
Abstract
Background and Aims:
The principle of complete mesocolic excision for colon cancer has been introduced to improve oncologic outcome. However, this approach is scantily discussed for laparoscopic surgery and there is a lack of randomized trials. This study examined oncologic and clinical outcome after laparoscopic wide mesocolic excision and central vascular ligation for colon cancer.
Material and Methods:
This is a review of prospectively gathered data from a single-institution colorectal cancer database. This study was conducted in the Central Hospital of Central Finland. From January 2003 to December 2011, 222 patients underwent laparoscopic colonic resections with wide mesocolic excision and central vascular ligation in the multimodal setting. The main measures of outcome were cancer recurrence and survival, with early recovery, 30d-mortality and morbidity, reoperation, readmission, and late complications as secondary outcomes.
Results:
The median follow-up was 5.5 (interquartile range (IQR) = 3.7–8.0) years. The 5-year overall survival for all 222 patients was 80.2% and disease-specific survival was 87.5%, and for those 210 R0-patients with stage I–III disease, 83.9% and 91.3%, respectively. The 5-year disease-free survival was 85.8%: stage I was 94.7%, stage II was 90.8%, and stage III was 75.6% (p = 0.004). Increasing lymph node ratio significantly decreased the 5-year disease-free survival. Conversion rate to open surgery was 12.2%. Thirty-day mortality was 1.3% and morbidity, 19.7%. Median postoperative hospital stay was 5 (IQR = 3–7) days.
Conclusion:
Laparoscopic wide mesocolic excision and central vascular ligation for colon cancer resulted in good long-term oncologic outcome. Randomized trials are needed to show that laparoscopic complete mesocolic excision technique would become the standard of care for the carcinoma of the colon.
Introduction
Mesocolic excision together with locoregional lymph node removal has long been applied in colon cancer surgery. However, the extent of mesocolic dissection has not been well standardized in contrast to rectal cancer surgery where total mesorectal excision (TME) along the embryological planes has significantly improved survival (1). Moreover, previous studies have shown that there is variability in the quality of colon surgery, and the long-term oncologic outcome after resection for colon cancer may not have been optimal (2, 3).
Earlier studies have indicated that the oncologic outcome of open colon cancer surgery is directly related to the extent and completeness of mesenteric excision (4–7). Based on these observations, the principle of complete mesocolic excision (CME) for colon cancer has been recently re-emphasized (2, 4, 5, 8). The concept of CME is based on wide mesenteric excision according to the embryological planes to remove mesenteric lymph nodes, central vascular ligation to remove central lymph nodes, and resection of an adequate length of bowel to remove pericolic lymph nodes (8).
Several randomized trials comparing laparoscopic versus open resection for colon cancer have shown that the laparoscopic method can provide an equivalent oncologic outcome, a similar rate of complications, and a faster short-term recovery than the open method (9–12). A recent consensus statement agrees that CME is equally well suited for open as laparoscopic surgery (8). However, CME technique is scantily discussed for laparoscopic surgery and there is a lack of randomized trials (8, 13, 14). The aim of this study was to assess the impact of laparoscopic wide mesocolic excision and central vascular ligation for colon cancer on clinical and oncologic outcome in the multimodal setting.
Materials and Methods
From 2003 to 2011, 222 patients with colon cancer admitted at the Central Hospital of Central Finland underwent a laparoscopic segmental colectomy using wide mesenteric excision and central vascular ligation. Preoperative staging was done by colo-noscopy and thoracoabdominal computed tomography (CT). Previous major abdominal surgery, body mass index >35 kg/m2 and patients with signifi-cant cardiac/pulmonary comorbidity in whom a prolonged laparoscopic surgery would have been potentially harmful were relative contraindications to laparoscopy. Excluded were patients undergoing open surgery, those with carcinoma occurring in the setting of inflammatory bowel disease, or emergency situation such as obstruction and perforation as well as those with radiological evidence of T4-disease necessitating a major en-bloc resection of adjacent organs. The main measures of outcome were cancer recurrence and survival, with early recovery, 30d-mortality and morbidity, reoperation, readmission, and late complications as secondary outcomes. Data were extracted from the local colorectal cancer database. Hospital records were also carefully reviewed. The study was approved by the ethics committee of the hospital.
Surgical Treatment
Perioperative care included the assessment and optimization of medical risk factors, selective use of mechanical bowel preparation, thromboprophylaxis with low molecular weight heparin and elastic stockings, standard anesthesia with epidural analgesia, avoidance of hypothermia, and increased oxygen concentrations. Nasogastric tubes were removed at the operation theater.
Laparoscopic surgery for colon cancer using the 4- or 5- trocar technique and mediolateral dissection along Toldt’s fascia was implemented in 2003. The Erlangen principles, first described by Hohenberger et al. in 2003 (4) and later re-emphasized by Hohenberger et al. (5), West et al. (2, 3), and an international consensus conference (8), were adopted in 2003 in order to standardize surgery. Laparoscopic surgery was initially done by three senior surgeons having experience in laparoscopic colorectal surgery for benign diseases since 1993.
Right colon cancers were managed with medial to lateral mobilization along the right side of the superior mesenteric vein and central ligation of ileocolic artery and right colic artery, when present, and preservation of the trunk of middle colic artery. Carcinomas of the hepatic flexure and right transverse colon were managed by extended right hemicolectomy and central transection of ileocolic, right colic artery, when present, and the trunk of middle colic artery. Gastroepiploic lymph nodes and lymph nodes over the pancreatic head were not routinely dissected. Tumors of the middle transverse colon were treated either with extended right hemicolectomy or with transverse colon resection and central ligation of middle colic artery.
Carcinomas of the left transverse colon or splenic flexure were treated with extended left hemicolectomy and central ligation of the middle colic artery and inferior mesenteric artery. Division of the inferior mesenteric vein and transverse mesocolon were done at the lower edge of the pancreas.
Carcinomas of the descending colon were managed with left hemicolectomy and central ligation of inferior mesenteric artery with distal limit in the upper third of rectum and division of inferior mesenteric vein at the lower border of the pancreas. Sigmoid and rectosigmoid tumors were treated with sigmoid resections with central ligation of inferior mesenteric artery and bowel transection in the upper rectum. Because lymphogenous spread of colon carcinoma to the pericolic nodes is at most for a distance of 10 cm, the aim was to achieve proximal and distal margins of 10 cm from the tumor. A 5-cm rule was accepted, if the anastomosis was made in the upper rectum. Ileocolic anastomoses were made side-to-side using linear staplers and left-side anastomoses were double-stapled using linear and circular staplers. The operation was considered non-curative, if the patient had synchronous distant metastases and/or the resection margins were involved.
Postoperative feeding consisted of free intake of liquids on the first postoperative day, semisolids on the second day, and normal food thereafter. Patients were discharged when they were able to have normal diet, pain free on oral analgesics, capable to handle their stoma, and mobilized. Conversion to open surgery was defined as a necessity to interrupt the laparosopic procedure and to proceed using conventional technique. Postoperative early complications were classified according to the Dindo–Clavien classification (15). Long-term morbidity was defined as surgical morbidity occurring more than 30 days after surgery.
Neoadjuvant and Adjuvant Treatment
Adjuvant postoperative chemotherapy consisting of 5-fluorouracil (FU) and oral folinic acid, oral capecitabine, or the FOLFOX-regimen since 2005 for 6 months were prescribed to medically fit patients having stage III tumors or high-risk stage II disease. Patients having two or more liver metastases during the follow-up usually received perioperative chemotherapy with FOLFOX-regimen and biologicals.
Pathological Examination
Tumors were staged by staff pathologists according to the sixth edition of the Union for International Cancer Control (UICC/TNM) categories (16). Pathological assessment of the quality of the surgical specimen according to the principles first described by West et al. in 2008 (2, 3) was not done in this study. Lymph node (LN) ratio was formed by defining the proportion of metastatic lymph nodes from total number of LNs examined. Intervals were determined using the following cut-off values: LN ratio I <10%, LN ratio II 10%–25%, and LN ratio III > 25%.
Follow-Up
Follow-up examination included carcinoembryonic antigen (CEA) every 6 months, annual clinical examination, ultrasonographic investigation of the liver, and chest radiograph as well as colonoscopy 4–5 years postoperatively. Further characterization of metastases was done using CT, magnetic resonance imaging (MRI), and CT-positron emission tomography (PET) examination since 2005. Surgery for recurrent disease was performed when appropriate. Locoregional recurrence was defined as a recurrent tumor at the anastomotic site or locoregionally in the abdomen, and diagnosed by CT, MRI, and endoscopy whether newly diagnosed distant metastases were absent or present. The causes of death were obtained from the National Cause of Death Registry.
Statistical Analysis
Results are given as mean (SD) or median (interquartile range, IQR). The Kaplan–Meier method was used to calculate survival and the differences between groups were compared with the log-rank test. Survival times were calculated from the date of surgery until the time of death or the end of follow-up. Analysis of prognostic factors for disease-free survival (DFS) was done using univariate and multivariate Cox proportional hazards regression model in stage I–III patients. Only variables with p < 0.20 at univariate analysis were entered in the multivariate analysis. All statistical tests were two-sided. A p less than 0.05 was considered significant. STATA (StatCorp 2009. Stata release 11, Statistical Software. College Station, TX: StataCorp LP) was used for statistical analysis.
Results
Baseline clinical and tumor characteristics are shown in Tables 1 and 2. Conversion to open surgery was done in 27 patients (12.2%). The reasons were unexpected invasion of adjacent organs/tumor adhesions in 10, bowel adhesions in five, otherwise difficult anatomy/obesity in nine, intraoperative complications in two, and technical problems in one. Multivisceral resections were performed in 10 patients having unexpected finding of adjacent organ invasion. Short-term surgical outcome is shown in Table 3.
Baseline characteristics and multimodal treatment.
SD: standard deviation; ASA: American Society of Anesthesiologists.
Figures in the columns are not additive because some patients had more than one comorbid condition or resection of other organs.
One patient with carcinoma of the ascending and sigmoid colon, other patients with an additional large adenoma not removable by colonoscopy or numerous adenomas.
Tumor characteristics and surgical specimen.
IQR: interquartile range; LN: lymph node.
One patient had carcinoma of the ascending and sigmoid colon.
Formalin-fixed specimens.
Operative data and short-term recovery.
IQR: interquartile range.
Figures in the column are not additive, because some patients had more than one complication.
Conservative treatment with antibiotics in four patients.
Postoperative deaths excluded (n = 3).
Long-Term Oncologic Outcome
No patients were lost to follow-up. Five of the 12 stage IV patients underwent secondary liver resection (n = 4) or cervical lymphadenectomy (n = 1) for metastases. During the median follow-up of 5.5 (IQR 3.7–8.0) years, 32 of the 210 R0-patients (15.2%) with stage I–III tumors had recurrent disease (locoregional and distant, nine (4.3%), distant only 23 (11.0%)), and 12 of them (37.5%) underwent 20 salvage operations for recurrent disease: liver resection, six; liver thermoablation, one; lung resection, eight; colon/small bowel resection, three; resection of ovary and bladder wall, one; resection of port site recurrence, one. Three other patients with a metachronous colon cancer underwent a second colon resection.
The 5-year overall survival (OS) for all 222 patients was 80.2% (95% CI: 74.0–85.1) and disease-specific survival (DSS) was 87.5% (81.9–91.4), and for those 210 R0-patients with stage I–III disease, 83.9% (77.7–88.4) and 91.3% (86.0–94.6), respectively. The 5-year DSS was 97.3% (82.3–99.6) for stage I, 95.6% (86.8–98.6) for stage II, and 83.5% (71.9–90.1) for stage III, p = 0.02. The 5-year DFS was 85.8% (80.1–90.0): stage I 94.7% (80.6–98.7), stage II 90.8% (82.3–95.3), and stage III 75.6% (64.0–83.9), p = 0.004 (Fig. 1). Increasing LN ratio significantly decreased the 5-year DFS rate: 91.7% (85.8–95.2) for LN ratio <10%, 77.1% (59.5–87.9) for LN ratio 10%–25%, and 56.1% (30.5–75.5) for LN ratio >25%, p < 0.001 (Fig. 2). Tumor site (right-sided 86.3% (78.2–91.5) vs. left-sided 85.3% (76.0–91.2, p = 0.69) had no impact on the 5-year DFS rate.
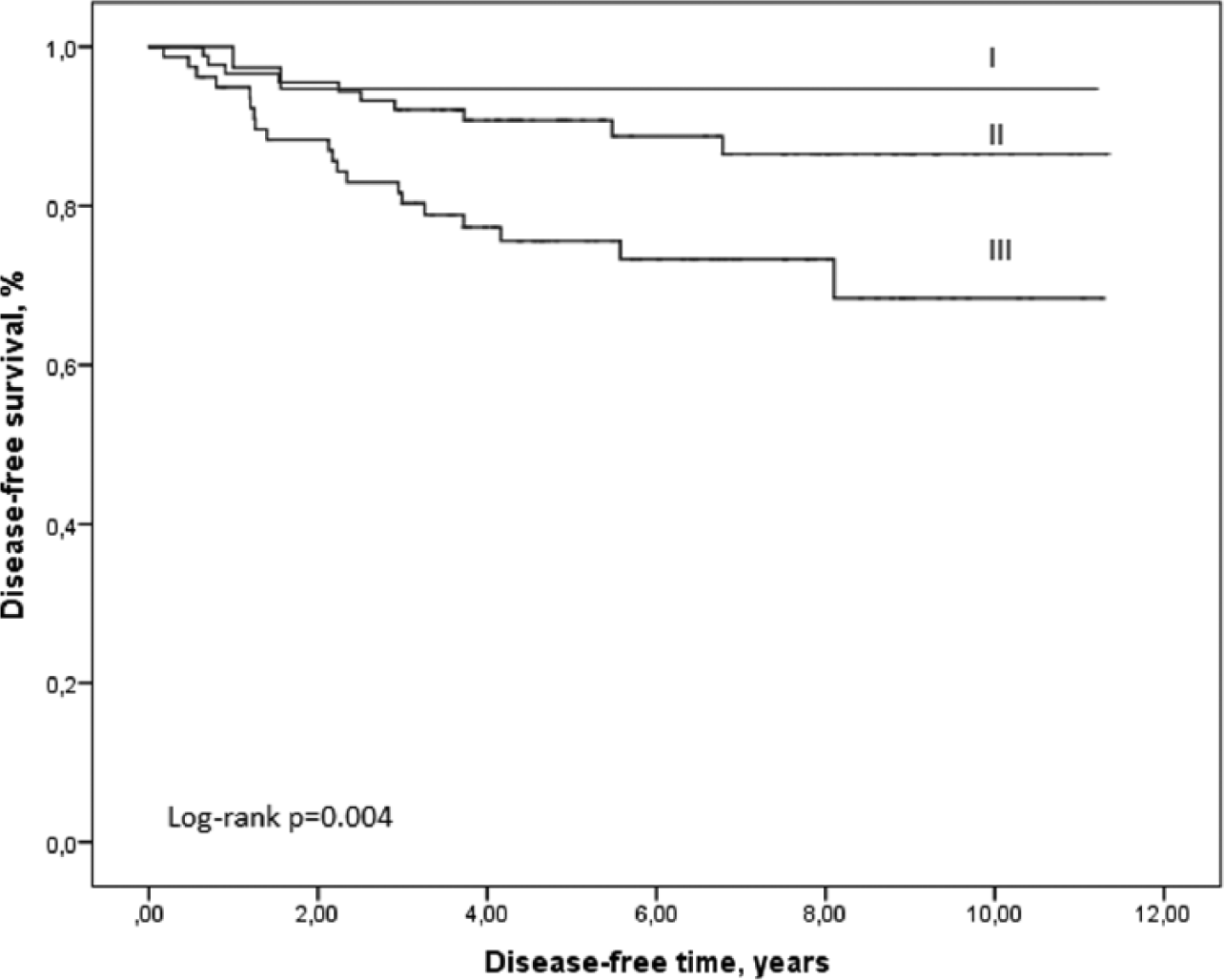
Disease-free survival by tumor stage I–III.
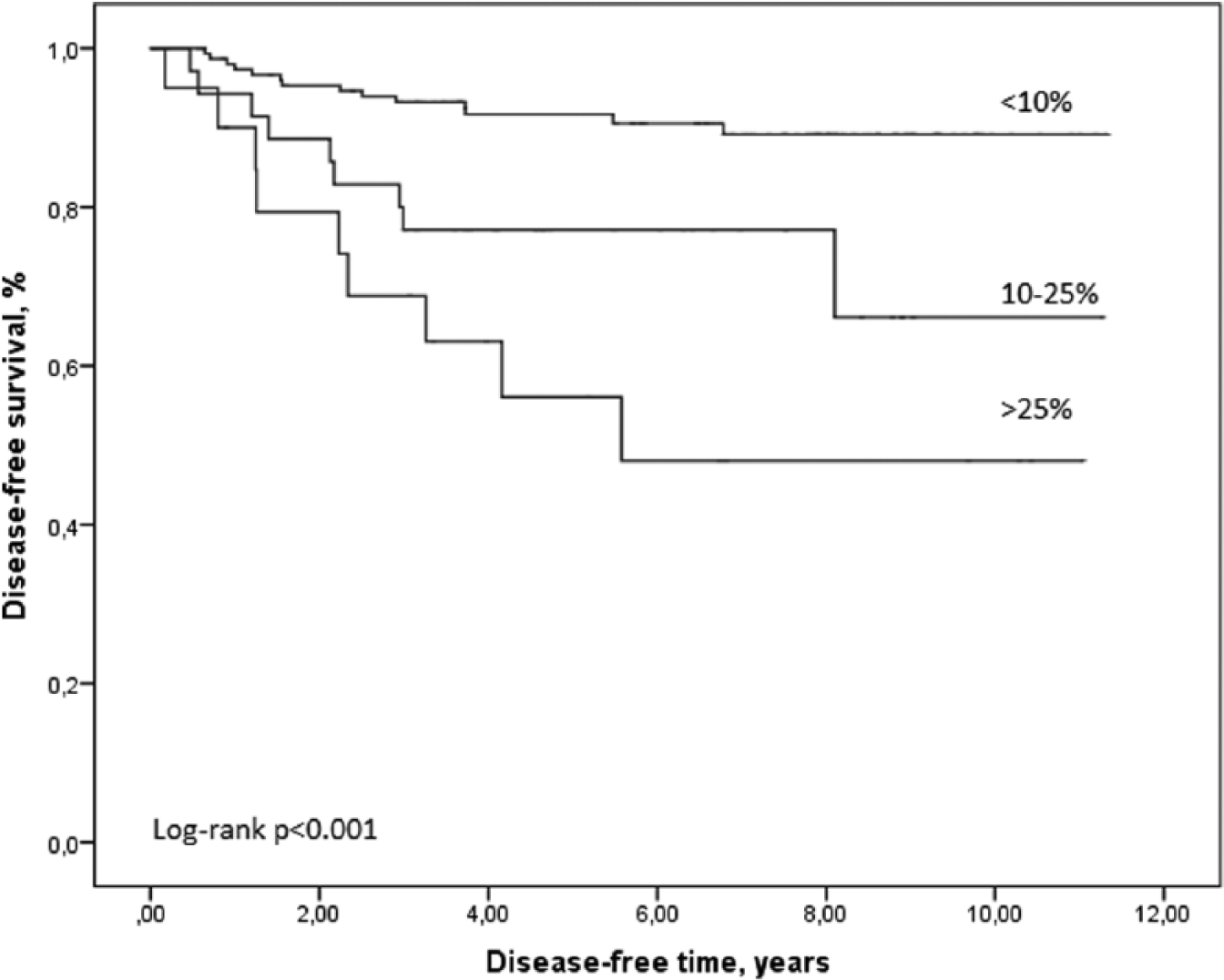
Disease-free survival by lymph node ratio in patients with stage I–III cancer.
Univariate and multivariate analyses for DFS were performed in 210 patients with stage I–III disease. Of all patient-, tumor-, and treatment-related factors, UICC stage (p = 0.007), LN ratio (p < 0.001), and adjuvant chemotherapy (p = 0.003) were prognostic factors for DFS in univariate analysis (Table 4). In multivariate analysis, LN ratio (p = 0.04) was the only independent prognostic factor for DFS, whereas other variables included in the multivariate model failed to achieve statistical significance.
Reduced univariate Cox regression model analysis of disease-free survival: UICC stage I–III patients (n = 210).
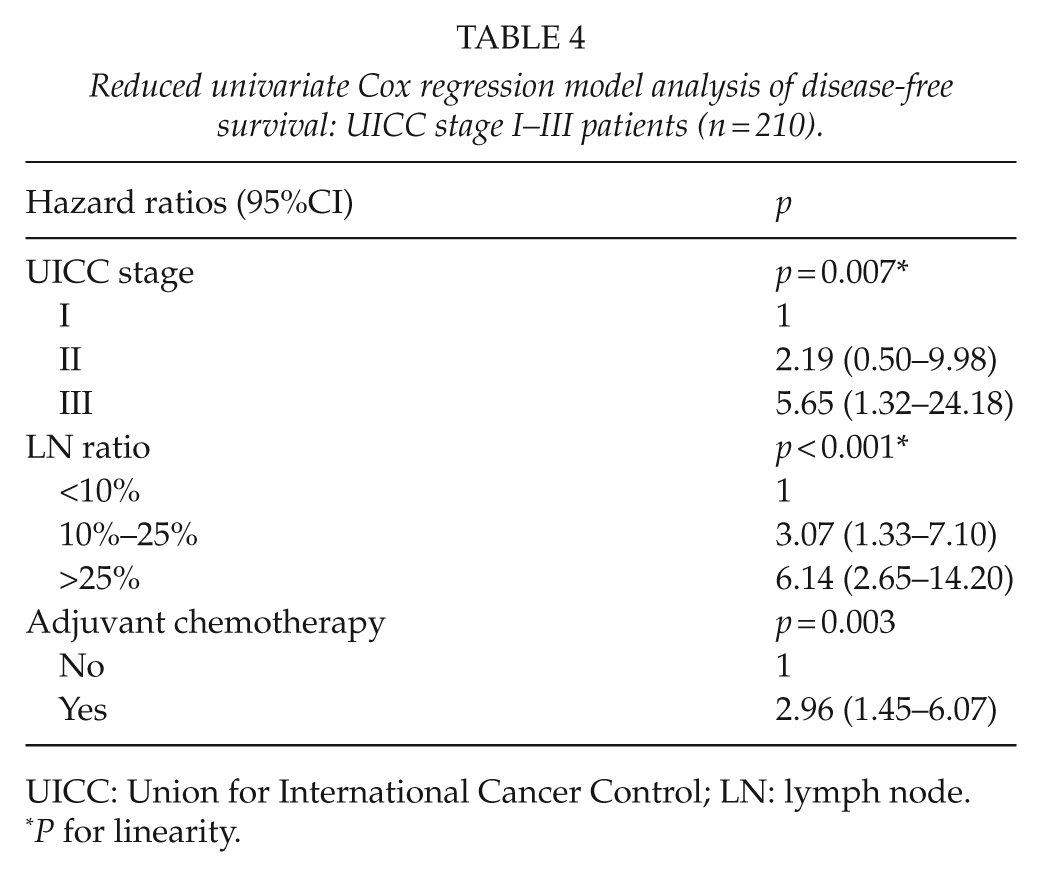
UICC: Union for International Cancer Control; LN: lymph node.
P for linearity.
Long-Term Complications
After excluding the 30-day postoperative mortality, late complications occurred in 13 of the 219 patients (5.9%) and subsequent late reoperation were performed in nine patients: five ventral hernias were corrected as well as two port site hernias. Two anastomotic strictures corrected with resection and re-anastomosis, and four patients with bowel obstruction were managed conservatively.
Discussion
Previous studies have shown that open resections with CME and central vascular ligation translate into low local recurrence rates and good overall survival (2, 5), and significantly improve DFS compared with conventional open colon resection (17). Laparoscopic CME surgery has been mainly reported for right-sided colon cancers (13, 14), and there is a lack of randomized trials. Our results show that after laparoscopic surgery for colon cancer according to the Erlangen principles (4, 5), medial to lateral mobilization of the colon along Toldt’s fascia and central vascular ligation within multimodal treatment strategy and an attempt to do salvage surgery for metastatic disease when feasible, the 5-year overall, disease-specific, and DFS rates as well as locoregional recurrence rates were comparable with those reported after open surgery by the Erlangen and Danish groups (5, 17). The extent of nodal involvement was the main prognostic factor for DFS after potentially curative (R0) resection. Overall, the laparoscopic surgery could be done with a relatively high rate of technical success, low postoperative mortality, overall short-term morbidity, reoperation and readmission rates, and short hospital stay.
The concept of CME has a similar rationale to that of TME for rectal cancer including central vascular ligation and removal of lymphovascular pedicle of the tumor-bearing colon segment within complete mesenteric envelope. Although the anatomy of the mesocolon and surgical planes has been extensively discussed for laparoscopic surgery as well as the rationale of CME (2, 3, 5, 8, 18), several studies have yielded conflicting results concerning the validity of wide mesenteric excision and lymphadenectomy with respect to survival despite a greater number of LN removed (19). In contrast, previous studies have shown that improving the plane of mesocolic dissection improved survival, especially in stage III patients (2, 17). Therefore, a good quality mesocolic excision along the anatomic planes to obtain intact mesocolic resection planes without rupture and cancer cell seeding might be equally important than the extent of mesocolic excision. In our study, the extent of mesocolic resection, when judged by the median length of proximal and distal resection margins as well as the number of LNs studied, can be considered adequate. Higher LN counts have been reported by other studies (5, 17), possibly reflecting tumor- and patient-related factors as well as the quality of the pathologic examination. The quality of mesocolic resection planes was not examined here because the quality criteria for the assessment of the surgical specimen were first introduced in 2008 (2).
The nodal positivity rate for colorectal cancer consistently approximates 40% across a wide range of studies internationally (20) as shown also here (39.6%). Our study also demonstrated that an increasing LN ratio was associated with the development of distant metastases and significantly reduced DFS. However, patients with negative LNs probably do not benefit from the CME technique. Previous studies have indicated that high LN ratio (21) and the presence of metastatic apical LNs in some patients with stage III tumors may reflect a more aggressive biological behavior and worse survival (19, 20). In agreement with that, a recent meta-analysis demonstrated that performing a high tie arterial ligation in colonic cancer to achieve apical LN clearance did not improve survival (22). Subpyloric and gastroepiploic LNs are not generally considered part of the colonic lymphatic system, but may harbor cancer cells in 1.1%–3.8% and 4% of cases, respectively. 8 According to recent consensus guidelines, the excision of these LN stations in cases of obvious tumor spread is warranted (8). This was not routinely done in our cohort of patients. Further studies are needed to assess the clinical relevance of extended lymphadenectomy.
Postoperative 30-day mortality rate (1.3%) in this study compares well with the reported range of 2%–5% from other European countries (5, 17). Also, the 30-day morbidity was in line with other reports. Anastomotic leakage is the most significant complication after colon resection. The reported incidence of symptomatic leakage in previous studies is commonly around 3%–10% (23–25) and being 9.4% here, was the main reason for laparotomy. Because most leaks occurred in left-sided anastomosis, one of the reasons may be a high tie, central vascular ligation causing hypoperfusion of the proximal colon limb (23, 24). The overall 30-day reoperation rate (7.7%) and 30-day readmission rate (5.5%) compare well with the figures reported from other centers. Late complications were rare. Although long-term hernia rates are expected to be infrequent following laparoscopic colon cancer surgery, five ventral hernias in patients who underwent conversion to open surgery were corrected surgically as well as two trocar site hernias. Two patients with anastomotic strictures underwent a late re-anastomosis.
A major challenge with this study and other similar studies is its single center nature and the lack of randomization and pathologic quality grading of the surgical specimens, first introduced by West et al. in 2008 (2). The learning curve and evolving laparoscopic experience may have played a role as well. However, laparoscopic colon surgery was done according to modern laparoscopic principles and technical aspects described by Hohenberger et al. already in 2003 (4). Our survival figures also compare well with those reported in the literature (5, 17), particularly in stage III patients, indicating that the quality of surgery has been reasonably good.
Conclusion
Laparoscopic wide mesocolic excision and central vascular ligation, today known as CME surgery, is a feasible technique for colon cancer surgery and results in good long-term oncologic outcome. Level 1 evidence for wide mesocolic excision and central vascular ligation is missing. Improving the plane of mesenteric dissection might be equally important. Randomized trials are needed to show that laparoscopic CME surgery would become the standard of care for the carcinoma of the colon in the future.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by the EVO-funding of the Central Hospital of Central Finland.