
Abstract
Background:
There is controversy regarding which is the best reconstruction technique after the pancreatoduodenectomy. Currently, there are no studies comparing the three most frequent reconstruction techniques: Whipple + Roux-en-Y gastrojejunostomy (WRYGJ), pyloric-preserving + Billroth II (PPBII), and Whipple + BII (WBII).
Methods:
Between 2012 and March 2023, 246 patients underwent pancreaticoduodenectomy with the following type of reconstruction techniques: (1) WRYGJ: 40 patients; (2) PPBII: 118 patients; and (3) WBII: 88 patients. A retrospective comparative study among these groups was performed.
Results:
No significant differences were found among the groups regarding duration of the surgery, the blood volume transfused, or caliber of the Wirsung duct. The size and types of tumors, the degree of differentiation and tumor invasion of the peripancreatic tissue, vascular and neural structures, and lymph nodes were similar among the groups. The rate of R0 resection was lower in WBII (62.5% [55/88]) than in WRYGJ (75% [30/40]) and PPBII (72% [85/118]), but statistically insignificant among the groups (p = 0.232). The incidences of relevant B/C postoperative pancreatic fistula (POPF) were similar among the groups: 7.5% (7/40) in WRYGJ, 17% (20/118) in PPBI, and 26.2% (23/88) in WBII (p = 0.292). In addition, the incidence of B/C delayed gastric emptying (DGE) was higher in WBII (27.3% [24/88]) than in WRYGJ (20% [8/40]) and PPBII (19.5% [23/118]) but statistically insignificance among the groups (p = 0.381). The incidence of medical and surgical complications, intensive care unit and hospital stays, morbimortality at 90 days, and 5-year survival were similar among the groups. Multivariate analysis revealed that POPF grade B/C was a risk factor for DGE grade B/C (odds ratio (OR) = 9.903, 95% confidence interval (CI) = 4.829–20.310; p < 0.001), and a <3-mm Wirsung duct was a risk factor for POPF (OR = 3.604, 95% CI = 1.791–7.254; p < 0.001).
Conclusion:
No technique was superior to the others. Only relevant POPF B/C was a risk factor for DGE B/C, and <3 mm Wirsung for a POPF.
Keywords
Context and Relevance
Regarding the controversy over the best reconstruction technique after pancreatoduodenectomy, we compared three reconstruction techniques (classical Whipple with isolated Roux-en-Y gastrojejunostomy (WRYGJ; n = 40), pyloric-preserving with B-II (PPBII; n = 118), and Whipple with Billroth II (WBII; n = 88). No significant differences were found among the groups regarding operative time, blood transfusion, tumoral invasion of lymph nodes, R0, hospital stay, 90-day morbimortality, and long-term survival. Relevant postoperative pancreatic fistula (POPF) was a risk factor for relevant delayed gastric emptying, and Wirsung duct <3 mm was a risk factor for POPF. Thus, neither reconstructive technique was superior to the other, but the prevention of POPF and the improvement in the management of pancreatojejunostomy with a <3-mm Wirsung duct could improve the results.
Introduction
Pancreatoduodenectomy (PD) has been universally accepted as therapy for pancreatic head and periampullary tumors due to the low rates of postoperative mortality in specialized centers, ranging from 0% to 3.8% in several recent series.1 –5 On the contrary, the rates of post-PD complications such as POPF, intra-abdominal abscesses, intra-abdominal hemorrhage, and delayed gastric emptying (DGE) remain unchanged. Thus, POPF is the most serious complication with an overall incidence between 19.5% and 33.5% according to several researchers.1 –3,5,6 DGE is a less severe, although it is the most frequent complication that develops in between 9.1% and 50% of patients and has been associated with a prolonged hospital stay, increased costs, and a decreased in quality of life.2,5 –8 With the objective to reduce the rate of POPF and DGE, several modifications have been performed over the classical Billroth II (BII) reconstructive technique after PD, with or without pyloric-preserving, such as the use of an isolated Roux-en-Y pancreatojejunostomy,6,9 –13 an isolated Roux-en-Y gastrojejunostomy,14 –17 and a more recently isolated Roux-en-Y draining pancreatojejunostomy and gastrojejunostomy. 18 However, the choice of the best reconstruction technique, based on achieving the lesser incidence of morbimortality and hospital length of stay, remains controversial. Therefore, many studies have been performed comparing BII versus Roux-en-Y reconstruction techniques after classical Whipple PD,14 –17,19 pylorus-preserving versus classical Whipple PD using BII reconstruction,8,20 and pylorus-preserving versus pylorus-resecting PD.21 –24
The aim of this study was to compare the three most common techniques of PD and subsequent gastrointestinal reconstruction, such as classical Whipple with isolated Roux-en-Y gastrojejunostomy (WRYGJ), pyloric-preserving with Billroth II (PPBII), and Whipple with Billroth II (WBII). To our knowledge, this type of study has not been previously reported.
Patients and methods
Study design and patient recruitment
Between January 2012 and March 2023, 262 patients underwent PD at our institution for tumors located in the pancreatic head and periampullary regions.
After the exclusion of 16 patients who underwent PD with different reconstruction techniques, a sample of 246 patients was divided into three groups according to the following PD and gastrointestinal reconstruction techniques: (1) patients with classical Whipple PD and reconstruction with Roux-en-Y gastrojejunostomy in an isolated loop (WRYGJ [n = 40; 16.3%]); (2) patients with pylorus-preserving PD and Billroth II reconstruction (PPBII [n = 118; 47.9%]), and (3) patients with classical Whipple PD and BII reconstruction (WBII [n = 88; 35.8%]). A flowchart of the patient selection process is shown in Fig. 1.
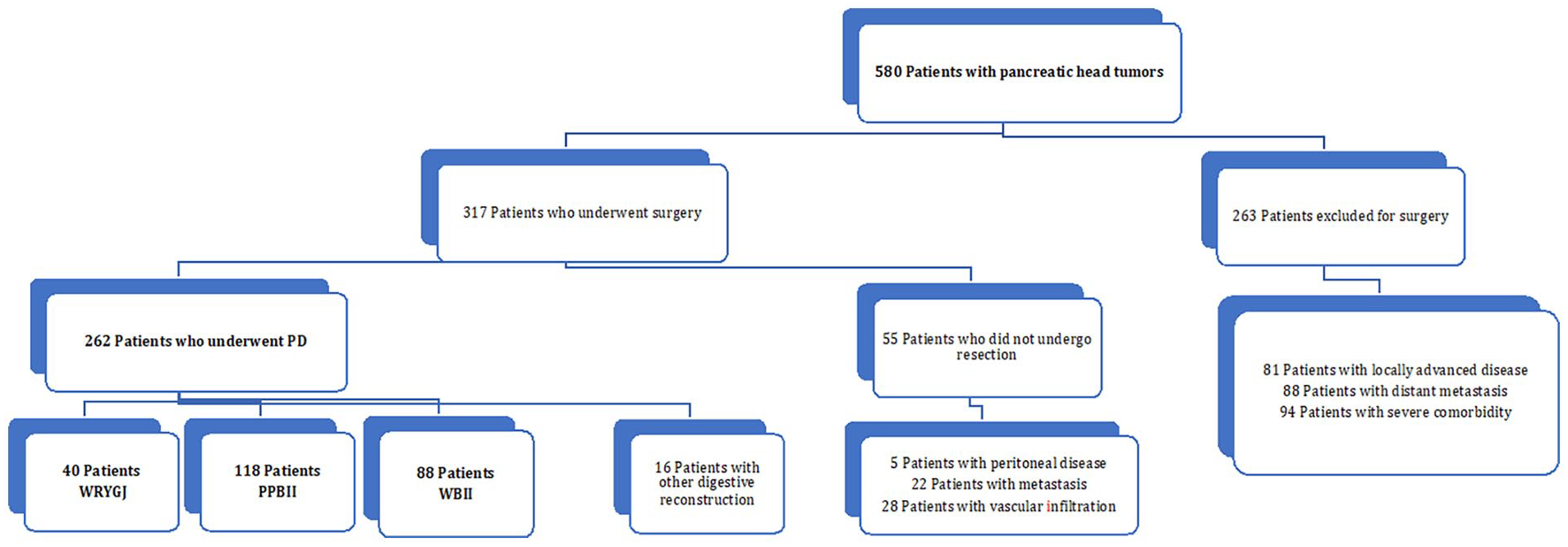
Flowchart of patient selection. Reconstruction techniques after pancreatoduodenectomy (PD): Whipple + Roux-en-Y-gastrojejunostomy (WRYGJ), Pyloric-preserving + Billroth II (PPBII), and Whipple + Billroth II (WBII).
A comparative analysis concerning of preoperative, intraoperative, and postoperative variables was performed among the three groups of patients.
Study endpoints
The primary endpoint was to analyze the incidence and risk factors of relevant B/C POPF and DGE. Secondary endpoints comprised the analysis of the remaining postoperative complications, length of hospital stay, hospital and 90-day mortality, and 1-, 3-, and 5-year survival. The last outpatient review of patients was carried out until December 2023.
Surgical techniques
The surgical details of PD have been previously described. 25 Pylorus-preserving PD was carried out in patients with tumor distant from the duodenum, and antrectomy was performed when the tumor was close to the proximal portion of the duodenum. During pylorus-preserving PD, the proximal duodenum was preserved 2–3 cm distal to the pylorus, dividing the right gastric artery and the pyloric branch of the vagus nerve. In classical Whipple PD, an antrectomy of 20%–30% without truncal vagotomy was performed.
The variation of pancreatojejunostomy was selected based on the surgeon’s experience and the presence of risk factors, such as a <3 mm Wirsung duct diameter and/or a soft consistency of the pancreas. Pancreatojejunostomy was usually performed with an end-to-side duct-to-mucosa anastomosis using the two-layer technique. The pancreatojejunostomy was performed using an external, internal, or non-ductal stent depending on the caliber of the Wirsung duct, pancreatic texture, and surgeon’s preference. The external stent was closed at discharge and removed 6 weeks after surgery at the outpatient clinic. Non-ductal stent was performed using either duct-to-mucosa pancreatojejunostomy or invagination pancreatojejunostomy. An end-to-side hepaticojejunostomy was performed 10–15 cm distal to the pancreatojejunostomy. An end-to-side gastrojejunostomy or duodenojejunostomy (in PPBII) was routinely performed in the antecolic position, approximately 60–65 cm distal to the hepaticojejunostomy. The Roux-en-Y reconstruction after classical Whipple PD was tailored using two jejunal loops. Sixty centimeters afar from the bilio-jejunostomy, a proximal jejunal loop was anastomosed end-to-side to the foot of the jejunal loop. The 60-cm-long distal jejunal loop, that comes from antecolic gastrojejunostomy, was brought downward to perform the referred foot of the loop jejunojejunostomy (Fig. 2). Two drains were placed superior and inferior to the pancreatojejunostomy.
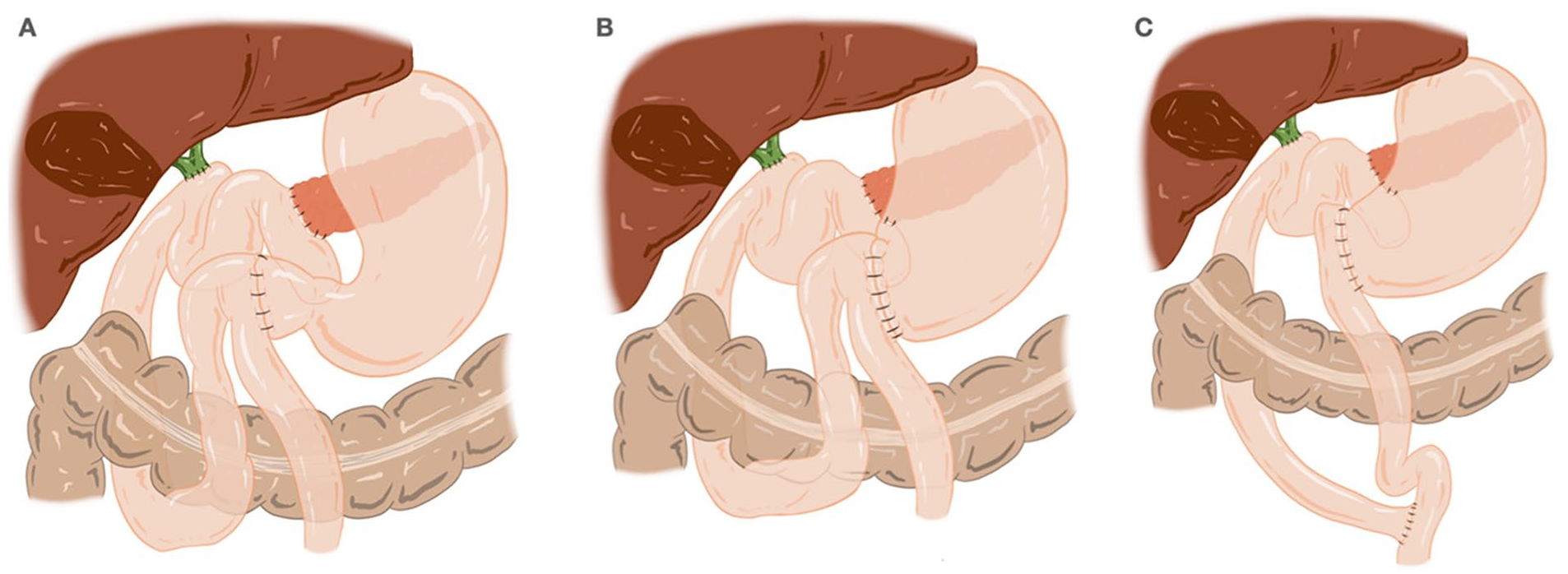
Reconstruction procedures after pancreaticoduodenectomy (PD): (A) Pyloric-preserving PD and Billroth II (PPBII; n = 118 cases); (B) Whipple resection and Billroth II (WBII; n = 88 cases); and (C) Whipple resection and Roux-en-Y gastrojejunostomy (WRYGJ; n = 40 cases).
Postoperative management
Postoperative parenteral nutrition was administered to all patients. Antibiotic prophylaxis was given with 2 g of iv cefazolin, and in patients with biliary stents, jaundice, or cholangitis, iv therapy with piperacillin + tazobactam 4/0.5 was administered every 6 h for 5 days.
Intra-abdominal drains were usually removed on the fifth or sixth postoperative day (POD) in the absence of a fistula, hemorrhage, or infection with amylase levels of abdominal drainage <400 IU.
In the absence of POPF, the nasogastric tube was usually removed on POD 3, and sips of water were progressively administered thereafter, administering a regular diet on POD 7. Prokinetics, such as octreotide (100 mg/mL every 8 h), erythromycin or metoclopramide, were often administered postoperatively if the patient had DGE, and octreotide (100 mg/mL every 8 h) was administered in patients with POPF.
Definitions
DGE was classified according to the definition approved by the ISGPS: grade A (mild), inability to tolerate solid oral intake by POD 7 and usually no vomiting; grade B (moderate), inability to tolerate solid oral intake by POD 14 with or without vomiting; and grade C (severe), inability to tolerate solid oral intake by POD 21 with or without vomiting. Grade A is not considered clinically relevant. 26
Pancreatic fistulas were classified according to the definition formulated by the ISGPS: grade A, biochemical fistulas; grade B, requirement of change in therapy or percutaneous drainage of collections; and grade C, clinical instability requiring drainage of collections or reoperations, leading to organ failure and/or mortality. 27 Postpancreatoduodenectomy hemorrhage (PPH) was classified according to the ISGPS definition. 28 Complications were reported using the Clavien classification. 29
Statistical analysis
Qualitative variables are expressed as absolute numbers, and relative frequencies are expressed as percentages. Associations were analyzed using the chi-square test or Fisher’s exact test, as appropriate. Most quantitative variables did not have a normal distribution according to the Kolmogorov–Smirnov test; therefore, all quantitative variables are expressed as medians and percentiles. The relationships between quantitative variables were analyzed using the Mann–Whitney U test.
All clinically significant variables and variables with p < 0.05 in a univariate analysis were subsequently investigated using a binary logistic regression model to evaluate the association between variables at baseline and 90-day mortality. We also investigated their relationship with grade B and C DGE. Results are expressed as odds ratios and 95% confidence intervals. Survival analysis was performed using the Kaplan–Meier estimator and log-rank test. A p-value < 0.05 was considered statistically significant. Statistical analyses were performed using the SPSS Statistics version 25 (SPSS Inc., Chicago, IL, USA).
Ethical aspects
This retrospective cohort study was approved by our institutional review board (approval no. 24/034) and conducted in accordance with the Helsinki Declaration of 1975 and revision in 1983. The need for local clinical research ethics committee approval was waived due to the retrospective nature of the study. This study was registered in a retrospective research registry (UIN researchregistry9298). Informed consent for surgical treatment was obtained from all patients before surgery. No funding was received for this study.
Results
In the comparison of the preoperative characteristics among the groups, the patients of the WRYGJ group were more frequently submitted to neoadjuvant chemotherapy, and patients of group WBII showed significantly higher values of serum bilirubin (p = 0.022). No significant differences were found in the comparison of the remaining variables among the groups (Table 1).
Preoperative characteristics of the patients.
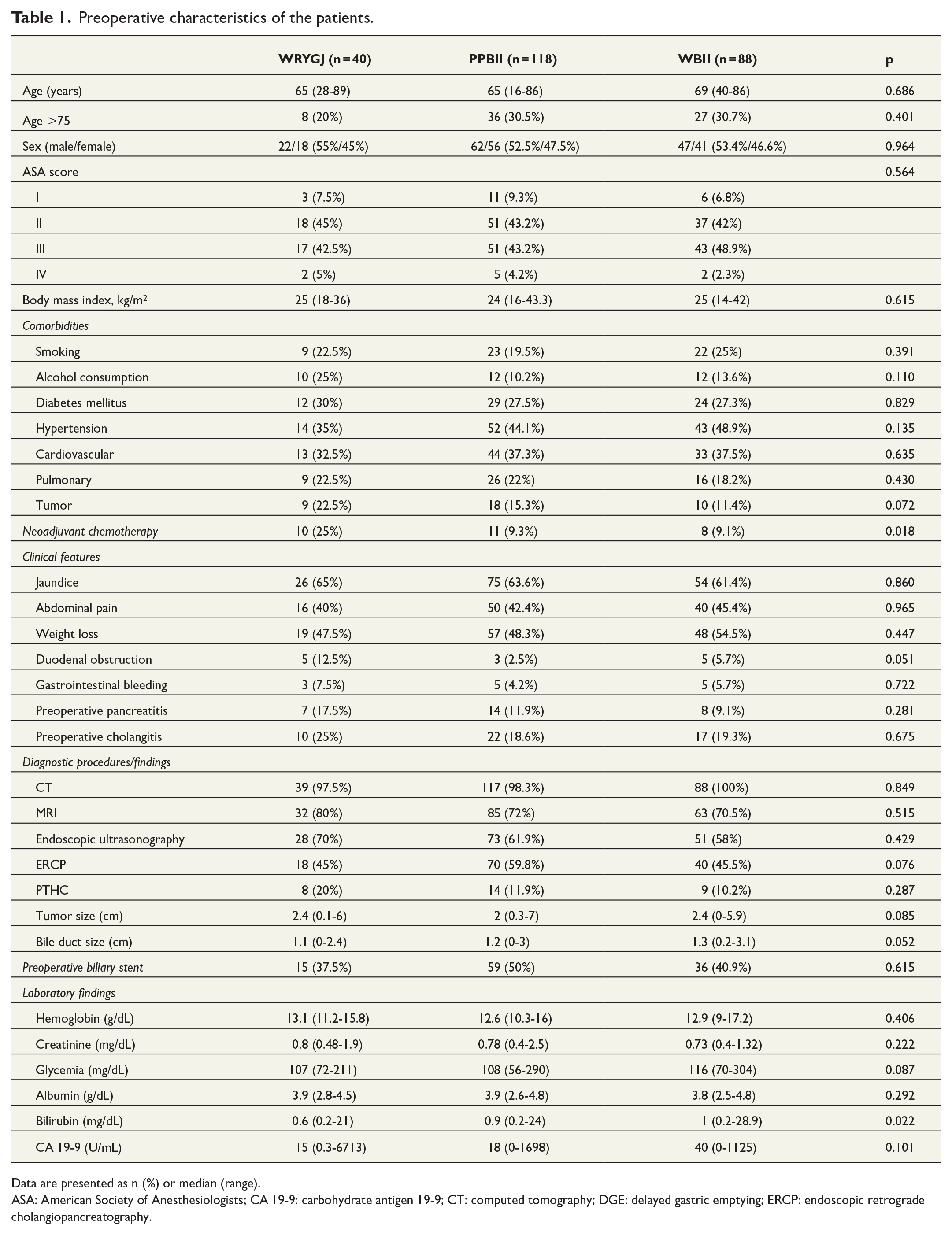
Data are presented as n (%) or median (range).
ASA: American Society of Anesthesiologists; CA 19-9: carbohydrate antigen 19-9; CT: computed tomography; DGE: delayed gastric emptying; ERCP: endoscopic retrograde cholangiopancreatography.
Regarding perioperative variables, duration of surgery, frequency and blood volume transfused, and caliber of the Wirsung duct did not show significant differences among the groups. No significant differences were detected among the different groups regarding the rate of consistency (hard or soft) of the pancreas (p = 0.130). The rate of vascular resection because of tumor invasion and use of octreotide in patients with POPF were similar among the groups. No significant differences were found among the groups about the size and types of tumors and tumor invasion of the peripancreatic tissue and around the celiac axis or superior mesenteric artery. The number of resected lymph nodes was significantly less in the PPBII group (p < 0.001). However, the frequency and number of lymph nodes invaded by the tumor were similar among the groups, as it occurs with macrovascular and neural invasion. The rate of R0 resection was lower in WBII but without statistically significance among the groups. Tumor staging (TNM) did not show significant differences between the groups (p = 0.514) (Table 2).
Perioperative variables and histological features.
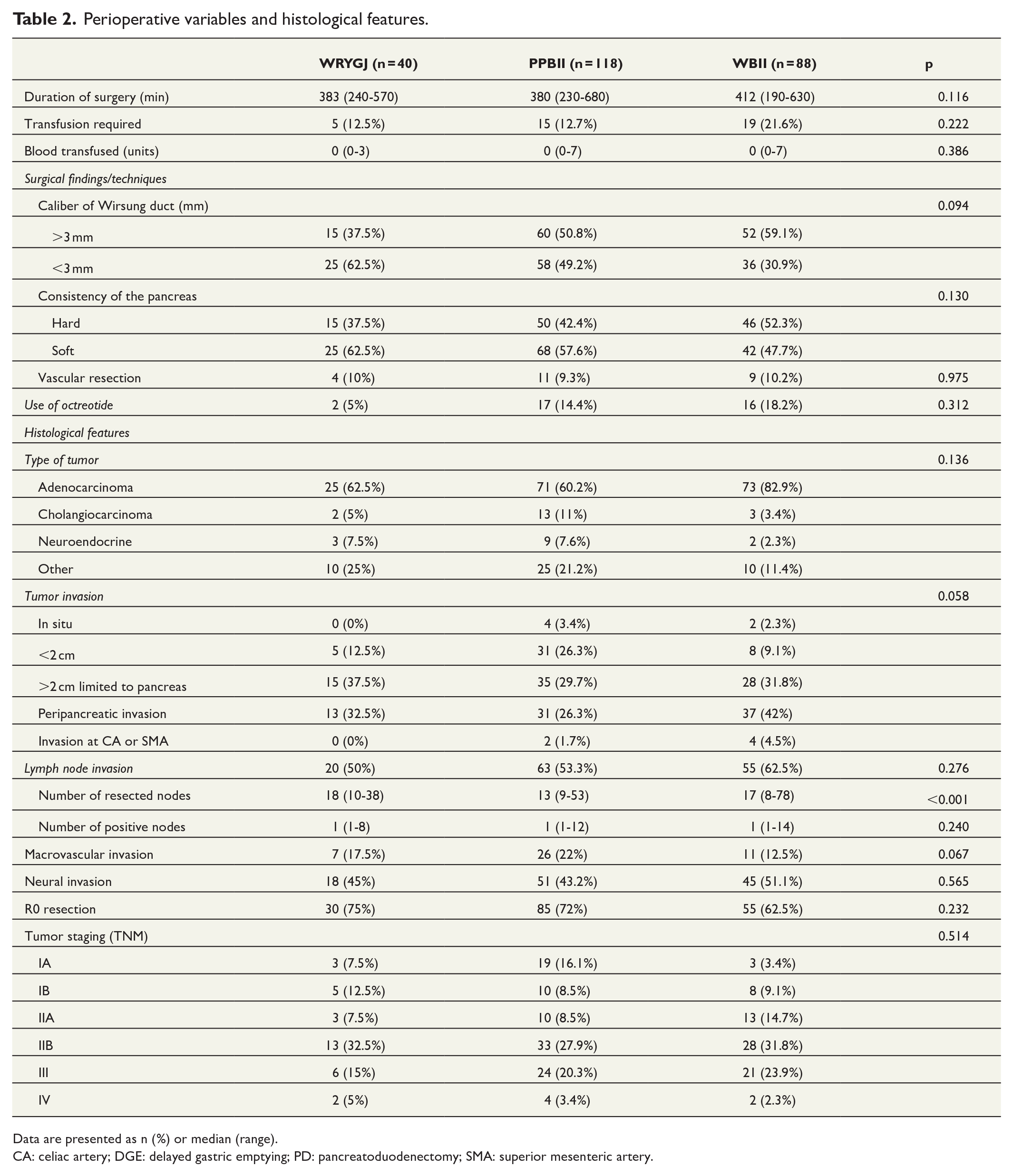
Data are presented as n (%) or median (range).
CA: celiac artery; DGE: delayed gastric emptying; PD: pancreatoduodenectomy; SMA: superior mesenteric artery.
No significant differences in the incidence of medical complications were recorded. The incidence of postoperative pancreatitis did not show significant differences among the groups (p = 0.561). The incidence of relevant B/C POPF and relevant B/C DGE was higher in the group WBII, but these differences did not reach statistical significance. The incidence of relevant B/C PPH was lower in the WRYGJ, but no statistical difference was found between the groups. The incidence of complications according to Clavien classification was similar among the groups. Intensive care unit stay was similar among the groups, although hospital stay was lower in WRYGJ, yet not showing significant differences. Throughout the follow-up, complications and morbimortality at 90 days were similar among the patients, except for the significantly higher incidence of de novo exocrine insufficiency in WBII (p = 0.049). No significant differences were seen regarding 1-, 3-, and 5-year actuarial patient survival among the groups, both in patients with malignant (p = 0.339) and non-malignant tumors (p = 0.271) (Table 3 and Fig. 3).
Morbimortality after PD and long-term survival.
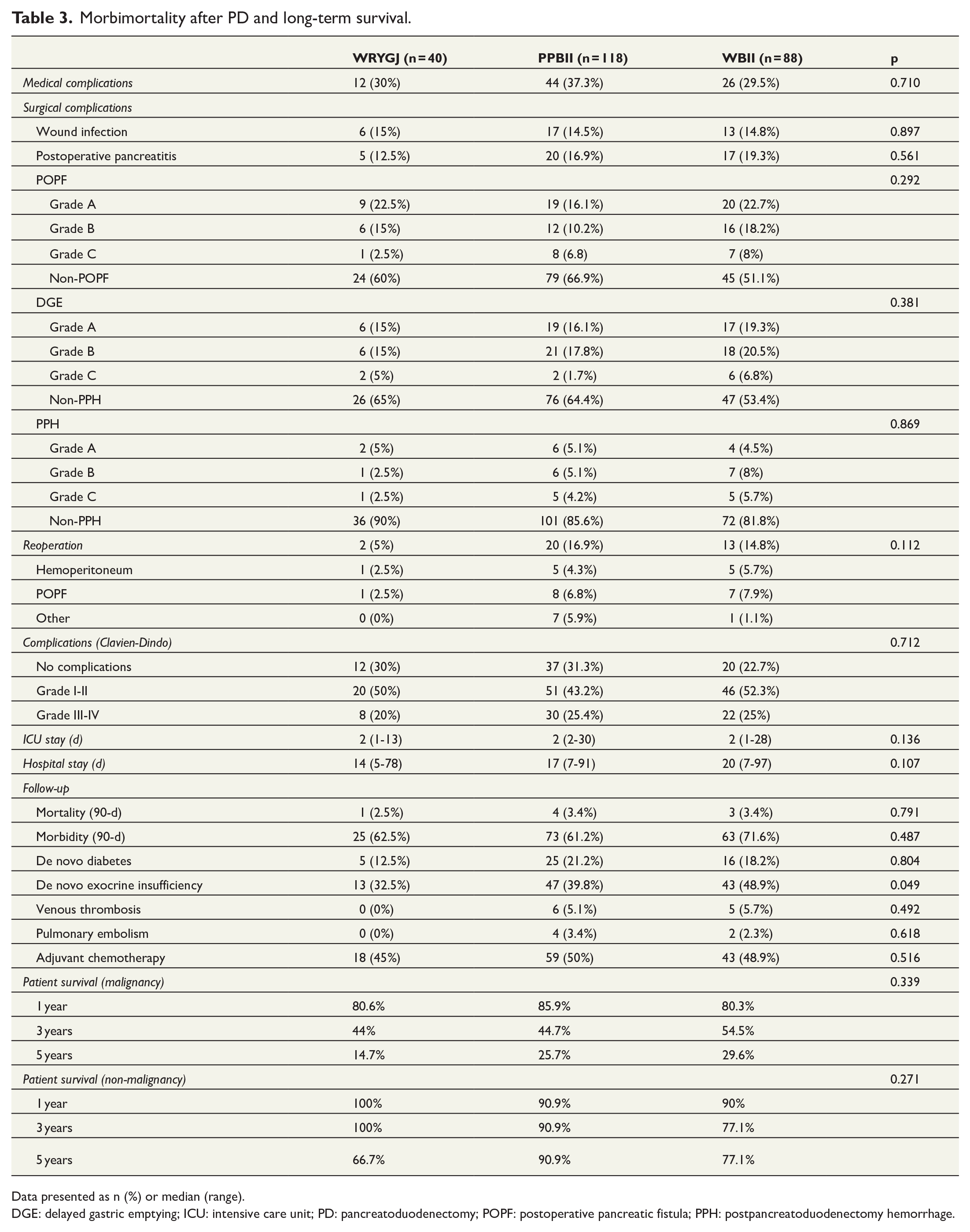
Data presented as n (%) or median (range).
DGE: delayed gastric emptying; ICU: intensive care unit; PD: pancreatoduodenectomy; POPF: postoperative pancreatic fistula; PPH: postpancreatoduodenectomy hemorrhage.
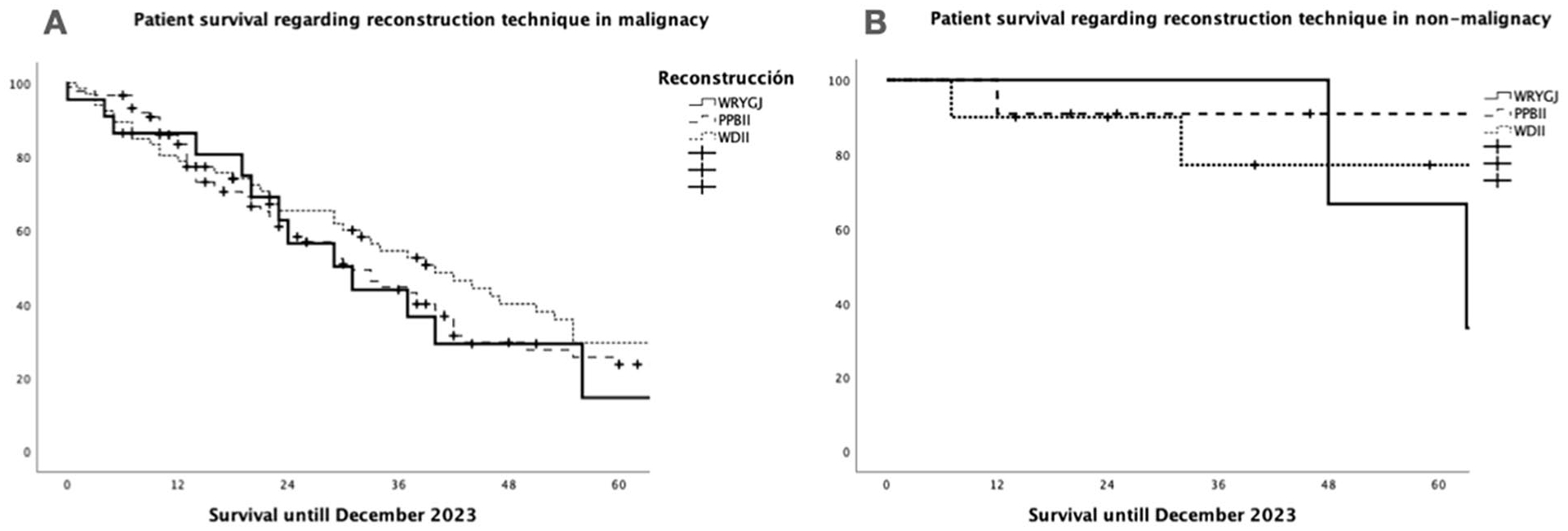
The 1-, 3-, and 5-year patient survival in the three groups of reconstruction after pancreatoduodenectomy (WRYGJ, PPBII, and WDII). (A) Patients with malignant tumor: no significant differences among the groups (p = 0.339). (B) Patients with non-malignant tumor: no significant differences among the groups (p = 0.271).
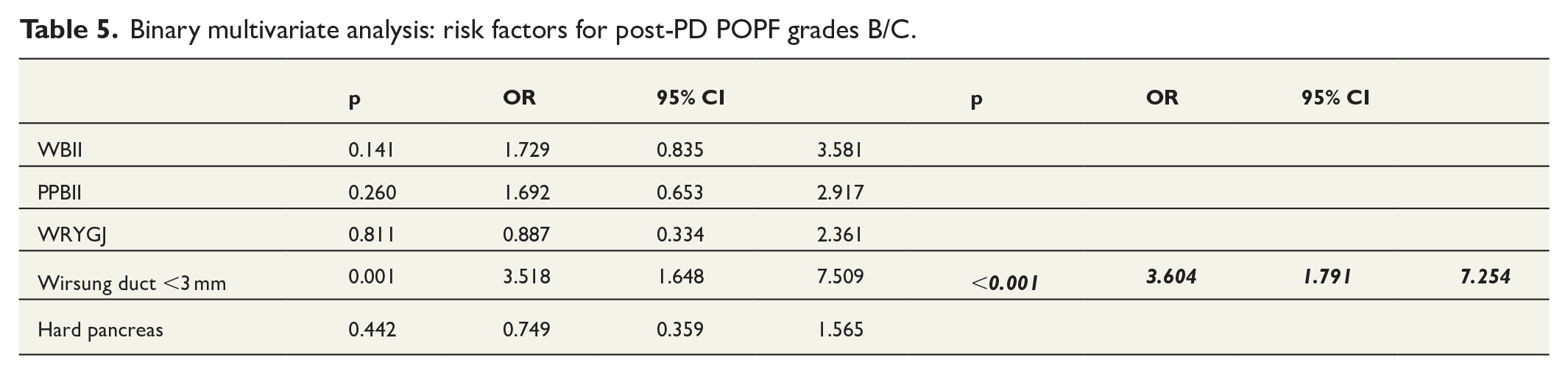
Binary multivariate analysis revealed that POPF-relevant grade B/C was a risk factor for DGE-relevant grade B/C (Table 4). In addition, another binary multivariate analysis demonstrated that the presence of a Wirsung duct with a <3-mm diameter was a risk factor for POPF (Table 5).
Binary multivariate analysis: risk factors for post-PD DGE grades B/C.
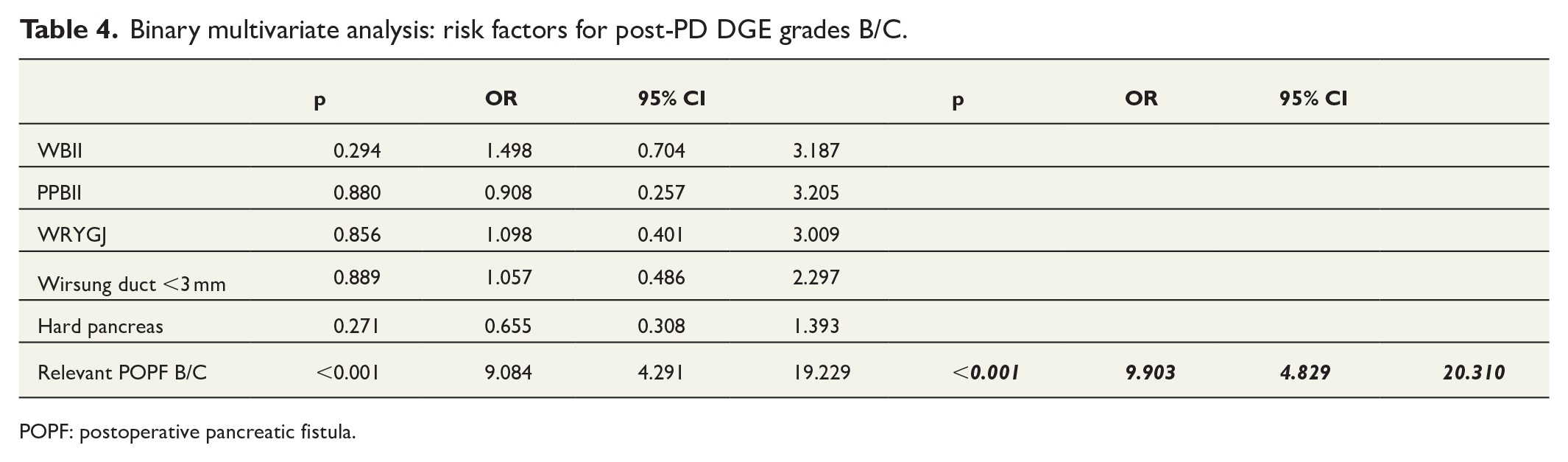
POPF: postoperative pancreatic fistula.
Binary multivariate analysis: risk factors for post-PD POPF grades B/C.
Discussion
A variety of research has been published comparing two gastrointestinal reconstruction techniques after PD; such as three randomized clinical trials,6,12,17 four retrospective comparative studies,10,14 –16 and two meta-analyses.13,19 The outcomes of the different reconstructive techniques after PD are very discordant. The argument to use an isolated Roux-en-Y pancreatojejunostomy versus BII reconstruction has been to divert the biliary secretion away from the pancreatic secretion to prevent activation of pancreatic enzymes by biliary secretion 30 with the intention to reduce the incidence of POPF and its subsequent risk of mortality, 31 whereas the reason to use an isolated Roux-en-Y gastrojejunostomy after PD is to reduce the biliary and pancreatic reflux that can theoretically minimize the rate of DGE.14 –17
The pathophysiology of DGE is not clearly known, being attributed to a multifactorial origin, including duodenal resection associated with reduced plasma motilin concentration, vagotomy, extended lymphadenectomy, antroduodenal ischemia, intra-abdominal collections or abscesses, and relevant grade B/C POPF as the main surgical causes for that complication.7,14,21,26,32 On the contrary, several perioperative risk factors, such as duodenal or ampullary tumors, <3 mm Wirsung duct, soft texture of the pancreas, pancreatic steatosis, significant transfusion, prolonged operation, and no use of Wirsung stent, have been associated with the development of POPF.33 –36
Several studies have been carried out comparing WBII with WRYGJ reconstruction to analyze the incidence of POPF and DGE as the most common and severe complication.14 –17,19 Concerning the surgical technique of WRYGJ, a jejunal loop has been used for the pancreatic and biliary anastomoses, joining at 40–60 cm from the bilio-jejunostomy to the 30–40 cm isolated jejunal loop that comes from the gastrojejunostomy.14,15,17 Our WRYGJ technique differs from the previously mentioned, measuring 60 cm for both jejunal loops. In agreement with other authors, we always use an antecolic position for the gastrojejunostomy because it has been associated with a significantly decreased incidence of DGE as opposed to the use of a retrocolic gastrojejunostomy position.14,17,32 It seems that gastric emptying is favored by the straight passage of the gastric content into the jejunum under the action of gravity 15 and the use of a Braun jejunojejunostomy. 37
In comparative studies analyzing PPBII and WBII techniques, the pancreas duct, bile duct, and duodenum or stomach are subsequently anastomosed with a jejunal loop, maintaining a jejunal length of 60–70 cm from biliary to gastric anastomosis.17,25
Several studies comparing WRYGJ with WBII or pyloric resection-BII have shown similarity of the preoperative variables between the groups,14,15,17 also finding no significant differences regarding operation time, blood transfusion, 14 and postoperative mortality.14,16,17 However, the overall and clinically relevant incidence of DGE was significantly higher in two series of WBII patients,15,16 lower in one, 14 and equal in the remaining. 17 In regard to the incidence of POPF, there was only one study that showed significantly lower incidence in patients with WRYGJ versus BII reconstruction, 15 being the incidence similar in three other studies.14,16,17 Two recent meta-analyses did not show statistically significant differences between both reconstruction techniques in terms of the incidence of POPF, bile leak, intra-abdominal abscess, and the length of hospital stay,19,38 except for the significantly lower incidence of relevant grade B/C DGE and shorter operation time in BII reconstruction. 38 Moreover, no significant differences between the groups were demonstrated regarding the incidence of DGE, operative time, blood transfusion, and overall morbimortality in one of those meta-analyses. 19
Controversial results are also seen in comparative studies between PPBII and WBII reconstruction techniques. Thus, PPBII has been associated with a significant reduction in surgery time and intraoperative bleeding, 22 although other authors did not find significant differences.20,23
Nevertheless, as has been previously referred,14,17,19 the duration of surgery and blood transfusion were similar among our three groups. In addition, the rates of soft pancreas and <3 mm Wirsung duct were higher in group WRYGJ, but without statistically significance. Nevertheless, both characteristics have been confirmed by several authors as risk factors for POPF.35,36 In line with the results of other authors, 1 our multivariate analysis showed that a <3-mm Wirsung duct was a risk factor for POPF grade B/C.
A theoretical advantage of WBII over PPBII has been suggested due to a better oncological resection that also avoids duodenal ischemia. 20 Our study did not reveal significant differences among the groups regarding histological features, except for the lower number of lymph nodes resected in PPBII, although the degree of tumoral invasion of lymph nodes was similar among the groups, demonstrating that the Whipple technique does not add any oncological advantages over the remaining techniques. Nevertheless, in the presence of massive pancreatic tumors, the choice of WBII over PPBII technique can be justified by getting a more extended resection yet having similar morbimortality for both techniques. 20
No significant differences were observed among the groups concerning TNM-staging. In three comparative studies, the incidence of DGE has been significantly higher in PPBII than in WBII,21,22,24 although the other three studies did not find significant differences.8,20,23 However, the presence of relevant POPF grade B/C has been pointed out as a risk factor for DGE.7,32 According to previous reports comparing PPBII with WBII techniques, there have not been observed significant differences concerning the incidence of POPF,20,23,24 postoperative morbidity, hospital stay,22,23,37 and long-term survival.20,22,39 Similarly, our study also revealed no significant differences among the groups concerning postoperative medical and surgical complications. The most severe complications such as relevant B/C POPF and relevant B/C DGE were higher but insignificant in the group WBII. In addition, no significant differences were observed among our groups regarding hospital stay, morbimortality at 90 days, and long-term survival, both in malignant and non-malignant tumors. In addition, a recent review of five reconstruction techniques following PD for pancreatic tumors after Roux-en-Y gastric bypass did not find evidence for the best technique of resection and reconstruction technique. 40
The retrospective nature of this study shows some limitations and is consequently subject to bias. Future prospective randomized studies with large sample sizes are necessary to demonstrate the best reconstruction technique after PD.
Conclusion
The present study did not find significant differences among the three compared reconstruction techniques after PD. Of note, we observed in multivariate analysis that relevant POPF B/C was a risk factor for DGE B/C and <3 mm Wirsung duct for a POPF. Prospective randomized studies are needed to demonstrate the superiority of one technique over the others, considering future studies to demonstrate a reconstruction technique with lesser bilio-gastric reflux that can improve the quality of life.
Footnotes
Acknowledgements
The authors acknowledge Dr Clara Fernández for the drawing of reconstruction procedures and Dr Paula Rioja for her contribution to the acquisition of data.
Author contributions
I.J.A. and C.J.-R. contributed to study conception and design, acquisition of data, analysis and interpretation of data, manuscript writing, drafting the work, and review and approval of the final version. All authors contributed to study conception and design, acquisition of data, drafting the work, and approval of the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was conducted according to the Helsinki Declaration and approved by the Institutional Review Board.
Informed consent
All study participants provided informed written consent before surgery.
Data statement
Data are available from the corresponding author upon request.