
Abstract
Background:
Pancreatoduodenectomies are complex surgical procedures with considerable postoperative morbidity and mortality. Here, we describe complications and outcomes in patients requiring surgical revisions following pancreatoduodenectomy.
Methods:
A total of 1048 patients undergoing a pancreatoduodenectomy at our institution between 2002 and 2019 were analyzed retrospectively. All patients with surgical revisions were included. Revisions were divided into early and late using a cut-off of 5 days after the first surgery. Statistical significance was examined by using chi-square tests and Fisher’s exact tests. Survival analysis was performed using Kaplan–Meier curves and log-rank tests.
Results:
A total of 150 patients with at least 1 surgical revision after pancreatoduodenectomy were included. Notably, 64 patients had a revision during the first 5 days and were classified as early revision. Compared with the 86 patients with late revisions, we found no differences concerning wound infections, delayed gastric emptying, or acute kidney failure. After late revisions, we found significantly more cases of sepsis (31.4% late versus 15.6% early, p = 0.020) and reintubation due to respiratory failure (33.7% versus 18.8%, p = 0.031). Postoperative mortality was significantly higher within the late revision group (23.2% versus 9.4%, p = 0.030).
Conclusion:
Arising complications after pancreatoduodenectomy should be addressed as early as possible as patients requiring late surgical revisions frequently developed septic complications and multiorgan failure.
Keywords
Context and relevance
Pancreatoduodenectomies are complex surgical procedures associated with a considerable postoperative morbidity even in high-volume centers. Whereas most postoperative complications are successfully addressed by interventional therapies, there are still complications that require a surgical revision. However, at the time of the surgical revision, many patients already run into a septic condition. In our analysis, we provide first data supporting the strategy of early surgical revisions in order to prevent further complications such as severe bleedings or multiorgan failure.
Introduction
Pancreatoduodenectomies are known as complex surgical procedures associated with considerable postoperative morbidity and mortality.1–4 While conservative treatment or interventional procedures (e.g., percutaneous biliary drainage) have shown a high success rate and therefore have become the treatment of choice in many cases, revision surgery is performed in 10%–20% of the cases.5,6 The most common causes of postoperative morbidity are pancreatic fistulas, postpancreatectomy hemorrhage (PPH), and delayed gastric emptying (DGE). 2 Pancreatic fistula is also the most important single cause of mortality following pancreatoduodenectomy. 2 Several risk factors have been identified that increase the rate of pancreatic fistulas after pancreatoduodenectomy such as body mass index (BMI), age, comorbidity, gland texture, duct size, and perioperative bleeding. 3 Although a special anastomotic technique and the use of somatostatin analogs may slightly decrease the risk of pancreatic fistula, they cannot prevent them. 3 The life-threatening character of type C pancreatic fistulas has been described in detail in a cohort of patients from five surgery departments in the northwest of France. 7 In this cohort, pancreatic fistulas following pancreaticoduodenectomies occurred in 16% of patients. One-third of these fistulas were type C fistulas which resulted in a mortality rate of almost 40%. Major causes for mortality in these patients were sepsis and recurrent bleeding episodes, 7 then called PPH.8–13 While hemorrhage occurring early after pancreas resections usually can be controlled easily surgically, management of hemorrhage occurring later than 5 days after primary surgery is complicated and is associated with significant mortality,8,9,13,14 in which hemorrhagic shock, uncontrollable rebleeding, sepsis, and multiorgan failure are the major causes of death. 12 Late hemorrhage is almost exclusively induced by pancreatic fistulas.9–12,14 One improvement of pancreatic surgery would therefore be the prevention of pancreatic fistula-induced complications. Complete pancreatectomy in high-risk patients would be an option to prevent fistulas but is associated with severe postoperative morbidity due to lasting exocrine and, more importantly, endocrine insufficiency.15,16
Furthermore, patients can experience severe complications that are unpredictable during primary surgery even by expert surgeons. A strategy of forming the pancreatoenteric anastomosis followed by early revision with reinspection of the pancreatic remnant and either pancreatectomy or conversion to other anastomotic techniques in patients with biochemically detectable fistulas prior to sepsis or bleeding events would be an option.
To provide first data potentially supporting this strategy, we analyzed in a retrospective cohort if patients running into severe complications can be identified in advance and which outcomes can be expected in patients with early and late surgical revisions.
Patients and methods
Patient collective
Our study was performed as a single-center study at the University Medical Center Freiburg. Clinical data of 1048 patients having undergone a pancreatoduodenectomy in our institution between January 2002 and December 2019 were evaluated retrospectively. All patients with pancreas resections entering the operating theater more than once were included in the analyses. Required surgical revisions were divided into early and late revisions by using a cut-off of 5 days after the initial pancreatoduodenectomy.
Data collection and variables
Data collection at our clinic is performed continuously using a prospectively maintained pancreatic surgery SPSS database. Besides demographic data, preoperative BMI, and ASA score, variables include details on duration of initial pancreatectomy, blood transfusion, indications for initial pancreatectomy and for the first surgical revision, as well as duration of hospital stay and in-hospital mortality. Follow-up studies with general practitioners or oncologists and cancer registries provide information on long-term survival. Complications requiring surgical revisions such as PPH or pancreatic fistula were graded by current international definitions.17–19 The severity of postoperative complications was graded following the Clavien-Dindo classification. 20
Statistical analysis
Statistical analysis was performed using SPSS (IBM SPSS Statistics for Windows, Version 27.0. IBM Corp., Armonk, NY, USA). After performing explorative analysis and descriptive statistics, statistical significance was examined by using chi-square tests and Fisher’s exact tests for categorical variables and ANOVA for continuous variables. Survival estimates were calculated using Kaplan-Meier curves and log-rank tests. Results with a p-value < 0.05 were considered statistically significant.
Ethics and patient consent
Data collection and analysis were performed in accordance with the Declaration of Helsinki and were approved by the local ethics committee (Ethics Committee of Albert-Ludwigs-University Freiburg, Germany, EK-No. 22-1068). Since 2014, patients scheduled for pancreatic surgery at our university hospital have given their written approval for data and tissue analysis. For the former years, there is no specific patient consent available, which we consider acceptable due to the retrospective character of our study.
Results
Descriptive analysis of patient collective and demographic data
From January 2002 to December 2019, a total of 1048 patients underwent a pancreatoduodenectomy (pylorus-preserving pancreatoduodenectomy or Whipple procedure) at the University Medical Center Freiburg. The most frequent indication for the initial pancreatoduodenectomy was pancreatic ductal adenocarcinoma, followed by periampullary carcinomas, chronic pancreatitis, and intraductal papillary mucinous neoplasm (Table 1). A total of 150 patients required surgical revisions after pancreatoduodenectomy and were included in the analysis. One to eight surgical revisions were performed (mean 1.75 revisions entire collective, 1.63 revisions early group, and 1.84 revisions late group, p = 0.301). For our analysis, we divided our cohort into early and late revisions, early when the first surgical revision was done within the first 5 days after pancreatoduodenectomy. A total of 64 patients (42.7%) underwent the first surgical revision during the first 5 days after the initial surgery (classified as early revision), whereas 86 patients (57.3%) had a revision after the fifth postoperative day (POD) (classified as late revision). There were no differences concerning age (p = 0.656), BMI (p = 0.446), or ASA score (p = 0.615) between early and late revisions. Interestingly, we could find a significant difference concerning the sex of patients. Male patients were overrepresented in the late revision group (69.8% male, 30.2% female), whereas women mostly belonged to the early revision group (53.1% female, 46.9% male, p = 0.004). Overall, comorbidities were distributed equally in both groups (p = 0.073), especially coronary artery disease (p = 0.567), arterial hypertension (p = 0.096), pulmonary (p = 0.547) or hepatic comorbidities (p = 0.522), chronic renal failure (p = 0.167), or diabetes mellitus (p = 0.202). However, a positive history of alcohol abuse (p = 0.026) or nicotine consumption (p = 0.040) was more likely in patients of the late revision group. The rate of blood transfusions in the context of initial pancreatoduodenectomy was equal between both groups (p = 0.372), whereas the duration of the initial pancreatectomy was significantly longer in the late revision group (461 min versus 419 min, p = 0.011) (Table 1).
Demographic data and indications for the initial pancreatoduodenectomy as well as for the first surgical revision.
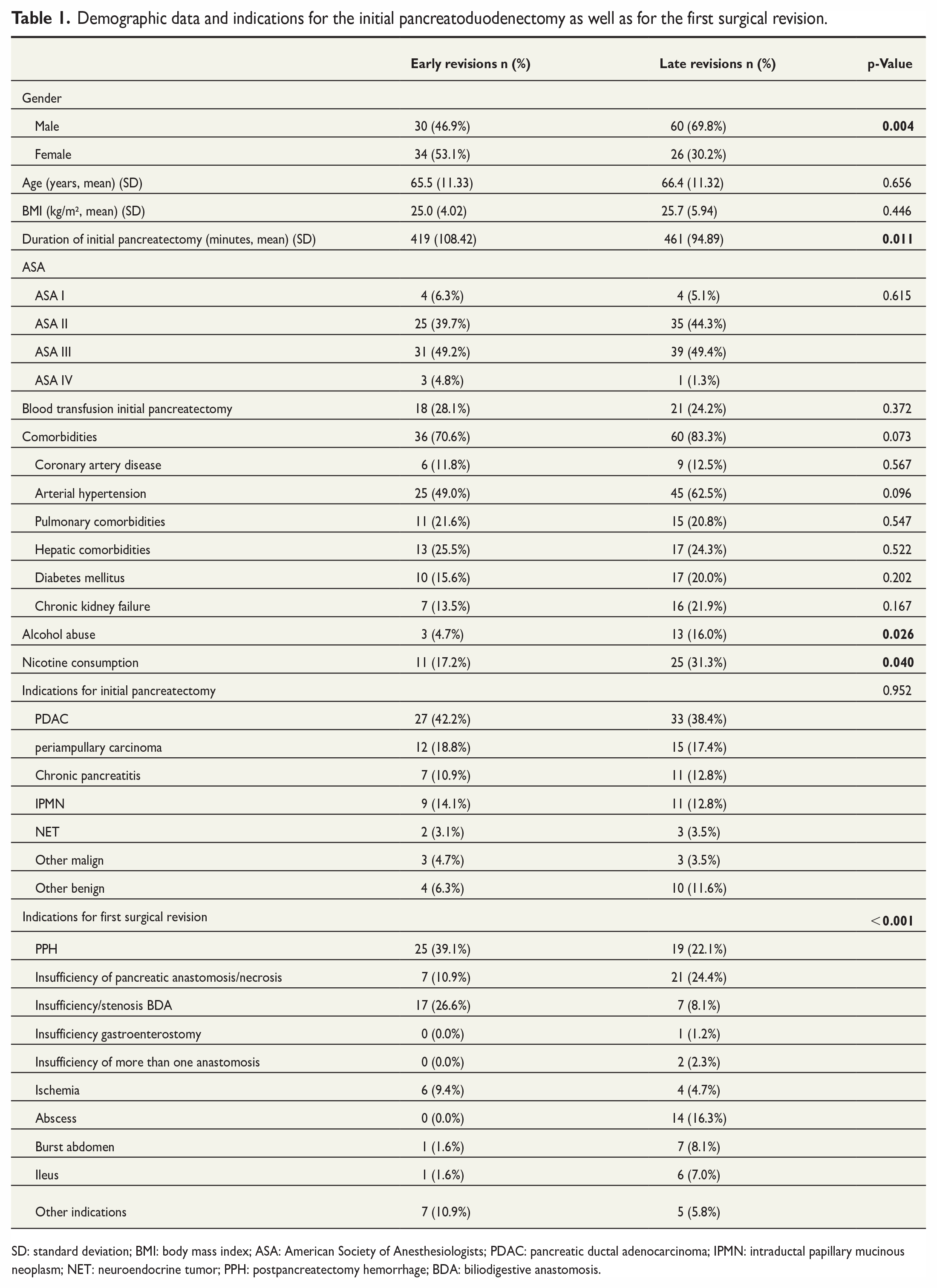
SD: standard deviation; BMI: body mass index; ASA: American Society of Anesthesiologists; PDAC: pancreatic ductal adenocarcinoma; IPMN: intraductal papillary mucinous neoplasm; NET: neuroendocrine tumor; PPH: postpancreatectomy hemorrhage; BDA: biliodigestive anastomosis.
Indications for the first surgical revision
Indications for the first surgical revision following pancreatoduodenectomy included PPH (29.3%), insufficiencies of pancreatoenteric anastomosis (pancreaticojejunostomy (PJ) or pancreatogastrostomy (PG)) in terms of type C pancreatic fistula or necrosis of pancreas remnant (18.7%), insufficiency or stenosis of the biliodigestive anastomosis (16.0%), insufficiency of gastroenterostomy (0.7%), insufficiencies of more than 1 anastomosis (0.7%), bowel ischemia (6.7%), intraabdominal abscesses (9.3%), burst abdomen (5.3%), ileus (4.7%), and others (8.0%) (Table 1). Indications for the first surgical revision after pancreatoduodenectomy were different between both groups with PPH and insufficiencies of biliodigestive anastomoses representing the majority of indications in the early revision group, whereas insufficiencies of pancreatoenteric anastomosis including necrosis of pancreas remnant, PPH, and abscesses were the major reasons for relaparotomy in the late revision group (p < 0.001) (Table 1).
Comparison of complications between early and late revisions
Comparing patients with early revisions with patients who underwent a late revision, we could not find any difference concerning wound infections (43.8% versus 54.1%, p = 0.138), DGE (41.9% early revision versus 29.3% late revisions, p = 0.080), postsurgical cholangitis (1.6% versus 3.5%, p = 0.423), postoperative pneumonia (15.6% versus 19.8%, p = 0.333), and thromboembolism (6.3% versus 11.6%, p = 0.203). Interestingly, we could find significantly more cases of postoperative sepsis in the late revision group (31.4% versus 15.6% in the early group, p = 0.020) and a trend toward a higher rate of acute kidney failure in patients with late revisions (19.8% late versus 9.4% early, p = 0.062). Moreover, more than a third (33.7%) of patients with late revisions needed a reintubation due to respiratory failure, whereas only 18.8% in the early revision group suffered from severe respiratory failure requiring a reintubation (p = 0.031) (Table 2).
Complications and length of hospital stay in patients requiring surgical revisions after pancreatoduodenectomies.
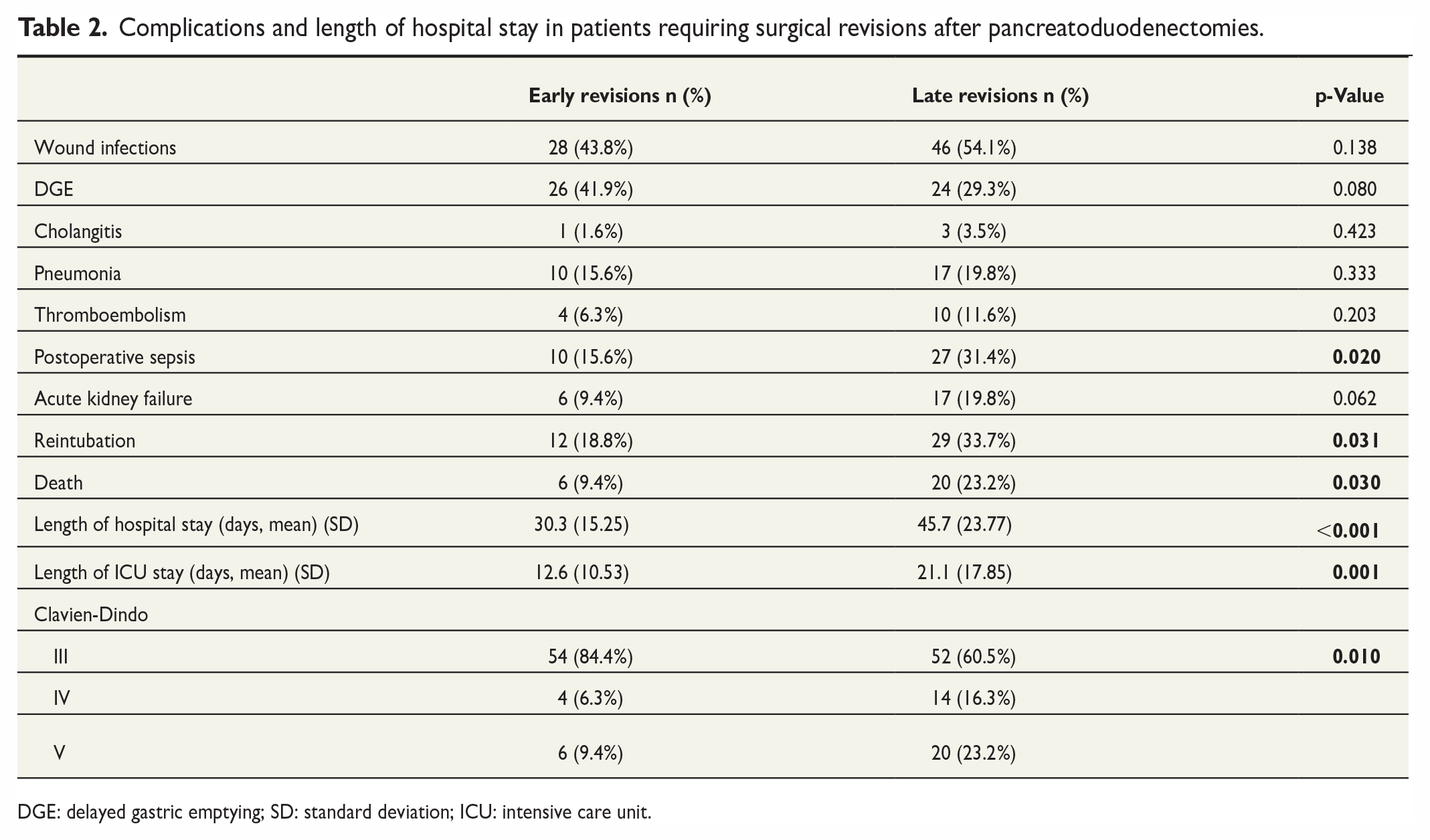
DGE: delayed gastric emptying; SD: standard deviation; ICU: intensive care unit.
Severity of complications and postoperative mortality
With regard to the severity of postoperative complications according to the Clavien-Dindo classification, we found significantly more severe complications (Clavien-Dindo grade IV or V) in patients with late revisions whereas patients with early revisions mainly range within grade III complications (p = 0.010) (Table 2). Concerning postoperative mortality, we could show a significant disadvantage in the late revision group with 23.2% of patients dying following surgery, whereas only 9.4% of patients in the early revision group died during the postoperative course (p = 0.030) (Table 2).
Surgical approach in case of insufficiencies of pancreatoenteric anastomosis or necrosis of pancreas remnant
In our patient collective, we found 28 patients who required a surgical revision due to complications concerning pancreatoenteric anastomosis resulting in a clinically relevant pancreatic fistula. Adding the patients who needed a surgical revision due to PPH caused by vessel erosion as a consequence of severe pancreatic fistula, there were altogether 43 patients with revision surgery due to complications concerning pancreatoenteric anastomosis. These patients were overrepresented in the late revision group with 35 patients (81.4%) belonging to the latter. We analyzed these patients with regard to the technique of surgical reintervention. In the early revision group, 37.5% of patients were treated by transformation of the insufficient PJ in a PG or by pancreatectomy of the pancreas remnant, respectively. One patient received a new formation of PG and another patient in the early group was treated by lavage and drainage. Among patients with late revisions, however, more than half of patients (54.3%) needed a salvage pancreatectomy, and only 11.4% received a conversion from PJ to PG. Almost a third (31.4%) of patients in the late revision group were surgically treated with lavage and drainage and again 1 patient received a new formation of PG. In this small collective of patients requiring surgical revisions due to severe problems concerning pancreatoenteric anastomosis, we observed a trend toward a higher rate of pancreatectomies in the late revision group (p = 0.157). Data concerning operative techniques are shown in Table 3. Analyzing overall complications in this small cohort, we could find significantly more respiratory insufficiencies requiring reintubation (60.0% versus 12.5%, p = 0.019) and a significantly higher rate of acute kidney failure (37.1% versus 0.0%, p = 0.040) in the late revision group, indicating multiorgan failure in patients with late revisions concerning complications following pancreatic fistula. As expected, there is a trend toward a higher postoperative mortality in patients with late revision concerning complications of pancreatoenteric anastomosis, but without reaching statistical significance in this smaller number of patients (p = 0.088) (Table 4).
Surgical approach in of insufficiencies of pancreatoenteric anastomosis or necrosis of pancreas remnant.
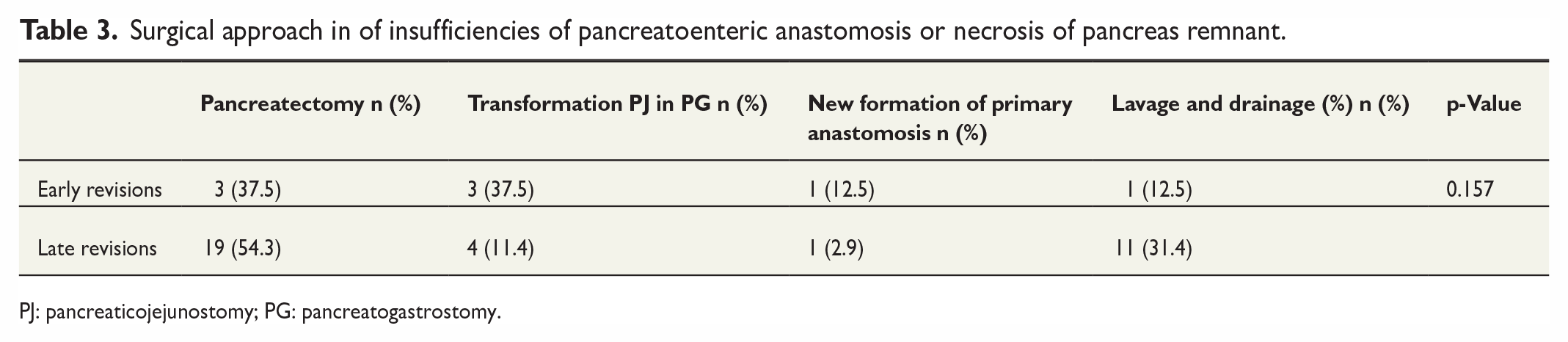
PJ: pancreaticojejunostomy; PG: pancreatogastrostomy.
Complications and length of hospital stay in patients with complications concerning pancreatoenteric anastomosis.
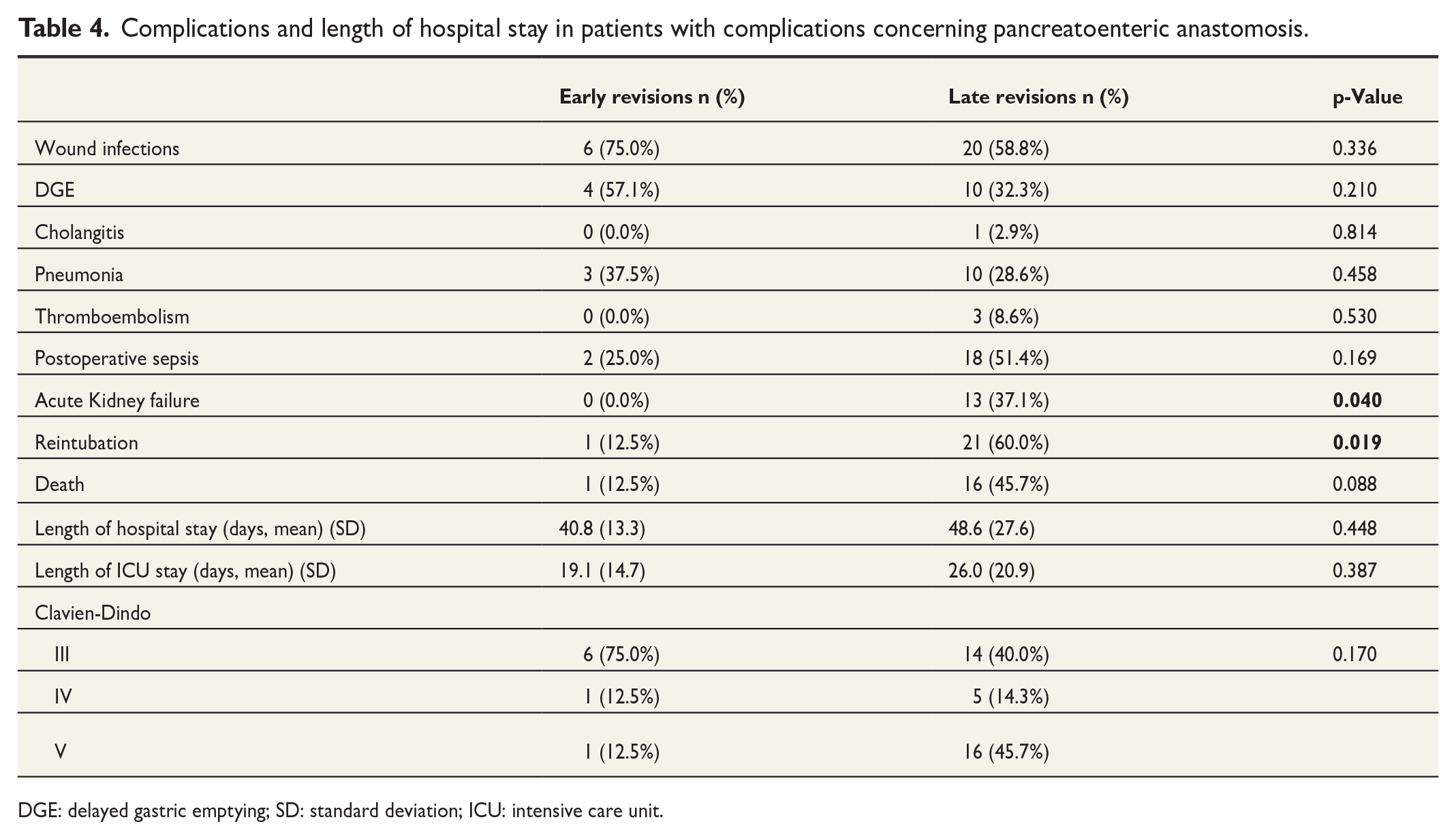
DGE: delayed gastric emptying; SD: standard deviation; ICU: intensive care unit.
In order to identify the patients who develop a clinically relevant pancreatic fistula requiring revision surgery in advance, we performed an analysis of the levels of amylase in (routinely placed) drains in the first PODs. All patients in the early revision group showed an elevated amylase level in the drainage on POD 1–3, whereas only 28 of the 35 patients (80%) were in the late revision group. In the 20% of patients in the late revision group who developed severe complications following pancreatic fistula in the further postoperative course, but without initial signs of a pancreatic fistula, we were not able to predict a complicated pancreatic fistula, possibly due to insufficient peripancreatic drainage. For the remaining 80% of patients with an initial fistula, we were not able to define early postoperative signs of later complications, since BMI and other laboratory results were distributed equally between both groups. What we observed, however, is that the patients having received an early revision due to severe pancreatic fistula during the first 5 PODs are characterized by significantly higher levels of amylase in drains during PODs 1–3 (Table 5).
Initial elevation of amylase postoperatively and level of amylase in drains on days 1 – 3 in patients developing complications concerning pancreatoenteric anastomosis.
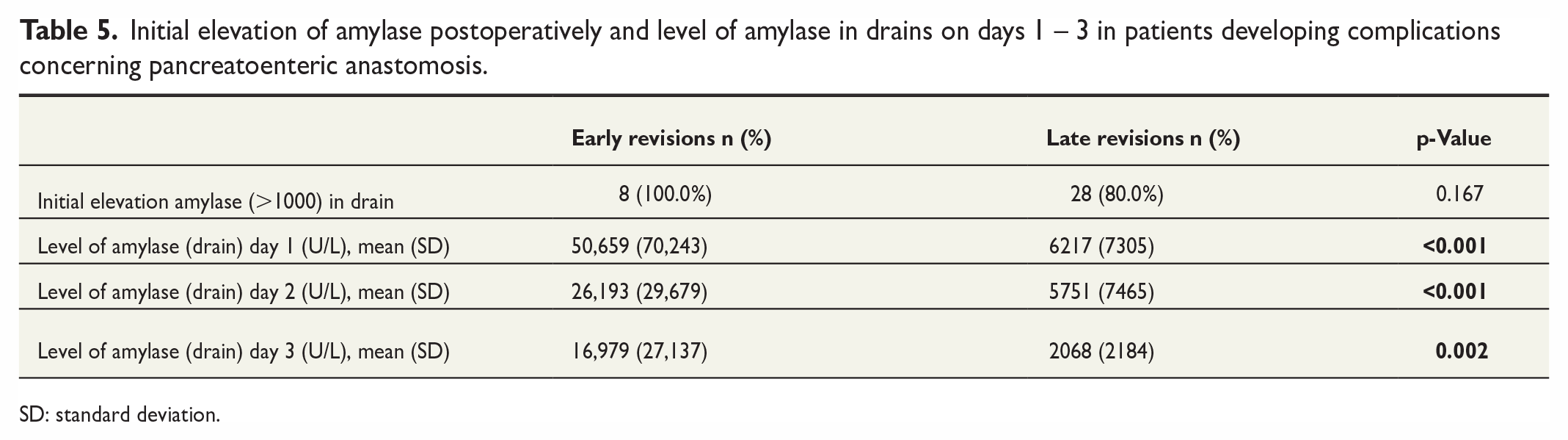
SD: standard deviation.
Length of hospital stay and survival analysis
As expected, the length of hospital stay was significantly longer in patients requiring late surgical revisions (45.7 days) compared with those with early revisions (30.3 days, p < 0.001) (Fig. 1A). The same applies for the length of stay at the intensive care unit (ICU). Patients with late revisions had to spend in medium 21.1 days at the ICU, whereas patients with early revisions only needed 12.6 days of intensive care treatment or surveillance (p = 0.001) (Fig. 1B).
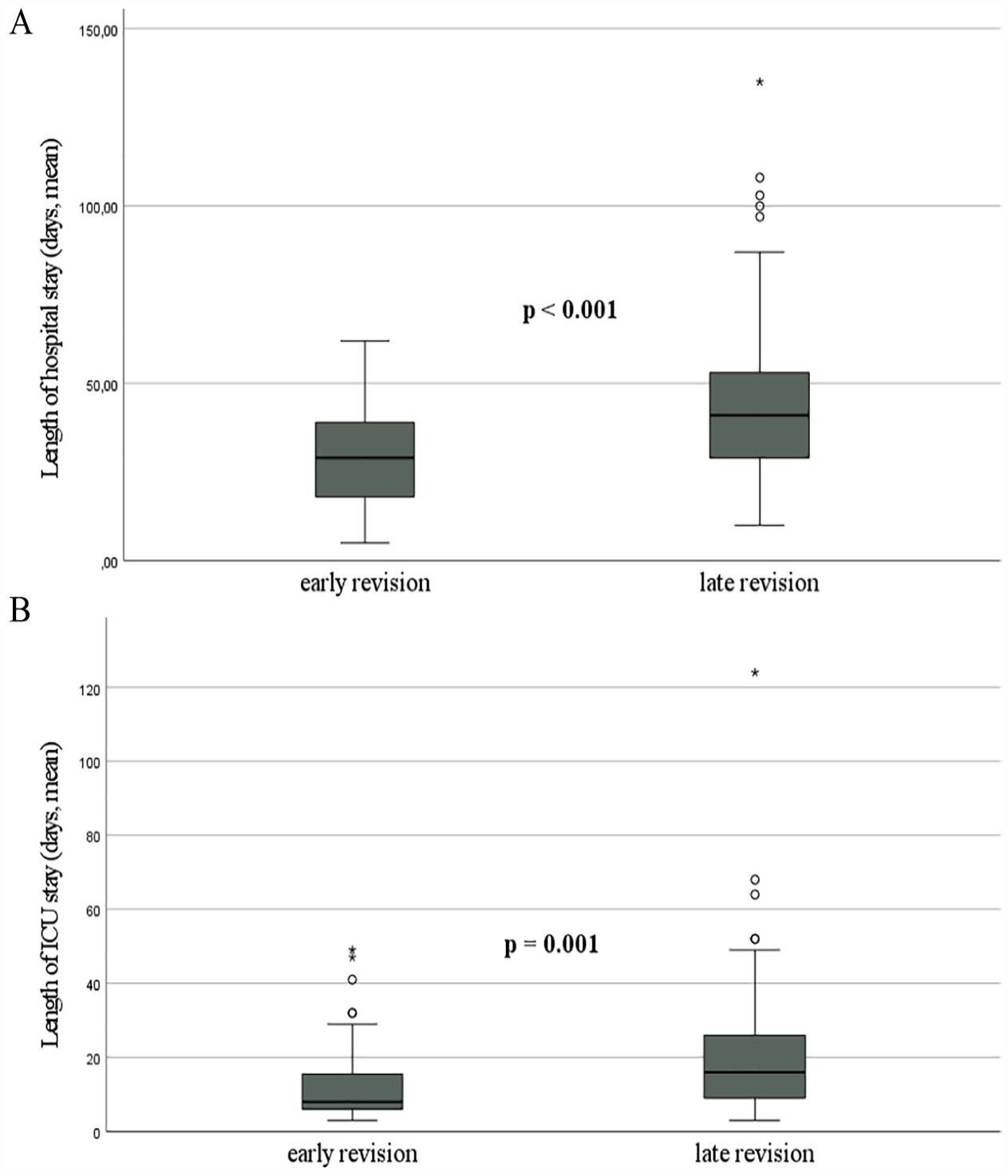
(A) Length of hospital stay and (B) length of ICU stay (entire collective).
Late revisions were also associated with a trend toward reduced overall survival, but without reaching statistical significance (p = 0.153) (Fig. 2A). Considering only patients with insufficiencies of pancreatoenteric anastomosis including late PPH, there was also a trend toward a reduced survival in the late revision group (p = 0.263) (Fig. 2B) not reaching significance due to the small number of patients.
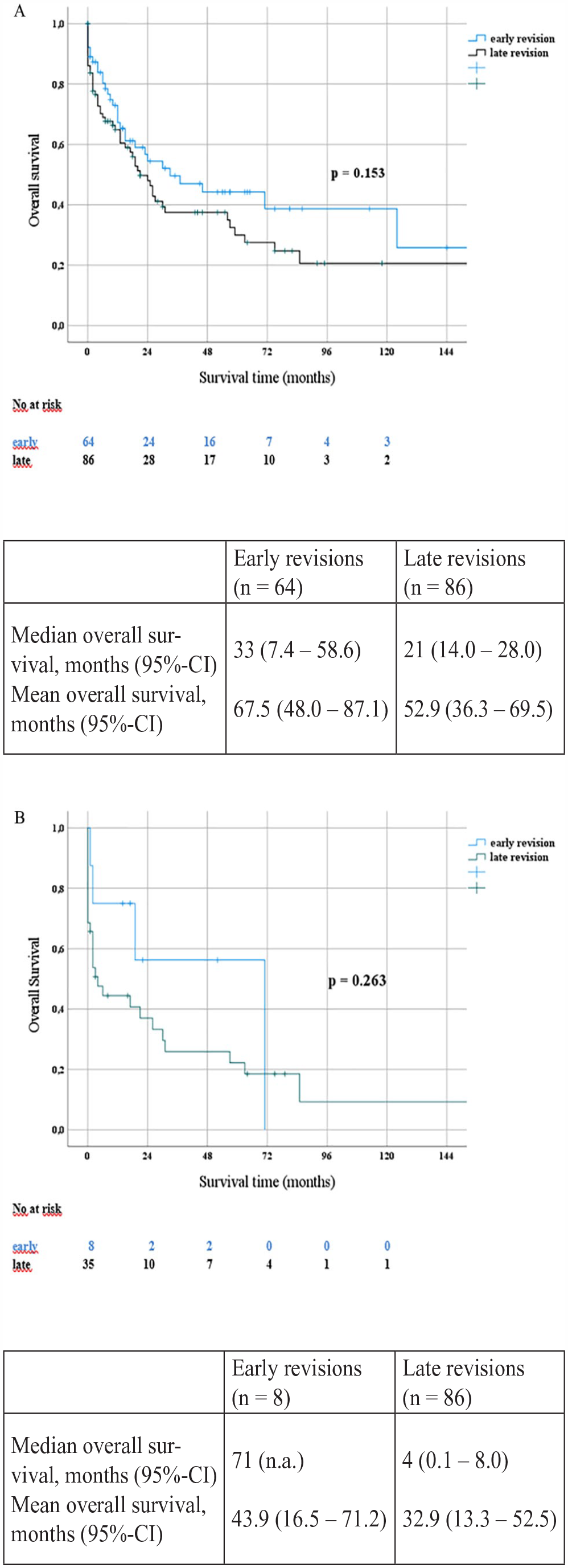
Kaplan–Meier curves overall survival. (A) Entire collective. (B) Patients with complications concerning pancreatoenteric anastomosis (including PPH based on pancreatic fistula).
Discussion
Pancreatoduodenectomies still belong to the most complex surgical procedures in visceral surgery, associated with an increased rate of postoperative morbidity and mortality. Especially insufficiencies of biliary anastomosis, PPH, and type C pancreatic fistulas require a revision.1,3,4,21 In recent years, interventional techniques such as angiography or endoscopy gained more and more importance in the management of complications after pancreatoduodenectomies.6,22 However, there are still severe complications or conditions like hemodynamic instability that require further and immediate surgical treatment.7–9,23 One of the most challenging decisions in pancreatic surgery is to decide to surgically revise and to define the ideal time point for revision surgery.
In our cohort, we found evidence for a significantly worse outcome in patients with revisions past the fifth POD. This is in line with a retrospective analysis of patients requiring relaparotomy due to pancreatic fistula, which showed that timely reintervention was essential to reduce postoperative mortality following reoperation after pancreatoduodenectomy. 24 In this cohort, the main factor predictive of death was the presence of organ failure on the day of relaparotomy. These results emphasize the need for an intense clinical monitoring of these patients and for early surgical revision if there are signs of imminent organ failure. Another group demonstrated that there was a notable shift to interventional techniques especially in the treatment of PJ leakage and late PPH, but that hemodynamic instability and early sepsis still are strong arguments for prompt revision surgery. 25 Failure of non-operative management requiring a surgical reintervention led to an increased mortality risk in this study. As a consequence, especially critically ill patients or patients with special risk factors should be screened carefully for the need of early surgical revision in order to prevent a higher mortality rate due to delayed relaparotomy. In a multicenter retrospective propensity score analysis from the Netherlands, relaparotomy versus interventional drainage of the clinically relevant pancreatic fistula was compared concerning in-hospital mortality and new-onset organ failure. 26 It could be shown that the rates of mortality and organ failure were significantly lower in the drainage group. However, in this study, relaparotomy and interventional drainage were performed quite late, namely, after a median of 8 (primary relaparotomy) or 9 days (drainage) following initial surgery and in patients with accessible fluid collections demonstrating the need for sufficient drainage of fluid collections.
In our patient cohort, PPH is the leading cause of relaparotomy in patients with early revisions and the second most frequent cause in those with late revisions. However, concerning PPH, early and late hemorrhage has to be regarded as separated from each other. Early hemorrhage after pancreatoduodenectomy (generally within the first 24 h after the initial pancreatic resection) is often caused by insufficient hemostasis or coagulopathy and is normally addressed by relaparotomy, whereas late PPH is the result of a complex multifactorial mechanism involving other pancreas-specific complications such as pancreatic fistula or bile leaks in which pancreas fluid or bile leads to a secondary erosion of blood vessels.13,18 Patients with early hemorrhage within 24 h after the initial surgery are normally still in a good condition without any signs of sepsis or organ failure and therefore often show a satisfying outcome following relaparotomy. For late PPH, an endovascular approach is the common strategy of treatment which offers the most promising results. A recent review could show a lower mortality risk for an endovascular approach compared with relaparotomy or endoscopy. 13 However, in hemodynamic instability or after failure of the angiographic approach, there is the need for relaparotomy. At the time of revision surgery, most of these patients suffer from skeptical complications or (multi)organ failure, explaining the worsened outcome after surgical revisions in patients with late PPH compared to early bleedings. This is consistent with the findings in our patient cohort with early revisions carried out mostly due to surgical bleedings, whereas late revisions due to PPH were emergency surgeries in case of erosion bleedings after failing of interventional therapies. Yekebas et al. 27 already described in 2007 in their patient collective a high association of poor outcomes in patients with PPH in cases of an accompanying pancreatic fistula and in the case of late hemorrhage after the fifth POD.
Interestingly, 80% of the clinically relevant pancreatic fistulas causing further complications in our late revision patients already were detectable during the first PODs. Unfortunately, in our patient collective, we were not able to identify further factors at this time that were indicating an adverse outcome. As a consequence, the surgeon’s expertise remains exceptionally important when it comes to make decisions toward relaparotomies.
This study has some limitations. First, it is a retrospective analysis of relaparotomies after initial pancreatoduodenectomy. However, a prospective study in this setting might be challenging, as most of the relaparotomies are performed as emergency surgeries without the time and often without cardiorespiratory stable and competent patients to be included in a study. Second, in our collective of patients, the rate of reoperations seems rather high at 14%, which is, however, in the range of other published series that report reoperation rates between 5.5% and 11.0% in older series28,29 up to 19.8% in a recently published study. 30 Unfortunately, especially for the early years of our patient collective, we do not have complete data sets of all patients concerning the softness of the pancreatic tissue and width of the pancreatic duct, but we could identify a soft pancreatic texture in about 40% of our patients and at least 16% of our patients had a so-called risky pancreas, that is, a soft pancreatic texture associated with a small pancreatic duct. Moreover, one reason for our rather high rate of relaparotomies might be our hospital standard with a proactive and early surgical approach of postoperative complications in order to prevent further complications whereas some of these complications, for example, bile leaks, may have been treated conservatively as well.
Third, our analysis covers more than 10 years in which there were some changes in the management of surgical complications after pancreatoduodenectomies with interventional techniques becoming more and more important. Nevertheless, when interventional drains or angiography fail to resolve the problem, a surgical approach in terms of a relaparotomy still is the required treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.