
Abstract
Background and Aims:
In spite of huge developments in liver surgery during the last decades, morbidity and mortality continue to pose problems in this field. The aim of this study was to identify preoperative predictors for postoperative mortality and morbidity in liver surgery.
Material and Methods:
In a single-center study, an extensive analysis of a prospective database, including clinical criteria and laboratory tests of patients undergoing liver surgery between July 2007 and July 2012 was performed. Cutoff values of selected laboratory tests were calculated.
Results:
In all, 337 patients were included in the study. Univariate analysis showed a statistically significant association of preoperative bilirubin, lactate, hemoglobin levels, platelet count, and prothrombin time with postoperative morbidity and mortality. Multivariate analysis revealed preoperatively elevated serum bilirubin and lactate levels as independent predictors for increased postoperative morbidity and mortality after liver surgery.
Conclusions:
The identified laboratory values showed a statistically significant association with postoperative morbidity and mortality in liver surgery and might be helpful in preoperative patient selection.
Keywords
Introduction
Improvements in liver surgery have resulted in remarkable reductions in mortality and morbidity over the last few decades. Due to the rapid development of liver dissection techniques, as well as improvements in anesthetics, the reported mortality rate of 50% for major liver resection in the 1970s has decreased dramatically (1). Even though the mortality rate is nowadays less than 5%, morbidity rates of up to 40% are still reported (2). Primarily, bleeding and biliary complications, as well as infections, are clinically the most serious problems (3). The high morbidity rates are explained by the rising numbers of liver resections due to the higher incidence of liver tumors (especially metastasis) and the increased percentage of extended resections (4). Moreover, patients undergoing liver surgery are increasingly older and present with more co-morbidity (5). Different studies in the literature discuss possible risk factors with regard to the outcome after liver surgery. Some authors analyzed factors influencing short-term outcome, while others focused on long-term survival, especially in cancer patients (6, 7). It has been shown that postoperative morbidity has an additional impact on the long-term and disease-free survival in cancer patients, and that the reduction of perioperative morbidity can also improve the oncological outcome of curative resection (7, 8). According to the literature, some risk factors for postoperative morbidity and mortality are defined, for example, higher ASA (American Society of Anesthesiologists) classification, steatohepatitis, liver cirrhosis, extent of resection, operating time, need for transfusions, and selected laboratory tests (9 –13). Many groups have analyzed defined subgroups of patients with specific malignancies (hepatocellular carcinoma, colorectal liver metastases), or underlying liver disease like liver cirrhosis (14). The majority of studies focus on intra- and postoperative risk factors of liver surgery. Only a few groups have analyzed preoperative parameters to predict postoperative mortality and morbidity (11).
The aim of this single-center study was to define predictors that help to identify preoperatively patients at risk for increased postoperative morbidity and mortality in liver surgery.
Methods
Patients
In this single-center study, patients’ data from July 2007 to July 2012 were prospectively recorded in an electronic database. Patients who received liver resections simultaneously with another operation such as colorectal resection, gastrectomy, esophagectomy, or pancreatectomy were excluded from the analysis, as were atypical liver resections during explorative laparotomy/laparoscopy and “secondary” liver resections. In all, 337 patients met inclusion criteria and were finally included in the database analysis.
Patient characteristics, pre- and postoperative treatment, laboratory values, operative procedures, intra- and perioperative data, complications, hospital stay, and others were recorded. Analysis of surgical procedures included anatomical segmentectomies, non-anatomical segmentectomies, right and extended right hemihepatectomies as well as left and extended left hemihepatectomies. It is of note that only non-laparoscopic liver resections were included in this analysis.
The study was performed along the principles of the Declaration of Helsinki and approved by the local ethical committee. A written informed consent of patients was obtained.
Statistical Analysis
Statistical analysis was performed using SPSS software, version 20 (SPSS Inc., Chicago, IL, USA) and R for Statistical Computing (R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics were given by median and range or interquartile range (IQR) for continuous data. The distribution of categorical data was presented in contingency tables showing absolute and relative frequencies. All statistical tests were conducted in an explorative manner on a two-sided 5% (α = 0.05) significance level.
Univariate analysis
Univariate analysis was performed to identify risk factors associated with rates of mortality, re-operation, morbidity, and surgical or medical complications. Mortality was defined as in-hospital mortality or 30-day mortality. Morbidity included surgical and medical complications. Surgical complications were defined as abdominal wall dehiscence, wound infection, intra-abdominal abscess, liver abscess, liver necrosis, liver hematoma, bilioma, icterus, biliary fistula, insufficiency of bile duct anastomosis, ascites, pneumothorax, ischemia, intra-abdominal bleeding, perforation of the gut, and mechanical ileus. Medical complications were defined as aspiration, upper or lower gastro-intestinal (GI)-bleeding, perforation of stomach ulceration, venous thrombosis, lung embolism, pleural effusion, pneumonia, other pulmonary complications, cardiac ischemia, cardiac arrhythmia, other cardiac complications, urinary infection, temporary dialysis, permanent dialysis, cholangitis, sepsis, liver failure, multi-organ failure, seizures, and damage to the central nervous system.
Gender and age were analyzed, as well as patients’ ASA score. Moreover, preoperative clinical symptoms (pain, jaundice, pruritus, bleeding complications, loss of weight, and reduced general condition); medical history, including co-morbidities (such as cardiac, pulmonary or renal diseases, diabetes mellitus, viral hepatitis, autoimmune hepatitis or liver cirrhosis with portal hypertension or cholelithiasis); and long-term medication (diuretics, aspirin, coumarines, vitamin K, oral contraceptives, or immunosuppressants) as well as specific oncological pre-treatments (chemotherapy, radiation, transarterial chemoembolization (TACE), radiofrequency-assisted ablation (RFA), and others) were analyzed in univariate analyses. Univariate analysis of the patient’s blood tests on day 1/0 preoperative to surgery, as well as analysis of intraoperative data (operation time, need of blood transfusion, and extent of liver resections) and postoperative data (need of transfusions, intensive care unit (ICU) stay, and days of mechanical ventilation) was performed.
To investigate the relationship between these potential risk factors and outcome, Mann–Whitney U tests were performed for continuous data and χ2 tests or Fisher’s exact test, depending on the cell counts of the respective contingency tables, for categorical data.
Multivariate analysis
Parameters that showed statistically significant differences in regard to mortality, overall morbidity, surgical complications, medical complications, and re-operations in the univariate analyses were included in a multivariate analysis.
The multivariate analysis was performed by logistic regression models designed with stepwise forward variable selection based on Akaike’s information criterion (AIC). The odds ratio (OR) and corresponding 95% confidence intervals (CIs) are presented for each predictor to quantify its relation to the investigated risks.
Definition of cutoff values
Cutoff values of selected preoperative laboratory tests (hemoglobin, hematocrit, lactate, bilirubin, platelet count) were calculated to define risk groups with maximally divergent risks for surgical or medical complications, morbidity, mortality, or re-operation. Statistical significance of such maximally selected test statistics was assessed in a permutation test framework (15).
A global cutoff value for each of the following laboratory tests was performed: serum hemoglobin, hematocrit, lactate, bilirubin, and platelet count. The global cutoff value was determined for a combined outcome that accounts for any event resulting from mortality, morbidity, surgical complications, medical complications, and re-operation.
Decision trees for preoperative blood tests
Decision trees perform successive binary splits in the selected preoperative laboratory results of lactate and bilirubin to produce risk groups for the outcomes mortality and morbidity (including surgical and medical complications) (15). They can be seen as a multivariate extension of the univariate cutoff determination described in the preceding steps. After the first split is found to separate the patient cohort into a high-risk and a low-risk group, it might be reasonable to divide these subsets even further. If this is the case, additional cutoff values are searched for within each subgroup. The procedure stops when there are no meaningful separations left.
Results
Patients’ Characteristics
Between July 2007 and July 2012, a total of 337 liver resections were finally included in our analysis. Detailed information about the analyzed cohort is shown in Table 1. The overall mortality of the cohort was 3.7%, whereas the overall morbidity was 32.7% with an overall re-operation rate of 8.3%.
Patients’ characteristics.
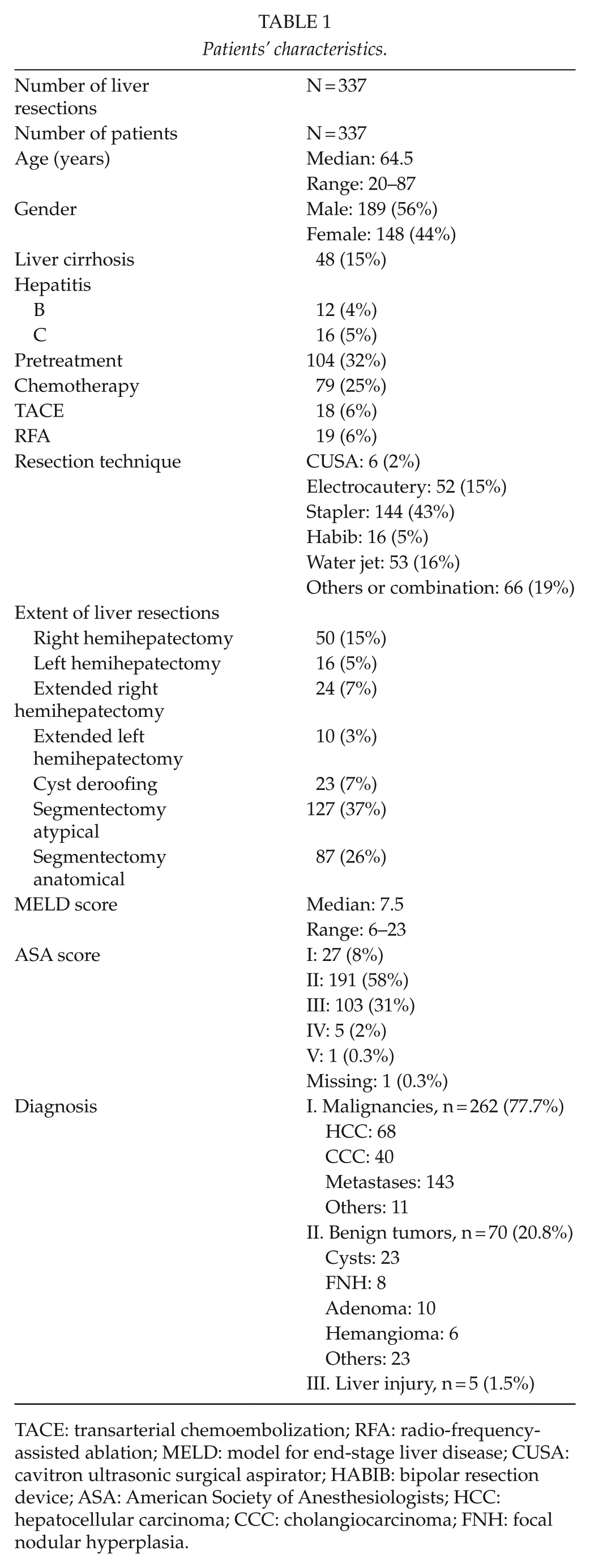
TACE: transarterial chemoembolization; RFA: radio-frequency- assisted ablation; MELD: model for end-stage liver disease; CUSA: cavitron ultrasonic surgical aspirator; HABIB: bipolar resection device; ASA: American Society of Anesthesiologists; HCC: hepatocellular carcinoma; CCC: cholangiocarcinoma; FNH: focal nodular hyperplasia.
Univariate Analysis
Age and gender
The median age was 64.5 years (range: 20–87 years). The cohort consists of 189 male (56%) and 148 female (44%) patients. There were no statistical significant differences in gender and age with regard to mortality, re-operation, and morbidity, surgical or medical complications. Nevertheless, some tendencies were observed: patients with medical complications showed a higher median age of 67.1 years compared to a median age of 63.8 years for patients without medical complications (p = 0.179). Similar results were seen with regard to in-hospital mortality: patients who died within 30 days after surgery showed a median age of 70.7 years (range: 31.5–85.9 years), whereas patients without mortality had a median age of 64.3 years (range: 19.9–86.7 years) (p = 0.198). The group of patients who died consisted of 69% male and 31% female patients. Of note, the mortality rate within the female cohort was 2.7% and within the male cohort 4.8%.
Medical history, long-term medication, pre-treatment, and ASA score
Patients presenting with increased postoperative morbidity had statistically significant more preoperative weight loss (p = 0.049) and blood loss (p = 0.046) had an increased rate of diabetes mellitus (p = 0.034), cardiac disease (p = 0.016), and long-term diuretic medication (p = 0.006), or were pre-treated with TACE (p = 0.019). Cardiac disease (p = 0.001) and long-term medication with aspirin (p = 0.010) and diuretics (p = 0.035) were associated with higher rates of surgical complications, whereas cardiac disease, diabetes mellitus (p = 0.036), liver cirrhosis (p = 0.033), and long-term medication with diuretics (p = 0.001) and preoperative chemotherapy (p = 0.024) were associated with medical complications. The group of patients in need of early re-operation showed a significant higher number of patients with long-term diuretic medication (p = 0.029). Neither medical history and long-term medication nor pre-treatment showed a statistically significant relation to in-hospital mortality.
However, higher ASA score was statistically significant associated with higher postoperative morbidity (p = 0.002) and mortality (p = 0.001) and need for operative revision (p = 0.008).
Preoperative laboratory results
The univariate analysis revealed that preoperative elevated serum lactate and bilirubin levels, as well as preoperative reduced prothrombin time, hemoglobin levels, and platelet count are associated with significantly higher rates of postoperative morbidity (including surgical and medical complications), re-operation, and in-hospital mortality. Detailed results are shown in Table 2.
Univariate analysis of preoperative laboratory tests (day 0) with statistical significance in regard to morbidity, re-operation, and mortality.
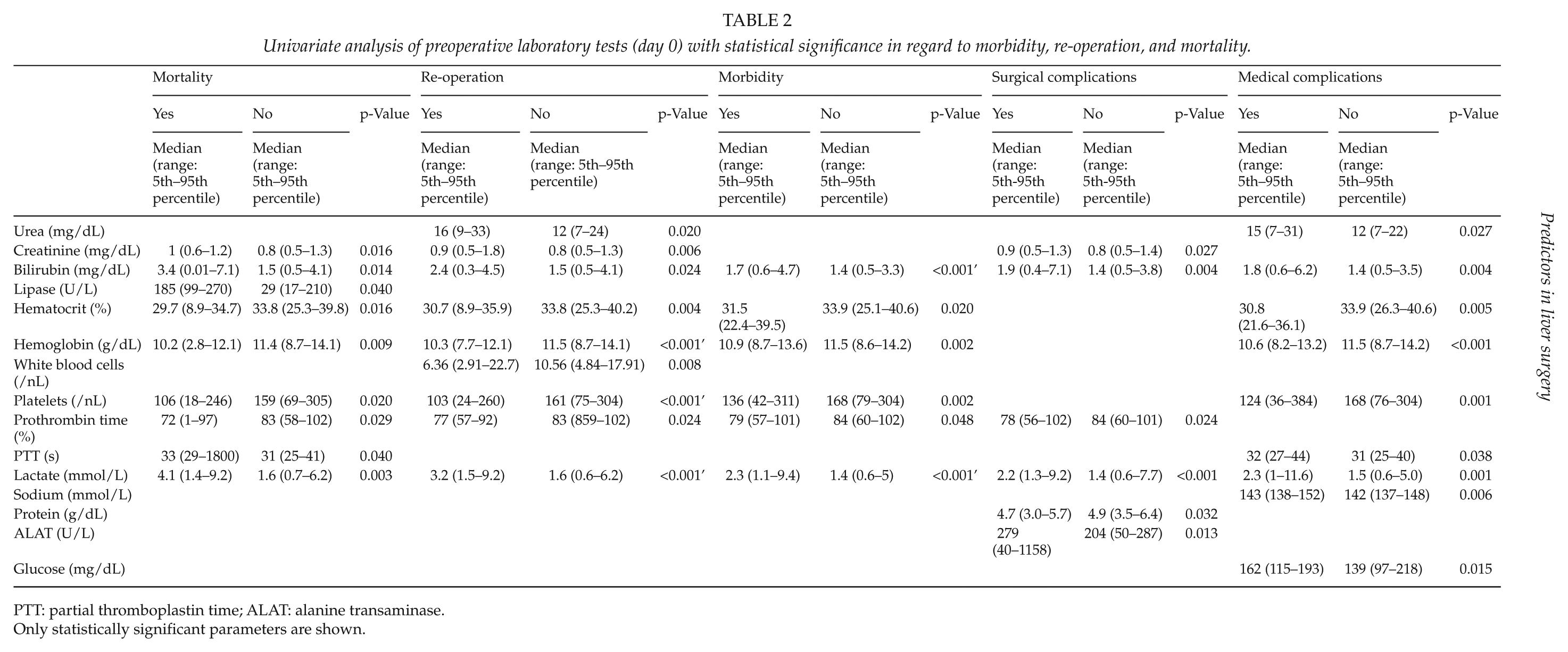
PTT: partial thromboplastin time; ALAT: alanine transaminase.
Only statistically significant parameters are shown.
Intra- and postoperative data
Univariate analysis showed statistically significant differences for morbidity, re-operation, and in-hospital mortality for elevated intra- and postoperative transfusions of packed red blood cells (PRBC) and fresh frozen plasma (FFP), longer operating time, as well as longer ICU stay and longer duration of mechanical ventilation (Table 3). Noteworthy is the fact that postoperative admission to the ICU was a former standard procedure for most patients after liver resections at our hospital.
Univariate analysis of perioperative parameters.
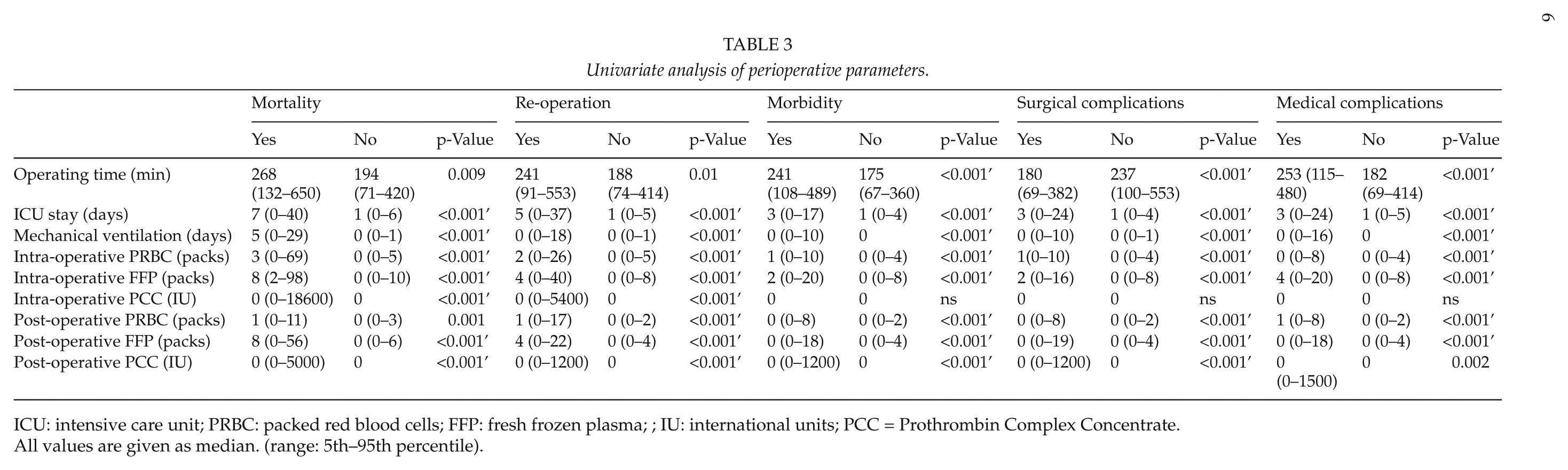
ICU: intensive care unit; PRBC: packed red blood cells; FFP: fresh frozen plasma; ; IU: international units; PCC = Prothrombin Complex Concentrate.
All values are given as median. (range: 5th–95th percentile).
Multivariate Analysis
In the multivariate analysis of preoperative parameters, independent risk factors for in-hospital mortality were preoperatively elevated serum bilirubin (OR: 1.441; 95% CI: 1.097–1.894; p = 0.009) and lactate levels (OR: 1.474; 95% CI: 1.145–1.898; p = 0.004). Regarding independent risk factors for short-term re-operation, the multivariate analysis revealed only preoperatively elevated lactate level (OR: 1.294; 95% CI: 1.116–1.5; p = 0.001), whereas independent risk factors for postoperative morbidity were preoperatively elevated bilirubin (OR: 1.43; 95% CI: 1.107–1.849; p = 0.008) level, preoperatively reduced hematocrit (OR 0.926; 95%CI 0.881–0.974; p = 0.003), and long-term medication with diuretics (OR: 2.054; 95% CI: 1.147–3.676; p = 0.016). More detailed analysis of postoperative morbidity provided preoperatively elevated bilirubin and lactate levels as well as long-term medication with diuretics as independent risk factors, whereas preoperatively reduced hematocrit and sodium levels and long-term medication with diuretics were provided as independent risk factors for non-surgical complications.
Calculated Cutoff Values Of Selected Blood Tests As Preoperative Predictors
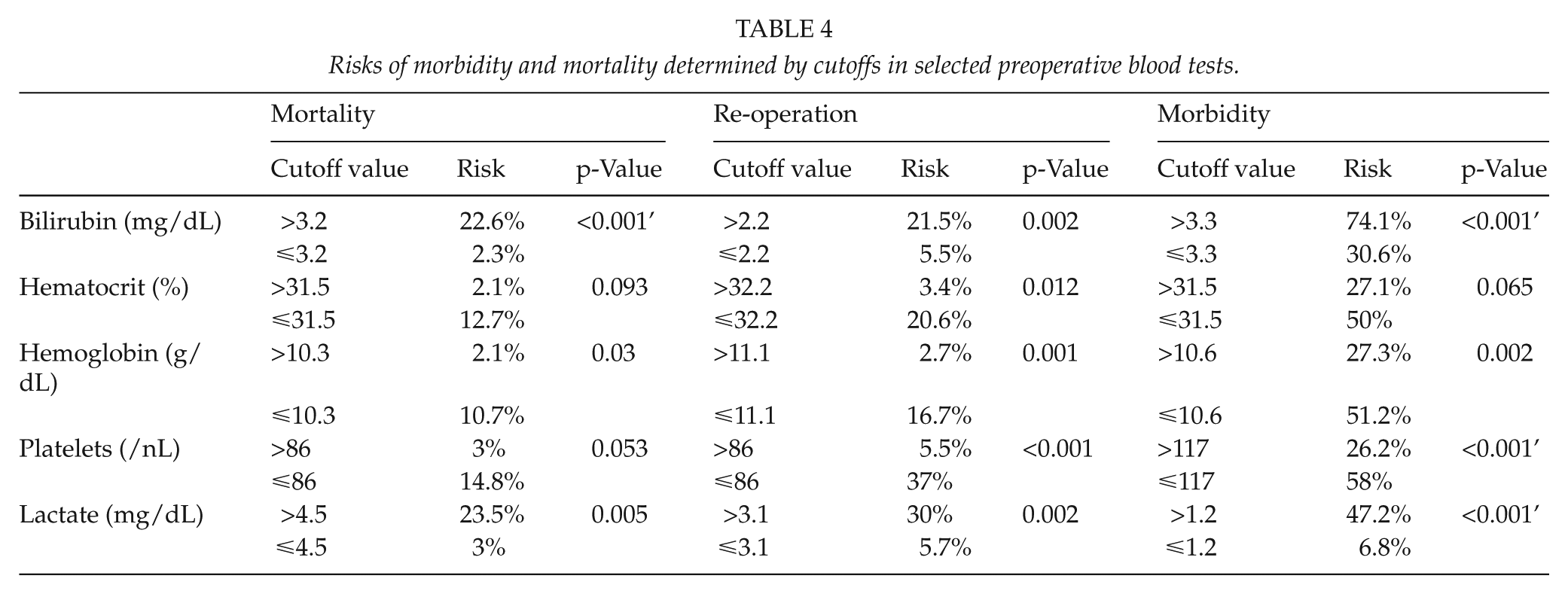
Preoperative serum bilirubin levels >3.2 mg/dL (normal range up to 1.2 mg/dL) were associated with a mortality rate of 22.6%, whereas patients with preoperative serum bilirubin levels ≤3.2 mg/dL had a mortality rate of 2.3% (p < 0.001). The mortality rate was 23.5% in patients presenting preoperatively with serum lactate levels >4.5 mmol/L (normal range up to 1.8 mmol/L) as compared to 3.0% in patients with serum lactate levels ≤4.5 mmol/L (p = 0.005). Another important predictor was the preoperative hemoglobin level; there was a mortality rate of 10.7% in patients with hemoglobin levels ≤10.3 g/dL (normal range 12–16 g/dL) as compared to 2.1% in patients with preoperative hemoglobin level >10.3 g/dL (p = 0.030) (Table 4).
Risks of morbidity and mortality determined by cutoffs in selected preoperative blood tests.
Global cutoff values for preoperative serum levels of bilirubin >3.3 mg/dL (p < 0.001’), of lactate >1.2 mmol/L (p < 0.001’), and preoperative hematocrit levels ≤10.6 g/dL (p = 0.001), preoperative platelet numbers ≤117/nL (p < 0.001’), and hematocrit ≤31.5% (p = 0.037) are associated with a higher combined risk of mortality, morbidity, surgical complications, medical complications, and re-operation.
Decision Trees Based On Selected Blood Tests
The risk for postoperative mortality and morbidity based on the cumulative influence of the preoperative predictors, bilirubin and lactate, can be estimated by decision trees. This multivariate analysis allows the definition of a more diverse set of risk groups compared to the univariate determination of cutoff values (Fig. 1A, B).
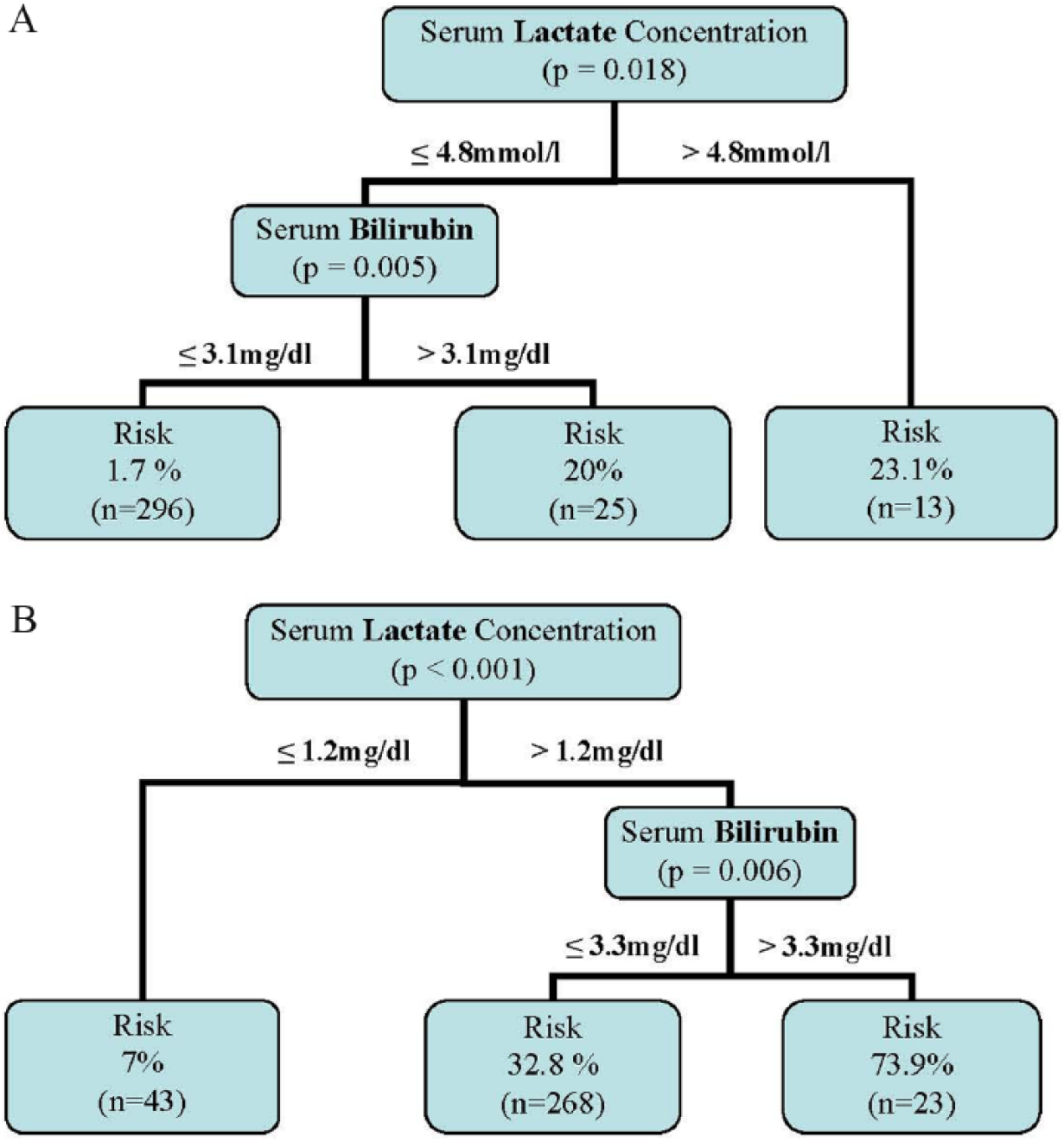
A) Decision tree for in-hospital mortality. Three patients were not included due to incomplete laboratory results at this timepoint. B) Decision tree for postoperative morbidity. Three patients were not included due to incomplete laboratory results at this timepoint.
Discussion
Liver surgery developed dramatically over the last decade due to technical and anesthesiological improvements (2, 16). As a consequence, more extended resections were performed and more co-morbid patients underwent liver surgery, which lead to constantly high morbidity rates. The aim of our study was to identify patients at risk before liver surgery by defining relevant predictors for postoperative morbidity and mortality. One major point of this study was to find easily accessible predictors that are routinely available in most hospitals before liver surgery without the need of additional tests and costs. Based on those parameters, the predictors should support surgeons in patient selection for critical indications. Predictors were revealed by extensive analyses of a single-center electronic database.
After extensive univariate analysis of preoperative laboratory tests, only elevated serum lactate and bilirubin levels as well as reduced hemoglobin/hematocrit levels and reduced prothrombin time and platelet numbers were associated with significantly increased in-hospital mortality and morbidity after liver surgery. More specifically, a multivariate regression model revealed preoperative elevated bilirubin and lactate levels as significant independent predictors for mortality and morbidity.
Bilirubin has been described by several groups as a predictor for liver function in liver surgery. Sitzmann and Greene (17) described bilirubin (but not renal function and medical illness) as a preoperative predictor in liver resections. Bilirubin was also described as a good predictor for liver function in cardiothoracic surgery: patients with chronic congestive heart failure undergoing valve operations show increased hepatic dysfunction, with increased mortality or morbidity, when bilirubin level is elevated or cholinesterase level is reduced preoperatively (18). However, most authors focus on the early postoperative bilirubin concentration to predict the postoperative course and possible liver failure. Balzan et al. (19) postulated the 50/50 rule with increased liver failure for postoperative elevated bilirubin level >50 mmol/L and reduced prothrombin time <50%. The 50/50 rule has been tested and confirmed by other groups in prospective studies (20). Mullen et al. (21) describe cutoffs of postoperative serum bilirubin concentrations of 7 mg/dL and an International Normalized Ratio (INR) of 2 that predict liver-related deaths.
Serum lactate concentration is a valuable predictor for liver function. Some authors described the use of lactate levels to estimate liver function and the regenerative capacity of the liver in the case of acute or chronic liver failure. Bernal et al. (22) used lactate level as a predictor for the outcome of acetaminophen-induced liver failure, whereas another group postulated hyperlactatemia to be a predictor in non-acetaminophen-induced liver failure (23). Macquillan et al. (24) used the combination of serum bilirubin and lactate levels to estimate the outcome in liver failure.
Only one group described the predictive value of postoperative lactate level after liver resection (25). However, to our knowledge, preoperative serum lactate concentration as a predictor for postoperative morbidity and mortality has not been described before.
The preoperative hemoglobin concentration, as well as the number of platelets, also plays an important role for the outcome after liver surgery. It has been described that a postoperatively low platelet count is associated with delayed liver function recovery after a partial liver resection (26).
Different to other studies, parameters for inflammation like C-reactive protein (CRP) or Procalcitonin (PCT) did not have significant relation to the postoperative outcome in our analysis. Furthermore, hypoalbuminemia, alkaline phosphatase, and acute phase proteins that are described to have predictive values did not qualify as predictors in our data (13, 27). In our analysis, neither the univariate nor the multivariate analysis revealed elevated CRP level or hypoalbuminemia as negative predictors for postoperative outcome.
Interestingly co-morbidities were not statistically significant associated with higher postoperative mortality. In contrast, higher ASA scores were significantly associated with higher morbidity and mortality rates. However, postoperative morbidity was higher in patients with long-term medication with diuretics, diabetes mellitus, cardiac disease, or after pre-treatment with TACE. Different from other studies, in this study, liver cirrhosis was neither associated with increased postoperative morbidity nor with mortality.
Differently, Poon et al. (28) did not find a statistically significant correlation between diabetes mellitus and morbidity and mortality after liver surgery. Preoperative chemotherapy is thought by some authors to cause poorer postoperative outcomes (29). Even though some authors have found that chemotherapy within 30 days before liver surgery did not increase postoperative morbidity and mortality, the median level of mortality was higher in the chemotherapy group. It is noteworthy that the time frame between chemotherapy and surgery varied widely in our patients.
Similarly, age and gender do not allow any prediction in regard to postoperative morbidity and mortality after liver surgery. However, male patients tend to have a higher morbidity. Although statistically not significant, higher age (older than 65 years) seems to be associated with higher mortality and morbidity. Wu et al. described a missing statistically significant correlation between age and morbidity/mortality after liver resections, but they showed statistically significant increased morbidity in patients with co-morbidities and higher extent of resections. Of note, these authors found reduced hemoglobin and albumin levels, as well as increased percentage of co-morbidities, in patients older than 65 years (5).
Perioperative parameters as operating time, intra- and postoperative transfusion of blood products, as well as ICU stay and prolonged postoperative mechanical ventilation have high impact on postoperative mortality and morbidity in this study. In detail, the multivariate logistic regression model revealed that only the length of mechanical ventilation and ICU stay are independent risk factors for increased postoperative mortality. Intra- or postoperative transfusion of FFP or PRBC, extended operating time, ICU stay, and mechanical ventilation were independent risk factors for postoperative morbidity or increased re-operation rate.
While the duration of mechanical ventilation and the length of ICU stay are rarely mentioned as independent risk factors for liver surgery outcome, the influence of the extent of resection, blood loss, and operating time on the postoperative situation has already been described by several groups (10). Shiba et al. (30) revealed an increased rate of pulmonary complications for patients who received blood products in hepatic resections for hepatocellular carcinoma. Additionally, early postoperative extubation seems to be associated with faster liver recovery after liver surgery. The positive end-expiratory pressure has eventually a negative impact on the liver function. Intra- and postoperative data might be helpful in estimating the outcome postoperatively, but do not help to predict the risks or to identify high-risk patients preoperatively. However, even though confirmed by other authors, those factors are not applicable as preoperative predictors.
Co-morbidities as well as age and gender were not classified as valuable predictors in our study. Therefore, the calculation specific of cutoff values for preoperative serum bilirubin, lactate, and hemoglobin concentrations and preoperative platelet count for predicting the risk of postoperative morbidity, re-operation rate, and mortality after liver surgery was performed. In addition, decision trees based on preoperative serum bilirubin and lactate concentrations were designed to preoperatively estimate patients’ postoperative risk.
Comparably, other groups defined cutoffs for laboratory tests for postoperative mortality and morbidity after liver surgery. The French group of Balzan et al. (19) defined a reduced prothrombin time <50% and an elevated serum bilirubin level >50 mmol/L on postoperative days 1–7 as strong predictors for postoperative mortality. Another group similarly focused on a cutoff of serum bilirubin level of 1 mg/dL in combination with special interleukins to be a predictor for postoperative complications (13). Of note is that those scores are based on postoperative tests and are not helpful in predicting preoperative risk. Differently, Breitenstein et al. (11) developed a preoperative scoring system (0–10 points) based on four parameters: ASA score, transaminase levels, extent of liver resection, and the need for an additional hepaticojejunostomy or colon resection. The score was developed for non-cirrhotic patients. Unlike those scores, our risk trees are based on preoperative laboratory results and can be administered to cirrhotic and non-cirrhotic patients. Moreover, unlike the findings of Breitenstein et al., our score is exclusively for hepatic resections and not for other accompanying visceral resections.
Conclusion
In summary, the analysis of patients’ characteristics, clinical history, and long-term medication, as well as intra- and postoperative data and laboratory tests revealed preoperative predictors for morbidity and mortality in liver surgery. While age and gender have no statistically significant association with the postoperative outcome, operating time, perioperative transfusions, length of mechanical ventilation, and ICU stay are risk factors for increased morbidity and mortality after liver surgery. Preoperatively elevated serum bilirubin and lactate levels are independent predictors for increased postoperative morbidity and mortality after liver surgery. The use of decision trees as well as the calculated cutoffs for levels of bilirubin, lactate, hemoglobin, and platelets might be helpful in identifying patients at risk before liver surgery.
Footnotes
Declaration of Conflicting Interests
All named authors hereby declare that they have no conflicts of interest to disclose.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.