intervention, whereof 92 were economically compensated (= avoidable), no difference between the periods (p = 0.11).
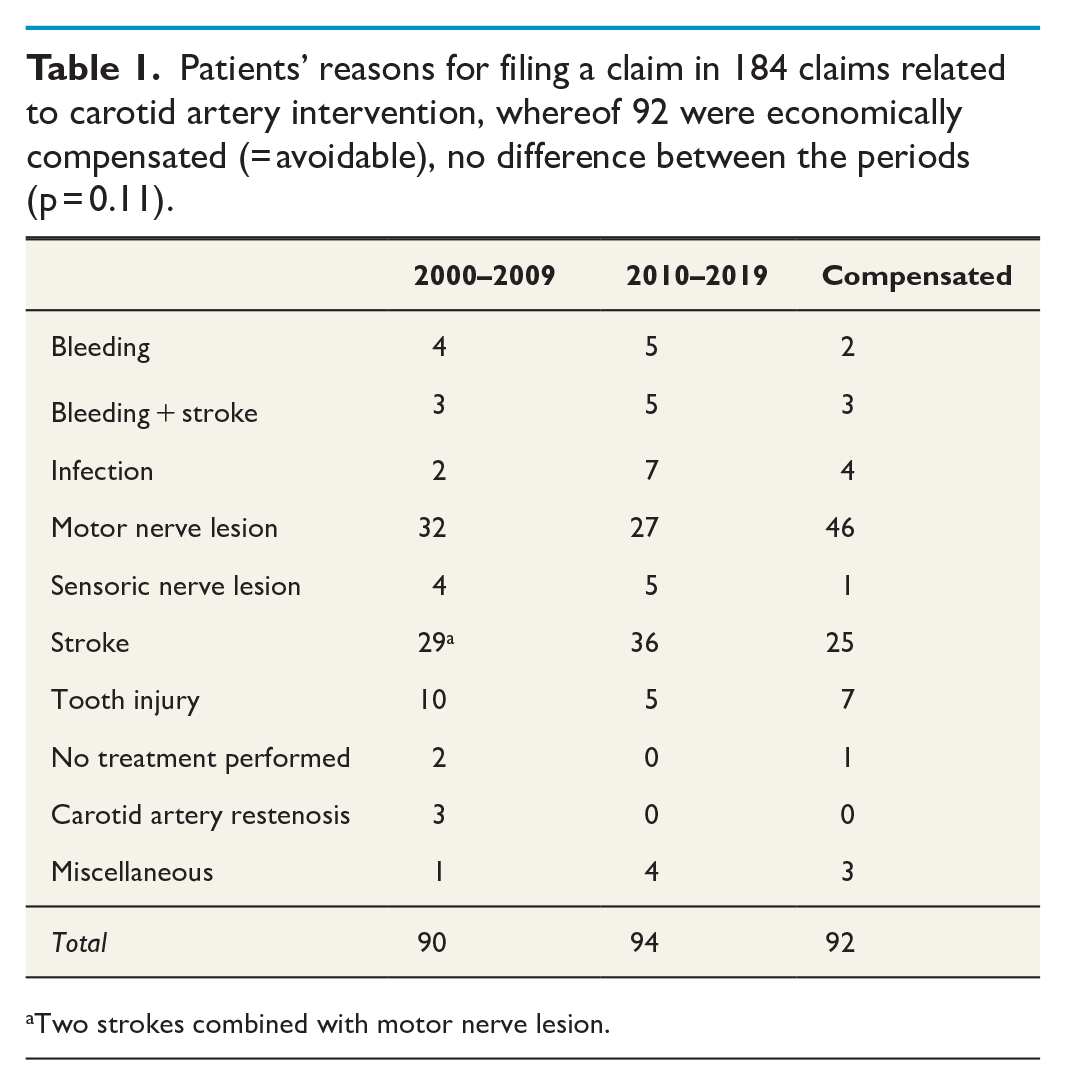
Two strokes combined with motor nerve lesion.
In Sweden, the question of economic compensation is dealt with separately from the legal system analyzing if there has been a treatment mistake, which is an important advantage. The magnitude of economic compensation is based on not only financial losses due to disability, but also pain and discomfort. Varicose vein surgery and carotid surgery claims dominate for claiming in vascular surgery. The compensation rate is higher than in a recent Finnish study. 1 Patient-reported claims do not give the correct incidence of complications, but probably more serious events are reported. Over this 20-year period, the number of claims was stable despite the significant reduction in carotid interventions. One likely explanation is the introduction in 2011 of the Patient Safety Act, which has resulted in an increase of filed claims to Löf in most medical fields. The two periods were similar regarding background data and reported claims. One difference is the more frequent use of thrombolysis. Another difference is the decrease in surgery for asymptomatic disease, reflecting recent recommendations to use antiplatelet prevention. 2 With adequate anatomical knowledge, intraoperative cranial nerve injuries should be avoidable and are not acceptable. Most cranial nerve injuries are caused by traction/pressure and are reversible.3,4 It seems reasonable to keep carotid intervention in high-volume clinics with vascular specialists 5 and other competent specialists: investigations, anesthesiology, intensive care, pharmacological prevention, and treatment, and so on.2,6
The decreasing number of carotid surgical interventions after 2009 will likely lead to a future decrease in insurance claims, but this hopeful assumption has to be further analyzed.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.