
Abstract
Background and objective:
To assess the effect of surgeon sex on short- and long-term outcomes after colon cancer resections.
Methods:
Clinical data of patients who underwent colon cancer resections between 2010 and 2020 at Helsingborg Hospital, Sweden, were retrospectively obtained from medical records. The sex of the surgeon of each procedure was recorded. Morbidity, mortality, and long-term survival were compared in patients operated by male and female surgeons.
Results:
Colon cancer resections were performed by 23 male and 9 female surgeons in 1113 patients (79% elective, 21% emergent). After elective surgery, there was no difference in postoperative complications, 30-day mortality, or long-term survival between patients operated by male and female surgeons. Following emergent resections, the complication rate was significantly lower in patients operated by female surgeons (41.3% vs 58.1%, p = 0.019). Similarly, the rates of R1-resections (0% vs 5.2%, p = 0.039), reoperations (3.8% vs 14.2%, p = 0.014), and intensive care unit (ICU) care (6.3% vs 17.4%, p = 0.018) were significantly lower for patients operated by female surgeons, but there was no difference in 30-day mortality (6.3% vs 5.2%, p = 0.767). Cox regression analysis showed that long-term and cancer-free survival in patients emergently operated by male surgeons was significantly shorter than that of patients operated by female surgeons (hazard ratio = 1.9 (95% confidence interval (CI) = 1.3–2.8), p = 0.001 and hazard ratio = 1.7 (95% CI = 1.1–2.7), p = 0.016).
Conclusions:
The short- and long-term outcome after elective colon cancer resections were similar in patients operated by male and female surgeons. The outcome following emergent resections performed by female surgeons compared favorably with that of male surgeons, with fewer complications and reoperations and better long-term survival.
Keywords
Context and Relevance
It is generally accepted that there are variations in surgical outcomes, and these are often attributed to patient-related factors, although there is increasing evidence to suggest that also surgeon-related factors affect postoperative outcomes.
As information regarding the effect of surgeon sex on postoperative outcome is limited, we retrospectively studied the short- and long-term results after colon cancer resections performed by male and female surgeons at a secondary care hospital. Elective resections were performed with similar quality by male and female surgeons, with comparable oncological quality, similar rates of complications and mortality, and similar long-term survival. Following emergent colon cancer resections, patients operated by female surgeons had fewer and less severe postoperative complications and better long-term survival.
Introduction
It is generally accepted that there are variations in surgical outcomes, and these are often attributed to patient-related factors such as age, comorbidities, or the severity of underlying disease. However, there is increasing evidence to suggest that also surgeon-related factors are associated with quality and postoperative outcome. 1 Although surgery is a craft specialty, technical proficiency is not the only surgeon-related determinant for a good postoperative outcome, and adequate knowledge, communication skills, and clinical judgment may be equally important for patient outcome.2,3 Thus, clinical experience and individual personality including surgeon attitudes and risk propensity, and the ability to facilitate teamwork may also be factors that influence patient outcome. 4
In the field of internal medicine, there are several studies reporting that male and female physicians practice medicine differently.5–11 These studies conclude that female physicians are more prone to use and follow guidelines, have more effective communication, and provide a more patient-centered care resulting in better quality of care and lower rates of mortality and readmissions compared with their male counterparts.6,11
Our interest in the potential effects of surgeon sex on postoperative outcome was stimulated by the report of Wallis et al. 3 who compared outcomes of male and female surgeons in over 100,000 patients after a wide range of different operations across many surgical specialties. They concluded that there was a small statistically significant difference in 30-day mortality in favor for patients operated by female surgeons, but no differences in the rates of complications or readmissions. In a similar study, Sharoky and coworkers reported short-term outcome after 44 different general surgery operations with a wide range of complexity. They concluded that patients operated by male and female surgeons had equivalent rates of inpatient mortality, postoperative complications, and prolonged length of hospital stay. 12 Similar short-term outcome in patients operated by male and female surgeons was also reported in a recent cohort study including patients who underwent elective distal gastrectomy, total gastrectomy, or low anterior resections performed by surgeons who were members of the Japanese Society of Gastroenterological Surgery. 13 Information regarding the effect of surgeon sex on postoperative outcome is limited, and available studies are inconclusive and based on a wide range of different surgical procedures with varying complexity.3,12
We therefore aimed to assess whether surgeon sex had an effect on the surgical outcomes in a more homogeneous cohort of patients undergoing a single, but more complex surgical procedure. The aim of this retrospective observational study was to evaluate the effect of surgeon sex on postoperative morbidity, mortality, and long-term survival following colon cancer resection in a secondary care hospital cohort.
Methods
Study population
All patients who underwent elective and emergent resections for colon cancer between 2010 and 2020 at Helsingborg Hospital, Sweden, were identified from the Swedish Colorectal Cancer Registry (SCRCR). The SCRCR is a validated national registry with a coverage of 98.5% of all colon cancers in Sweden. 14 Helsingborg Hospital is a secondary care hospital with a catchment area of 350,000 residents. Patients younger than 18 years of age, patients who underwent colon resections for benign disease, and patients with rectal or appendix cancer were not included. Unplanned colon resections performed within 48 h after acute admission were defined as emergency operations, and all other resections were defined as elective procedures. No patients with a need for elective or emergency colon resections were referred to other hospitals, and the postoperative care was provided at the colorectal surgery unit. The use of stents as a bridge to elective surgery in patients with obstructing colon cancers was not practiced during the study period.
The sex of the most senior surgeon actively participating in each of the colon resections was recorded. The yearly median number of all colon resections (elective and emergency procedures) for cancer in which the surgeons had actively participated was calculated. Colon resections for benign disease and rectal cancer were not included in this annual number. The overall surgical experience, defined by the date from surgical board certification to the date of surgery, was calculated for the surgeons of all resections. Night surgery was defined as a surgical incision time between 17:00 and 07:00 h.
Demographic, clinical data, and tumor characteristics of the patients were obtained from the SCRCR. To obtain additional data and to validate the information from the registry, three researchers conducted a retrospective review of the medical records. A guideline for retrospective medical record reviews was followed to reduce the risk of information bias during data collection. 15 The Charlson Comorbidity Index (CCI) was used to classify the comorbidity burden of the patients, 16 and the stage of colon cancer was categorized from I to IV. 17 Patients in whom all visible tumors were not removed during the procedures were defined as having macroscopically generalized cancer. The Clavien–Dindo classification (grades II to IV) was used to characterize the nature and severity of complications. 18 Preoperative treatment decisions were made at a multidisciplinary tumor board (MDT) in all patients undergoing elective resections. Decisions regarding adjuvant treatment were made postoperatively at MDT for all patients.
The primary outcomes of interest were the occurrence and the severity of complications, the need for intensive care unit (ICU) care, reoperations, and the 30- and 90-day mortality rates in patients operated by male and female surgeons. The long-term overall- and cancer-free survival was assessed and compared in the same groups of patients as secondary aims.
Statistical analysis
As continuous data were not normally distributed results were reported as medians and 25th–75th percentiles, and comparisons were made using non-parametric statistics. The Mann–Whitney U-test was used to compare continuous data between two groups. Proportions were analyzed using the chi-square test. Binary logistic regression analyses were used to evaluate associations between multiple factors on binary outcomes, and variables considered clinically important were entered simultaneously for adjustments in the regression models. The factors adjusted for in patients having elective resections included patient sex, the American Society of Anesthesiologists (ASA) classification, pathological tumor stage, annual resection volume, overall surgical experience, and the surgical approach. For emergent resections, adjustments were made for the same factors with the addition of nighttime surgery and indication for emergent surgery. From the day of surgery, the cumulative overall survival was plotted using the Kaplan–Meier method, counting deaths as events and the remainder as censored as of the last day of follow-up. Similarly, cancer-free survival was plotted counting deaths or cancer recurrence as events and the rest as censored. Comparisons of cumulative survival between groups were made using the log rank test. Cox regression analysis was performed to assess the effect of multiple variables and to adjust for potentially confounding factors on overall- and cancer-free survival. For elective resections, adjustments in the Cox models were made for patient sex, patient age, ASA classification, tumor stage, annual resection volume, overall surgical experience, and surgical approach. Adjustments for emergent resection were made for the same factors with addition of nighttime surgery and indication for emergent resections. A p < 0.05 was considered statistically significant.
All statistical analyses were performed using the IBM SPSS® Statistics ver. 25 (IBM Corp., Armonk, NY, USA). The study was approved by the Swedish Ethical Review Authority (2019-04329).
Results
During the study period, 1113 patients underwent resection for colon cancer at Helsingborg Hospital. Eight-hundred and seventy-eight (79%) of these patients underwent elective resections and 235 (21%) emergency resections. All colon resections were performed by board certified general surgeons. Elective colon resections were performed by 10 male and 9 female surgeons with similar median annual resection volumes (11.8 (7.2–23.9) vs 18.7 (7.8–28.0) resections per year, p = 0.762). There was no significant difference in the resection volumes between 23 male and 8 female surgeons performing the emergency procedures (11.0 (6.5–24.9) vs 6.0 (1.6–18.2), p = 0.122). Eight of the female surgeons who performed elective resections also performed emergent resections and 10 male surgeons performed both elective and emergent resection whereas 13 male surgeons performed emergent resections only. There was no significant difference in the overall surgical experience of male and female surgeons performing elective and/or emergent resections (12.3 (7.6–19.7) vs 16.3 (9.2–21.3), p = 0.712 and 16.3 (9.6–21.7) vs 19.3 (6.2–21.3), p = 0.122, respectively).
In patients who underwent elective resections, female surgeons operated a statistically significantly larger proportion of female patients, but no such difference was observed in patients who underwent emergency resection (Table 1). The distribution of emergency resection due to mechanical obstruction, perforation, or anemia/bleeding was similar in patients operated by male and female surgeons (80.0% vs 87.5%, 12.9% vs 12.0%, and 7.1% vs 2.5%, respectively, p = 0.253). There was no difference in the proportion of emergent colon resections performed during nighttime between male and female surgeons (24.5% vs 22.5%, p = 0.731).
Clinical characteristics of patients who underwent elective and emergent colon cancer resections performed by female and male surgeons.
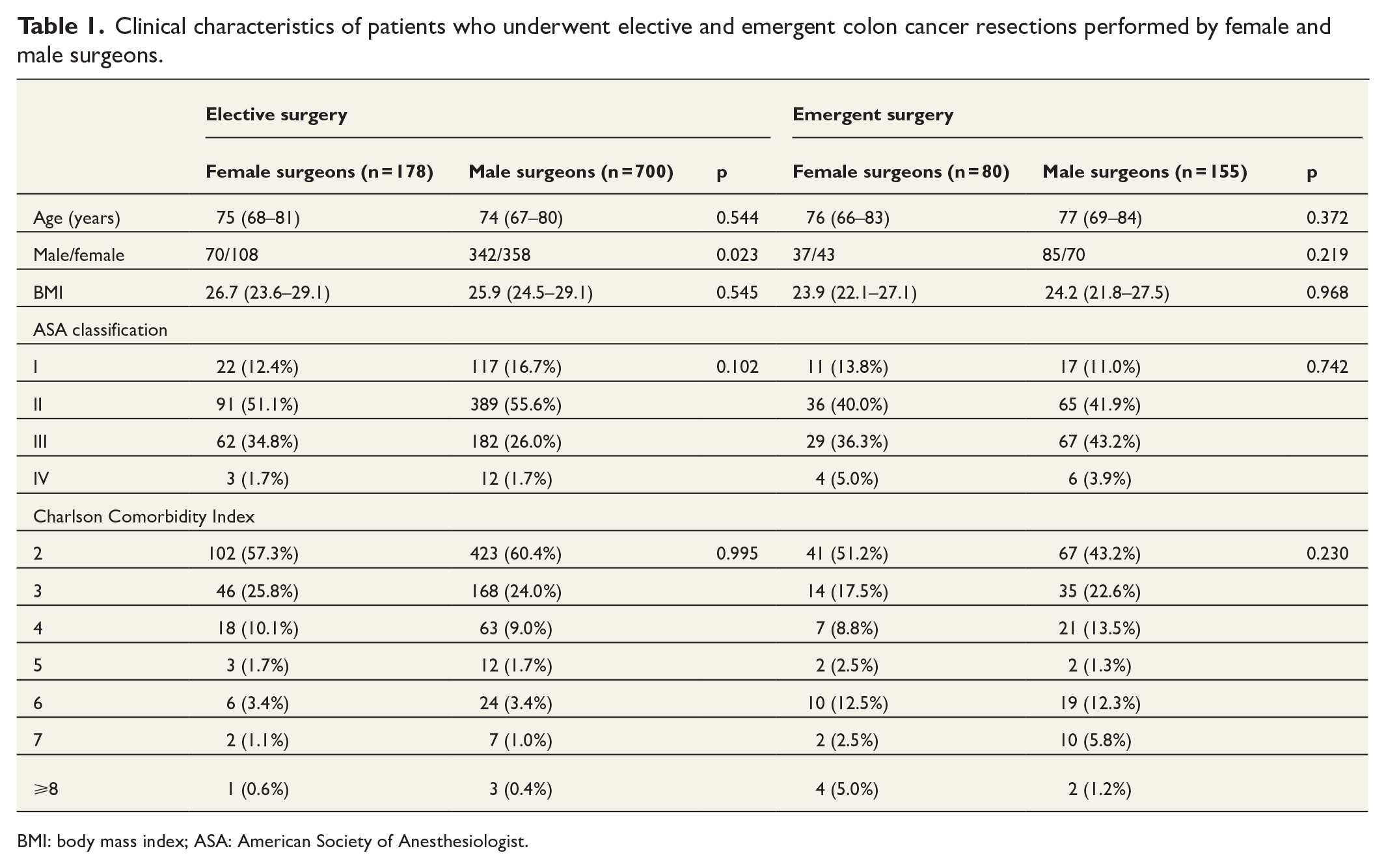
BMI: body mass index; ASA: American Society of Anesthesiologist.
There was no statistically significant difference in the distribution of the types of resections performed by male and female surgeons, but the proportion of elective laparoscopic resections was statistically significantly higher in patients operated by male surgeons (Table 2). Furthermore, the operating time, the lymph node yield, and the tumor stage were similar regardless of surgeon sex. After emergency colon resection, the rate of R0-resections was statistically significantly higher in patients operated by female surgeons, but no such difference was seen in patients who underwent elective resections.
Characteristics of elective and emergent colon cancer resections in patients operated by female and male surgeons.
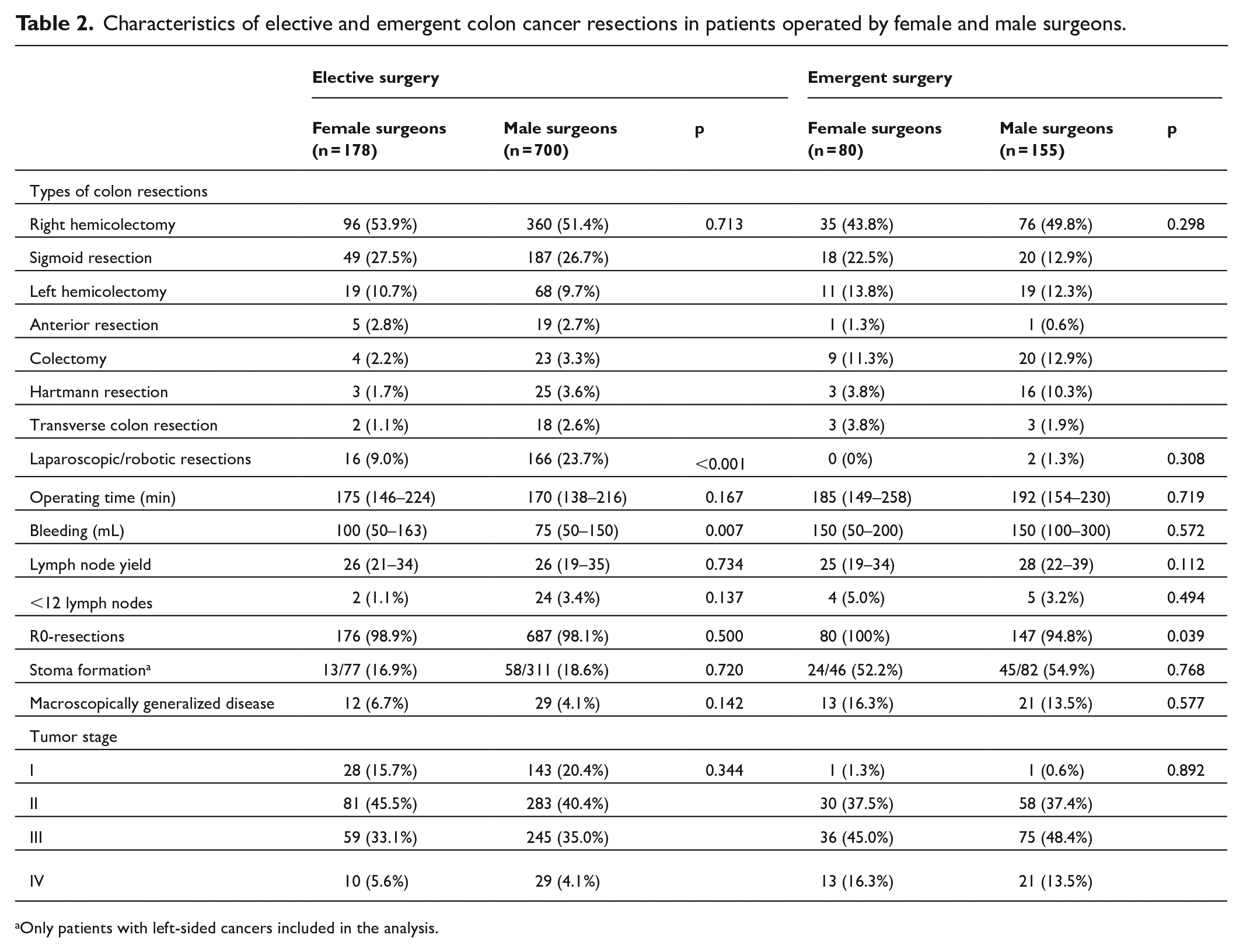
Only patients with left-sided cancers included in the analysis.
The proportion and the severity of complications following elective colon resection were similar in patients operated by female and male surgeons. Following emergency resection, the overall complication rate and the rate of complication Clavien–Dindo III or greater were statistically significantly lower in patients operated by female surgeons (Table 3). After elective colon resections, the need for care at the ICU, the proportion of reoperations, and unplanned readmissions were similar in patients operated by male and female surgeons. The proportion of 30- and 90-day mortality following elective and emergency colon resection were similar regardless of surgeon sex.
Postoperative complications and outcome after elective and emergent colon cancer resections in patients operated by female and male surgeons.
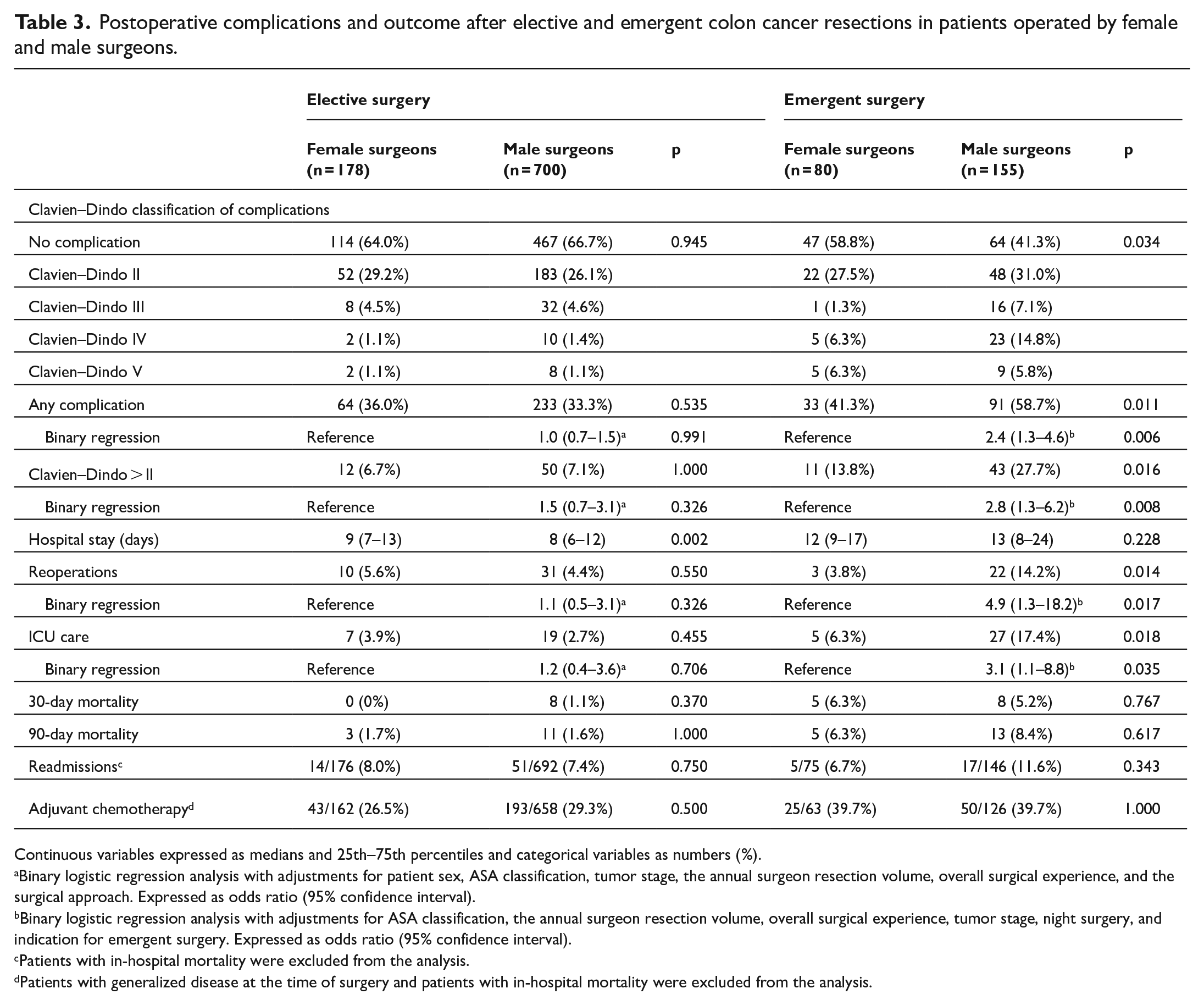
Continuous variables expressed as medians and 25th–75th percentiles and categorical variables as numbers (%).
Binary logistic regression analysis with adjustments for patient sex, ASA classification, tumor stage, the annual surgeon resection volume, overall surgical experience, and the surgical approach. Expressed as odds ratio (95% confidence interval).
Binary logistic regression analysis with adjustments for ASA classification, the annual surgeon resection volume, overall surgical experience, tumor stage, night surgery, and indication for emergent surgery. Expressed as odds ratio (95% confidence interval).
Patients with in-hospital mortality were excluded from the analysis.
Patients with generalized disease at the time of surgery and patients with in-hospital mortality were excluded from the analysis.
Emergent surgery.
Variables Binary regression:
Variables Cox regression:
Elective surgery.
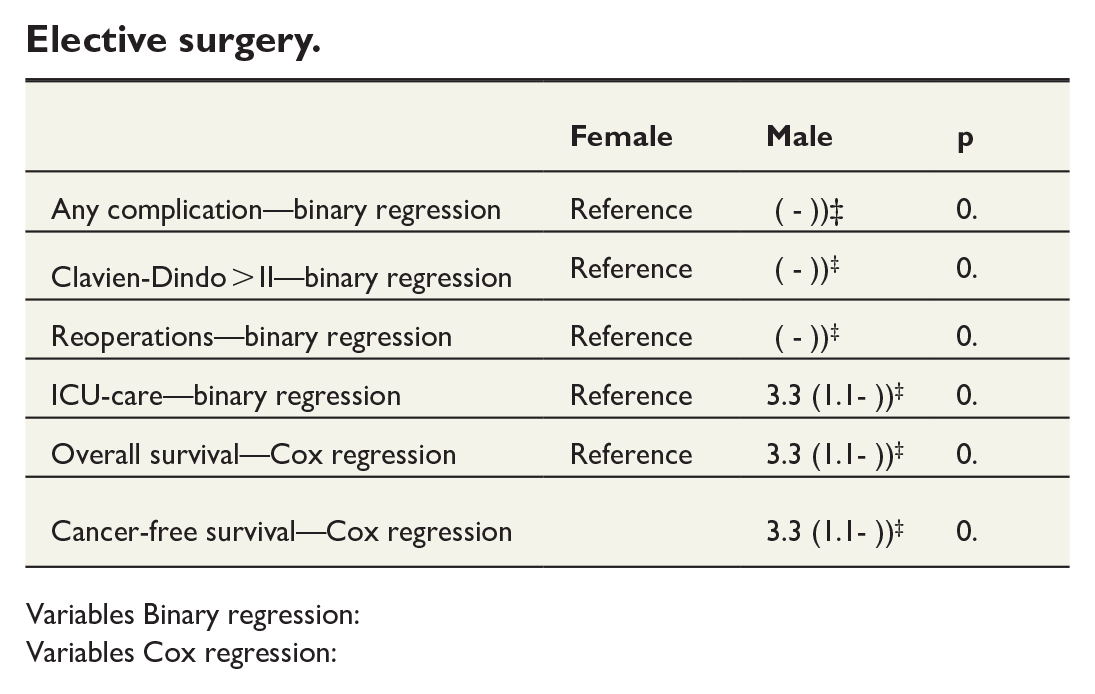
Variables Binary regression:
Variables Cox regression:
The cumulative survival of patients undergoing elective colon cancer resection was similar in patients operated by female and male surgeons (Figure 1). Following emergency resection, the long-term survival was statistically significantly better in patients operated by female surgeons (Figure 2). In a Cox regression analysis with adjustments for factors perceived as clinically relevant for survival, emergent colon resections performed by male surgeons were associated with a significantly shorter survival (hazard ratio (HR) = 1.9 (95% confidence interval (CI) = 1.3–2.8), p = 0.001).
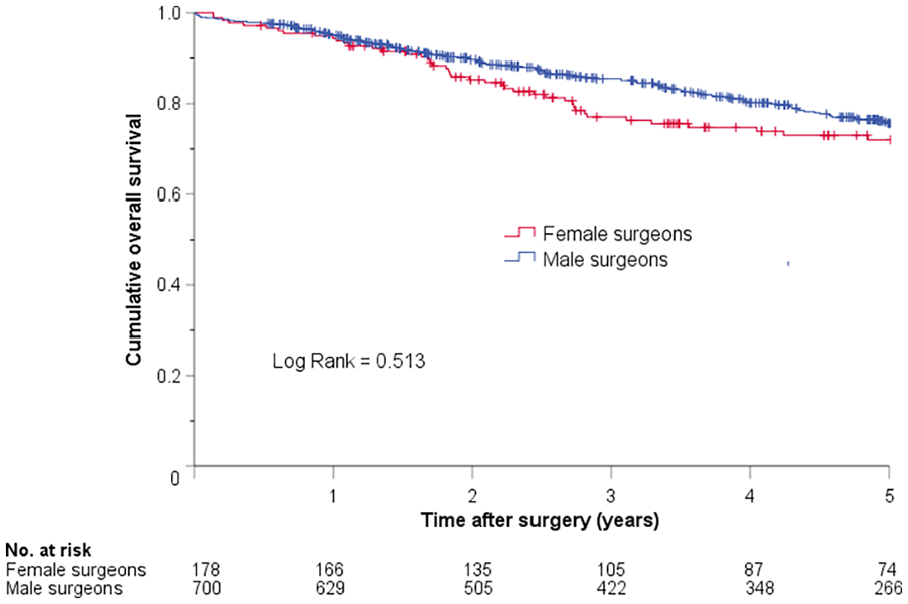
Kaplan–Meier plot showing cumulative overall survival in patients who underwent elective colon cancer resections performed by female and male surgeons.
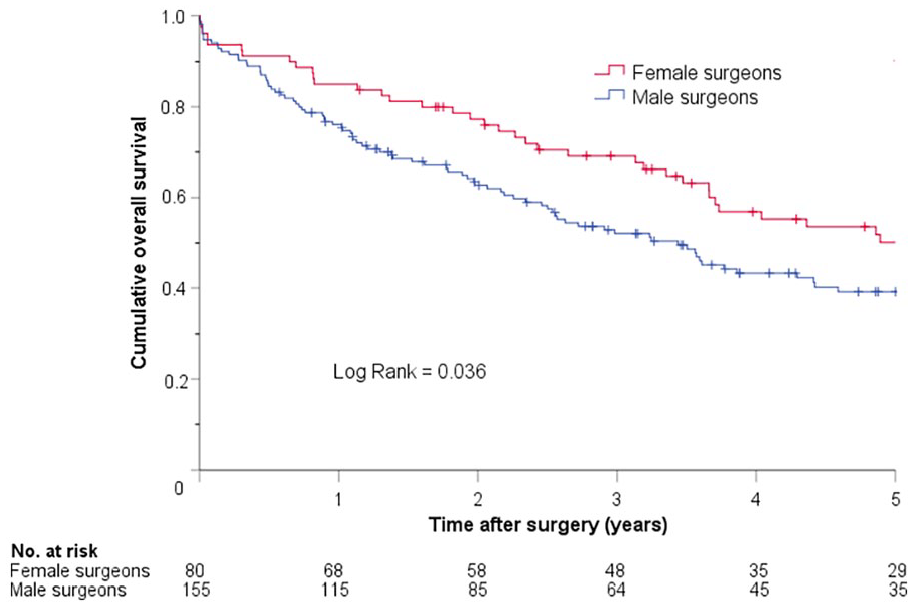
Kaplan–Meier plot showing cumulative overall survival in patients who underwent emergent colon cancer resections performed by female and male surgeons.
Of the patients without macroscopically generalized cancer at the time of surgery, there was no surgeon sex-related difference in the cumulative cancer-free survival in patients who underwent elective colon resection (Figure 3). However, patients undergoing emergency resections performed by female surgeons had statistically significantly longer cancer-free survival compared with those operated by their male counterparts (Figure 4). In an additional Cox regression analysis adjusting for clinical factors considered to potentially affect survival, there was a significant association between emergent resections performed by male surgeon and shorter cancer-free survival (HR = 1.7 (95% CI = 1.1–2.7), p = 0.016).
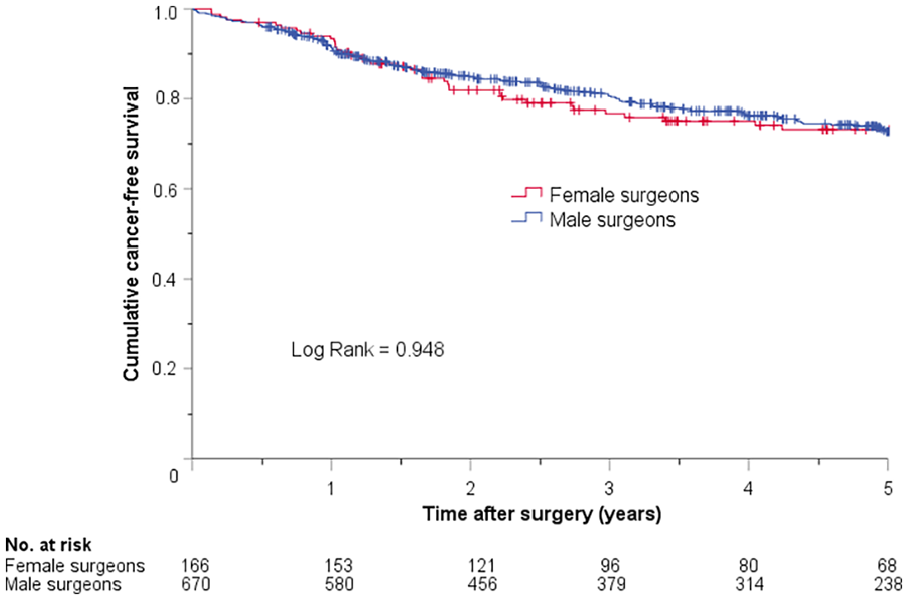
Kaplan–Meier plot showing cumulative cancer-free survival in patients who underwent elective colon cancer resections performed by female and male surgeons.
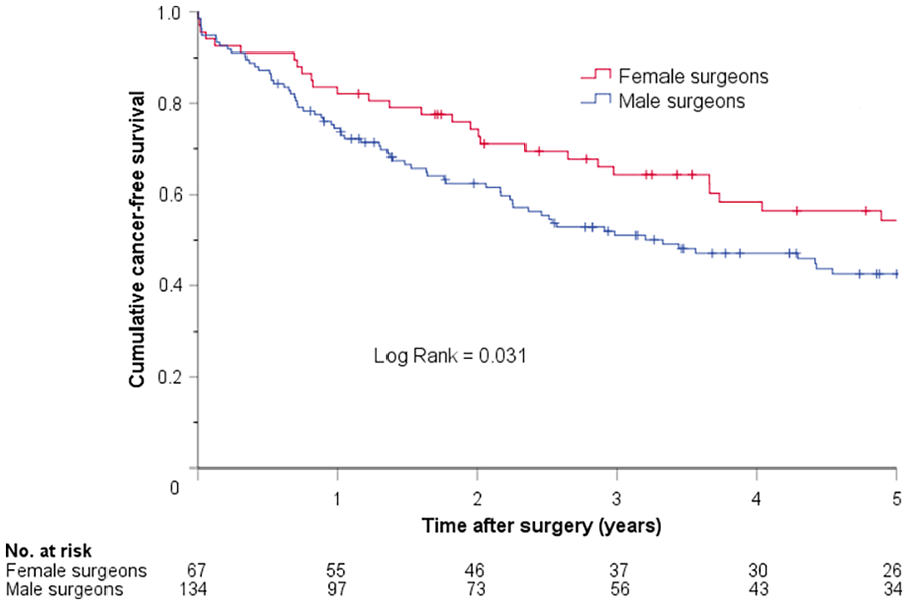
Kaplan–Meier plot showing cumulative cancer-free survival in patients who underwent emergent colon cancer resections performed by female and male surgeons.
Discussion
To our knowledge, this represents the first study comparing short- and long-term outcomes of elective and emergency colon cancer resection in patients operated by male and female surgeons. This retrospective observational cohort study found no surgeon sex-related difference in the short- or long-term outcome in patients who underwent elective resection for colon cancer as both male and female surgeons provided comparable oncological quality, similar rates of complications and mortality, and similar long-term survival. However, following emergency colon cancer resection, we observed that patients operated by female surgeons had fewer and less severe postoperative complications, less reoperations, ICU care, and furthermore, better long-term survival and longer cancer-free survival.
The observation that the complication and mortality rates were equally good in patients who underwent elective colon resections performed by male and female surgeons indicates equivalent technical proficiency of male and female surgeons further supported by the similar median number of resected lymph nodes and the proportion of R0-resections. The similarities in the quality of the oncologic technique most likely explain the observation that the long-term and cancer-free survival was similar in elective patients, regardless of the sex of the surgeon.
The observation that the postoperative outcome was equivalent in patients undergoing elective colon resections performed by male and female surgeons, but differed significantly following emergent surgery is intriguing. Every elective case is preceded by assessments of the patient’s condition and comorbidity, and the treatment decisions are made at MDT. Consequently, elective colon resections are well-planned and performed on physiologically stable patients, often in a stress-free environment where unplanned adverse events are rare. This is in contrast to the surgical challenge to perform emergent resections as the surgeon has to face the additional challenge in managing acute surgical problems in patients who are often in a poor physiologic condition due to perforation or mechanical obstruction. The magnitude of this challenge may often be substantial as a variety of time-critical, high-pressured, and occasionally unfamiliar situations require decisions in clinically difficult circumstances, that is, the surgical challenge during emergency resection is greater compared to corresponding elective situation.
The observed differences in the rates of complications, reoperations, and ICU care after emergent resections performed by male and female surgeons are interesting, but a causal relation is, difficult to prove. The differences in postoperative results could potentially be explained by patient-related factors and that more complicated cases was operated by male surgeons. However, patient-related factors such as age, ASA classification, CCI, tumor stage, and the distribution of perforation and mechanical obstruction were similar in patients operated by male and female surgeons. This observation suggest that the complexity of the procedures was equivalent in patients operated by male and female surgeons, and the adjustments for these factors in our regression models did not change the observation that the sex of the surgeons had a significant influence on postoperative outcomes.
Apart from patient-related factors, the observed differences in postoperative outcome following emergency colon resection may potentially be explained by factors related to the surgeons. Surgical specialization may potentially affect outcomes, although conclusions in available reports are controversial with several studies reporting similar outcomes after emergent colon resections performed by specialized colorectal and non-colorectal surgeons.19–25 As colorectal surgeons generally have higher annual resection volumes than non-colorectal surgeons, we used resection volumes as a proxy for surgical specialization in the regression models, but these adjustments did not change the effect of the surgeon sex on the outcomes. The observation that the outcome following emergent colon resections was better in patients operated by female surgeons, regardless of surgical specialization, was further strengthened in an additional sensitivity analysis including only patients operated by the 10 male and the 8 female surgeons who performed both elective and emergent colon resections. Although we made adjustments for median annual resection volumes in our regression models, the numerical but non-significant difference in resection volumes in emergent resections performed by male and female surgeons raises a concern for a volume effect on the outcome. To address this concern, we made a sensitivity analysis by excluding all patients who had emergent resections performed by surgeons with an annual resections volume lower than 5 per year. Although the number of patients included in the analyses was somewhat lower, the significant difference regarding overall and severe complications, reoperations, and ICU care in favor of patients operated by female surgeons remained. This observation reduces the likelihood of a volume effect and strengthens the suggestion that there was a true difference in outcome following emergent colon resections performed by male and female surgeons.
The observed differences in long-term and the cancer-free survival after emergent resections in favor for patients operated by female surgeons is interesting but difficult to explain as patient characteristics and tumor stages were similar in patients operated by male and female surgeons. Although patients operated by female surgeons had a significantly higher proportion of R0-resections, a casual association is difficult to prove and the reasons for the observed survival advantages remains unknown. As patients operated by female surgeons had a significantly lower proportion of complications, and the occurrence of complications has been shown to correlate with poor long-term survival,26,27 one can speculate as to whether the observed difference in long-term survival could partially be explained by the corresponding difference in the rate of complications.
Studies suggesting that male and female physicians practice medicine different than their male counterparts may possibly explain the observed differences in postoperative outcomes following emergency colon resection. Female physicians have been shown to possess superior communication skills5–11 and successful surgery depends on effective teamwork involving collaboration, coordination, and communication both in the operating room and on the surgical ward.28–29 It has also been shown that female physicians adhere more closely to evidence-based guidelines and provide more patient-centered care, which are characteristics that may be favorable for patients in need of emergency surgery.5–11 Furthermore, it has been shown that female physicians are more risk averse than their male counterparts,5–11 which may affect the selection of patients for surgery and/or the decision whether to perform resections or not. Hypothetically, these traits, which in general appear to characterize female physicians, may make them better suited for management of patients in emergent situations. This assumption is supported by a study that showed that patients with cardiac arrest treated by female physician code leaders had a higher adjusted likelihood of return to spontaneous circulation and survival. 29
The major limitation of this study is the retrospective observational nature of this study as retrospective studies generally are inferior to prospective trials regarding precision and validity. Another limitation is the single-center cohort study design as local variations within the group of surgeons and the surgical teams, or possible differences in indications for surgery may decrease the generalizability of these results. However, the homogeneous cohort of patients undergoing a single, but a more complex surgical procedure with a relatively high rate of complications is a clear strength of our study. Furthermore, the use of administrative data allows the comprehensive identification of readmissions and complications occurring anywhere else in the whole province.
In conclusion, the short- and long-term outcome after elective colon cancer resections was similar in patients operated by male and female surgeons. The outcome following emergent resections performed by female surgeons compared favorably with that of male surgeons, with fewer complications and reoperations, and better long-term survival. These observations need to be confirmed in future studies and the potential underlying mechanisms must be explored as they offer the potential to improve surgical care.
Footnotes
Author contributions
A.Ö. participated in the acquisition of data and data analysis. J.E. participated in research design, the acquisition of data, the data analysis, and in the writing of the manuscript. S.B.-L. participated in the acquisition of data and in the writing of the manuscript. H.B. participated in critical review of the manuscript. T.V. participated in critical review of the manuscript. M.E. participated in critical review of the manuscript. S.Ö. participated in research design, the acquisition of data, the data analysis, and in the writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Thelma Zoéga Foundation.
Research ethics and patient consent
The study was approved by the Swedish Ethical Review Authority (2019-04329), and according to the approval, informed consent was not needed.