
Abstract
Background and aims:
Acute appendicitis is the most common surgical emergency worldwide. Obtaining a correct diagnosis and timely management can be challenging even in modern medicine. Hence, appendicitis is still considered a “high-risk” diagnosis for litigation and claims of malpractice. Few studies have investigated the pattern and outcome of claims for appendicitis in a contemporary universal health care system. The aim of this study is to analyze compensation claims related to the investigation and treatment of appendicitis in Norway.
Methods:
An observational study based on claims from the Norwegian System of Patient Injury Compensation (NPE) from 2005 to 2023. Population rates of appendicitis treatment were obtained from the Norwegian Patient Registry (NPR; data from 2016 to 2023) and Statistics Norway (SSB).
Results:
Altogether 207 compensation claims were filed for appendicitis and 56 (27%) received compensation. The probability of receiving compensation was not influenced by age, gender, or geographical location. The most common reasons for compensation granted were delayed diagnosis (n = 25, 45%) and delayed treatment (n = 5, 9%). The most common reasons for the 151 (73%) denied claims were predictable complication (n = 48, 32%) and condition caused by an unrelated disease (n = 40, 26%). Out of the 59,450 appendectomies performed, 96 claims were filed to NPE, giving a claim rate of 0.16% or 1 claim for every 620 appendectomies. For the entire study period, there was a total payout of 27.2 mill NOK (approximately 2.4 mill EUR) with a mean of 460,000 NOK (approximately 40,000 EUR) and a median of 75,000 NOK (approximately 6,600 EUR) per claim.
Conclusion:
In acute appendicitis, about a quarter of claims are compensated due to malpractice. More than half of the approved claims involved delays in diagnosis or treatment, which can be related to the clinical challenges of diagnosing appendicitis.
Context and relevance
Acute appendicitis is the most common emergency surgical condition and remains a clinical challenge even in modern medicine. Malpractice claims regarding appendicitis are mainly due to diagnostic errors and technical issues related to surgery. Compensation claims in Norway are relatively low with a claim rate of 0.16%, and with no significant geographic or demographic influence on outcomes. Of the 207 claims filed in a 20-year period, 56 (27%) of the claims were approved, while 151 (73%) were denied compensation. The most common reasons for compensation granted were delayed diagnosis or treatment, or technical faults. Advancements in appendicitis diagnostics have the potential to optimize clinical management and mitigate the risk of future malpractice litigation.
Introduction
Acute appendicitis is the most common emergency surgical condition worldwide, with a lifetime incidence of 6.7%–8.6%.1,2 In 2019, there were 17.7 million new cases globally, and 1.5 million disability-adjusted life years (DALYs) were attributed to appendicitis. 3 Appendicitis thus represents a significant burden to the health care systems globally. While there has been a growing focus on non-operative treatment in recent years,4,5 the vast majority of patients in high-income countries still undergo surgery, primarily laparoscopic appendectomy. As a result, appendectomy remains one of the most commonly performed surgical procedures around the world.
Diagnosing acute appendicitis remains a challenge, 6 and the growing emphasis on conservative treatment has further complicated the process. A key difficulty lies in distinguishing between uncomplicated and complicated appendicitis, 7 the latter requiring surgical intervention. In Norway, diagnostic and treatment protocols vary between the hospitals, 8 reflecting the lack of a standardized national approach. Internationally, consensus guidelines for diagnosis rely largely on moderate- to low-quality evidence, contributing to variability in clinical practice. 6 In the Western world, appendicitis is considered a “high-risk” diagnosis in malpractice claims, with diagnostic errors being the leading cause of litigation.9–13
Another frequent cause of litigation following appendectomy is technical error, such as inadequate removal of the appendix or perforation of adjacent organs.14,15 These complications are particularly associated with the laparoscopic technique—a surgical approach that offers numerous benefits to patients, such as faster recovery and reduced scarring but presents greater challenges for inexperienced surgeons. Appendectomies are often performed as training procedures for surgical trainees, and while this practice is generally considered safe,16,17 a learning curve is inevitable. Surgical outcomes are expected to improve as the surgeon gains experience. 18 Although laparoscopic appendectomy is regarded as a technically straightforward procedure, anatomical variations, patient-specific factors, and the severity of inflammation can unexpectedly increase its complexity.
In Norway, most malpractice claims related to economic compensation are processed through the Norwegian System of Patient Injury Compensation (NPE). This system allows patients to file claims without incurring case management costs or requiring their own attorney. While Norwegian law permits direct lawsuits against practitioners and hospitals, such lawsuits are extremely rare.
The high volume of appendectomies performed, along with ongoing advancements in diagnostic methods and treatment strategies for appendicitis, underscores the importance of examining malpractice claims related to this procedure. Changes in clinical practice, including the increasing use of imaging techniques and a growing preference for non-surgical management in select cases, have influenced how appendicitis is diagnosed and treated. Understanding malpractice claims in this context can provide valuable insights into areas of potential medical error, patient safety concerns, and the impact of evolving guidelines on surgical outcomes. Norway’s unique malpractice claim system, managed through the NPE, offers a rare opportunity to analyze nationwide data on patient injuries and compensation claims. Unlike legal systems where litigation costs and attorney fees can be barriers to filing claims, the NPE ensures accessibility for all patients. This centralized approach allows for a comprehensive overview of malpractice trends.
This study aims to analyze compensation claims related to the investigation and treatment of appendicitis in Norway. It seeks to examine the influence of age and gender, identify potential geographical differences, and explore the reasons why claims are either approved or denied.
Methods
Study ethics
Approval by the Regional Ethics Committee (REK) was not required since all the data were based on already anonymized records from the NPE and on publicly accessible data from the Norwegian Patient Registry (NPR) and Statistics Norway (SSB).
Study setting
The Norwegian health system is founded on the principles of universal access and divided between primary and specialist health care. There are approximately 40 hospitals in Norway performing acute surgery, all of which are public. The national government is responsible for hospital care, which are handled through four Regional Health Authorities (RHAs): North, Mid, South-East, and West. 19
NPE is a government agency under the Norwegian Ministry of Health and Care Services (npe.no). Patients who believe they have suffered harm due to errors or omissions in the healthcare system can file a complaint with NPE free of charge. To qualify for compensation, a patient must have experienced either a financial loss of at least 10,000 NOK or a permanent medical disability of at least 15%. NPE is a service to all patients regardless of whether they have been treated by a general practitioner, at an emergency room, at a public hospital, or at a private hospital. The NPE system is based on the no-blame principle, where the complaint claims are handled outside the legal system and the NPE compensates the costs. 20 The legal system in Norway also gives patients the right to sue practitioners and/or hospitals directly.
Study design
This observational study is based on national data within a universal health system and based on complaints filed to NPE. As an observational cohort study, we have used the recommendations from the STROBE guidelines where applicable. 21
Claims data
The data from NPE cover the claims decided in a 20-year period from 2005 to 2024. As a result of the NPE guidelines, the claim can be filed up to 3 years after the patient (or next of kin) is realizing that an alleged injury has occurred.
Data to assess population statistics for procedures and diagnostic codes
The NPR publishes data on the number of diagnoses and procedures, and these data were used to register activity. These data are only openly available for the time period 2016–2023. Hence, patient administrative data are limited to this period. Population data from Statistics Norway (SSB) were used to estimate population data from each geographical region.
Study data retrieval
Data on malpractice claims
Data from all claims received by the NPE from 2005 to 2024 regarding diseases of the appendix defined by ICD codes 22 were collected: K35 Acute appendicitis, K36 Other appendicitis, K37 Unspecified appendicitis, and K38 Other diseases of the appendix including subgroups (Supplementary information; Table S-1). The data were provided in an anonymized version, and no patient sensitive data were included. The claims were analyzed for the following data: (1) overall number of complaints, patient demographics, age and sex, and number of complaints resulting in a compensation; (2) geographical region (Northern, Middle, South-Eastern, and Western health trust); (3) reasons for compensation granted; and (4) reasons for compensation denied.
Population data
NPR data are openly available for the period from 2016 to 2023, and these were collected on ICD codes on diseases of appendix and Classification of Surgical Procedures (NCSP) codes 23 regarding appendectomy: JEA00 Appendectomy, JEA01 Laparoscopic Appendectomy, and JEA10 Appendectomy with drainage.
The NPE data give an overview of the payout for the period.
Study groups
The population density and thus the population base vary between the four RHAs, and the population base also varies somewhat between somatic and psychiatric health services between the regions. Analyzing compensation claims in relation to the four health regions, data from SSB was obtained to define the population number for somatic healthcare for each of the four regions.
Definitions for claim outcomes with reasons for approval or denial
The NPE data provide a short description on the treatment the patient has received and the injury that the patients claim to have suffered, as well as a short description of the expert’s assessment. The conclusion on whether compensation has been granted or denied is also included. Using these short descriptions, the causes were retrospectively categorized and thematically analyzed by the authors in order to find overarching reasons for both granted and denied compensation claims.
The causes for compensations being granted were categorized into four overarching main groups: Delayed diagnosis, Delayed treatment, Technical issues, and Postoperative/Follow-up complications.
Compensations being denied were categorized into six groups: No delayed diagnosis, No injury proven, Injury without financial loss or permanent medical disability, Predictable complication, Condition attributed to the underlying disease (not treatment), and Condition caused by an unrelated disease.
Statistical methods
Statistical analyses were done by SPSS v.26.0.0.1 (IBM SPSS; Armonk, NY, USA). Demographic data were analyzed using descriptive statistics. Group comparisons were performed using the Chi-square test or Fisher’s exact test where applicable.
All statistical tests were two-tailed, and a P < 0.050 was regarded as statistically significant.
Results
During the study period, the NPE handled 207 compensation claims related to appendicitis, and out of these, 56 (27%) were granted compensation. The number of cases varied from 4 to 19 per year with a median of 9 cases (Fig. 1). Neither gender nor age group appeared to influence the likelihood of receiving compensation (Fig. 2).
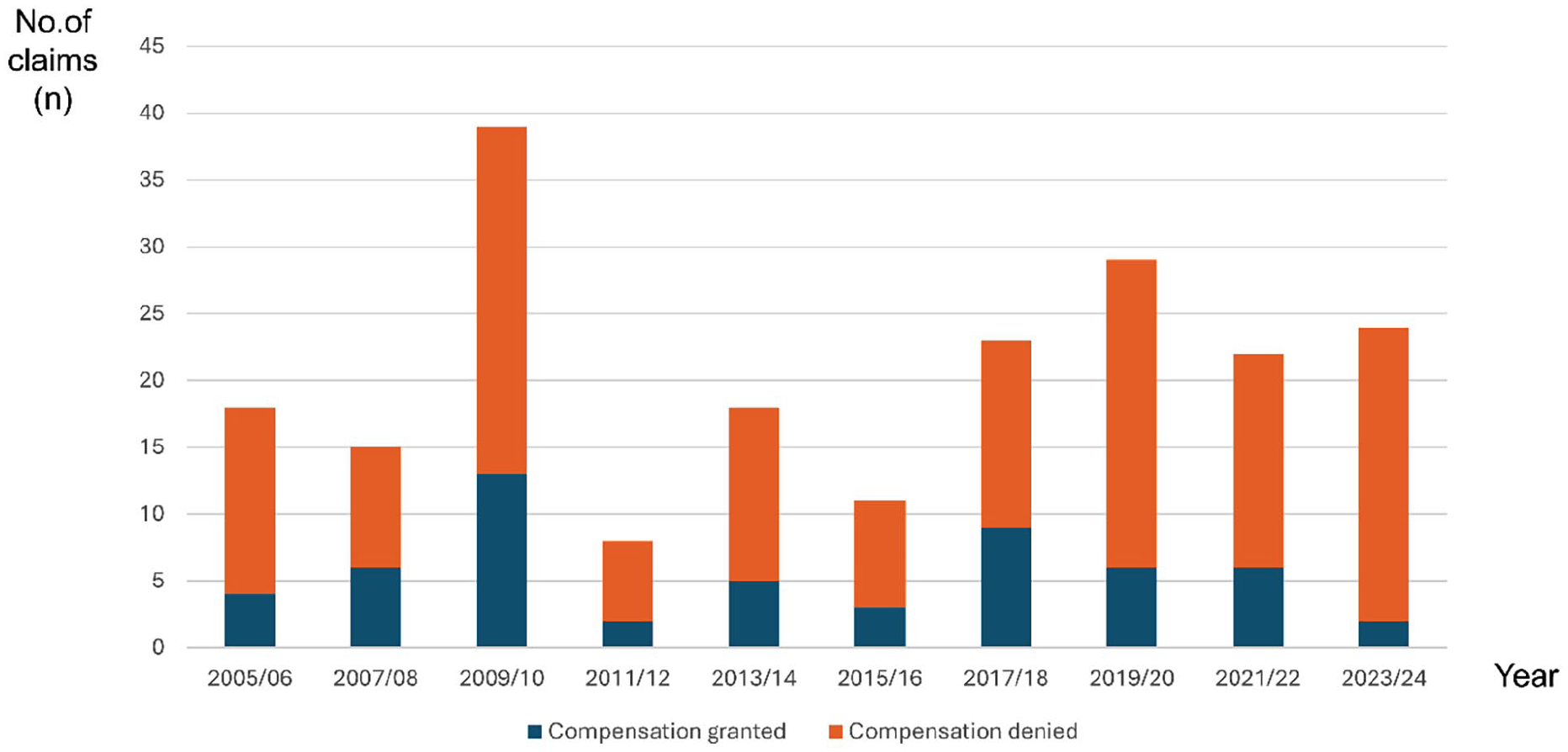
Number of cases granted/denied for each 2-year period.
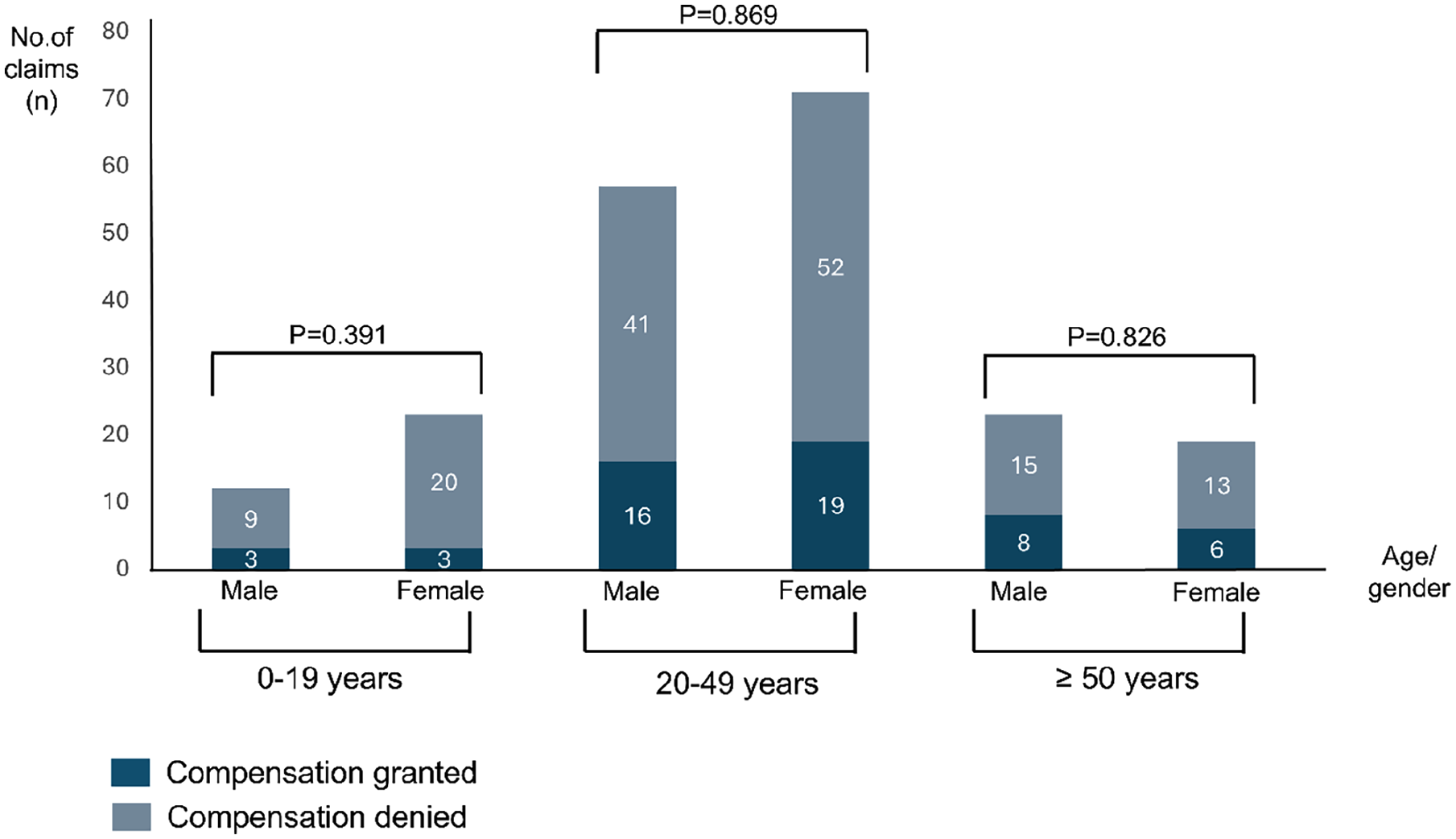
Compensation granted/denied in relation to age and gender.
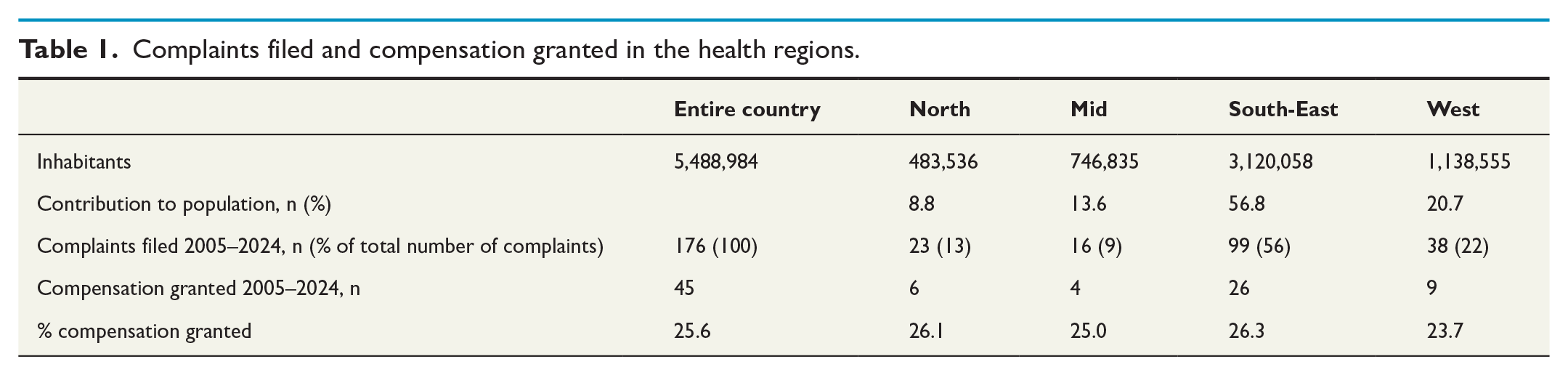
Of the 207 complaints, 176 (85%) were associated with one of Norway’s four specialist healthcare regions (North, Mid, South-East, and West). After adjusting for population size in each region, no differences were found in either the number of claims filed or the number of compensations granted (Table 1).
Complaints filed and compensation granted in the health regions.
The remaining 31 (15%) of the complaints were associated with either primary healthcare (n = 12), emergency rooms outside hospital (n = 16), or private healthcare (n = 3). Out of these, 11 of the claims (35%) were granted compensation, while 20 (65%) were denied compensation.
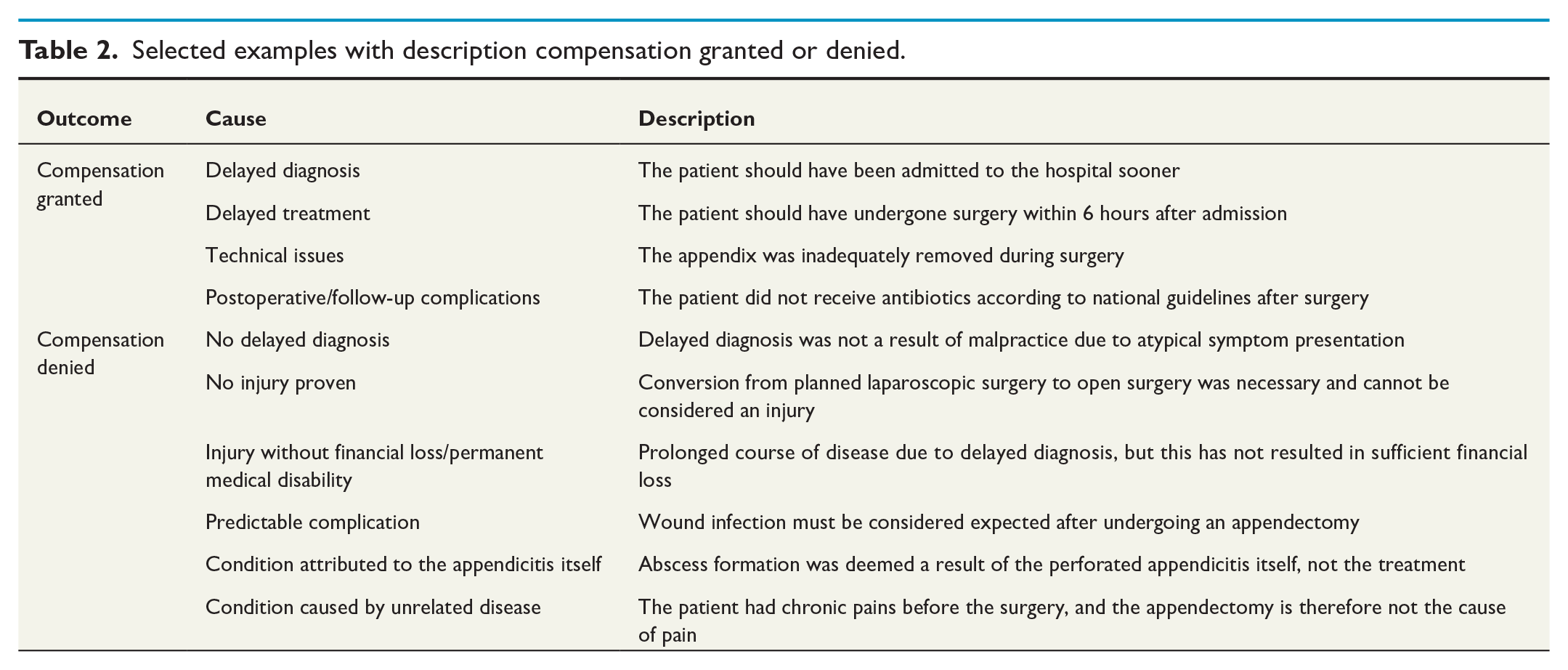
The causality for compensation being granted or denied is presented in Fig. 3 with examples given in Table 2.
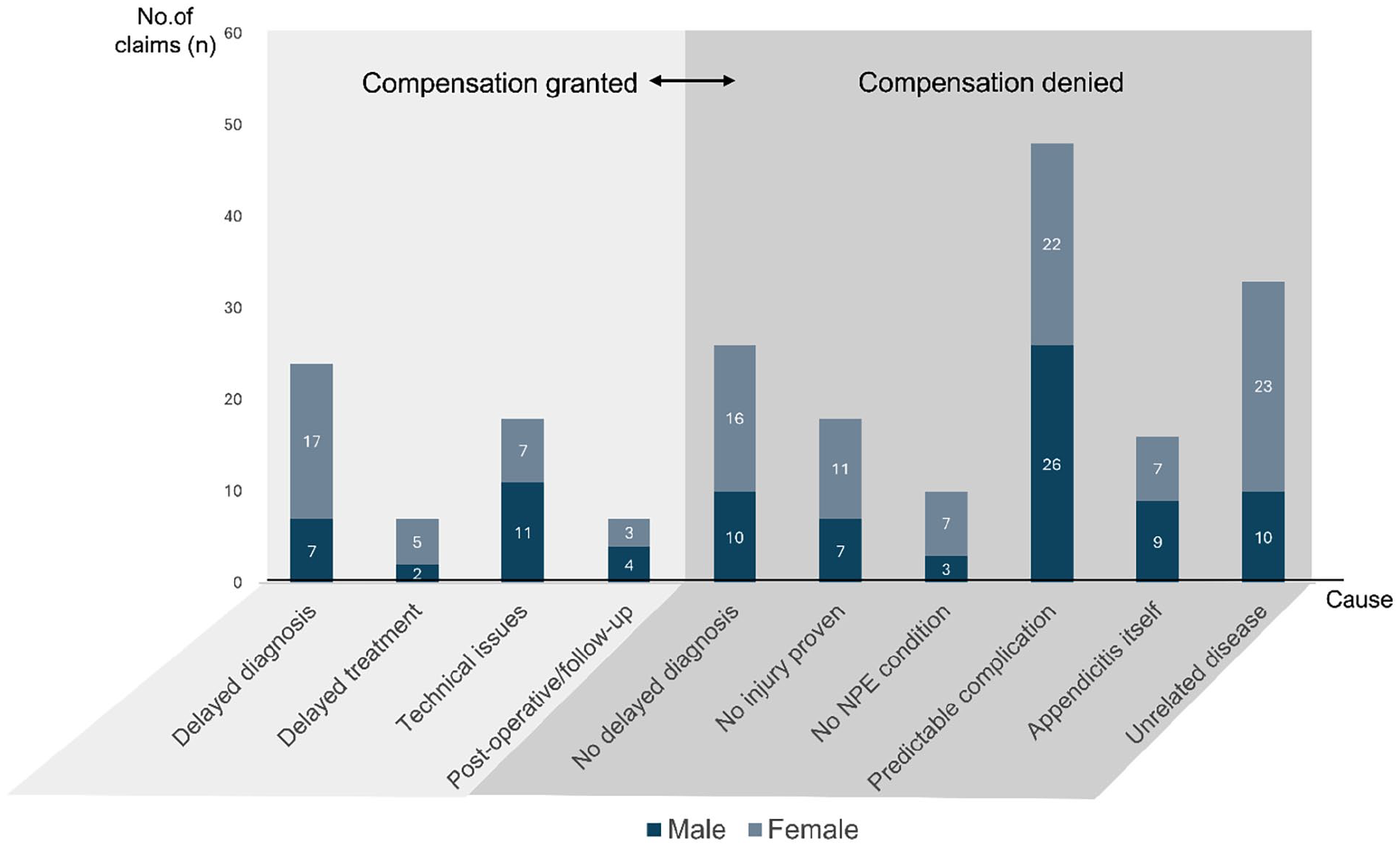
Claims with compensation granted and denied.
Selected examples with description compensation granted or denied.
Incidence of appendicitis and rate of appendectomy in the population 2016–2023
A total of 59,503 diagnoses of appendicitis and other diseases affecting the appendix vermiformis were recorded in Norwegian hospitals. Some individuals may have received multiple diagnoses, making it difficult to determine the exact number of affected patients. However, the most frequently assigned diagnosis was recorded 35,022 times, indicating a high total patient count.
During the same period, 59,450 appendectomies were performed, meaning that each year 0.14% of the population undergo an appendectomy.
In this period a total number of 96 claims were filed to NPE, giving a complaint rate of approximately 0.16% per appendectomy performed. For the entire study period (2005–2024), the total payout for the claims where compensation was granted was 27.2 mill NOK (approximately 2.4 mill EUR) with a mean of 460,000 NOK (approximately 40,000 EUR) and a median of 75,000 NOK (approximately 6600 EUR) per granted claim. Figures are not adjusted for changes in money value.
Discussion
Over a 20-year period, 27% of the complaints filed with the NPE resulted in compensation. Most of these claims were attributed to delayed diagnosis or treatment, as well as technical issues. Neither demographic factors nor geographical variations appeared to influence the likelihood of receiving compensation. Among the denied claims, about one-third involved patients who were found not to have suffered any injury, while another third was attributed to predictable complications. Despite the high number of appendectomies performed, the overall number of complaints is 207 in 20 years.
No differences were found between the four health regions, likely because each includes both small and large (university) hospitals, and data on individual hospitals were unavailable.
In more than half of the claims where it was concluded that an injury had occurred (i.e. where compensation was granted), the reason for injury was either delayed diagnosis (43%) or delayed treatment (13%). This is in accordance with several other studies,12,14 and diagnostic error remains the most common cause of litigation. 9 The challenges of diagnostics and the varying routines for diagnostics and treatment may at least in part contribute to both delayed referral to hospital and to in-hospital delay, and more robust guidelines may be an important way of improving the diagnostics.
In four of the claims, the expert defined a specific recommended time frame for the procedure, stating that the surgery should have been performed within 6 h. It is not informed whether these patients had an uncomplicated or a complicated appendicitis. International consensus states that “in-hospital delay up to 24 h is safe in uncomplicated acute appendicitis,” 6 and this has recently been supported by a Nordic trial. 24 This does not apply to complicated appendicitis which should be operated sooner. However, as guidelines regarding appendicitis and appendectomy, to a great extent, are based on rather weak recommendations, this could potentially open for subjective assessments by the expert, and thus may lead to unwanted variation in the management of the claims.
The second most common reason for granted compensation was technical error, with the primary causes being inadequate removal of appendix or perforation of an adjacent organ. The NPE data does not provide information on the surgeons’ experience level, making it impossible to draw definitive conclusions on whether trainee participation may have contributed to the technical errors.
An important finding of this study is that the number of complaints filed to NPE regarding appendicitis is 0.16% of all appendectomies performed. This probably reflects that appendicitis is a disease with low mortality rates (0.1% for uncomplicated appendicitis, 5% for complicated appendicitis 25 ) and relatively low morbidity, and is in accordance with comparable countries such as England. 15
Limitations
Since NPE is based solely on patient-reported claims, it captures only those cases where individuals actively choose to file a claim. However, there are no available data on the total number of patients who experience potential harm but do not report it. This gap limits the ability to assess the true incidence of medical errors or dissatisfaction and may lead to an underestimation of the scope of the problem in healthcare quality and safety assessments. In fact, previous research has demonstrated that the majority of patients suffering a medical injury does not sue. 26 The number of actually suffered injuries may therefore be substantially higher than the number of filed complaints indicates.
Another weakness of this study is that the data provided by NPE provides a limited information on causality, and if further in-depth analysis of each claim should be performed, this would require a written consent from every single patient.
As the data are from Norway, this may limit the generalizability in countries with a different health system and not least with a different compensation system. However, there is no reason to believe that the results differ from comparable countries. The purpose of the study was to highlight areas that could be available for improvement and one important deduction is that better and more robust guidelines could lead to improvements. This should be of universal interest to those involved in diagnosing and treating appendicitis.
This study provides a comprehensive overview of malpractice claims related to appendicitis in Norway, highlighting key factors influencing compensation outcomes. Despite the high number of appendectomies performed, the complaint rate remains low. The findings underscore the importance of standardized diagnostic and treatment guidelines to minimize delays and improve patient safety. Further research and enhanced transparency in hospital data could facilitate benchmarking and quality improvement. These insights may be valuable not only in Norway but also in other healthcare systems aiming to optimize appendicitis management and reduce malpractice claims.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969251363823 – Supplemental material for Claims filed after perceived malpractice in management of acute appendicitis: An observational nationwide cohort study
Supplemental material, sj-docx-1-sjs-10.1177_14574969251363823 for Claims filed after perceived malpractice in management of acute appendicitis: An observational nationwide cohort study by Benedicte Skjold-Ødegaard, Geir S. Braut, Hege L. Ersdal and Kjetil Søreide in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors would like to thank Mette Willumstad Thomsen, senior advisor in NPE, for providing data for the study.
Authors’ note
Malpractice claims regarding appendicitis are mainly due to diagnostic errors and technical issues related to surgery. Advancement in diagnostics has the potential to mitigate the risk of malpractice litigation.
Author contributions
All the authors have contributed to the conception and design of the study; acquisition of data; analysis and interpretation of data; drafting the article and revising it critically for important intellectual content; and the final approval of the version to be submitted.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.S. has done occasional work for NPE as an expert witness or judicial work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: B.S.-Ø. has a PhD scholarship from the University Fund Rogaland, Department of Gastrointestinal Surgery at Stavanger University Hospital and Department of Surgery at Haugesund Hospital.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.