
Abstract
Background:
Small intestinal neuroendocrine tumors are the most common of small bowel malignancies with a clinical incidence of about 1 per 100,000 persons per year. There has been a threefold increase in the incidence of small intestinal neuroendocrine tumor during later decades, but there are no studies that clarify whether this is due to a true higher incidence or if the rise is a mere product of, for instance, improved diagnostic modalities. The aim of this study was to investigate the incidence of clinical as well as subclinical small intestinal neuroendocrine tumors found at autopsy as well as describing the frequency of concomitant malignancies in patients with small intestinal neuroendocrine tumor.
Materials and methods:
An autopsy registry from the Malmö county population from 1970 to 1982 with an 87% autopsy rate was used. The clinical autopsy reports for patients coded for the existence of “carcinoid tumor” were scrutinized for the presence of small intestinal neuroendocrine tumor, metastatic disease, and concomitant malignancies. Details of patients with clinically diagnosed small intestinal neuroendocrine tumor during this time period were gathered from the Swedish Cancer Registry.
Results:
The mean annual incidence of small intestinal neuroendocrine tumor during this period was 5.33 per 100,000 individuals, and the mean annual prevalence was 581 per 100,000. The cause of death in the majority of cases was not due to small intestinal neuroendocrine tumor. In total, 48% of the people with small intestinal neuroendocrine tumor had at least one other malignancy, most commonly colorectal cancer.
Conclusion:
Most small intestinal neuroendocrine tumors are subclinical, and persons living with them will often die due to other causes. There was a high rate of multiple primary tumors (40%), suggesting that multiple tumors seem to arise before the advent of metastatic disease. Moreover, a comparably high rate of associated colorectal carcinoma was found.
Keywords
Introduction
Small intestinal neuroendocrine tumors (SI-NETs) are the most common of small bowel malignancies, with a rising incidence over the last decades (1, 2). The clinical incidence in Sweden between 1991 and 2005 was 1.33 per 100,000 (3), and other large registries report an incidence of 0.6–1.2 per 100,000 in previous studies (1, 2, 4–8). SI-NETs usually have a slow progression, and many patients present with generalized disease (9–11), often times years after the onset of symptoms (12). In an earlier autopsy study by Berge and Linell (13), antecedent to this article and from the same population but covering the years 1958–1969, the reported post mortem incidence (clinical incidence added to autopsy findings of SI-NET) was 5.4 per 100,000, with 90% of tumors not diagnosed before autopsy. The large proportion of tumors that never gain clinical significance may be due to the indolent nature of the tumor as well as unspecific symptoms. The present study had several aims; to validate the high incidence in the Berge et al. study, and to investigate whether if the rising clinical incidence in SI-NET is due to a true increase in incidence or improved methods of detection. An increase in the true incidence of SI-NET of the reported threefold magnitude would require a fundamental change in SI-NET oncogenesis or a shift in the abundance of pro-oncogenic factors. Further studies would be warranted to elucidate this transformation in SI-NET occurrence. Also, since there is a high rate of synchronous malignancies in the presence of clinical SI-NET (14–16), the frequency of other malignancies in patients with SI-NET at autopsy was scrutinized.
Materials and methods
An autopsy registry of the Malmö county population from 1970 to 1982 was used. After this period, the rate of necropsies declined drastically, due to changes in legislation and public opinion. All necropsies in this series were performed at one hospital, Malmö General Hospital, Malmö, Sweden. Any pathological findings during these autopsies were coded according to the Systematized Nomenclature of Pathology code, defined by the College of American Pathologists in 1965.
The necropsies were performed according to a standardized protocol that has been described by Berge: The gastro-intestinal canal was slit up, rinsed and examined macroscopically. Gross changes were examined microscopically. At all necropsies, tissue for microscopic examination was taken from all lobes of the lungs, the myocardium, kidneys, liver and spleen. In patients with malignant tumours, the microscopic examination was extensive and included not only the primary tumour, but also metastases, if any, and regional, mediastinal, para-aortic and supraclavicular lymph nodes. Carcinoids were diagnosed mainly on a morphological basis. All cases were not examined routinely for argentaffinity and/or argyrophilia. (Berge and Linell, 1976)
This article only concerns patients who were submitted to a clinical autopsy since the autopsy protocols from forensic autopsies could not be made available.
After obtaining approval from the local ethics committee, the registry was queried for autopsy protocols coded for the presence of “carcinoid tumor” (systematized nomenclature of pathology (SNOP) 8241 and 8243, SI-NETs in modern nomenclature was included in “midgut carcinoids” at the time). For all these patients, the cause of death according to the pathologist was recorded. Non-Malmö-residents were excluded. We also gathered the cause of death for all deaths in the Malmö region from the Swedish Cause of Death registry for patients in age group 25–44 years and older (we did not include younger patients since the youngest patients with a recorded SI-NET at autopsy were 36). Incidence was calculated as the sum of all patients diagnosed clinically (from the Swedish Cancer Registry) and by autopsy (from abovementioned records) divided by the number of inhabitants in the Malmö county per year. Autopsied patients with a beforehand clinically diagnosed SI-NET were excluded from the incidence calculation if they had deceased that year. Malmö county together with all patients with a tumor found at autopsy divided by total number of autopsies.
Incidences of concomitant cancers were compared using normal approximation of Poisson distribution. Results were considered statistically significant if p < 0.05. Data collected from autopsy records were recorded in Filemaker (Filemaker Pro, Filemaker Inc., Santa Clara, California). Data analyses were performed in RStudio (RStudio, Version 0.99.893).
Results
During the study period, 35,784 deaths occurred and in 87% of these deaths, an autopsy was performed (23,446 clinical, 7588 forensic) (17). During the study period, the autopsy rate declined somewhat (Fig. 1), but the mean clinical autopsy rate was 66%. In total, 299 autopsy protocols with the presence of “carcinoid tumor” were extracted, but when reviewing the individual autopsy reports, there were 70 records without any note of a NET and 5 records of stillborn infants, also without any note of a NET. These were declared misclassified and excluded. Among all patients with NETs, 161 patients had SI-NET. The remaining patients had neuroendocrine tumors as presented in Table 1. The most common other NET was bronchial NET, in concordance with Berge’s findings (13).

Frequency of clinical autopsies in Malmö country 1970–1982, per gender and total, per year.
General data.
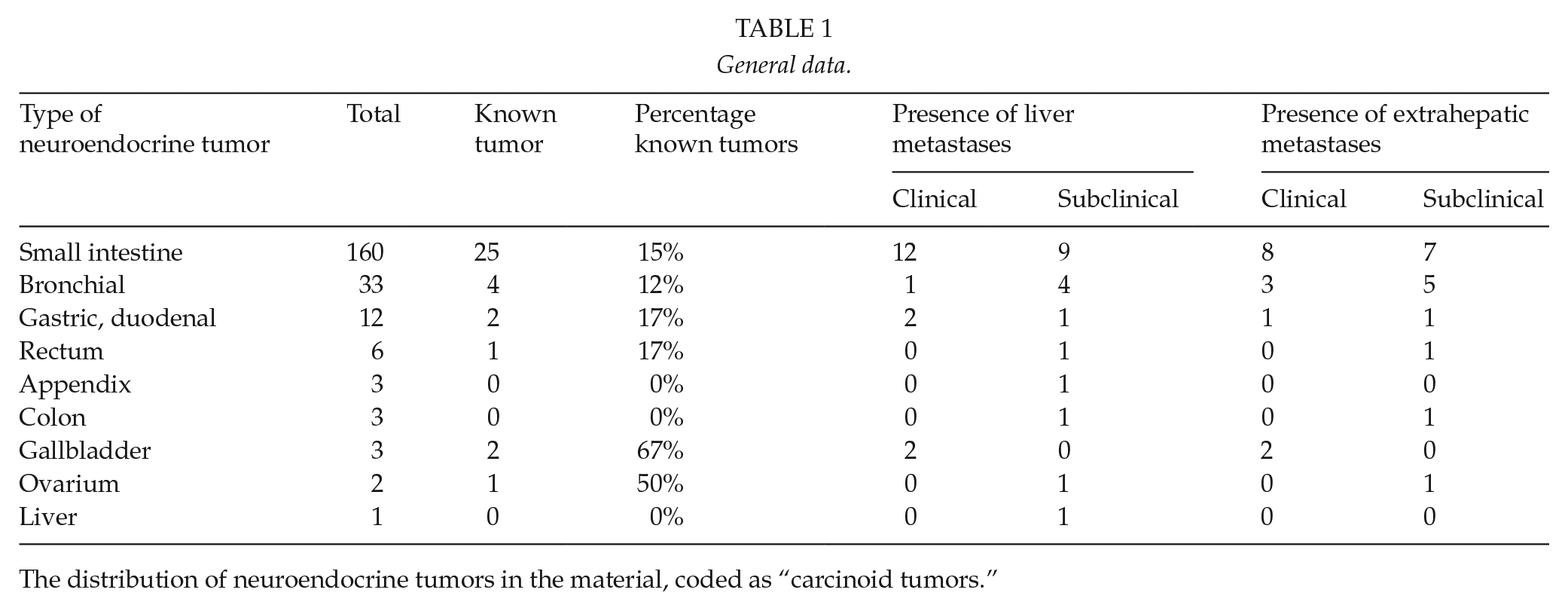
The distribution of neuroendocrine tumors in the material, coded as “carcinoid tumors.”
Reviewing the data further, 25 (15.5%) patients had a previously known SI-NET. Out of the patients with a subclinical tumor, 97 (71%) had a tumor confined to the bowel lumen in contrast with patients with a clinically known SI-NET where 12 of the 25 clinically known patients (48%) had extra luminal growth of the tumor. Metastatic disease was found in 31% of the individuals with SI-NET (50 patients), distributed as shown in Table 2. Most individuals, 60%, had a solitary primary SI-NET, whereas 40% had two or more primary tumors. In the subclinical cohort, 57% (77/136) had more than one primary tumor. Ten patients (5 clinical and 5 subclinical) had insufficiency of the tricuspid valve of the heart but only 4 of them, all of them with clinically known NET and with liver metastases, had signs of cardiac insufficiency. Interestingly, only patients without liver metastases had a primary liver cancer (4 patients).
Distribution of metastatic disease in SI-NET at autopsy.
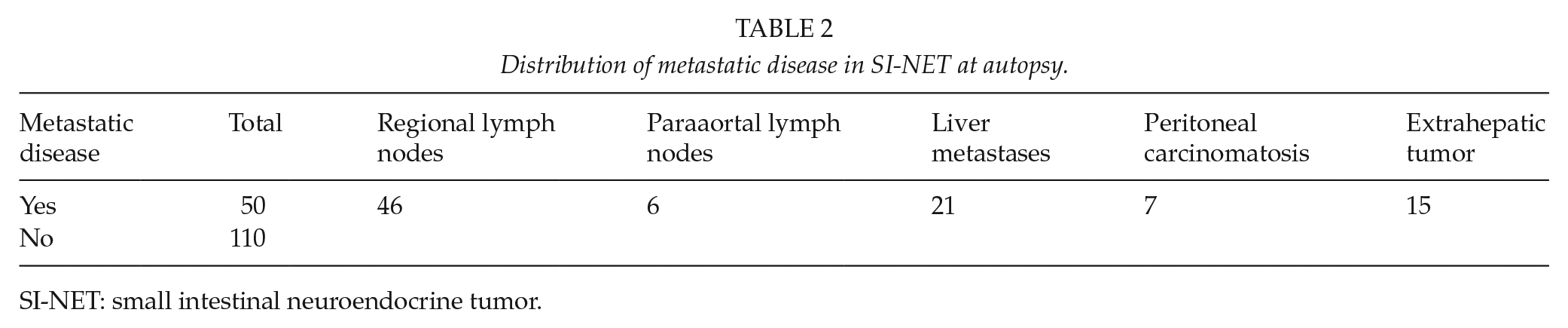
SI-NET: small intestinal neuroendocrine tumor.
Earlier studies have reported a high incidence of synchronous tumors of other origin (14–16), and in this series, synchronous tumors were evident in 48% of persons with SI-NET. A total of 77 patients had a morphologically different tumor (11 patients had more than one) than the SI-NET, most commonly colorectal cancer (21% (16/77)) followed by prostate cancer (18%) and lung cancer (18%). For comparison, we used the reported incidence of colon cancer (4.5%, 698/15,398) from the same population (older than 35 years) for the years 1958–1969 (18). The incidence of colon cancer in the patients with SI-NET (10%, 16/161) was significantly higher than the incidence in the entire cohort (p = 0.03). In the entire cohort, from the same region but from the years 1958–1969, the incidence of at least one malignancy found at autopsy was 44.4% (18). In this article, there were unfortunately no data on the number of patients with multiple tumors. Given that 8214 tumors were found in 7246 patients, the maximum number of people with multiple tumors would be 968. Thus, the maximum incidence of multiple malignancies was 13.3%. Thereby, harboring a SI-NET would seem to increase the likelihood of having another malignancy with 360% (p =< 0.0001), compared to patients with other malignancies.
One patient had a synchronous neuroendocrine tumor; a rectal NET. In addition, another 10 patients had multiple synchronous malignancies that were not of neuroendocrine origin. The causes of death in patients with SI-NET were similar to the general population (Table 3). Specifically looking at the patients with undiagnosed tumor, we found four patients who died due to an undiagnosed, metastatic NET.
Causes of death in the Malmö population and in patients with SI-NET.
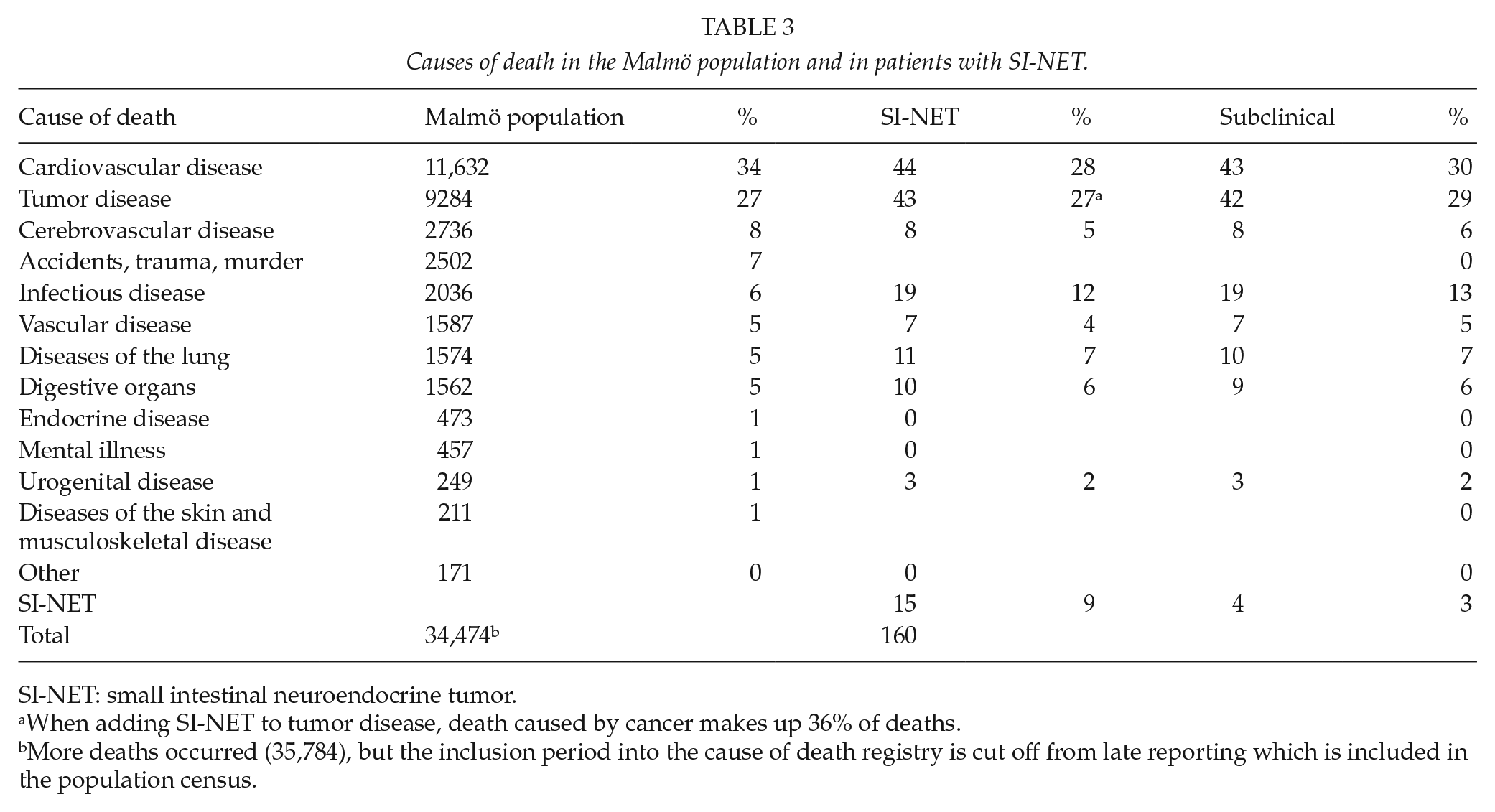
SI-NET: small intestinal neuroendocrine tumor.
When adding SI-NET to tumor disease, death caused by cancer makes up 36% of deaths.
More deaths occurred (35,784), but the inclusion period into the cause of death registry is cut off from late reporting which is included in the population census.
In addition, drawing data from the Swedish Cancer Registry during the period 1970–1982, we found an additional 13 patients who had been diagnosed with SI-NET and died during the study period but had not had a clinical autopsy performed at their death. Including these patients in our data, the mean incidence of SI-NET, either as a clinical finding or during autopsy, was 5.33 per 100,000 and year (Table 4, two autopsied patients were excluded from the incidence calculation due to clinical diagnosis in 1968 and 1969). Since there was a large gender discrepancy in the clinical SI-NETs as well as SI-NETs found at autopsy, we also calculated incidence per gender. This resulted in different mean incidences, during the time period 1970–1982, for men (13.6 per 100,000) and women (7.0 per 100,000) (p = <0.001). The mean prevalence of SI-NET in this cohort was 581 per 100,000 (approx. 6/1000) inhabitants. Furthermore, age-related incidence and prevalence were studied. The prevalence of SI-NET peaked in the age group 60–69 (7.3 per 1000). Incidence on the other hand increased with increasing age (Fig. 2).
Incidence and prevalence of SI-NET in Malmö 1970–1982.
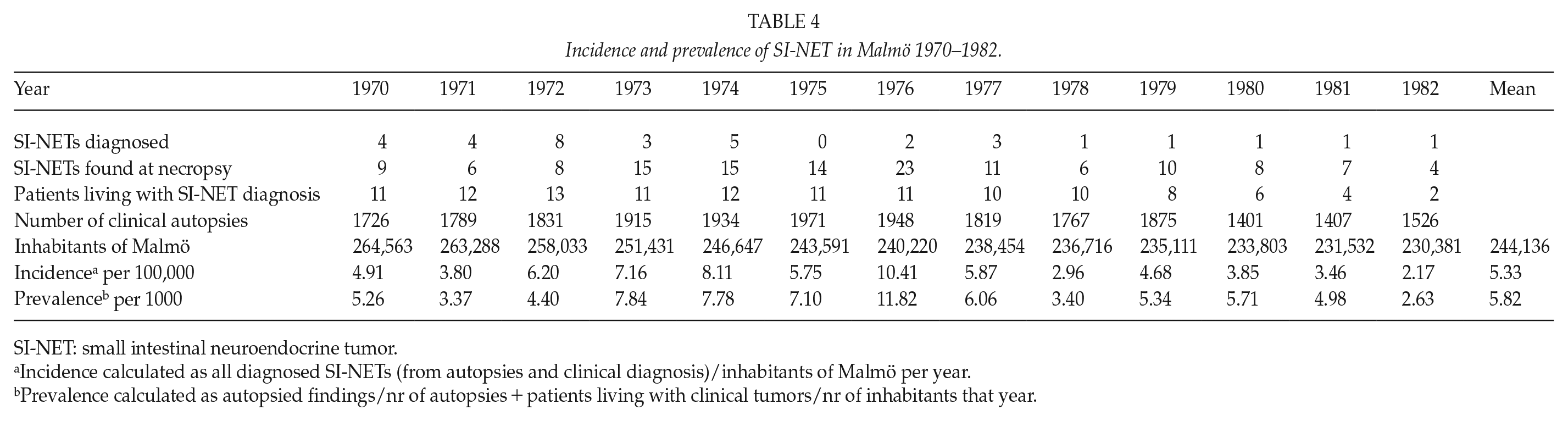
SI-NET: small intestinal neuroendocrine tumor.
Incidence calculated as all diagnosed SI-NETs (from autopsies and clinical diagnosis)/inhabitants of Malmö per year.
Prevalence calculated as autopsied findings/nr of autopsies + patients living with clinical tumors/nr of inhabitants that year.
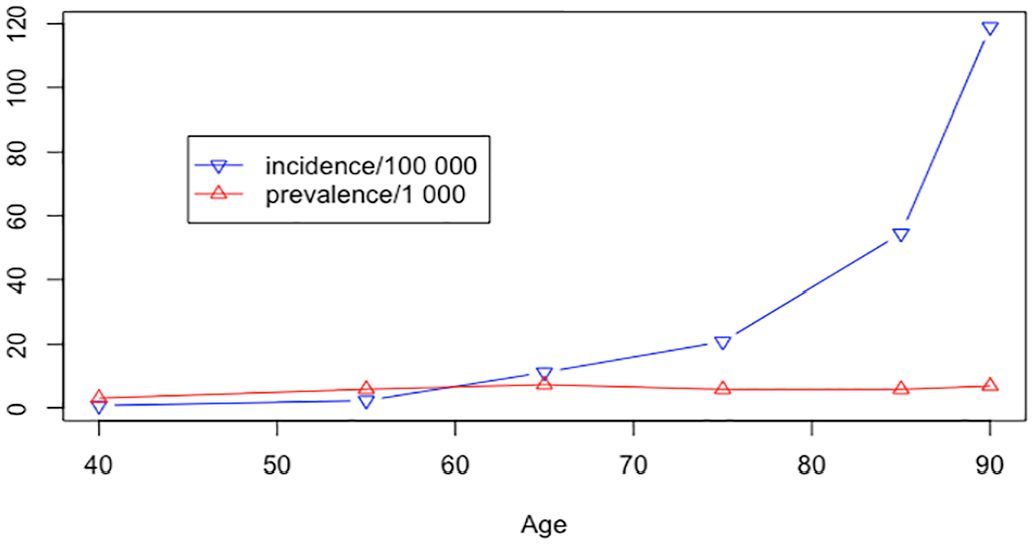
Incidence and prevalence of SI-NET by age.
Discussion
Small intestinal NETs are most often subclinical, presumably because of lack of symptoms or because early symptoms are generally too unspecific to alert a physician. The overall annual incidence of SI-NET was 5.33 per 100,000 when clinical findings of SI-NET as well as tumors found at necropsies during the study period were included. These findings underscore that SI-NETs generally have a slow progression since only 15.5% of patients had a tumor that was diagnosed ante mortem. Indeed, the cohort was collected between 1970 and 1982, and a higher rate of clinically detected tumors is anticipated if the study would have been performed on a more recent cohort, which is noted on the described increase in incidence by other authors (1, 2). Our data also show that patients with SI-NET often occur in conjunction with malignancies of other origins, since close to half (48%) of the patients in this study had at least one other malignancy. In Berge’s preceding study, the incidence of other coexisting malignancies was 40.7% (all “carcinoids” not discriminated for SI-NET) (13). In both these studies, there is a marked difference in the incidence of other malignancies. Comparing the same cohort, that is, Berge’s two studies, the incidence of having two malignancies is increased by 300%. This finding suggests that the risk of harboring other tumors is significantly increased in SI-NET. This could be explained by a genetic difference that predisposes for other malignant tumors in SI-NET, or possibly, by pro-oncogenic properties of small, non-metastasized SI-NETs. One could argue that the population with SI-NET was older (i.e. more likely to develop malignancies), but the mean age in the whole autopsied cohort was 73.3 years compared to 73 in the SI-NET cohort. SI-NET patients may thus be at a higher risk of developing concomitant colon cancer, as the colon cancer incidence of this study was twice the incidence of the ones with SI-NET compared to the total cohort. This finding may suggest the introduction of routine colonoscopies in patients with SI-NET. Considering that some centers are discussing screening for colorectal cancer in the general population, screening patients with SI-NET including intubation of the distal ileum (and with an estimated double risk of colon cancer) could possibly detect earlier cancers and improve survival. Indeed, our data also contradict the notion that the higher rate of colon cancer found in some studies could be due to higher rate of investigations of the bowel, since the majority of persons with SI-NET were subclinical and therefore not screened for colon cancer. Similarly, previous results from the Swedish Cancer Registry, including the same time period as the present study also found an increased incidence of a secondary malignancy (14).
Certainly, the incidence of cancer, found at autopsy, increases with age. Suen et al. reported that a total cancer incidence at autopsy of 3752 consecutive patients from New York between 1960 and 1971 was 32.5% (40.3% for men, 23.9% for women) in patients older than 65 years. The most common malignancies were lung (18.1%), prostate (16%), and colon cancer (11.3%) (19). This cohort was not scrutinized for endocrine tumors, but the incidence of small bowel cancer was 0.9%. Given that SI-NET constitutes 44% of all clinical small bowel cancers in the United States (20), this would give an incidence of SI-NET of approximately 0.4%.
Probably, improved diagnostic procedures as well as an aging population mostly explain the rising clinical incidence of SI-NET in the western world during recent years. The persons with SI-NET tumors had a mean age of 73 years (75.5 if excluding clinical tumors), validating that SI-NET is a disease that more commonly presents in the elderly. There is a significant gender difference, with the incidence of SI-NET in men being almost twice the incidence in women, which corresponds well to the increasing incidence of clinical SI-NETs , especially in men. Indeed, clinical SI-NETs were more common in women in data from before 1975 (3, 6), whereas men are predominant in more recent data (21). We would expect, if our future holds a gender-neutral increase in life expectancy, that the incidence for SI-NET will continue to increase, especially among men.
In our data, the estimated mean prevalence of SI-NET in this population is 0.5% (581 per 100,000 persons). This finding seems reasonable compared to estimates of more common cancers; for instance, the estimated prevalence for undiagnosed invasive breast cancer has been reported as 1.5% (22), 49% for undiagnosed prostate cancer in men older than 79 years (23), 11% for undiagnosed differentiated thyroid cancer (24), and 1.4% for undiagnosed renal cell carcinoma (25). In general, SI-NETs do not most likely contribute to the death of these patients, as causes of death were similar in the population with or without SI-NET.
Carcinoid heart disease has been reported as the primary clinical presentation in 20%–70% of patients with carcinoid syndrome (26, 27). It was certainly common during the time of the current study. Most patients in this series were not symptomatic, but 10 patients had plaques on the tricuspid valve and 4 patients had metastatic disease and heart failure, possibly due to carcinoid heart disease. It was more common with tricuspid valve insufficiency in patients with liver metastases (38% (8/21)) compared to patients without liver metastases (1.4% (2/139)), strengthening the theory that carcinoid heart disease usually begins with the occurrence of plaques of the tricuspid valve, usually explained by right-sided serotonin induced valvulopathy (26, 27).
Up to 40% of persons with undiagnosed SI-NET have multiple mucosal tumors. Interestingly, the rate of multiple tumors is similar in most clinical cohorts (28). This finding suggests that multiple SI-NET tumors might arise before the occurrence of mesenteric metastases. This might be due to submucosal spread of a single progenitor tumor, or due to changes in the local milieu of the small bowel where SI-NETs arise. To our knowledge, this is the first study that has reported such a finding.
There are some limitations in this study. The available data concern autopsy protocols drawn from 66% of the citizens that died during this period. Including patients with a clinically diagnosed tumor that died during the study period, however, increases the likelihood that our findings are close to the correct values. It seems unlikely that individuals with subclinical SI-NET die from causes that do not warrant a forensic autopsy to a larger extent than other citizens, which otherwise would cluster SI-NETs in the clinical autopsy group. One might question that what impact these historic data have on modern day medicine. The declining rate of necropsies in modern society makes more recent studies difficult to interpret and susceptible to considerable bias, especially when considering rare diseases. To be able to report a true incidence of rare diseases, the rate of autopsies needs to be as high as possible; not possible in contemporary circumstances, making the Malmö autopsy registry truly unique.
In conclusion, the prevalence of subclinical SI-NET is much higher than anticipated. One would therefore expect to find a small bowel NET in 0.7% of all laparotomies in 60- to 69-year-olds. In an earlier article, we could show that patients operated for acute abdominal symptoms with the incidental finding of SI-NET are doing better than patients having elective surgery for known disease, explained by the acute patients being in a lower TNM stage (29). This fact, together with the findings in this study, especially the four subclinical patients who indeed died from their SI-NET, strengthens the notion that the small bowel should, when appropriate, be examined thoroughly for nodules in the small bowel at abdominal surgery for other causes. It is, however, not the opinion of the authors that screening programs for SI-NET should be implemented as subclinical tumors are difficult to find even with modern imaging techniques. In a recent study, 68Ga-DOTATOC/TATE-PET/CT was found to be more sensitive than contrast enhanced computer tomography but still failed to detect 52.5% of primary tumors (30). Furthermore, since subclinical tumors most often stay subclinical, the recommendation to an aging patient upon finding a small tumor nodule in the small bowel would be very difficult. As in several other cancers such as low-grade prostate cancer or papillary microcarcinoma of the thyroid, the treatment for some patients may be more harmful than the disease.
Footnotes
Acknowledgements
We are thankful to the Ihre Foundation, the Uppsala Health Region, and Statisticon for valuable support. We would like to express appreciation to Lena Luts, department head at the time of data acquisition, at Clinical Pathology, Lund University Hospital for assistance with data retrieval.
Author’s Contributions
PH and ON conceived the study and planned the study design.
PH, ON, JE, and MÖ acquired and collected the data.
JE and HG performed the data analysis, all authors participated in data interpretation.
JE wrote the first draft. All authors reviewed the article critically and approved the final article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been made possible mainly due to funding from the Bengt Ihre Foundation, the Bergholm/Eriksson Foundations at Uppsala University, and the Göran Gustafsson Foundation.