
Abstract
Frailty is a common phenomenon in older adult population and associated with an elevated risk of adverse health outcomes. Recent studies have demonstrated that patients with frailty undergoing surgery had a significantly higher morbidity and mortality compared to those without frailty. This is particularly important in patients with cancer because the prevalence of frailty is persistently high across a spectrum of primary cancers. Identifying frailty in oncological patients undergoing surgery may provide an important preoperative intervention opportunity to mitigate operative risks. In this review, we provide an overview of frailty and its association with other geriatric syndromes. We will also review the impact of frailty on postoperative outcomes focusing on the field of surgical oncology. We then describe currently available tools to objectively measure frailty to provide clinicians with various practical tools that may be adopted in their clinical practice. Finally, we will describe potential interventional programs, including the recently introduced Geriatric Surgery Verification program by the American College of Surgeons, that may be institutionally adopted to mitigate postoperative complications and improve meeting patient-centered goals in the frail patient population.
Keywords
Introduction
In geriatric medicine, frailty represents a geriatric syndrome that encompasses a complex interplay of physical, cognitive, and psychosocial factors, leading to an elevated risk of adverse health outcomes, such as functional decline, falls, disability, increased hospitalization, and greater mortality. 1 Recent review article by Kim et al., described the two major concepts that are incorporated in defining frailty. First, frailty is seen as a syndrome. A prominent example is the Fried’s frailty phenotype (FFP). 2 According to the work by Fried et al., frailty is defined as a clinical state fulfilling three out of five phenotypic criteria indicative of decreased energy levels, including diminished grip strength, reduced energy, slowed walking speed, low physical activity, and unintended weight loss. 1 Second, frailty is seen as a state of accumulated age-related deficits leading to an overall poor state of health. In this type of definition, degree of frailty is quantified using frailty indices to sum up the total number of deficits assessed. 1 Even though the concept of frailty is commonly correlated with the older adult population and is thoroughly studied in geriatric medicine, it is not uniquely confined to this field nor to the older adult. In actuality, the impact of frailty spans across different age groups and specialties in medicine, particularly in surgery.
Frailty is common and increasing in prevalence. A longitudinal analysis of primary care data from a cohort of adults aged 50 years and above in the United Kingdom showed that the prevalence of frailty increased from 26.5% in 2006 to 28.9% in 2017, with the average age of frailty onset being 69 years. 3 In the United States, one study estimated that 15% of the elderly population not residing in nursing homes were frail with an additional 45% being classified as prefrail. 3 Certain factors have been demonstrated to influence the prevalence rates of frailty including age, sex, race/ethnicity, and socioeconomic status. For example, frailty is more frequently observed among older adults, women, racial and ethnic minorities, individuals living in residential settings, and populations with lower income. In the surgical population, the exact prevalence of frailty may vary and is influenced by various factors including patient population, clinical characteristics, and the type of surgery. In the field of surgical oncology, the prevalence of frailty is variable but persistent across a spectrum of primary cancers. Among patients with cancers that require high-risk operations, such as hepatobiliary and pancreatic cancer patients, the overall estimates of frailty prevalence were higher than the average population at 39%. 4 Among patients with cancer that require medium-risk operations, such as colorectal cancer patients, frailty prevalence ranged from 12% to 56% with most studies reporting frailty prevalence rate between 20% and 40% in a systematic review of 15 studies. 5 While frailty prevalence is lower, it is persistent even in patients with cancer that require low-risk operations, such as breast cancer patients. Minami et al., using the Surveillance, Epidemiology, and End Results linked to the Medicare database, found that frailty was seen in 4.1% of women aged ≥ 65 years with ductal carcinoma in situ or Stage I hormone and Human epidermal growth factor receptor 2 (HER-2) receptor-positive breast cancer. In addition, they noted that frailty status worsened during treatment in 21.4% of patients who received locoregional therapy for early-stage breast cancer, including lumpectomy or mastectomy. 6
Identifying frailty in patients undergoing surgery is important to anticipate and mitigate operative risks. Gill et al. performed a population-based retrospective study to estimate the mortality after major surgery in community-living older US adults and found that mortality was considerably elevated among older adults who were frail. 7 Frailty has also been linked to other adverse clinical outcomes, including postoperative complications, delirium, unfavorable discharge disposition, and hospital readmission.8–11 To identify and minimize the negative impact of frailty, many interventional programs have been developed across multiple disciplines. Some notable programs include prehabilitation programs, geriatric co-management programs, Enhanced Recovery After Surgery (ERAS) protocols, and geriatric surgery verification (GSV) programs. Prehabilitation programs focus mostly on exercise, nutrition, and psychosocial counseling with the goal of improving overall postoperative health and recovery. 12 In geriatric co-management programs, geriatricians work with providers from other specialties to address the unique needs of the older adult undergoing surgery to optimize perioperative management. The ERAS protocols represent a multidisciplinary care approach consisting of elements aimed at optimizing evidence-based perioperative care processes. 13 While ERAS is not exclusive for older patients, the principles in ERAS are well suited for the compromised patient like the older surgical patient. The American College of Surgeons’ GSV initiative encompasses 32 standards tailored to addressing geriatric syndromes in older adults undergoing surgical procedures. 14
Frailty in surgery acts as a valuable tool for risk assessment and prognostication. By diagnosing frailty earlier in the perioperative pathway affords the opportunity to assess risk, modify the syndrome, perform informed shared decision-making, and plan the most appropriate surgical (and non-surgical) pathway. 1 In this review, we will discuss (1) available tools to measure frailty; (2) impact of frailty on postoperative outcomes; (3) geriatric syndrome and frailty; (4) interventional programs to mitigate postoperative complications in frail surgical patients; (5) barriers to implementing interventional program in geriatric surgical oncology; and (6) establishment of patient-centered goals of care in frail patients. Our objective is to demonstrate that frailty assessments are paramount for surgeons to tailor treatment plans and optimize outcomes while enhancing patient preferences. We performed a literature review using PubMed, Embase, World Wide Web, CINAHL, and Cochrane Library databases searching for studies published between 1 January 2000 and 31 May 2024 for each of the subheadings.
Available tools to measure frailty
With frailty screening becoming part of national practice guidelines/recommendations in several countries like the United States 15 and Britain (https://www.bgs.org.uk/cpocfrailty), it is paramount to identify the right tools to measure frailty. There are many frailty risk assessment tools and scoring systems that have been widely used in assessing patients for frailty. Between 2001 and 2023, close to 70 frailty scales have been developed worldwide, as discussed in a recent review on global frailty screening tools. 16 Some of the most commonly used frailty assessment tools include the FFP, modified frailty index (mFI), Memorial Sloan Kettering–frailty index (MSK-FI), the Comprehensive Geriatric Assessment (CGA), the Edmonton Frailty Scale (EFS), the Flemish version of the Triage Risk Screening Tool (fTRST), and the clinical frailty scale (CFS).17–19 Table 1 summarizes some of the most common frailty assessment tools used. Frailty screening tools vary in the criteria they use to make assessment, and in usability, and provider preferences. Most of these frailty measurement tools, particularly frailty indices, rely on quantifying the number of deficits among those assessed across multiple domains, including physical, psychological, and social aspects. 2 In contrast, some screening tools focus on various physical characteristics or phenotypes of frailty. Another subset of frailty screening tools relies on clinical judgment, as illustrated by the CFS, which is commonly used in geriatric medicine, due to its simplicity and effectiveness. 16 The CFS consists of nine items (for a total of nine points) with each point on the scale accompanied by a visual chart and a written description of frailty to help in its classification. 16 The scale ranges from 1 (very fit) to 9 (terminally ill), and scores equal to or above 5 denotes frailty. 16 The CGA is another relevant non-numerical tool used in geriatric medicine that encompasses multiple domains and problems encountered in the older adult, including functional status, comorbidities, cognitive and mental health, fatigue, socioeconomic and environmental factors, nutrition, presence of geriatric syndromes, and polypharmacy. 17
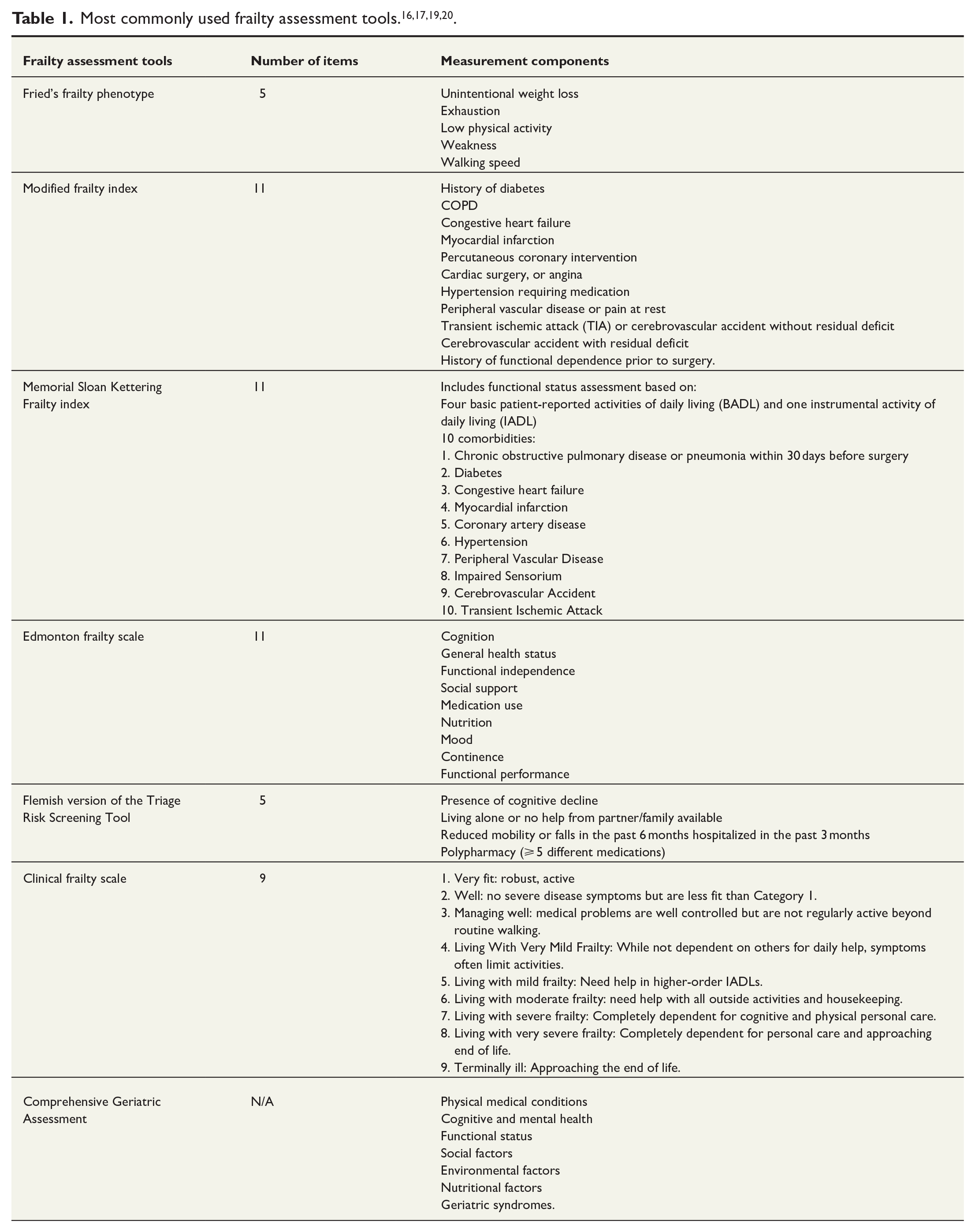
Within the surgical field, there is a lack of agreement on a single tool. 17 Presently, frailty tools such as the Frailty Index (FI) and mFI are most frequently used for preoperative frailty evaluation.17,21 The FI was developed using the Canadian Study of Health and Aging (CSHA) data and is a 70-item index that includes elements from patient history, physical exam, and laboratory values to identify and define factors influencing frailty.17,22 The mFI is a simplified adaptation of the original 70-item CSHA-FI and includes 11 items that are more feasible and easier to use in clinical practice.17,22 Factors included in the mFI include history of diabetes, chronic obstructive pulmonary disease (COPD), congestive heart failure, myocardial infarction, percutaneous coronary intervention, cardiac surgery, angina, hypertension requiring medication, peripheral vascular disease or pain at rest, transient ischemic attack or cerebrovascular accident without residual deficit, cerebrovascular accident with residual deficit, and history of functional dependence prior to surgery (Table 1).17,22,23 Each of the listed variables contributes 1 point to the total score.17,22 After adding up the points, the total is divided by 11 resulting in a scale ranging from 0 to 1.0, and an mFI score > 0.36 indicates frailty.17,22 In summary, there are many frailty assessment tools available for use; however, it is important to note that not one singular tool has shown superiority.
Impact of frailty on postoperative outcomes
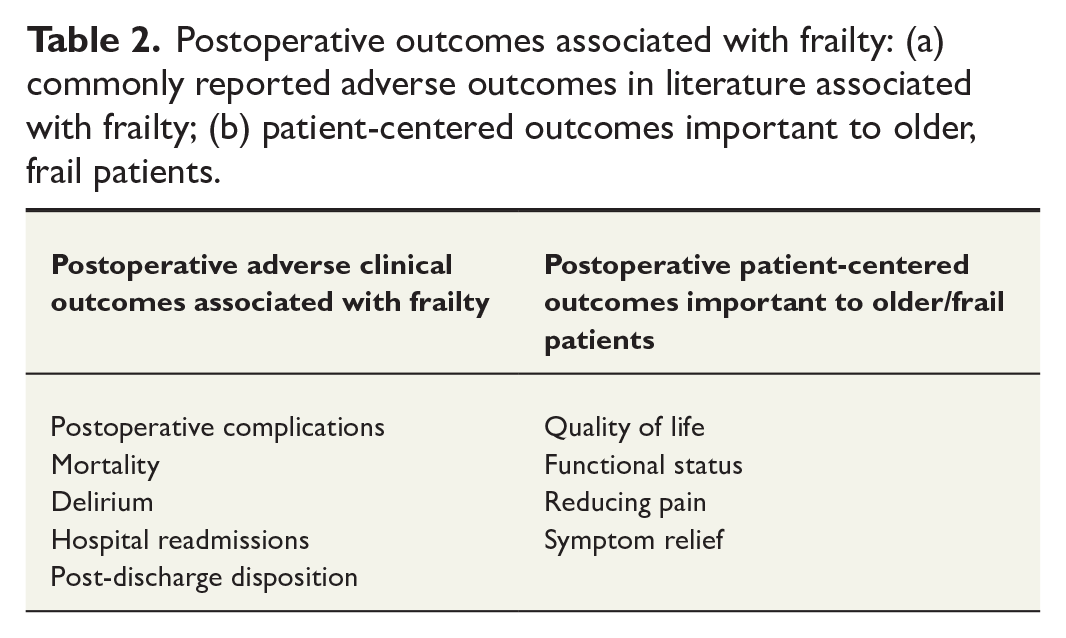
The surgical oncology subpopulation with frailty is characterized by even higher vulnerability due to the additional reduction of physiologic reserve from cancer. 24 This subpopulation is predisposed to unfavorable postoperative outcomes, including increased complications, mortality, delirium, hospital readmissions, and suboptimal discharge disposition (Table 2).
Postoperative outcomes associated with frailty: (a) commonly reported adverse outcomes in literature associated with frailty; (b) patient-centered outcomes important to older, frail patients.
Postoperative complications
In a systematic review and meta-analysis investigating the association between FRAIL scale and postoperative complications in older surgical patients, Gong et al. 25 found that postoperative complications, including cardiovascular, respiratory, infectious, and renal failure, were significantly higher for frail compared with non-frail patients with an odds ratio of 3.11. In a separate retrospective cohort study to examine the relationship between frailty and anastomotic leak after an elective colectomy, Dressler et al. 26 found that frail patients were at increased odds of anastomotic leak compared with non-frail patients with an odds ratio as high as 2.41 (95% CI 1.47–3.96) in patients with mFI score of 3. The authors also demonstrated that rescuing this subset of frail patients who experienced an anastomotic leak event appeared even more challenging with a greater proportion of frail patients experiencing mortality (5.9% versus 3.4%), septic shock (21.0% versus 16.1%), myocardial infarction (2.9% versus 1.1%), and pneumonia (11.8% versus 6.8%) compared with non-frail patients after an anastomotic leak. 26
Mortality
There is much research dedicated to examining the relationship between frailty and mortality after surgery. Geroge et al. performed a cohort study across nine noncardiac specialties and categorized procedures according to operative stress score and by case-mix (i.e. low intensity, moderate intensity, high intensity). 27 The authors found that frailty was associated with postoperative mortality across all noncardiac surgeries regardless of the case-mix. 27 In another study involving adults who underwent elective oncologic surgery, it was observed that individuals with higher levels of frailty experienced reduced long-term survival when compared to those with lower frailty levels. 28 Using a frailty index developed and validated for population-based health administrative data, this study found that every 10% increase in the frailty index corresponded to 1.60-fold relative decrease in survival. 28
Delirium
As discussed in the next section, frail patients typically have multiple comorbidities, including cognitive impairment, which increases the risk for delirium after undergoing surgery. In addition, the use of anesthesia, hospitalization and unfamiliar surroundings, postoperative pain medications, and acute illness alone can further exacerbate the risk of developing postoperative delirium in this population. In a recent meta-analysis examining the relationship between preoperative frailty and postoperative delirium in adults 65 years and older undergoing elective surgeries, it was found that these patients have greater odds of developing postoperative delirium compared with non-frail patients of the same age with an odds ratio of 2.14 (95% CI 1.43–3.19). 8 With the incidence of postoperative delirium in patients undergoing noncardiac surgery reportedly ranging between 15% and 54%, the risk of postoperative delirium in frail patients can be very significant. 29 Preoperative geriatric assessments and screening for frailty can help identify delirium risk factors in surgical patients, thus allowing the subsequent implementation of delirium prevention protocols in this subpopulation prior to undergoing surgery. A retrospective review of surgical oncology patients who underwent preoperative CGA at Memorial Sloan Kettering Cancer Center revealed the incidence of delirium in this population to be relatively low at 19% and suggest the importance of geriatric assessments to mitigate risk of postoperative delirium. 30
Readmissions
Frail patients are more likely to be readmitted to the hospital after undergoing surgery. A retrospective cohort study conducted on older adults at the Veterans Affair (VA) hospitals undergoing orthopedic, general, and vascular surgeries found that frailty measured by mFI was independently associated with 30-day readmissions. 9 The lowest readmission rate (7.9%) was among patients with no frailty components, and the highest readmission rate (42.9%) was among patients with highest number of frailty components. 9 In 2020, Tatar et al. 10 used the mFI to study readmissions after elective colorectal surgery for patients with cancer and found that mFI correlated with readmissions in this group of cancer patients.
Discharge disposition
Discharge disposition planning begins in the preoperative phase and entails an array of assessments and screenings to help in the decision-making process. Screening patients for frailty can help plan for a patient’s discharge disposition. In a systematic review and meta-analysis, Shaw et al. studied the association of frailty with postoperative discharge disposition in patients undergoing cancer surgery and found that frailty was significantly associated with adjusted discharge disposition, which was defined in this study as discharge to a rehabilitation facility, acute care facility, skilled nursing facility, or other nonhome location. 31 In another review that included 20 studies on the evaluation of postoperative transitions in care for older adults undergoing major surgery, only two articles evaluated and reported frailty in the study population. This suggests that screening for frailty as part of postoperative discharge planning is not yet standardized practice. Implementing this however can deeply impact the process and help formulate appropriate care plans that accommodate the preferences and needs of the frail older adult patient, reducing suboptimal discharges. 32
Geriatric syndromes and frailty
The term “geriatric syndromes” does not correspond to a specific illness or a disease group but is a constellation of common health conditions occurring in the older adult that influences functional status and quality of life (QOL). 33 Some of the most common geriatric syndromes associated with frailty include malnutrition, falls, dementia, and polypharmacy. These are important pieces to consider together when evaluating patients with frailty undergoing surgery.
Geriatric surgical oncology patients are highly susceptible to malnourishment. This leads to increased risk of frailty through different mechanisms, including muscle atrophy and loss of muscle mass, functional and cognitive decline, and chronic inflammation. Poor nutrition with frailty is also associated with 90-day postoperative mortality. 34 Fortunately, studies suggest nutrition is a reversible and modifiable risk factor for frailty, particularly when healthier dietary changes are implemented along with a multi-domain approach using nutrition supplements combined with exercise training regimens. 35
History of falls is part of the geriatric syndrome with an association to worse postoperative outcomes. Jones, et al., performed a prospective cohort study of 235 subjects aged 65 years and older undergoing elective colorectal and cardiac operations. 36 The predictor variable—report from the subject stating a history of having fallen in the 6 months prior to the operation—was associated with a significantly higher 30-day complications in both colorectal (59% versus 25%) and cardiac (39% versus 15%) surgeries compared to nonfallers. 36 Notably, the authors also reported that the prevalence of preoperative fall history was prevalent (33%) in subjects aged 65 years and older. 36
Frailty also often exists with cognitive impairment. 37 A recent systematic review reported high prevalence of frailty in older adults, 65 years of age and above, who are living with dementia. Koria et al. found that frailty prevalence can range from 50.8% to 91.8% in the acute care setting, and from 24.3% to 98.9% in the community setting. 37 This presents a challenge in surgical decision-making capacity, which is further complicated by the fact that the existence of both frailty and cognitive impairment has been linked to a significantly higher likelihood of experiencing adverse postoperative outcomes and complications, highlighting the importance of cognitive impairment assessments in patients with frailty.25,38
In the context of polypharmacy, frail older adults tend to have a complex medication regimen that may be very challenging to navigate through secondary to drug-to-drug interactions, side effects, and medication compliance. 39 However, little is known in the literature about specific guidelines on managing polypharmacy in the frail population undergoing surgery. In one recent retrospective cohort study, Jónsdóttir et al. looked at the incidence of polypharmacy in the surgical patients older than or equal to 18 years of age, and found a high incidence of 33.4% in new postoperative polypharmacy (5–9 medications) and hyper-polypharmacy (greater than or equal to 10 medications). 40 For patients with existing preoperative polypharmacy, the incidence of postoperative hyper-polypharmacy was 16.3%. 40 Given the number of associated comorbidities in a frail patient, these numbers are likely significantly higher and needs to be considered preoperatively. The postoperative pain assessment and management of the frail older adult also present significant challenges along with polypharmacy, as these patients depend more on opioids for pain relief compared to their non-frail cohorts making them more vulnerable to risk of side effects and drug-to-drug interactions.41,42
Intervention programs for frail surgical patients
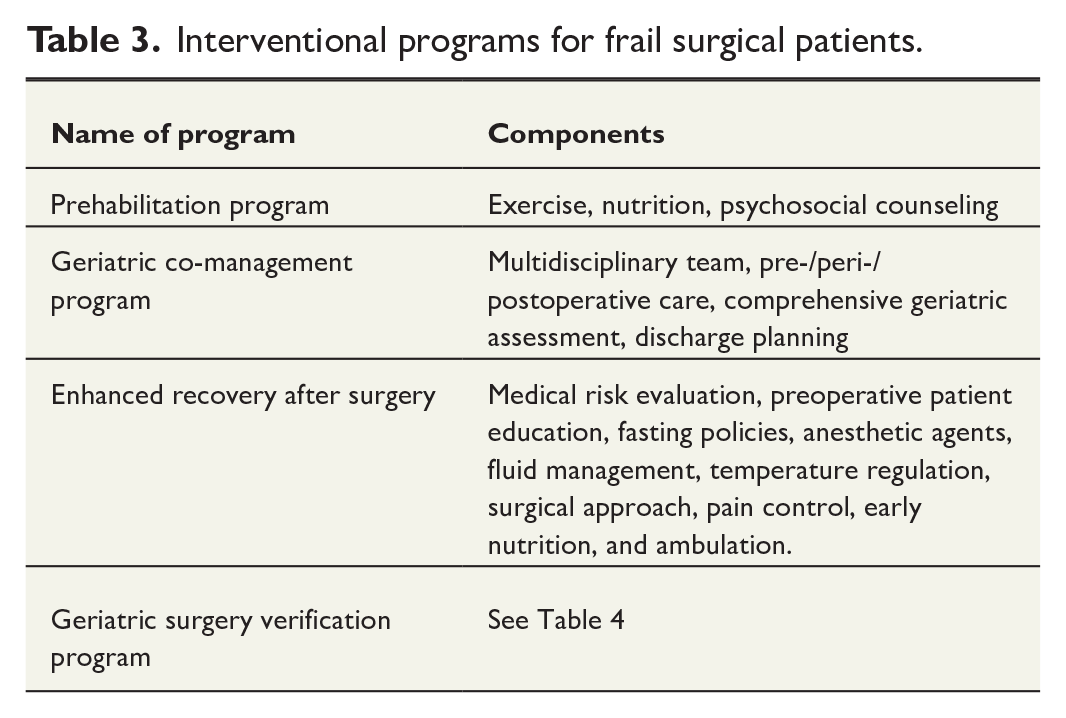
To lessen the severity of unfavorable consequences of frailty in surgical patients, interventional programs have been developed to improve patient outcomes (Table 3).
Interventional programs for frail surgical patients.
Prehabilitation programs
Prehabilitation programs are programs that entail a multidisciplinary and inclusive approach to managing postoperative health. These holistic programs focus on different aspects of postoperative recovery, including functional, behavioral, and social components. 12 In a systematic review published in 2020, Gracie et al. evaluated the influence of prehabilitation on postoperative outcomes in frail surgical patients. The authors found that prehabilitation programs, which encompassed exercise, nutrition, and psychosocial counseling, were a cost-effective method to decrease adverse postoperative outcomes. 12 In surgical oncology patients, Berkel et al. conducted a randomized controlled trial to evaluate the effects of a 3-week community-based exercise program on 30-day postoperative complications in high-risk patients and found that the rate of postoperative complications was significantly lower in the prehabilitation group (32.7%) compared with the control group receiving standard care (58%).43,44
Geriatric co-management programs
Geriatric co-management programs are programs where geriatricians work with other providers in different specialties to help coordinate the demands and needs of the older adult patient. In surgery, co-management programs have been established in different specialties, including orthopedic, trauma, neurosurgery, vascular, and oncologic surgery, with the aim of optimizing outcomes during the pre-, peri-, and postoperative periods. 45 McMillan et al. 46 demonstrated that the implementation of geriatric co-management programs in older adult patients with cancer undergoing elective cancer surgery is associated with lower 90-day postoperative mortality. The authors also found that the benefits of geriatric co-management are independent of the degree of patient frailty meaning that geriatric co-management benefits all older surgical patients and not just the frail. 46
Enhanced recovery after surgery
The ERAS protocols represent an integrated multidisciplinary approach consisting of principles targeted at optimizing perioperative process of care. 13 Key components of ERAS pathway principles include (1) preoperative strategies, such as medical risk evaluation, prehabilitation, patient education, and fasting policies; (2) intraoperative strategies, consisting of use or proper anesthetic agents, lung-protective ventilation, fluid management, temperature regulation, and appropriate surgical approach; and (3) postoperative strategies, such as pain control and prevention of nausea and vomiting and enabling early nutrition and ambulation.47,48 In surgical oncology, a review article published in 2022 highlighted that ERAS protocols have been associated with less postoperative complications and increased return to intended oncologic treatment. 49 In colorectal surgeries in particular, ERAS protocols and pathways have been shown to decrease postoperative complications and hospital length of stay.48,50,51 Specific to older adults, Tejedor et al. conducted a retrospective cohort study demonstrating that ERAS protocol implementation in older adults ≥ 70 years of age undergoing elective colorectal cancer surgery had a significant impact on decreasing major postoperative complications, anastomotic leakage, postoperative mortality, and length of stay when compared to a control group without ERAS protocol. 52 No studies have been performed to our knowledge that looked at ERAS protocol implementation specifically in frail patients.
Geriatric surgery verification program
The GSV initiative is a program consisting of 32 GSV evidence-based standards (Table 4) developed in 2019 by the American college of Surgeons with support from The John A. Hartford Foundation.14,53,54 The program is designed to improve and enhance surgical outcomes in the vulnerable geriatric surgical patient by employing early intervention and prevention policies, thus maximizing therapeutic responses through a collaborative team approach. 14 The key components of the program include emphasis on multidisciplinary care, comprehensive geriatric perioperative assessments, and patient-centered care focused on addressing patient-specific needs and preferences. The literature regarding GSV implementation in surgery is expanding across different subspecialties. In colorectal surgery, GSV implementation has helped physicians screen and identify older adults at risk for adverse surgical outcomes, such as postoperative delirium. 54 Training modules and courses have also been developed to educate hospital staff and physicians on how to implement these standards, with the aim of identifying frailty in this surgical subpopulation and managing geriatric syndromes during and after the surgery. 54
GSV program standards.
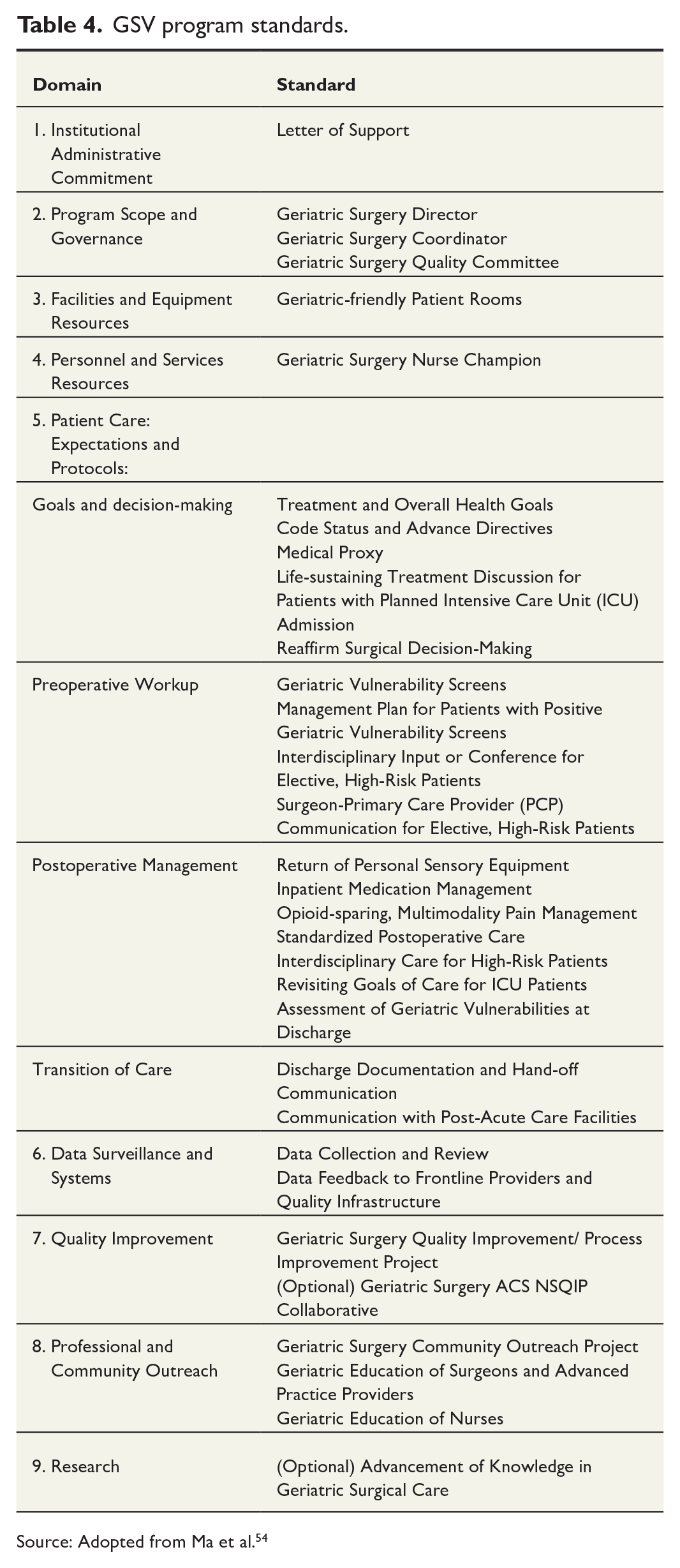
Source: Adopted from Ma et al. 54
Barriers to implementing interventional programs
The above intervention programs have contributed to decreasing adverse outcomes leading to improved QOL. Despite these programs being readily applied, there remain barriers in implementation. These barriers exist at various levels, including provider-, patient-, and system-levels.
At provider-level, it is challenging to navigate through multidisciplinary team approaches and care coordination among different staff members, including surgeons, other specialists, registered nurses, nurse navigators, and social workers. There needs to be enough time and resources for staff and providers to be able to perform all the appropriate assessments and screening tools required. Due to the time commitment, provider documentation can also be adversely affected, and that is when providers focus on documenting procedural goals and expectations, rather than patient needs and preferences. 55 Healthcare providers also need to be educated on the practices and standards of the above interventions, even before implementing them. At the patient level, it becomes difficult to comply and adhere to these interventions for several reasons, including poor health literacy and reluctance of taking part in a time-consuming protocol. 55 Finally, it is also financially demanding at the system level to provide all the resources necessary to implement these programs as hospitals must devote appropriate staffing and equipment needed to carry out these interventions. Some of the above barriers can be mitigated by the presence of a nurse navigator and involvement of palliative care team.
Nurse navigators’ roles are crucial in overcoming many barriers to a successful perioperative interventional program for frail patients, particularly within the GSV program. An oncology nurse navigator is defined as a professional RN with clinical knowledge in oncology to offer individualized assistance to patients, families, and caregivers to overcome healthcare system barriers. They oversee the patient's journey from initial identification through preoperative assessment, optimization of perioperative and postoperative care, patient education, and postoperative follow-up. Palliative care team services have been increasingly used in the past decade in surgical oncology in the preoperative phase, but there remain no guidelines as to which patients will benefit most from these services. 56 In a recent article, Tao et al. discussed the potential role of frailty in determining which patients are referred for a palliative care consultation and reported how frail cancer patients may benefit even more from these services, as these consultations target specifically the vulnerabilities associated with frailty. 56
Establishing patient-centered goals of care in frail patients
It is imperative to discuss goals of care when managing frail patients in the surgical oncology population. The multicenter Geriatric Surgical Assessment and Functional rEcovery after Surgery (GOSAFE) Study was one of the fundamental studies published in 2022 that reported on QOL as an outcome measure after cancer surgery and found that in addition to being treated for cancer and lessening the burden of the disease, the authors demonstrate that older adults aspire to improve other outcome measures as well, including functionality, independence, and maintaining or even improving the QOL. 57
Areas of preoperative discussion to consider include questions related to maintaining independence or improving functional status, improving QOL, and reducing pain or other burdensome symptoms. One method of answering these important questions is through “Patient-reported Outcome Measures,” or PROM questionnaires. 58 These questionnaires are self-completed tools that focus on the patient’s view of their health status at a given point in time and include the patient’s functional status, psychological well-being, and QOL.58,59 These questionnaires have been useful across different areas of study, including surgical oncology, as they help to identify the impact of surgical treatment on a patient’s QOL.58,60
Conclusion
Frailty is a geriatric syndrome that is becoming increasingly recognized as an important patient factor in surgical oncology. Frailty has been associated with adverse outcomes, including greater 30-day mortality, greater odds of developing postoperative delirium, higher readmission rates, unfavorable discharge dispositions, and increased risk of postoperative complications including wound complications and anastomotic leaks. Increasing data continue to emerge on the importance of frailty assessment and frailty screening tools in preoperative evaluation. Multiple frailty assessment tools have been developed with many showing ease of use, though none has demonstrated superiority. These tools have shown that the prevalence of frailty varies across different types of surgeries, including high-, medium-, and low-risk surgeries. Several interventional programs have been developed to reduce the negative impact of frailty, including geriatric co-management program, which is an emerging intervention that emphasizes the vital role of the geriatrician in helping surgical teams manage the complex medical conditions of the frail older adult perioperatively. Frailty assessment has also enabled surgeons to focus on what matters most to patients and what is important to them, addressing conversations regarding goals of care and QOL. There is considerable room for further research in the field of frailty and its implications in surgical oncology, particularly on topics relating to the coordination of care among different specialists and the role of each team member.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.