
Abstract
Background and aims:
Patients with small intestinal neuroendocrine tumors (siNETs) frequently present emergently due to bowel ischemia or bowel obstruction. The influence of emergency surgery on the prognosis of siNET remains controversial. The aim of this study was to investigate the association between type of presentation (emergency/elective) and oncological outcome.
Methods:
Clinicopathological data of patients who underwent bowel resection and were treated due to siNET at the Charité — Universitätsmedizin Berlin, Germany were analyzed retrospectively.
Results:
A total of 165 patients underwent bowel resection for siNET. Of these, 22.4% (n = 37) were emergency and 77.6% (n = 128) were elective procedures. A preoperative known diagnosis was less common in patients with emergency surgery (48.6% vs 85.2%; p < 0.001) and complete resections of all tumor manifestations were performed less often (32.4% vs 50.8%; p = 0.049), while more completion operations had to be performed (24.3% vs 11.1%; p = 0.049). Overall survival (OS) and progression-free survival (PFS) of emergently operated patients were reduced (5-year OS: 85.2% vs 89.5% (p = 0.023); 5-year PFS: 26.7% versus 52.5% (p = 0.018)). In addition, emergency surgery was negatively associated with OS after multivariable regression analysis.
Conclusion:
Emergency surgery in siNET patients is associated with adverse oncological outcomes including shorter OS and PFS. Prevention of emergency conditions should be emphasized in advanced disease.
Twitter summary
A relevant part of patients suffering from small intestinal neuroendocrine tumors (siNETs) present with conditions requiring emergency surgery such as small bowel obstruction or bowel ischemia. Analyses of the impact of emergency surgery on oncological outcome in these patients revealed conflicting results. This study includes a retrospective outcome analysis of siNET patients treated at Charité — Universitätsmedizin Berlin comparing patients operated in elective and emergency settings. We demonstrate impaired overall and progression-free survival in siNET patients undergoing emergency surgery. The findings suggest that in siNET patients adequate diagnostic work-up and early elective surgery should be promoted to prevent NET-associated complications and the need for emergency surgery. Moreover, more intense follow-up and more aggressive medical therapy management in siNET patients following emergency surgery should be discussed.
Context and relevance
A relevant part of patients suffering from siNETs present with conditions requiring emergency surgery such as small bowel obstruction or bowel ischemia. Until now, analyses of the impact of emergency surgery on oncological outcome in these patients revealed conflicting results. This study includes outcome analyses of patients undergoing small bowel resection for siNET comparing patients operated in elective and emergency settings. We demonstrated impaired overall and progression-free survival in siNET patients undergoing emergency surgery. Possible reasons were fewer curative operations, higher incidence of carcinoid heart disease and increased number of patients with distant metastases. Emergency surgery was found a negative prognostic factor for overall survival. This finding promotes adequate diagnostic work-up and early elective surgery to prevent NET-associated complications and the need for emergency surgery. Finally, closer postoperative follow-up and therapy management in siNET patients following emergency surgery should be discussed.
Introduction
Small intestinal neuroendocrine tumors (SiNETs) are the most common subtype within the group of gastroenteropancreatic NETs. 1 Symptoms usually appear in advanced stages and may include unspecific symptoms, for example, abdominal pain or gastrointestinal bleeding as well as hormone-related symptoms such as diarrhea and flushing. Owing to this relatively indolent behavior, most siNETs are diagnosed when already metastasized to lymph nodes or distant organs. 2 The only curative treatment is surgical resection of all tumor manifestations. However, even patients with metastatic and/or unresectable disease face a relatively good prognosis, especially in well and moderately differentiated tumors. 3
In many cases, mesenteric fibrotic mass formation occurs around lymph node metastases due to a so-called desmoplastic reaction, which can be detected radiologically by its characteristic stellate or spoke-wheel appearance.4,5 Mesenteric fibrosis can lead to various complications, including deterioration of bowel function, which can result in acute bowel obstruction or intestinal ischemia. 6 Patients presenting with these conditions often require emergency surgery, leaving little time for additional diagnostics. Recommendations for appropriate management in such are vague, and evidence on oncological outcome is scarce. Some studies indicate comparable outcomes for emergency and elective surgery in siNET patients, 7 while others report earlier disease recurrence and shorter survival for patients undergoing emergency surgery.3,8 Elective surgery, on the contrary, is typically performed in patients with histologically proven siNET, often diagnosed by colonoscopy or the detection of liver metastases. Nevertheless, the timing of surgery for patients with distant metastases remains a critical and individualized decision, essential for effectively preventing acute bowel obstruction or ischemia.9,10
In gastrointestinal surgery, studies show poorer postoperative outcomes in emergency patients, with higher complications rates and short-term mortality compared to elective patients.11,12 In malignant diseases, such as colorectal cancer, initial emergency surgery is associated with impaired long-time oncological outcome.13–15
Since emergencies requiring immediate surgery are unpredictable, understanding their impact on oncological outcomes is crucial. This study aimed to evaluate the association between emergency or elective surgery and oncological outcome in siNET patients. We hypothesized that emergency surgery is a risk factor for impaired outcome.
Methods
Patient demographic and clinical data
Patients treated for siNET at the European Neuroendocrine Tumor Society (ENETS) Center of Excellence at the Charité — Universitätsmedizin Berlin, Germany between January 2010 and December 2020 were identified from the Charité Comprehensive Cancer Center (CCCC) database. The study included patients who underwent resection of the primary tumor; with diagnosis established either prior, during, or after surgery. Exclusion criteria were non-resection of the primary tumor, age under 18 years, G3 NETs, neuroendocrine carcinomas, and missing data on urgency indication. Data retrieved from medical charts included age, sex, American Society of Anesthesiologists (ASA) status, tumor stage (UICC 8th edition), 16 tumor node metastasis (TNM) classification and tumor grading according to the World Health Organization (WHO) grading system. Carcinoid syndrome was defined as the combination of flushing and diarrhea and/or wheezing; carcinoid heart disease (CHD) was defined as the presence of tricuspid valve insufficiency diagnosed by echocardiography. Lymph node spread patterns were classified into locoregional (stage I–II according to Ohrvall et al.), 17 central (stage III), and extended central including retroperitoneally extending lymph nodes and peripancreatic lymph nodes (stage IV). Hepatic tumor burden was identified via cross-sectional imaging. Time to surgery was calculated as time from diagnosis to surgery.
Surgery and histopathological data
Independent of preoperatively known siNET, indication for bowel resection was divided into elective surgery, including all electively planned abdominal surgeries, and emergency surgery, including all high urgent and emergency operations due to acute conditions requiring urgent surgery. The performance of systematic lymphadenectomy (LAD) was assessed. Details about resection margins and residual tumor classification (R status) were collected from the histopathological report. R status was defined as no (R0), microscopic (R1), and macroscopic (R2) evidence of residual tumor tissue. Bowel resections were grouped into partial ileal resection, ileocecal resection, right hemicolectomy, extended right hemicolectomy, right hemicolectomy and partial ileal resection, and other. Procedures including right hemicolectomy with/without small bowel resections were defined as extended resections. The resection was considered complete if all macroscopic tumor mass was removed and as incomplete if only tumor mass reduction could be achieved. This included cases where the primary and lymph node metastases were fully removed, but distant metastases remained. Secondary resections following incomplete primary resections were termed completion surgery. Postoperative complications were classified according to Clavien–Dindo; major complications were defined as ⩾3a. 18
Follow-up parameters
Patients were followed up according to the ENETS consensus guidelines 19 with data included through 31 December 2022. Disease progression was determined by an interdisciplinary tumor board based on clinical assessment, laboratory markers (Chromogranin A), and cross-sectional imaging (computed tomography [CT] or magnetic resonance imaging [MRI] and somatostatin receptor imaging) according to the response evaluation criteria in solid tumors (RECIST, version 1.1). 20 NET-related deaths including those due to siNET metastasis, tumor compression, CHD, or other conditions attributable to advanced siNET disease, were recorded based on medical records. Usage of adjuvant therapies was assessed.
Statistical analysis
Continuous variables are presented as medians (range) and categorical variables as frequencies and percentage. Group comparisons for continuous variables were performed using either the Mann–Whitney U-test or Kruskal–Wallis test. For categorical variables, the chi-square test or Fisher’s exact test were used. Survival analyses were performed according to the Kaplan–Meier method; survival rates were compared using log-rank tests. Overall survival (OS) was defined as time between bowel resection and death, progression-free survival (PFS) as time between bowel resection and first postoperative progress. Patients who did not reach the endpoints or were lost to follow-up were censored at the last follow-up visit. Univariable Cox regression analysis identified potential factors influencing OS and PFS with results displayed as hazard ratio (HR) with 95% confidence interval (95% CI). Multivariable Cox regression adjusted for confounders, including covariates with p < 0.1 in the univariable analysis. For OS, up to three variables were included, following the rule of 10 events per variable.21,22 Known confounders for emergency surgery and OS included age, 3 ASA score,15,23 and preoperative diagnosis, 3 of which age and ASA score were included. For PFS, up to nine variables could be included. Advanced tumor size (T3/T4),7,8 lymph node metastasis (N1 status),8,24,25 and distant metastasis.25,26 were identified as additional potential confounders.
Statistical analyses were performed using SPSS Statistics software, version 27 (IBM Armonk, NY, USA). Missing data were indicated and were excluded analysis by analysis. The significance level was set to 0.05. The study was approved by the local Institutional Ethics Committee of Charité — Universitätsmedizin Berlin (EA2/064/09) and was conducted in accordance with the Declaration of Helsinki. All patients provided informed consent for registry participation, data collection, and analysis.
Results
Patient characteristics
Five hundred and ten patients with siNET were identified from the CCCC database, and 165 patients met the inclusion criteria (Fig. 1). Of these, n = 128 were operated in an elective setting, while n = 37 were emergency surgeries.
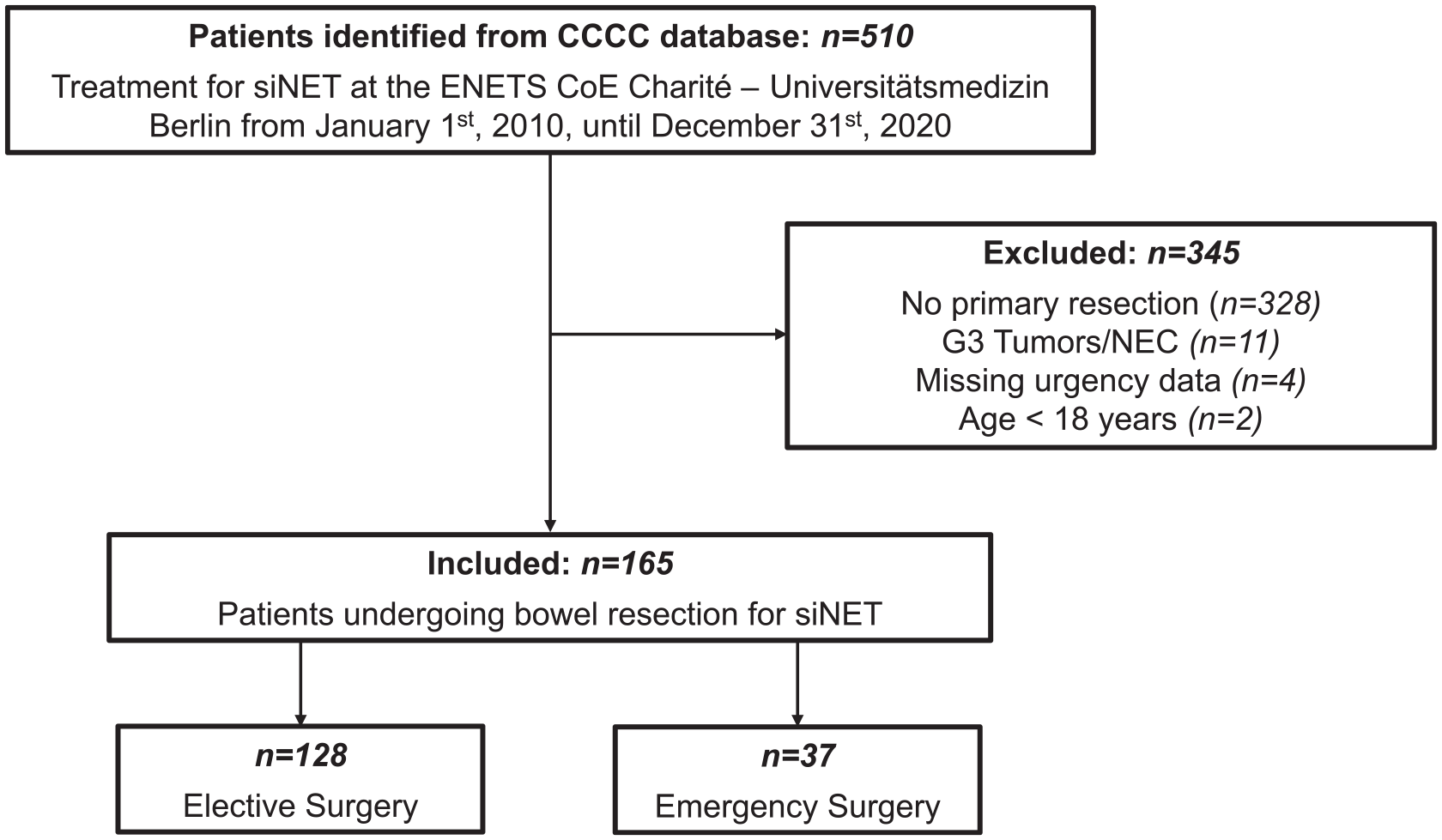
Patient inclusion and exclusion. siNET; small intestinal neuroendocrine tumor; CoE, center of excellence; NEC, neuroendocrine carcinoma.
Comparison of elective and emergency patients
Patient characteristics and a comparison between elective and emergency surgery cohorts are shown in Table 1. In the emergency group, the diagnosis was more often known preoperatively, and extended and complete resections were performed less frequently. Completion surgeries were more common, and adjuvant therapy including SSA therapy was used more frequently. Emergency patients had higher rates of postoperative disease recurrence or progression. They also tended to be older, have more T3/T4 tumors, higher 30-day mortality, more CHD, and more distant metastases, although these differences were not statistically significant. No differences were found regarding gender, ASA status, carcinoid syndrome, lymph node metastasis location, hepatic tumor burden, UICC stage, N stage, residual tumor classification, grading, Ki67, minor and major postoperative complications, 30-day morbidity, and multifocal tumor occurrence (Table 1).
Characteristics and comparison of siNET patients undergoing bowel resection in elective and emergency settings.
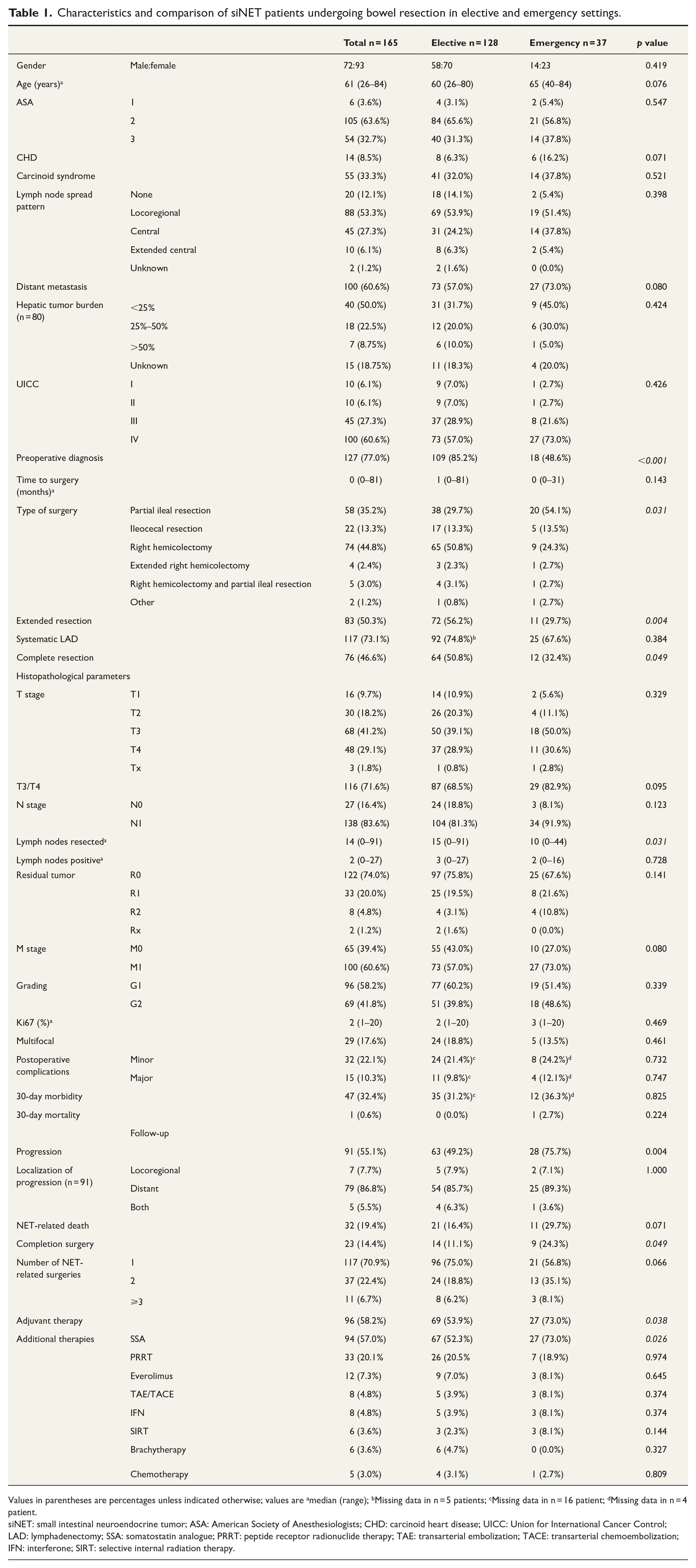
Values in parentheses are percentages unless indicated otherwise; values are amedian (range); bMissing data in n = 5 patients; cMissing data in n = 16 patient; dMissing data in n = 4 patient.
siNET: small intestinal neuroendocrine tumor; ASA: American Society of Anesthesiologists; CHD: carcinoid heart disease; UICC: Union for International Cancer Control; LAD: lymphadenectomy; SSA: somatostatin analogue; PRRT: peptide receptor radionuclide therapy; TAE: transarterial embolization; TACE: transarterial chemoembolization; IFN: interferone; SIRT: selective internal radiation therapy.
In the cohort of patients who underwent emergency surgery for siNET, the diagnosis was already established in n = 18 (48.6%) cases. The characteristics of these patients are detailed in Supplementary Table 1. Among those patients with a known diagnosis of siNET, n = 11 (61.1%) had planned surgery prior to emergency presentation, n = 4 (22.2%) had surgery recommended, and n = 3 (16.7%) were ineligible for surgery due to comorbidities including CHD. Seven patients were already receiving SSA therapy; and one patient had received peptide receptor radionuclide therapy (PRRT). Only time to surgery, which was shorter in patients without preoperative diagnosis, differed significantly.
Survival analysis
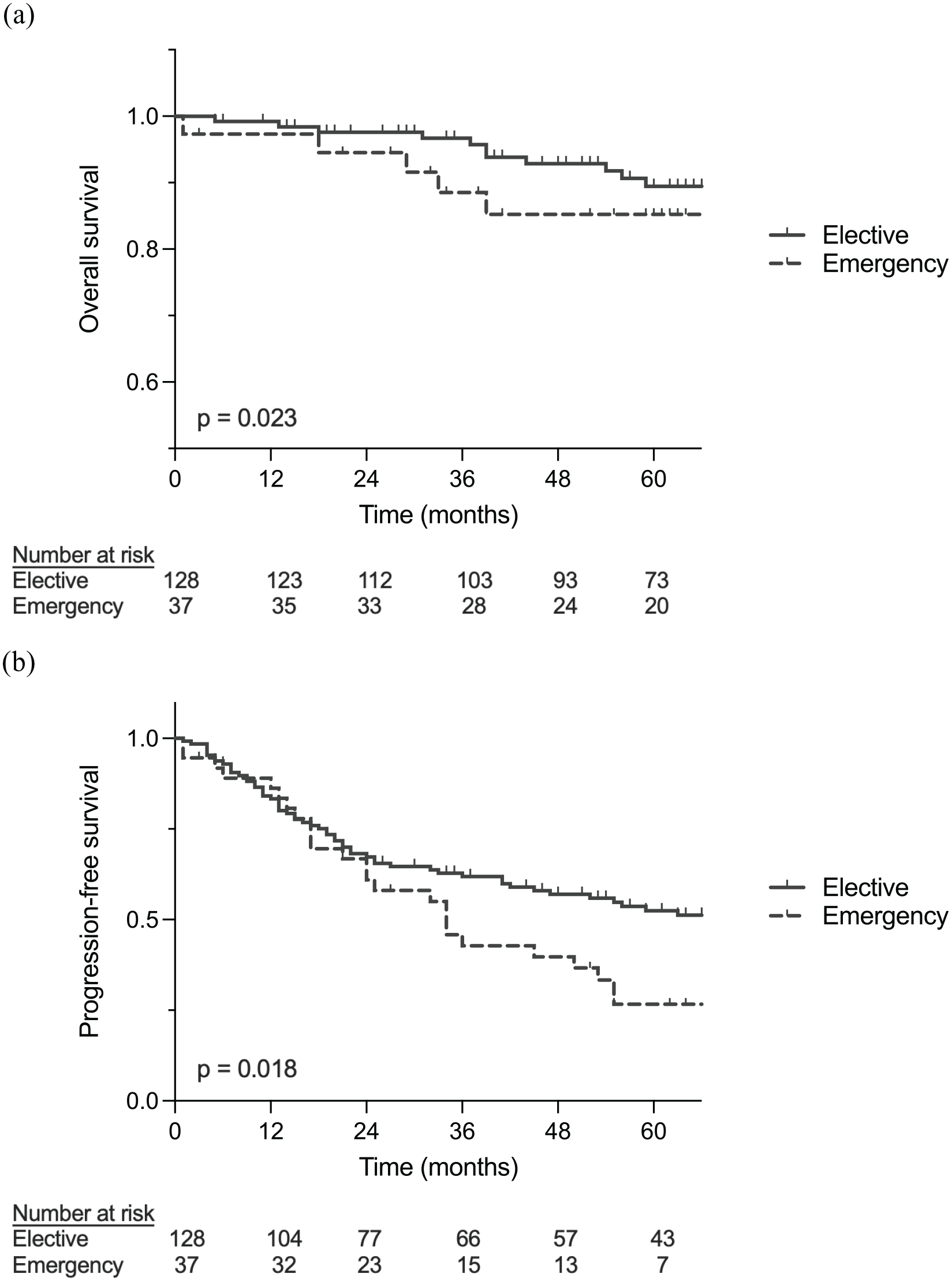
Within the median follow-up time of 66 months (interquartile range: 40–87 months), there were 32 (19.4%) deaths, with 21 in the elective cohort and 11 in the emergency group. Disease recurrence or progression was reported in 91 patients (55.1%), with 63 in the elective and n = 28 in the emergency group. As shown in Fig. 2A, OS in the elective surgery group was longer with a median estimated survival of 14.1 years (95% CI: 9.4–18.8) versus 8.3 years (95% CI: 3.3–13.4) and 5-year survival rates of 89.5% (95% CI: 82%–94%) compared to 85.2% (95% CI: 68%–94%). PFS was also longer in the elective surgery group with median estimated survivals of 6.1 years (95% CI: 3.9–8.2) versus 2.8 years (95% CI: 2.4–3.3) and a 5-year PFS rate of 52.5% (95% CI: 43%–61%) versus 26.7% (95% CI: 13%–42%) (Fig. 2B).
Comparison of
Cox proportional hazard model—Overall and progression-free survival
To identify the association of emergency surgery with OS and PFS, univariable and multivariable Cox regression analysis were performed. In the univariable model ASA3 status, carcinoid syndrome, emergency surgery, positive resection margins, distant metastases, tumor multifocality, and debulking surgery were identified as negative prognostic factors for OS (Table 2). After adjusting for confounding of age and ASA 3 in the multivariable regression analysis, emergency surgery was confirmed to increase the risk for impaired OS with an HR of 2.281 (95% CI: 1.077–4.834). Regarding PFS, univariable analysis revealed CHD, emergency surgery, T3/T4 status, N1 status, tumor grading, distant metastasis, and incomplete surgery as negative prognostic factors (Table 3). When adjusting for T3/T4 status, N1 status and distant metastasis, no effect of emergency surgery on PFS was observed.
Univariable and multivariable Cox regression analysis for variables affecting OS in siNET patients.
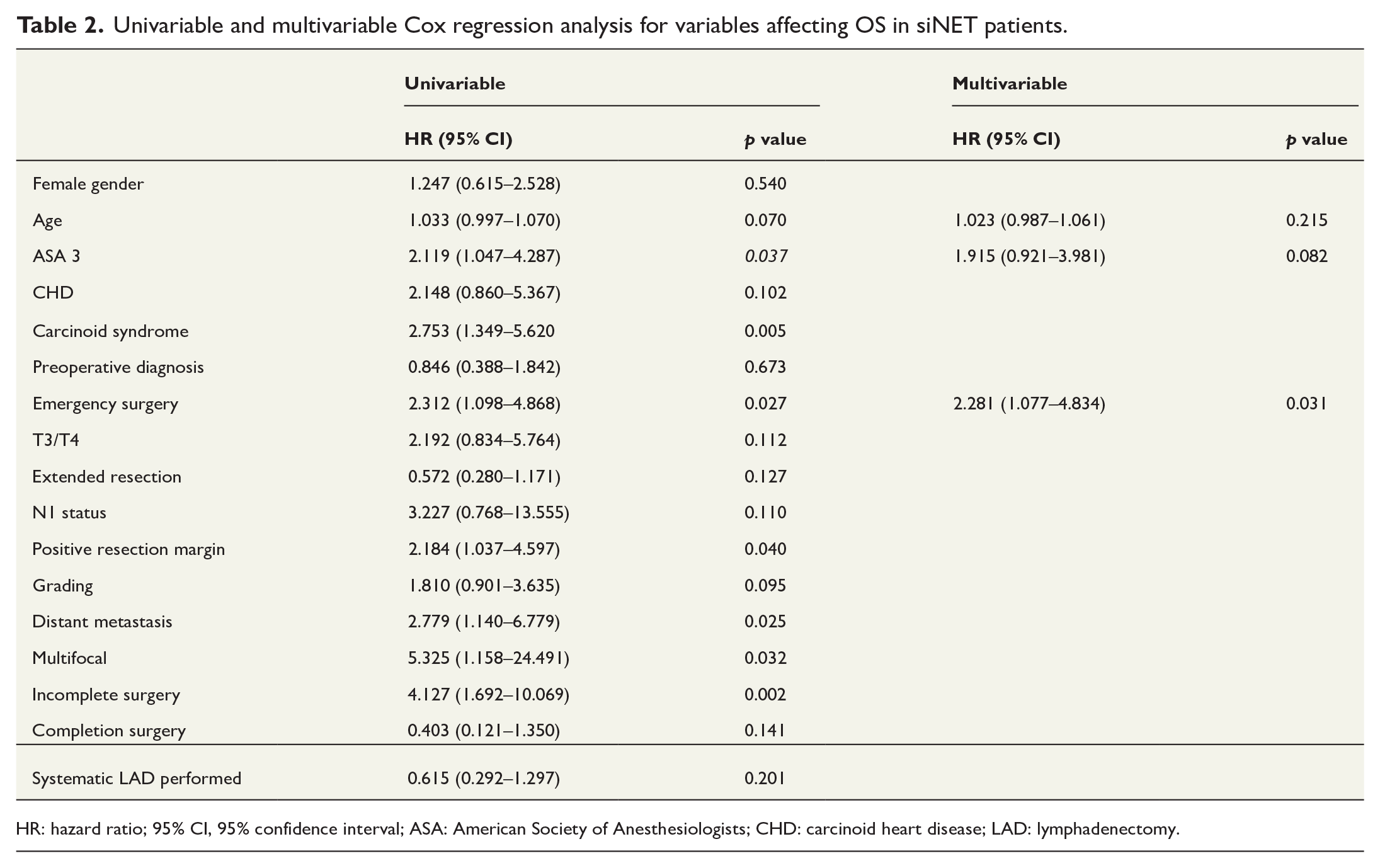
HR: hazard ratio; 95% CI, 95% confidence interval; ASA: American Society of Anesthesiologists; CHD: carcinoid heart disease; LAD: lymphadenectomy.
Univariable and multivariable Cox regression analysis for variables affecting PFS in siNET patients.
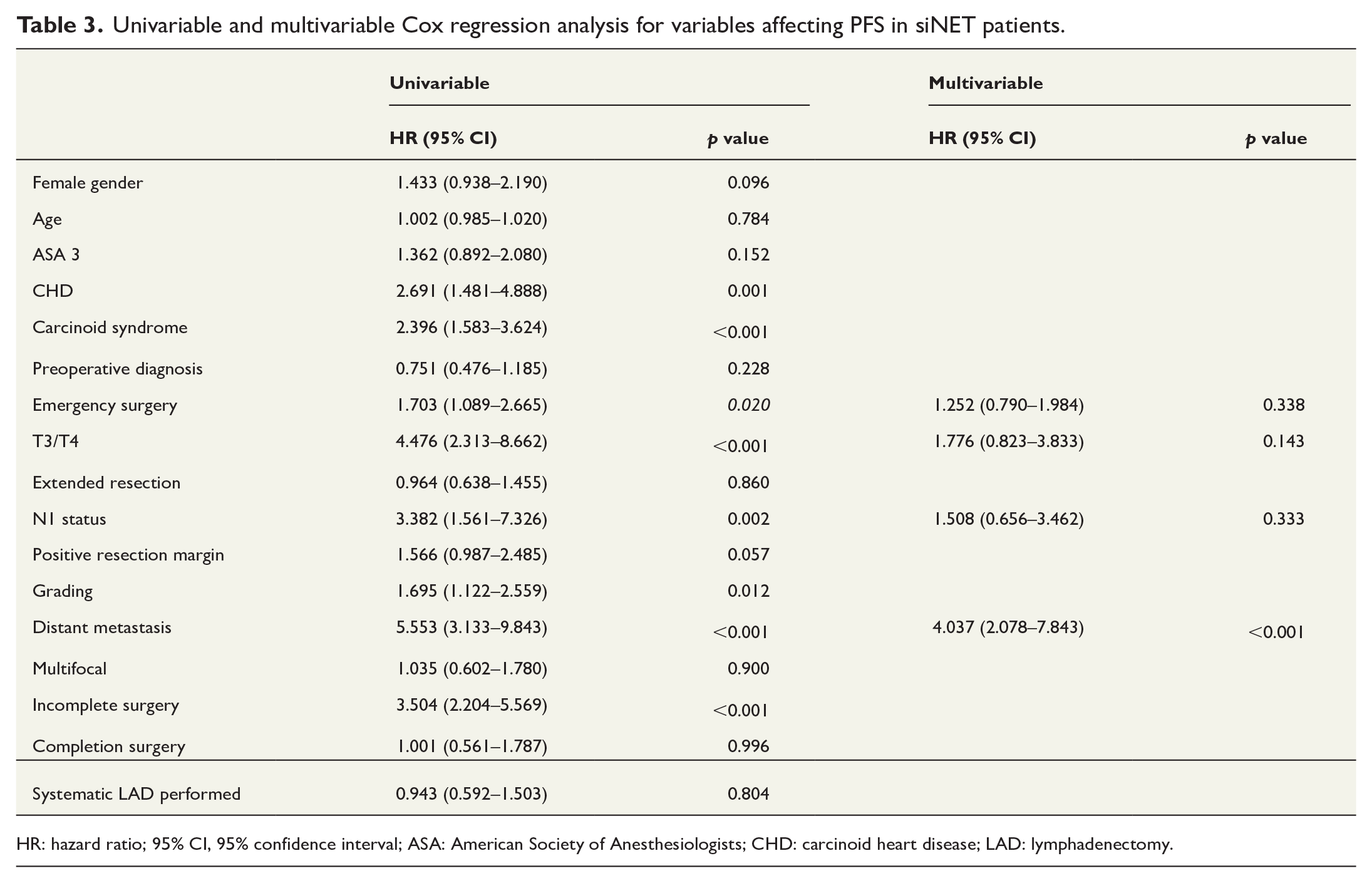
HR: hazard ratio; 95% CI, 95% confidence interval; ASA: American Society of Anesthesiologists; CHD: carcinoid heart disease; LAD: lymphadenectomy.
Discussion
There is conflicting evidence regarding the oncological outcomes of patients undergoing emergency surgery for siNET. In this study, both OS and PFS of siNET patients were impaired in siNET patients who underwent emergency surgery. Possible reasons included older age, fewer curative operations, higher incidence of CHD, and more patients with distant metastases. Multivariable analysis further identified emergency surgery as risk factor for impaired OS.
Consistent with the literature, all siNET patients in the study cohort had a relatively good prognosis with 5-year OS rates of 89.5% in elective and 85.2% in emergency surgery patients.27,28 When comparing the prognosis of elective and emergency siNET patients, the literature shows mixed results. Manguso et al. found no difference in oncological outcomes between siNET patients operated under elective and emergency conditions. 7 Eriksson et al. even identified emergency surgery as favorable prognostic factor for OS. However, in their study, around 75% of the elective cohort (n = 99) had stage-IV disease, whereas approximately 75% of the emergency group (n = 194) were in stage I–IIIb 29 suggesting that disease stage, a known prognostic factor, likely confounded the outcomes, favoring emergency patients. In contrast, Folkestad et al. 3 demonstrated shorter median OS in emergency patients and identified elective surgery as independent positive prognostic factor for survival, aligning with the results of this study.
The unfavorable oncological outcomes observed in siNET patients undergoing emergency surgery are consistent with findings from numerous studies highlighting worse outcomes after emergency surgery for gastrointestinal malignancies.13,14,15,30,31 In this study, emergency patients tended to be older, to have higher rates of CHD and distant metastases and tended to have larger tumors. Although these differences were not statistically significant, they indicate important trends regarding factors potentially influencing outcome differences between the two surgery cohorts. Age, CHD, UICC stage IV, and tumor size have previously been reported to negatively influence oncological outcome in siNET,32–36 indicating vulnerable patient groups that require vigilant monitoring. Multivariable analysis revealed an association between emergency surgery and OS even after adjustment for the known confounders age and overall health status. Consistent with the findings of Folkestad et al., no significant association between emergency indication and PFS was revealed after adjustment for T3/T4 stage, N1 stage, and distant metastasis. 3 These results suggest that the effect of emergency indication on — at least — PFS was confounded by, for example, advanced disease (UICC stage IV). In addition, other unknown confounding variables not included in this study must be considered. Further research with larger study cohorts is needed to identify additional prognostic factors for siNET prognosis.
Interestingly, nearly 50% of the emergency siNET patients had a preoperative NET diagnosis with recommended surgical therapy in most of these patients. About 78% (n = 14) of these patients had stage IV disease. Currently, surgery is recommended for unresectable advanced disease to prevent emergency conditions such as bowel obstruction or ischemia.9,10 Obviously, timing of surgery in these patients is of utmost importance. Preoperative surveillance to identify, for example, increasing sub-ileus conditions should be thoroughly performed.
Although patients with siNET have a relatively good prognosis, identification of risk factors for adverse outcome is of paramount importance for appropriate postoperative treatment and follow-up management. The presented data suggest an association between emergency surgery and poorer outcome, even after complete tumor resection. Current guidelines recommend follow-up examinations every 6–12 months in G1/G2 siNET patients after curative resection and every 3–6 months after debulking surgery. 19 Based on this study, closer follow-up of siNET patients after emergency surgery, including low-threshold indications for adjuvant therapy, should be discussed and encouraged.
The poorer survival of siNET patients undergoing emergency surgery, may stem from limited surgical radicality in the emergency setting. Achieving adequate oncological resection, including systematic LAD for siNET, is challenging and requires significant surgical experience. Despite fewer right hemicolectomies and more secondary completion surgeries in emergency cases, there were no differences in systematic LAD or R status. However, extended resection and completion surgery did not affect OS or PFS, suggesting these factors do not explain the outcome differences. Similarly to the findings of Manguso et al., this study noted fewer resected lymph nodes in the emergency cohort, although the number of positive lymph nodes was comparable. 7 However, with 15 and 10 resected lymph nodes in the respective groups, the numbers of resected lymph nodes were above the established threshold for adequate systematic LAD.9,37
This study has limitations. First, the study cohort is relatively small, although comprising 165 patients, which is substantial for a single-center study given the rarity of the disease. Second, this study was retrospective in nature. While prospective multicenter studies are necessary to elucidate oncological outcome and prognostic factors in siNET, well-conducted retrospective studies with comprehensive follow-up data may still provide valuable insights. This is particualary relevant for investigating the impact of emergency surgery in siNET, as randomized trials are not feasible. Despite including multivariable analysis to mitigate confounding effects of emergency verus elective surgery, residual unmeasured, and unknown confounding cannot be completely excluded.
Based on the results, emergency surgery correlated with poorer oncological outcome. Increased awareness for siNET is crucial to reduce diagnostic delays. Once diagnosed, identifying and monitoring patients at risk for emergency surgery is essential to prevent NET-associated complications and the need for emergency surgery.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969241271841 – Supplemental material for Emergency surgery influences oncological outcome in small intestinal neuroendocrine tumors
Supplemental material, sj-docx-1-sjs-10.1177_14574969241271841 for Emergency surgery influences oncological outcome in small intestinal neuroendocrine tumors by Frederike Butz, Leonie Supper, Lisa Reinhard, Agata Dukaczewska, Henning Jann, Uli Fehrenbach, Charlotte Friederike Müller-Debus, Tatiana Skachko, Johann Pratschke, Peter E. Goretzki, Martina T. Mogl and Eva M. Dobrindt in Scandinavian Journal of Surgery
Footnotes
Author contributions
Frederike Butz: Study conception and design, Acquisition of data, Analysis and interpretation of data, Drafting of manuscript, Critical revision of manuscript.
Leonie Supper: Acquisition of data, Critical revision of manuscript.
Lisa Reinhard: Acquisition of data, Analysis and interpretation of data, Critical revision of manuscript.
Agata Dukaczewska: Study conception and design, Critical revision of manuscript.
Henning Jann: Study conception and design, Critical revision of manuscript.
Uli Fehrenbach: Study conception and design, Critical revision of manuscript.
Charlotte Friederike Müller-Debus: Study conception and design, Critical revision of manuscript.
Tatiana Skachko: Study conception and design, Critical revision of manuscript.
Johann Pratschke: Study conception and design, Critical revision of manuscript.
Peter E. Goretzki: Study conception and design, Critical revision of manuscript.
Martina T. Mogl: Study conception and design, Analysis and interpretation of data, Drafting of manuscript, Critical revision of manuscript.
Eva M. Dobrindt: Study conception and design, Analysis and interpretation of data, Drafting of manuscript, Critical revision of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.