
Abstract
Background:
The impact of surgical specialization on long-term survival in patients undergoing emergent colon cancer resections remains unclear.
Method:
A retrospective analysis was conducted on all patients who underwent emergent colon cancer resections at a secondary care hospital between 2010 and 2020. The most senior surgeon performing the procedures was classified as colorectal surgeon (CS) or non-colorectal surgeon (NCS). NCS was further divided into acute care surgeons (ACSs) or general surgeons (GSs). Overall survival (OS) and cancer-free survival (CFS) were compared in patients operated by surgeons with different specializations.
Results:
A total of 235 emergent resections were performed during the study period, of which 99 (42%) were performed by CS and 136 (58%) by NCS. In adjusted Cox regression analyses, OS and CFS were similar in patients operated on by CS and NCS (hazard ratio (HR) for OS: 1.02 (0.72–1.496), p = 0.899 and HR for CFS: 0.91 (0.61–1.397), p = 0.660). Similarly, OS and CFS were equivalent in patients operated by ACS and CS (HR for OS: 1.10 (0.75–1.62), p = 0.629 and HR for CFS: 1.24 (0.80–1.92), p = 0.343). However, patients operated by GS had significantly shorter OS and CFS (HR for OS: 1.78 (1.05–3.00), p = 0.031 and HR for CFS: 1.83 (1.02–3.26), p = 0.041) compared with those operated by ACS and CS.
Conclusion:
Long-term survival after emergent colon cancer resections was similar in patients operated on by CS and NCS, and the subgroup of ACS, indicating equivalent comparable surgical quality. The less favorable poorer survival observed for patients operated on by GS may possibly be due to less frequent exposure to colorectal and emergent surgery.
Keywords
Introduction
Colorectal cancer is the second most common cancer worldwide, accounting for 10% of global cancer incidence and 9.4% of cancer-related deaths. 1 Surgical resection remains the only curative treatment for colon cancer, with 70%–80% of patients being suitable for resection with curative intent. 2 Many patients with colon cancer initially have vague or no symptoms, and up to 30% of patients present late often with emergent symptoms due to mechanical obstruction or perforation.3–5
The high proportion of patients in need of emergent surgery is a significant challenge, as these individuals tend to have less favorable outcomes with more frequent and severe complications, higher postoperative mortality, and shorter long-term survival compared with patients undergoing elective resections.3–8 The relatively poor outcomes following emergent resections are often attributed to patient-related factors, as these patients typically are older, have more comorbidities, present with more advanced tumor stages, and are in worse physiological condition than those undergoing elective procedures. 9
In addition to patient-related factors, growing evidence suggests that surgeon-related factors—such as surgical experience and surgical specialization—may influence postoperative outcomes.10–13 Several studies have shown superior short- and long-term results after for elective colon resections performed by colorectal surgeons (CSs) compared with those of non-colorectal surgeons (NCS).11,12,14,15 However, the management of patients requiring emergent surgery due to mechanical obstruction or perforation is more complex, and the surgical challenge is substantially greater than that of elective resections. Some studies of emergent colon cancer resections report fewer complications and lower postoperative mortality in patients operated by CS, 16 but most studies, including one recently published by our group, 17 report similar morbidity and mortality rates in patients operated by CS and NCS. These observations suggest that the quality of emergent colon resections performed by CS and NCS generally is equivalent.18–22
In sharp contrast to the relative abundance of studies comparing short-term outcomes following emergent colon cancer resections performed by surgeons of different specializations, there is scarcity of reports on long-term survival outcomes. To our knowledge, the only available study reported that patients undergoing emergent colon resections performed by CS had significantly higher 5-year survival rates compared with those operated on by NCS. 2
The lack of reports on long-term outcomes following emergent resections for colon cancer performed by surgeons with different specializations stimulated us to conduct this retrospective study. The primary aim was to compare the effect of surgical specialization on overall survival (OS) and cancer-free survival (CFS) in patients undergoing emergent colon cancer resections at a secondary care hospital.
Methods
Study population
This retrospective study included patients aged 18 years and older who underwent resections for colon cancer at Helsingborg hospital between 2010 and 2020. The Swedish Colorectal Cancer Registry (SCRCR) was used to identify patients and extract demographic and clinical data. The SCRCR is a nationwide, prospective registry for colorectal cancer with near-complete coverage. 23 Patients operated for appendiceal neoplasms or rectal cancer were excluded from the study. Medical records for each patient were reviewed to obtain additional clinical information and validate the data from the registry. Retrospective medial record review guidelines were followed to minimize information bias during data collection. 24
Colon cancer staging was based on the Tumor-Node-Metastasis (TNM) classification system. 25 Unplanned colon resections performed within 48 h of acute admission were classified as emergent, while all other procedures were classified as elective. Emergent resections performed between 5:00 pm and 7:00 am were considered nighttime surgeries, while those performed during the remaining hours were classified as daytime surgeries. Postoperative care and follow-up were managed by the hospital’s colorectal surgery unit. Postoperative treatment and follow-up were determined at multidisciplinary tumor board conferences (MDT). All patients participated in a standard follow-up program, which included computed tomography scans at 1 and 3 years post-surgery, and colonoscopy 3 years after surgery. Long-term oncological outcomes, including locoregional and systematic recurrence, were recorded. Patients were followed until death or for a maximum of 5 years postoperatively.
Surgeons and surgical specialization
The overall surgical experience of the surgeons was assessed by calculating the time from their board certification in general surgery to the date of surgery for each resection. Information regarding the date of board certification was obtained from the Swedish National Board of Health and Welfare for each surgeon. In cases where more than one board-certified surgeon actively participated in the procedure, the most senior surgeon was identified based on their time from board certification to the date of the resection. Surgeons were categorized into two groups based on their surgical specialization: CSs and NCSs. The NCS group was further subdivided into two categories: acute care surgeons (ACSs) and general surgeons (GSs). For this study, GS included all board-certified surgeons with other specializations than CS or ACS. In Sweden, colorectal surgery and acute care surgery are not recognized official as surgical specializations. Therefore, CS were defined as surgeons regularly working at the hospital’s colorectal unit, while ACS referred to surgeons regularly working at the unit for trauma and emergency surgery.
Statistics
The distribution of continuous variables was assessed using the Kolmogorov–Smirnov test. Since the data were not normally distributed, results were presented as medians and 25th–75th percentiles. The Mann–Whitney U-test was used to compare continuous variables between two groups, and the Kruskal–Wallis test was used for comparisons among multiple groups. Categorical variables were presented as numbers and percentages, and differences between groups were analyzed using the Chi-square test.
Kaplan–Meier curves were used to describe the OS and CFS, and comparisons between groups were made using the log rank test. OS was plotted from the day of surgery, counting deaths as events and the remainders as censored as of the last day of follow-up. Similarly, in patients without macroscopically eveident generalized cancer, CFS was plotted counting cancer reccurence or deaths as events and the rest as censored.
Cox regression analyses were performed to assess the effects of multiple variables and adjust for potential confounding factors influencing survival. Adjustments for patient age, gender, ASA classification, tumor stage, overall surgical experience, indication for emergent surgery, nighttime surgery, and adjuvant chemotherapy were entered simultaneously in the regression models. A p-value of less than 0.05 was considered statistically significant.
All statistical analyses were performed using the IBM SPSS® Statistics version 25 (IBM Corp., Armonk, NY, USA). The study was approved by the Swedish Ethical Review Authority (2019-04329).
Results
Study population
Between 2010 and 2020, a total of 1121 patients underwent colon resections for colon cancer at Helsingborg hospital. Of these, 235 (21%) patients underwent emergent procedures. No patients requiring emergent surgery were referred to other hospitals, and the use of stents as a bridge to elective surgery was not employed during the study period. A laparoscopic approach was used in two (1%) patients, while the remaining patients underwent conventional open surgery. Following data validation, there were no missing data.
All emergent resections were performed by 30 senior board-certified surgeons, of whom 14 were classified as CS and 16 as NCS. The NCS group consisted of 5 ACSs and 11 GSs. Ninety-nine (42%) of the emergent resections were performed by CS, and 136 (58%) of the resections were performed by NCS, of which 107 (79%) were performed by ACS and 29 (21%) by GS.
The median number of annual colon cancer resections performed by CS was significantly higher than that performed by NCS (18.7 (9.1–27.5) versus 2.4 (0.9–5.98), p < 0.001). However, the median overall surgical experience was similar between the two groups of surgeons (CS: 10.5 years (7.2–20.7) versus NCS: 14.0 years (6.5–20.9), p = 0.790). The annual resection volumes of ACS (5.9 (3.2–12.2)) and GS (1.6 (0.9–5.4)) were significantly lower than those of CS (p < 0.001), but there was no difference in overall surgical experience among the three groups of surgeons: CS (10.5 (7.2–20.7) years), ACS (16.0 (8.0–20.5) years), and GS (14.0 (5.0–21.5) years; p = 0.889).
The median follow-up for all patients was 3.6 years, ranging from 0.0 to 5 years. The median follow-up for patients who died was 1.5 years (range 0.0–4.99 years), while the median follow-up for patients who did not die during through the 5-year follow-up was 5.0 years (range 2.4–5 years).
Outcomes associated with surgical specialization
Patient demographics, including age, gender, ASA class, and the indications for emergent surgery, were similar across the different surgeon specialization groups in patients who underwent colon resections performed by surgeons with different specializations (Tables 1 and 2). Similarly, the types of colon resections, the proportion of nighttime resections, and the proportion of patients treated with adjuvant chemotherapy were equivalent in all groups of patients. In comparison with patients operated by CS, the number of resected lymph nodes and tumor stages were similar in patients operated by CS and those operated by NCS, including the subgroups classified as ACS and GS.
Patient characteristics and descriptions of surgical procedures in patients who underwent emergent colon cancer resections performed by colorectal and non-colorectal surgeons.
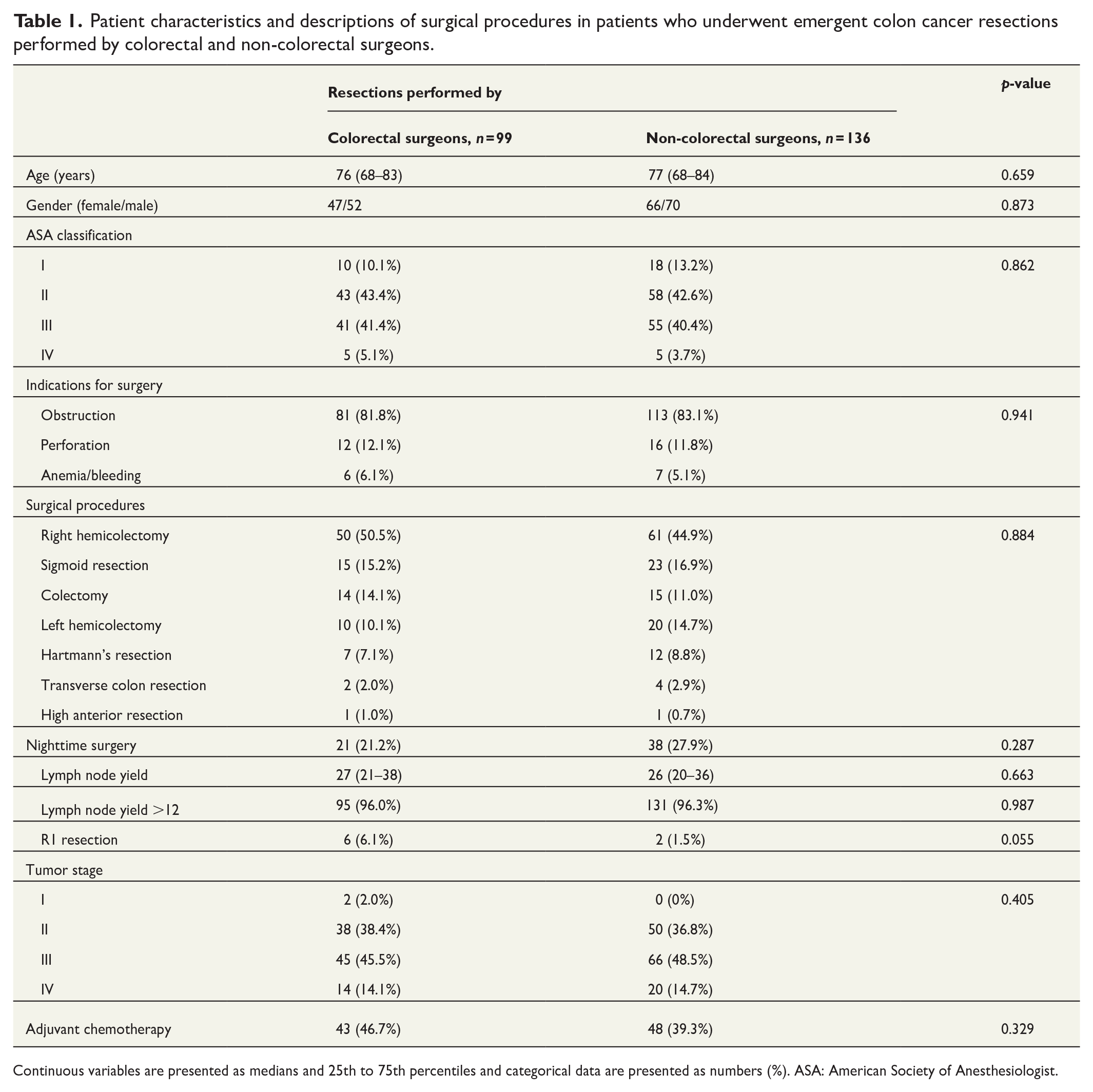
Continuous variables are presented as medians and 25th to 75th percentiles and categorical data are presented as numbers (%). ASA: American Society of Anesthesiologist.
Patient characteristics and descriptions of surgical procedures in patients who underwent emergent colon cancer resections performed by colorectal surgeons, acute care surgeons, and general surgeons.
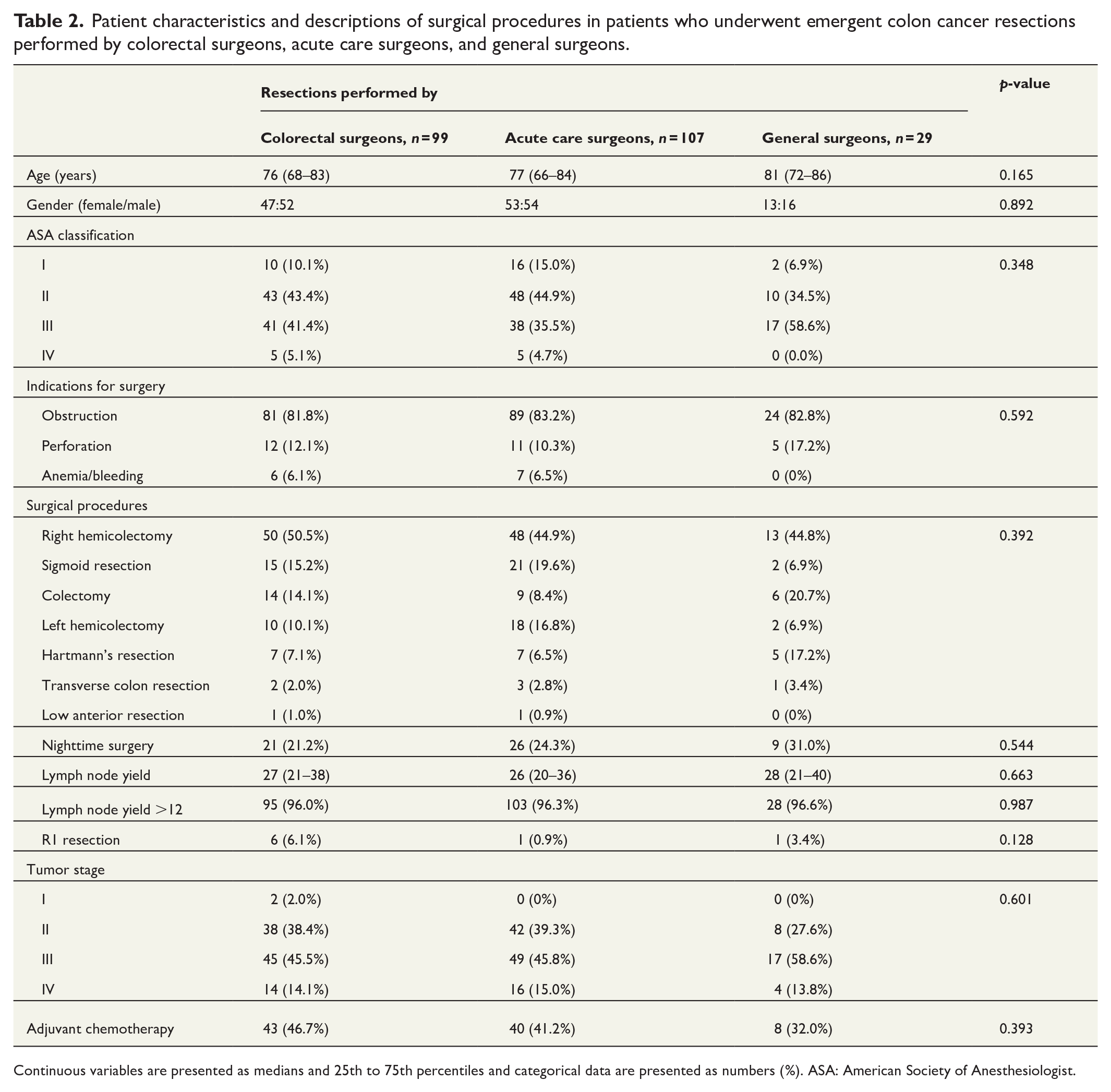
Continuous variables are presented as medians and 25th to 75th percentiles and categorical data are presented as numbers (%). ASA: American Society of Anesthesiologist.
The cumulative OS and CFS was similar in patients who underwent emergent colon cancer resections performed by CS and NCS (Figs 1 and 2). This observation was confirmed by Cox regression analyses with adjustments for factors perceived as clinically relevant confounders (hazard ratio (HR) for OS: 1.02 (0.72–1.46), p = 0.899; HR for CFS: 0.91 (0.61–1.37), p = 0.660).
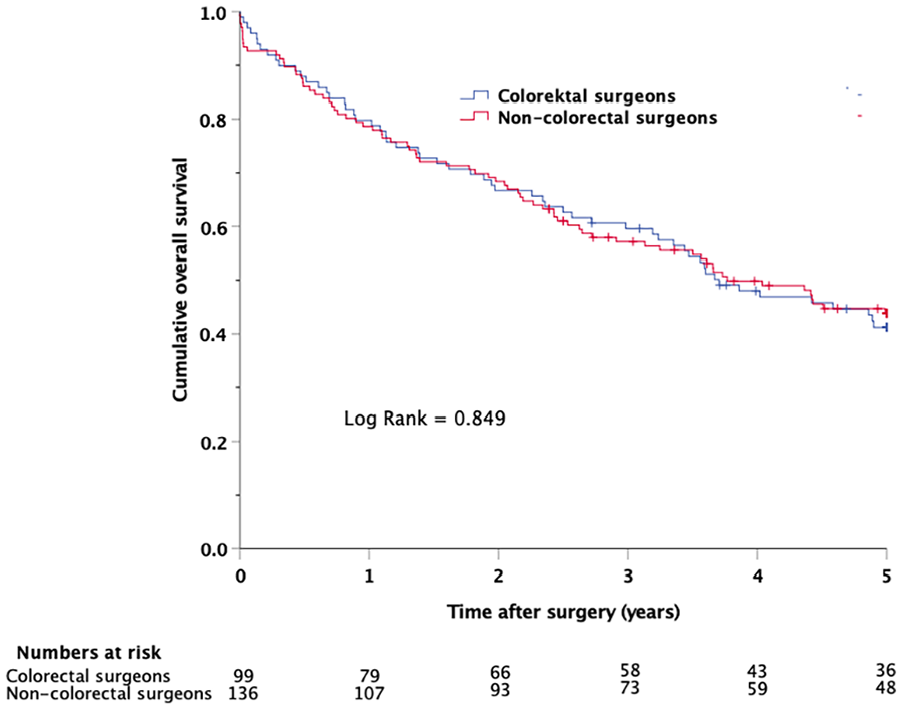
Kaplan–Meier plot showing cumulative overall survival in patients who underwent emergent colon cancer resections performed by colorectal and non-colorectal surgeons.
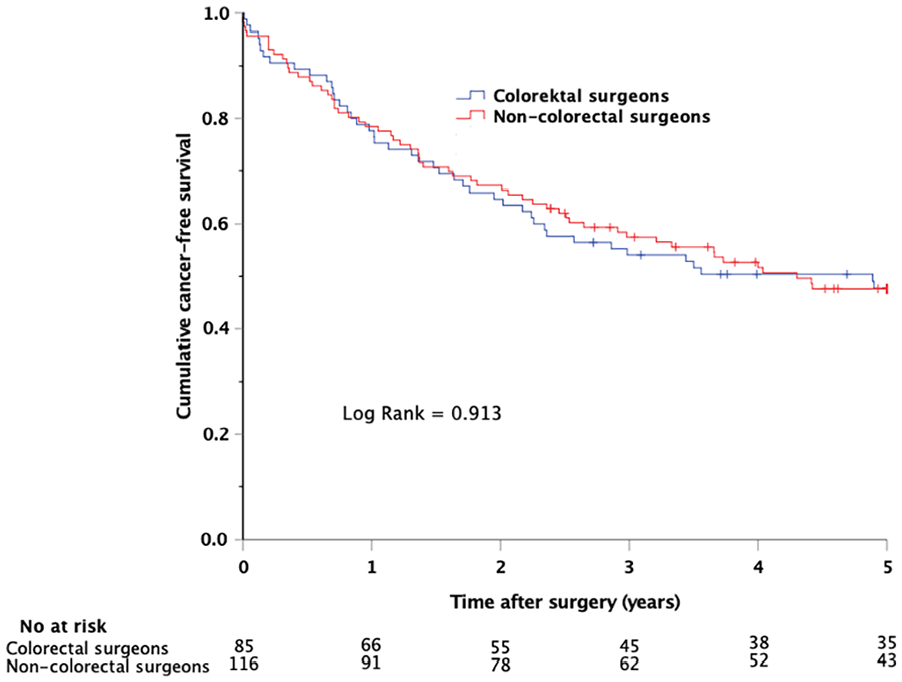
Kaplan–Meier plot showing cumulative cancer-free survival in patients who underwent emergent colon cancer resections performed by colorectal and non-colorectal surgeons.
However, the cummulative OS and CFS differed significantly in patients operated by CS, ACS, and GS, with similar survival curves for patients operated by CS and ACS, but with less advantageous survival in patients operated by GS (Figs 3 and 4). Complementary adjusted Cox regression analyses revealed no differences in OS or CFS between patients operated by ACS and CS (HR for OS: 1.10 (0.75–1.62), p = 0.629; HR for CFS: 1.24 (0.80–1.92), p = 0.343). In contrast, resections performed by GS were significantly associated with shorter OS and CFS, with adjusted HRs nearly twice as high as those for ACS and CS (HR for OS: 1.78 (1.05–3.00), p = 0.031 and HR for OS 1.83 (1.02–3.26), p = 0.041).
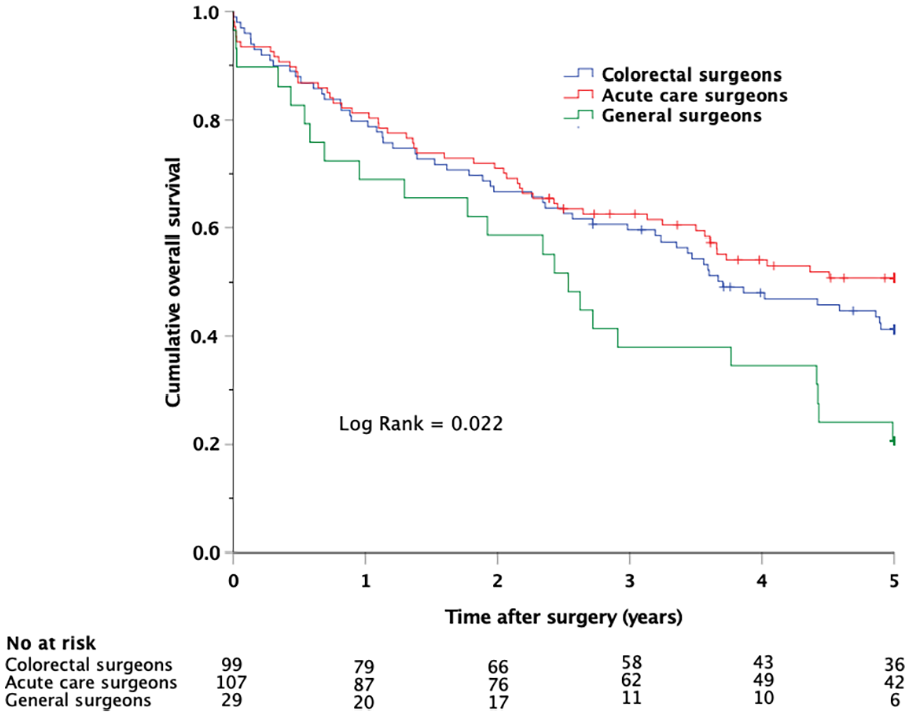
Kaplan–Meier plot showing cumulative overall survival in patients who underwent emergent colon cancer resections performed by colorectal surgeons, acute care surgeons, and general surgeons.
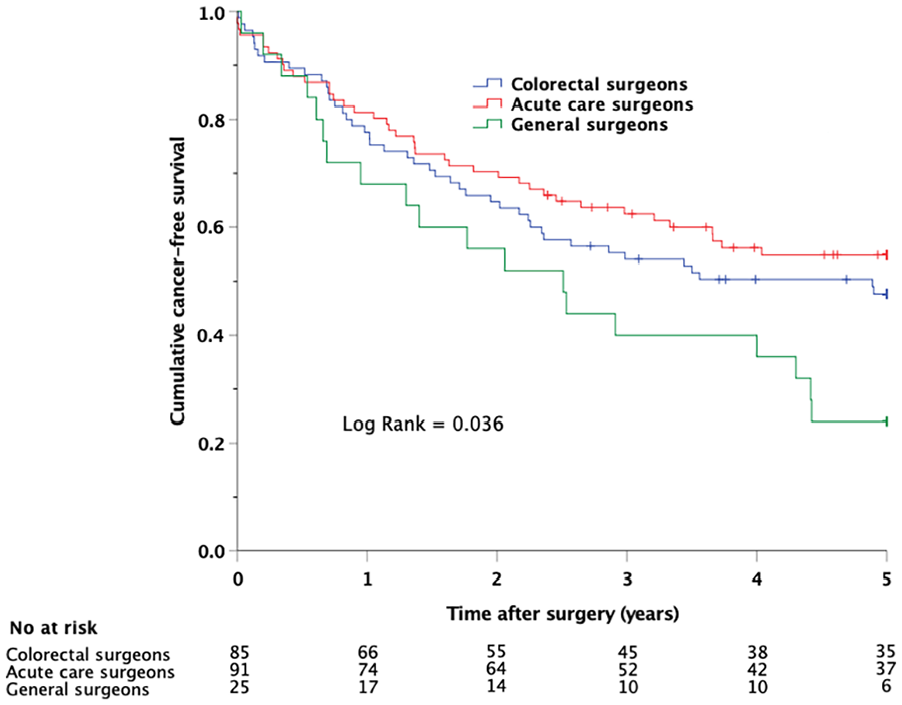
Kaplan–Meier plot showing cumulative cancer-free survival in patients who underwent emergent colon cancer resections performed by colorectal surgeons, acute care surgeons, and general surgeons.
Discussion
This study assessed the influence of surgical specialization on long-term outcomes after emergent resections for colon cancer. The primary observation was that the number of harvested lymph nodes, the proportion of R0 resections, OS, and CFS were similar in patients operated on by CSs and NCSs, including the subgroup of ACSs. The results suggest that oncological quality of resections performed by ACSs and CS was equivalent. However, patients operated on by GSs had less favorable long-term outcomes, with shorter OS and CFS.
It is well established that patients undergoing elective colon resections for cancer performed by specialized CS experience lower morbidity and postoperative mortality compared with those operated on by NCS.11,13–15 This has contributed to an increasing centralization of colorectal surgery to high-volume centers.26 However, the management of patients requiring emergent colon resections for cancer is more challenging than that of patients who undergo elective procedures, and the favorable outcomes for patients operated by CS in elective settings cannot be directly extrapolated to emergent procedures. Elective colon cancer surgery is always preceded by thorough assessments of the patient’s condition and comorbidity, and treatment decisions are made at MDT meetings. Consequently, elective resections are typically well planned and performed on physiologically stable patients, often in a stress-free environment where unexpected adverse events are rare. This is in sharp contrast to the surgical challange to perform emergent resections in which the surgeon have to confront the additional challenge, to manage acute surgical problems in patients who are in a deranged physiological state due to mechanical obstruction or intestinal perforation. The magnitude of this challenge may often be substantial, as a variety of time-critical, high-pressured and occasionally unfamiliar situations require decisions in difficult clinical settings. This implies that the surgical challange to manage patients with acute complications of colon cancer is greater than that of corresponding elective situations.
Although surgical specialization implies expertise in a specific area of surgery, specialization alone does not imply surgical competence such as technical proficiency, good clinical judgment, or extensive surgical experience. Specialized CSs generally have substantial experience in performing adequate oncologic surgery for colon cancer, but may lack experience in managing acute surgical problems in critically ill patients. Conversely, ACSs may have extensive experience in managing acute surgical problems in critically ill patients, but may have less experience in performing comprehensive oncological dissections. Given the complex nature of emergent surgery for colon cancer, it is not immediately obvious which type of surgical specialization is best suited for these procedures.
Although there are some reports suggesting that specialized CSs have better short-term outcomes following emergent resections for colon cancer, 16 there are numerous studies reporting similar morbidity and mortality rates in patients who underwent emergent colon resections performed by CS and NCS.17–22 In contrast to the relative abundance of studies of the effect of surgical specialization on short-term results, it is problematic that similar reports on long-term survival outcomes are lacking. To our knowledge, the only available report on long-term outcomes following emergent resections for colon cancer performed by surgeons with different specializations is a retrospective study based on data from the SCRCR, which included 2931 emergent resections performed in Sweden between 2007 and 2010. 2 In contrast to the findings in the present study, Bergvall et al. reported an odds ratio for 5-year mortality in patients operated by NCS that was more than two times higher than that of patients operated on by CS, concluding that long-term survival was superior for patients operated by CS.
The contrasting conclusions between the present study and that of Bergvall et al. may be attributed to differences in the definitions of emergent surgery and the relative importance of the participation of surgeons with an interest in colorectal surgery. In the present study, emergent surgery was defined as resections performed within 48 h of admission. In contrast, in studies solely based on data from the SCRCR, emergent surgery is defined as procedures conducted during an unplanned admission due to acute medical conditions, regardless of the time from admission. 27 This broader definition of emergent surgery is problematic because it leads to more heterogenous groups of patients that are difficult to compare as they require surgery at different times from admission depending on the severity of their conditions. The most critically ill patients willrequire immediate surgery, even during nighttime, when CS may not be available at many surgical units. Furthermore, the less critically ill patient can often wait until the following morning or even longer. Thus, it is possible that a definition of emergent surgery with no time limit leads to to a selection of less critically ill patients being operated on by CS several days after admission, which may lead to more favorable postoperative outcomes compared with those of surgeons with other specializations.
Although there was no significant difference in the proportion of resections performed by CS and NCS during nighttime in the present study, this perception is supported by a study from a tertiary center in Norway. They reported that only 7% of emergent colorectal cancer resections were performed by specialized gastrointestinal surgeons at night, which was significantly lower than the proportion of emergent resections performed by this group of during daytime. 28 Another potential reason for the contrasting conclusions of the studies is the relative importance of the involvment of of surgeons with an interest in colorectal surgery. Studies solely based on data from the SCRCR only have information on the highest formal competence in colorectal surgery but lacks information regarding the competence of other surgeons actively involved in the procedures. In Sweden, and most likely in many other countries, emergent resections for colon cancer are rarely performed by a single surgeon alone. It is therefore not uncommon that a relatively inexperienced surgeon with an interest in colorectal surgery performs emergent colon resections in collaboration with a more experienced non-colorectal surgeon. There was a marked difference in the proportion of emergent resections performed by CS in the study by Bergvall et al. and the present study (68% vs. 42%). This discrepancy may be due todifferences in the emphasis placed on the involvement of surgeons with an interest in colorectal surgery.
In the study by Bergvall et al., CSs were registered as the highest surgical competence, regardless of the experience and competence of other surgeons involved in the procedures, whereas we defined seniority and responsibility based on surgical experience alone. It is possible that Bergvall and coworkers registered resections as being performed by CS although they were performed in collaboration with more experienced surgeons with other specializations, a procedure for wich the latter rather than the former, has the overall responsibility for the quality and outcome. Consequently, the contrasting results and conclusions of the two studies may be explained by differences in the definitions of emergent surgery in combination with differences concerning the significance placed on the participation of CS, regardless of the surgical experience of other surgeons involved in the procedure.
The observation that the tumor stage, the lymph node yield, the rate of R0 resections and the OS and CFS were similar in patients operated on by CS and ACS suggests that the oncological quality of resections for colon cancer performed by these groups of surgeons was equivalent. However, the less favorable long-term survival observed in patients operated on by GS is more difficult to explain as tumor characteristics and lymph node yield were comparable with those of patients operated on by CS and ACS. In a previous study based on the same study population, patients who underwent emergent colon resections performed by GS had significantly more frequent and severe postoperative complications. 17 Given that complications are associated with poor long-term survival,7,29,30 one can speculate as to whether the observed differences in long-term survival could be explained by a higher complication rate in patients operated by GS. However, as the group of patients operated on by GS was relatively small, conclusions should be made with caution.
A key strength of this study is the homogeneity of the study population, with no patients having rectal cancer or benign disease. The clear definition of emergent surgery only including resections performed within 48 h of admission, as well as the identification of the specialization of the most senior surgeon actively involved in the procedures, also adds to the study’s robustness. Limitations of the study include its retrospective nature, which may limit precision and validity compared with prospective trials, although conducting a prospective randomized trial in this setting would be extremely challenging. Another limitation is the single center cohort design that may limit generalizability, as local variations in patient selection and surgical practice may influence outcomes. Furthermore, as the definition of surgical specializations may vary between studies, conclusions may not be universal, and comparisons should be made with caution.
In conclusion, the findings of this study suggest that emergent resections for colon cancer were performed with equivalent oncological quality by CS and NCS, and the subgroup consisting of ACS. This was suggested by similar numbers of harvested lymph nodes, similar R0 resection rates, and similar OS and CFS. However, patients operated on by GS had less favorable long-term survival, possibly due to less frequent exposure to both colorectal and emergent surgery. Regular rotations at acute care and colorectal units to preserve competence and maintain surgical quality may be needed to improve long-term outcomes for patients requiring emergent colon cancer resections.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Research ethics and patient consent
The study was approved by the Swedish Ethical Review Authority (2019-04329) and according to the approval informed consent was not needed.
Clinical trial registration
Not applicable.