
Abstract
Introduction:
The perioperative morbidity following pancreas surgery remains high due to various specific complications: postoperative pancreatic fistula, postpancreatectomy hemorrhage, and delayed gastric emptying. The International Study Group of Pancreatic Surgery has defined these complications. The aim of this study is to evaluate the clinical applicability, to validate the International Study Group of Pancreatic Surgery definition, and to evaluate the postoperative morbidity.
Methods:
Between 2004 and 2014, 769 patients underwent resection. Data were collected in a prospective database. Univariate examination was performed using the χ2-test. Continuous data were tested with the Mann–Whitney U-test. Student’s t-tests and Fisher’s exact tests were performed.
Results:
A total of 542 patients were included in this study. In all, 91 (16.8%) patients developed postoperative pancreatic fistula, 69 of them clinically relevant grades B and C postoperative pancreatic fistula. Grades B and C postoperative pancreatic fistulas were significantly associated with a longer hospital stay. The postoperative pancreatic fistula grade significantly correlated with re-operation. Totally, 32 (5.9%) patients developed postpancreatectomy hemorrhage. Postpancreatectomy hemorrhage grade was significantly associated with re-operation and 30-day mortality. In all, 14 of 19 patients with grade C postpancreatectomy hemorrhage (73.7%) were re-operated; 3 had a simultaneous postoperative pancreatic fistula C. Grade B postpancreatectomy hemorrhage significantly prolonged hospital stay. Grade C postpancreatectomy hemorrhage significantly prolonged intensive care unit stay. Grade C postpancreatectomy hemorrhage led to longer intensive care unit stay but a shorter hospital stay. Delayed gastric emptying occurred in 131 (24.2%) patients. The delayed gastric emptying grade was significantly associated with re-operation. Nine of the re-operated patients had a simultaneous postoperative pancreatic fistula C. Grades A, B, and C delayed gastric emptying were associated with prolonged hospital- and intensive care unit stay.
Conclusion:
Delayed gastric emptying is the most common specific complication after pancreas resection, followed by postoperative pancreatic fistula and postpancreatectomy hemorrhage. The International Study Group of Pancreatic Surgery definitions are well applicable in clinical routine and the different grades correlate well with severity of clinical condition, length of hospital or intensive care unit stay, and mortality. Their widespread use can contribute to a more reproducible and reliable comparison of surgical outcomes in pancreas surgery.
Keywords
Introduction
The perioperative mortality following pancreatic surgery has decreased over the past decades to below 5% in high-volume centers (1, 2). This is caused by improved operative techniques, perioperative care, and management of complications (3). The overall perioperative morbidity, however, remains as high as 60% as reported in some studies (4, 5). Specific complications following pancreas resection include postoperative pancreatic fistula (POPF), postpancreatectomy hemorrhage (PPH), and delayed gastric emptying (DGE). With an incidence of 2%–20% (6), POPF is one of the most common specific complications following pancreatic surgery. According to the literature, the rate of DGE varies between 19% and 57% (7). The rate of PPH is about 1%–8% (8). The discrepancies observed in the reported frequencies of these complications are caused by the lack of internationally accepted classifications and definitions in the past. Over the past years, the International Study Group of Pancreatic Surgery (ISGPS) has defined and classified the specific complications following pancreas surgery (6–8). These classifications are gaining increasing acceptance. The aim of this study is to evaluate the clinical applicability and validate the ISGPS definition and to evaluate postoperative morbidity, clinical course, and mortality following pancreas surgery at a high-volume center over a period of 10 years according to the ISGPS definition.
Material and Methods
Data Collections
Between January 2004 and December 2014, 769 patients underwent pancreatic surgery at the Department of Surgery of the University Medical Centre Mannheim. The prospective database comprises all patients who receive pancreatic resections (9, 10). Patients with acute necrotizing pancreatitis with several procedures were excluded from the further analysis. Patients who underwent pancreas resection as part of a multivisceral resection due to soft tissue tumors such as sarcoma or gastrointestinal stroma tumor were also excluded from the further analysis. Patients with missing data for postoperative complications were also excluded from the analysis. The data analyzed in this study comprised demographics, pathology report, TNM classification in malignant tumor, preoperative presenting symptoms, preoperative procedures, laboratory values, American Society of Anesthesiologists (ASA) score, details of surgical therapy, hospital course, postoperative hospital stay, intensive care unit (ICU) stay, need for re-intervention or re-operation, and postoperative mortality. If the patients had any complications, these were categorized according to the definition of the ISGPS (see below). Data were partially complemented by clinical notes of the patients. Patients were informed on collecting their data in the databank for purpose of further general anonymous analysis. Follow-up was performed through personal contact with the patient or the patient’s primary physician and was terminated in December 2014 or at the time of the patient’s death.
Surgical Technique
The reconstruction after partial pancreaticoduodenectomy (PD; classic Kausch–Whipple or pylorus-preserving procedure) was performed as reported earlier (11). Since January 2007, a pancreaticogastrostomy (PG) was performed in case of a high-risk gland (soft pancreas texture with a small duct) (11). Patients with high-risk glands received perioperative octreotid until postoperative day (POD) 5. Patients with PG had a nasogastric tube for 48 h as an indicator drain for intraluminal hemorrhage and received high-dose pantoprazol (40 mg intravenous (i.v.) bid). Patients with a standard duct-to-mucosa pancreaticojejunostomy (PJ) received neither octreotid nor high-dose pantoprazol. Two soft drains were placed and patients received fluid diet on PODs 2 and 3. As of POD 4, if tolerated, they could eat solid meals. In all patients, the amylase content in the drains was measured before removal. If the amylase level was less than three times of the upper limit of normal serum amylase, the drains were removed on day 5; otherwise, the drain at the pancreatic anastomosis was left in situ. In distal pancreatectomy, the main duct was closed with a non-resorbable monofilament 5-0 suture and the remnant was closed using resorbable monofilament 4-0 horizontal mattress sutures. All patients after pancreas resection spent a few days on the surgical intermediate care unit. Those with a complicated perioperative course were treated on the ICU if indicated.
Definitions
Postoperative complications evaluated in this study were POPF, PPH, and DGE after pancreatic surgery. These complications were assessed and categorized according to the definition and classification by the ISGPS for POPF (6), PPH (8), and DGE (7), respectively. In brief, the ISGPS classification is characterized by grading each complication into three grades. Grade A complications require only minor adjustments in management and can always be managed conservatively. Grade B complications require a significant change from normal clinical pathway, while Grade C complications require major invasive interventions in the case of POPF and PPH or markedly prolonged nasogastric drainage in the case of DGE.
The operative procedures included in this study were pylorus-preserving or classic pancreaticoduodenectomy (Whipple), pancreatic left resection, duodenum-preserving pancreatic head resection, and total pancreatectomy. Diagnoses included malignant tumors or benign conditions including chronic pancreatitis.
Statistical Analyses
The statistical analyses were performed using SPSS for Windows, version 15.0 (SPSS, Inc., Chicago, IL, USA). All clinical and pathological characteristics were stratified to build categorical or nominal variables. The cut-off points for categorizations were based on previously described cut-off points and/or recursive partitioning as described previously (12). Continuous data are presented as median and range values. Univariate examination of the relationship between the assessed criteria and the different patient cohorts was performed using the χ2-test. Student’s t-tests and Fisher’s exact tests were used for comparisons between groups. Mann–Whitney U-test was used as a non-parametric test to compare the continuous data without a normal distribution. A p value of <0.05 was considered significant. Significant factors (at p < 0.10) at the univariate level were entered into the multivariate model. A Cox regression analysis with stepwise backwards elimination based on the likelihood ratios was employed to test for independent predictors of survival.
Results
A total of 769 patients underwent a pancreas resection at the Department of Surgery of the University Hospital Mannheim. In all, 29 patients had acute necrotizing pancreatitis with a total of 172 procedures and were excluded from the further analysis. In addition, 26 patients underwent pancreas resection as part of a multivisceral resection due to soft tissue tumors such as sarcoma or gastrointestinal stroma tumor. These were also excluded from the further analysis. Additional 29 procedures were excluded because of missing data for postoperative complications. Totally, 542 patients consisting of 243 (44.8%) women and 299 (55.2%) men with a median (range) age of 65 (21–88) years were included in this study. A total of 326 (60.1%) patients had a neoplasm and 216 (39.9%) patients had a benign disease of the pancreas. Patients with a benign condition were those with a chronic pancreatitis, microcystic adenomas, ampullary adenoma, or pancreatic pseudocyst. Neuroendocrine carcinoma, ampullary, distal bile duct or duodenal neoplasms, high-grade intraductal papillary mucinous neoplasm (IPMN), mucinous cystadenocarcinomas, and solid pseudopapillary neoplasms were classified as neoplasms.
The operative procedures consisted of classical Kausch–Whipple operation (PD) in 43 (7.9%) patients, pylorus-preserving pancreaticoduodenectomy (PPPD) in 314 (57.9%) patients, duodenum-preserving head resection in 21 (3.9%) patients, pancreatic left resection in 114 (21%) patients, total pancreatectomy in 46 (8.5%) patients, and segment resection in 4 (0.7%) patients (Table 1). There were no statistically significant differences between various procedures (Supplementary Table 1) or various diagnoses (Supplementary Table 2 : Complications in various diagnoses) regarding the rate of different complications.
Demographics of our patient cohort.

PPPD: pylorus-preserving pancreatic head resection; DPPHR: duodenum-preserving pancreatic head resection; BMI: body mass index.
POPF
A total of 91 (16.8%) patients developed a POPF following the operation, 69 of them clinically relevant grades B and C POPF: 22 (4.1%) patients grade A, 49 (9%) patients grade B, and 20 (3.7%) patients grade C. A total of 32 (35.2%) patients with POPF underwent re-operation: 5 patients with grade A, 12 patients with grade B, and 15 patients with grade C. The re-operations in patients with grade A POPF were due to reasons other than POPF (e.g. wound infection, revision of the bilio-digestive anastomosis) so these patients remained classified as grade A POPF. The POPF was treated conservatively in these patients. An increasing grade of POPF was significantly associated with a higher re-operation rate (p < 0.0001). A higher POPF grade was not significantly associated with a higher 30-day mortality.
Of the 49 patients with grade B POPF, 5 patients (10.2%) received a new drain computed tomography guided and 2 (4.1%) ultrasound guided. The other patients were discharged with drain in situ. They were seen once a week in the outpatient clinic where they received an ultrasound and laboratory check up. The drain, the amount, and the consistency of the effusion were examined. None of these patients had to be readmitted in the hospital. The drains were removed in the further course. In 12 patients (24.5%), a re-operation had to be performed due to infected soft tissue necrosis or deep wound infection. A revision of the anastomosis, an intraabdominal lavage, or completion pancreatectomy was not necessary.
In case of grade C POPF (n = 20), 15 patients (75%) received a revision operation involving completion pancreatectomy (7 patients), conversion of the PJ to PG (1 patient), or drainage of abscess and debridement (7 patients). One patient, who was initially discharged with the drain in situ, was readmitted to the intermediate care unit with sepsis, received i.v. antibiotics, and underwent a re-operation with drainage of a large intraabdominal abscess. Five patients had an interventional therapy with a drain placement. They were classified as grade C due to severe worsening of their clinical condition with a need for ICU therapy.
PPH
A total of 32 (5.9%) patients developed PPH: 3 (0.55%) patients grade A, 10 (1.8%) patients grade B, and 19 (3.5%) patients grade C. In all, 22 (68.8%) patients with PPH underwent re-operation: 2 patients with PPH grade A, 6 with PPH grade B, and 14 with PPH grade C. The PPH grade was significantly associated with the re-operation rate (p < 0.0001). In addition, a total of 10 (28%) patients with PPH died within 30 days following the operation: 1 patient with grade A PPH and 9 patients with grade C PPH. The PPH grade was significantly associated with 30-day mortality (p < 0.0001; Table 2).
Re-operation rate and 30-day mortality after pancreatectomy.
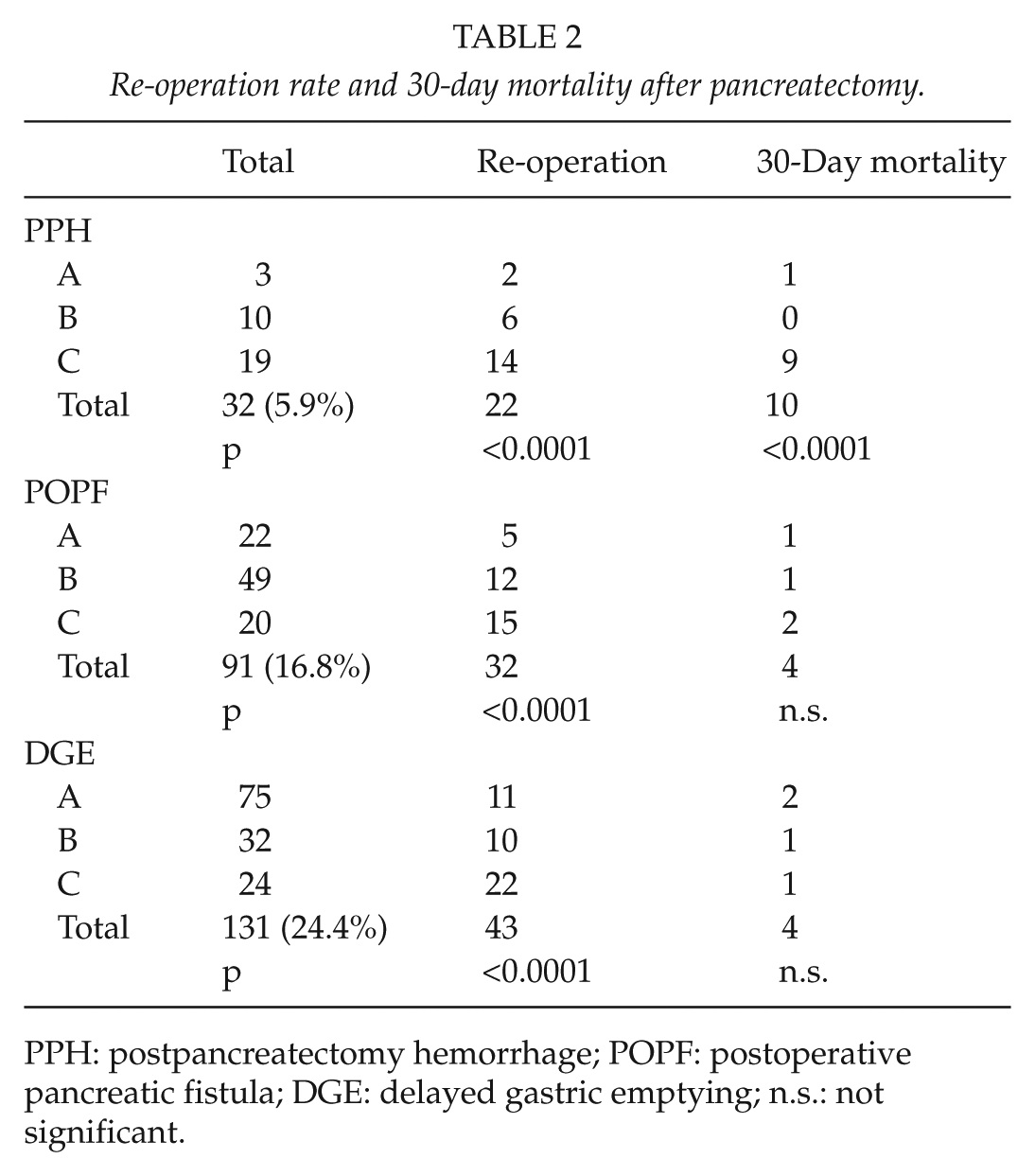
PPH: postpancreatectomy hemorrhage; POPF: postoperative pancreatic fistula; DGE: delayed gastric emptying; n.s.: not significant.
The three patients with a grade A PPH did not receive any specific intervention regarding PPH. One of these patients had to be re-operated due to a complicated course with biliary peritonitis and small bowel lesion. The other patient had a bloody effusion in his drain, which sustained spontaneously without intervention. He was re-operated due to sepsis. Intraoperatively, a surgical focus could be ruled out and the patient was put on an anti-mycotic therapy due to candida sepsis.
Ten patients had PPH grade B. Two of them received conservative therapy with blood transfusion on the ICU. Three patients were treated endoscopically due to intraluminal bleeding. One of them also had a re-operation during his hospital stay due to bleeding from the PG. A total of six patients had a re-operation: five patients underwent re-laparotomy only due to PPH with an extraluminal bleeding from mesocolon, omentum, or PG. One patient underwent re-laparotomy and had a conversion of PJ to PG; this patient had a complicated course with PPH grade B, POPF grade C, and DGE grade C. This was the only patient in this group who had a simultaneous POPF grade C.
In all, 19 patients had PPH grade C. Three patients could be treated endoscopically. In one patient, an angiography with coiling was performed. Fourteen of 19 patients with PPH grade C underwent re-operation. In one of these patients, a pseudoaneurysma of the right hepatic artery was seen intraoperatively, which was ligated. Due to persisting bleeding postoperatively, an angiography with coiling was performed, so he received both therapies.
Of the 14 patients with a re-operation, 3 had POPF C. In one of these patients, the bleeding was due to subhepatic and subphrenic abscess. She received a completion pancreatectomy. The next patient with a simultaneous POPF grade C and PPH grade C had a bleeding from the celiac trunk and an abscess in the pancreatic bed. She received a revision with lavage, necrosectomy, and distal pancreatectomy. The third patient had a bleeding from the stomach with an abscess due to a dorsal anastomosis leakage. He received programmed lavage on the ICU. One patient with PPH grade C refused any further therapy and died thereafter.
DGE
DGE occurred in 131 (24.2%) patients; 32 (5.9%) patients suffered grade B DGE and 24 (4.4%) patients grade C DGE. A re-operation was performed in 43 (32.8%) patients with DGE: 11 patients with grade A, 10 patients with grade B, and 22 patients with grade C. DGE grade was significantly associated with re-operation (p < 0.0001) but not with 30-day mortality (Table 2).
Now concentrating on 10 of the patients with DGE grade B who were re-operated, 2 had simultaneously POPF grade C. Three patients had simultaneously POPF grade B. All these five patients received a re-laparotomy with lavage and abscess drainage. One further patient with grade B DGE had simultaneously PPH grade B with bleeding from the PG. So the operations in this patient addressed both problems. One patient had peritonitis without an abscess and received a lavage. The other three patients had an abscess and received a re-operation with lavage and abscess drainage.
Regarding the 22 patients with grade C DGE who were re-operated, 9 had simultaneously POPF grade C. These patients received a re-operation with lavage and abscess drainage; 5 patients received a completion pancreatectomy or distal pancreatectomy with or without splenectomy; 1 received a conversion of PJ to PG. One patient with DGE grade C had a simultaneous POPF grade B. This patient got re-operated and received a left hemihepatectomy due to liver necrosis. So the condition of these patients could well have been worsened or actually caused by simultaneous grade B or C POPF.
Hospital and Icu Stay
Grades B and C POPF were significantly associated with a longer hospital stay (p < 0.001). Regarding the ICU stay, grade C POPF was significantly associated with a longer stay (p < 0.001). A tendency for a longer ICU stay could be demonstrated for grade B POPF, which was, however, statistically not significant (p = 0.06). In comparison to patients without PPH, those with a grade B PPH had a significantly longer hospital stay (median (range): 23 (12–129) days versus 15 (3–245) days). The ICU stay was not signifi-cantly prolonged in patients with grade B PPH in comparison to those without PPH. Regarding patients with grade C PPH in comparison to those without PPH, the ICU stay was significantly longer (median (range): 7 (0–144) days versus 3 (0–71) days, p < 0.0001). The difference in the total-hospital stays, however, was not statistically significant between these two groups (see Table 3). This could be explained by the fact that grade C PPH was also associated with a higher 30-day mortality: 9 of 19 patients (47.4%) with grade C PPH died within 30 days in comparison to 0% of patients with PPH grade B. Patients with grade C PPH had a significantly longer ICU stay with a more complicated course leading to higher 30-day mortality and as a result shorter total-hospital stay. Grades A, B, and C DGE were all significantly associated with a longer hospital and ICU stay (p < 0.001; Table 3).
Length of hospital and intensive care unit stay after pancreatectomy.
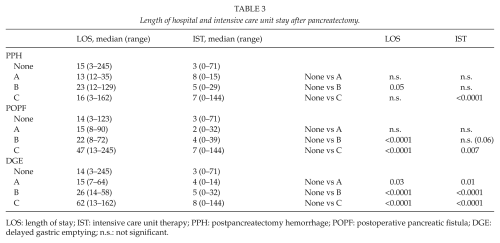
LOS: length of stay; IST: intensive care unit therapy; PPH: postpancreatectomy hemorrhage; POPF: postoperative pancreatic fistula; DGE: delayed gastric emptying; n.s.: not significant.
Discussion
Characteristic of the Complications
More than 500 patients who underwent pancreatic resection were included in this study. DGE was the most common complication following pancreatic resection in this collective with an incidence of 24.2%, followed by POPF with an incidence of 16.6%. PPH with an incidence of 5.9% was a rare complication in comparison with DGE and POPF. In a study by Bassi et al. (13) in 2005, the reported incidence of DGE was as low as 2% in patients having undergone a PG or 10% in patients following PJ. This study, however, was performed prior to the introduction of the ISGPS definition of DGE. The definition of DGE in the mentioned study was the need for nasogastric tube decompression for more than 10 days following the operation (13). Our results regarding DGE are in accordance with a more recent study by Cameron and He (14) in 2015 including 2000 patients with a pancreas resection with a DGE rate of 21%. POPF with a rate of 16.6% was the second most common complication. Its incidence lies closer to that reported in this study by Cameron and He (14) (15%) as well as in previous studies by Bassi et al. (13) (13%–16%) or Duffas et al. (15) (19%) PPH with an incidence of 5.9% was the least common complication in this study which is comparable with the PPH rate in the study by Bassi et al. (13) in 2005 (4%–7%) and Grutzmann et al. (16) in 2012 (5.7%).
Clinical Implication of the Complications
There was a significant association between the re-operation rate which is in fact one of the several parameters used for grading and the increasing grade of the three complications (see Table 2). The only complication which was significantly associated with a higher 30-day mortality rate and a higher re-operation rate with increasing grade was PPH. This may be due to the small overall number of grade C pancreatic fistulas.
In addition, the total length of hospital stay (LOS) and length of ICU stay can be used as further factors reflecting the clinical course and prognosis of the patients. Regarding PPH, the LOS was longer in grade B PPH in comparison to grade C PPH. The ICU stay was, however, longer in grade C PPH than grade B PPH. This could be explained by the fact that grade C PPH was also associated with a higher 30-day mortality: 9 of 19 patients (47.4%) with grade C PPH died within 30 days in comparison to 0% of patients with PPH grade B. Patients with grade B PPH had a longer LOS. They, however, recovered well and could be discharged from the hospital. This further underlines the clinical implication of grade C PPH following pancreas resection. In their study in 2012, Grutzmann et al. (16) showed similar results concerning grade C PPH with a mortality rate up to 41%. DGE grade A was the only grade A complication which was significantly associated with a longer hospital and ICU stay. Grade A POPF or PPH, however, was not significantly associated with a longer LOS or ICU therapy, demonstrating a low clinical relevance of grade A POPF or PPH. These results demonstrate that the ISGPS definition of the complications is an objective, valid, and useful tool for discriminating between different complication grades with a significant clinical relevance for the course of the disease and the patients’ outcome.
Therapeutic Consequence of the Complications
POPF
In case of grade B POPF, all patients had a drain which remained in place for more than 7 days after the operation. A revision of the anastomosis or completion pancreatectomy was not necessary in any of these patients. Fifteen of 20 patients with grade C POPF (75%) received a revision operation with 5 patients receiving an interventional therapy with a new drain placement. These patients revealed a severe clinical impairment and a need for ICU therapy. These results demonstrate that the ISGPS score is valid and clinically applicable. The association between severity of POPF, the clinical condition of the patient, and the financial consequences of the fistulas has already been demonstrated by Pratt et al. (17). Pratt et al. (17) could also demonstrate an association between increasing fistula grade and prevalence of other complications, In this study, the presence and increasing severity of POPF was also significantly associated with the presence and severity of DGE (p < 0.0001).
PPH
Concerning the therapeutic consequence of PPH, 14 of the 19 patients with PPH grade C (73.7%) were re-operated. Three of the 10 patients (30%) with PPH grade B were re-operated due to bleeding. A re-operation due to bleeding was not necessary in any of the patients with grade A PPH. In addition, 3 of the 14 (21.4%) patients with PPH C who were re-operated had a simultaneous POPF C. Of the six patients with PPH B with a re-operation, one (16.7%) had a POPF C. There is significant association between the re-operation and the severity of PPH. These results demonstrate, on one hand, how critical this complication is; on the other hand, they underline the necessity for a clear therapeutic algorithm in case of this complication. In this study, 73.7% of the patients with PPH grade C underwent re-operation. Grutzmann et al. (16) described a similar re-operation rate of 74% in their study.
It could be demonstrated that the presence of PPH was significantly associated with the presence of DGE (p < 0.0001). In the literature, there has been evidence for the association of PPH and POPF (16, 18). This association could not be demonstrated in this study though the causal relationship is obvious in clinical routine.
DGE
The presence of PPH and POPF was significantly associated with DGE. In this study, it was seen that of the 10 patients with grade B DGE who got re-operated, 3 had a simultaneous POPF B and 2 had a simultaneous POPF C. One further patient had a simultaneous PPH B. In addition, 9 of the 22 re-operated patients with DGE C had a simultaneous POPF C and one patient had a simultaneous POPF B. So the condition of these patients could well have been caused or even worsened by a simultaneous POPF B or C. The association between DGE and other complications has been described in the literature (19–21). The statistical association between DGE and PPH could, however, not be demonstrated in the mentioned studies (19, 20). DGE is one of the most common complications following pancreas resection. According to the literature, there are various risk factors leading to DGE such as nerve damage or ischemia of stomach following a partial gastrectomy or a pancreas resection, pylorus spasm, an intraoperative damage of the vagus nerve, as well lack of hormone stimulations following resection of duodenum (7, 22). DGE often results in a longer LOS and higher financial costs (20). In this study, there was no association between DGE and 30-day mortality. There was, however, a statistically significant association between increasing severity of this complication and the re-operation rate, the LOS, and the length of the ICU therapy. An association between increasing grade of DGE and LOS could also be shown in the study by Park et al. (19).
There are limitations in our study. First of all, this is a retrospective analysis of data from a prospective database. Furthermore, due to incomplete and missing data, certain interesting parameters such as texture of the pancreas and diameter of the duct could not be included in this study for the further analysis.
Conclusion
This study represents a large series of patients following pancreatic resection and evaluates the incidence of specific postoperative complications and its course according to the ISGPS definitions. The postoperative morbidity following pancreatic resection remains high with DGE being the most common specific complication, followed by POPF and PPH. The study confirms that the ISGPS definitions of these complications are clinically relevant and that increasing grade is associated with a severe clinical condition and an increasing affection of the outcome. In addition, these definitions are objective and clinically well applicable in the diagnosis and therapy of the specific postoperative complications. Furthermore, they avoid misunderstanding and allow a valid comparison between various surgical techniques, pharmacological therapy, and complication rates following pancreas surgery. Pancreatic resection remains a demanding procedure with serious and clinically relevant complications. Using ISGPS definitions, these complications can be diagnosed objectively and correctly and treated adequately and promptly using a definition guided therapy algorithm.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.