
Abstract
Background:
Post-hepatectomy liver failure (PHLF) is the leading cause of postoperative mortality following major liver resection. Between December 2012 and May 2015, 10 consecutive patients with PHLF (according to the Balzan criteria) following major/extended hepatectomy were included in a prospective treatment study with the molecular adsorbent recirculating system (MARS). Sixty- and 90-day mortality rates were 0% and 10%, respectively. Of the nine survivors, four still had liver dysfunction at 90 days postoperatively. One-year overall survival (OS) of the MARS-PHLF cohort was 50%. The present study aims to assess long-term outcome of this cohort compared to a historical control cohort.
Methods:
To compare long-term outcome of the MARS-PHLF treatment cohort with PHLF patients not treated with MARS, the present study includes all 655 patients who underwent major hepatectomy at Karolinska University Hospital between 2010 and 2018. Patients with PHLF were identified according to the Balzan criteria.
Results:
The cohort was split into three time periods: pre-MARS period (n = 192), MARS study period (n = 207), and post-MARS period (n = 256). The 90-day mortality of patients with PHLF was 55% (6/11) in the pre-MARS period, 14% during the MARS study period (2/14), and 50% (3/6) in the post-MARS period (p = 0.084). Median OS (95% confidence interval (CI)) was 37.8 months (29.3–51.7) in the pre-MARS cohort, 57 months (40.7–75.6) in the MARS cohort, and 38.8 months (31.4–51.2) in the post-MARS cohort. The 5-year OS of 10 patients included in the MARS study was 40% and the median survival 11.6 months (95% CI: 3 to not releasable). In contrast, for the remaining 21 patients fulfilling the Balzan criteria during the study period but not treated with MARS, the 5-year OS and median survival were 9.5% and 7.3 months (95% CI, 0.5–25.9), respectively (p = 0.138)).
Conclusions:
MARS treatment may contribute to improved outcome of patients with PHLF. Further studies are needed.
The initial pilot study was registered at ClinicalTrials.gov (NCT03011424).
Keywords
Context and Relevance
Post-hepatectomy liver failure (PHLF) accounts for the majority of 90-day mortality following major hepatectomy. In 2018, a prospective study investigating the safety and feasibility of the molecular adsorbing recirculating system (MARS) in patients fulfilling the 50:50 criteria demonstrated a very low 90-day mortality (1/10 patients). Prospective trials evaluating treatment modalities in PHLF patients are very rare, and until today, long-term results are not available. Hence, the present study reports the 5-year outcome of the MARS study population compared with two historical control cohorts. The results support further treatment studies in PHLF patients and might be useful for the design and power calculation of related studies in the future.
Introduction
Liver surgery is considered a standard and safe procedure in specialized centers with decreasing morbidity and mortality. However, significant differences are observed dependent on the underlying disease and extent of resection.1,2 Of all complications, post-hepatectomy liver failure (PHLF) has been identified as the main cause of postoperative 90-day mortality. 3 The incidence of PHLF is estimated to be 5%–10%. 4 Despite advances in many areas of peri-operative care, there are no other treatment options than medical support for patients with PHLF according to recent recommendations.4,5 Even though there are several reviews available in the literature, evidence-based guidelines for the treatment of PHLF are still lacking. 6
In a previously published prospective safety and feasibility pilot study, we described our experience with early postoperative extracorporeal liver support therapy with the molecular adsorbent recirculating system (MARS) in patients with PHLF. 7 Briefly, the potentially beneficial effects of MARS in PHLF patients are based on its ability to not only remove water-soluble but also albumin-bound toxins along with its potential to positively influence different circulatory parameters in severely ill patients, like increase in the mean arterial pressure and decrease in portal venous pressure gradient.8–10 The study showed early MARS to be safe, with a low 90-day mortality of 10%. Long-term results and effects of MARS treatment on long-term survival, however, have not been evaluated before.
In this study, we evaluate and compare the long-term results of patients with PHLF treated with MARS to patients with PHLF who were not treated with MARS.
Methods
Study design
Patients aged 18 years or older undergoing major hepatectomy (⩾3 Couinaud segments) between 1 January 2010 and 31 December 2018 at Karolinska University Hospital, Stockholm, Sweden, a tertiary referral facility, were eligible for inclusion in the study. Patients with conventional two-stage hepatectomy or pre-operative future-liver remnant augmentation (major hepatectomy following portal venous ligation or embolization) were included, but patients undergoing an associating liver partition and portal vein ligation for staged hepatectomy procedure were excluded (as this was an exclusion criterion for the MARS study).
The entire cohort was divided into three time periods: a pre-MARS period including patients from 1 January 2010 until 30 November 2012, a “MARS-study” period from 1 December 2012 until 31 May 2015 and a “post-MARS” period from 1 June 2015 until 31 December 2018. Data regarding the pre- and post-MARS cohorts were collected retrospectively from the electronic patient folder system. Data for the MARS-study period were collected prospectively. Collected data included demographics, comorbidities, indication for surgery, operative variables, and blood tests, as depicted in Table 1. Postoperative complications were graded according to the Clavien–Dindo classification. 11 Major complications were defined as ⩾Clavien–Dindo 3b. PHLF was graded according to the International Study Group of Liver Surgery (ISGLS) 12 and Balzan criteria. 13 The 90-day mortality rate and overall survival (OS) were compared for the total time period as well as for patients with PHLF treated with MARS and those not treated with MARS.
Peri-operative characteristics including postoperative morbidity and mortality in patients undergoing major hepatectomy pre-MARS, MARS, and post-MARS period.
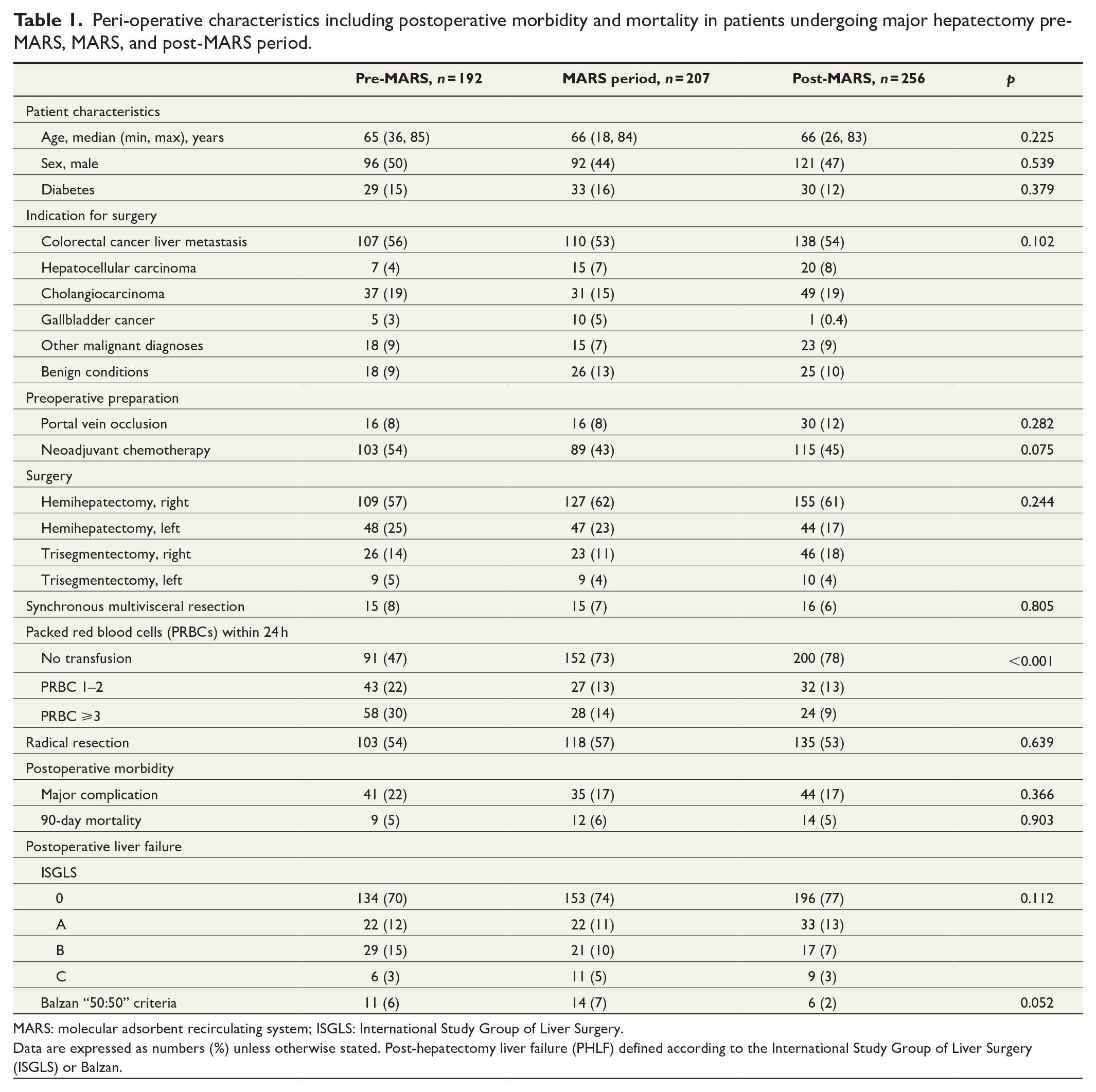
MARS: molecular adsorbent recirculating system; ISGLS: International Study Group of Liver Surgery.
Data are expressed as numbers (%) unless otherwise stated. Post-hepatectomy liver failure (PHLF) defined according to the International Study Group of Liver Surgery (ISGLS) or Balzan.
At Karolinska University Hospital, MARS was used in two PHLF patients in the pre-MARS study period and in three patients in the post-MARS period. In these patients, the indication for MARS treatment was secondary or immediate severe liver failure following hepatectomy and thus they did not meet the Balzan criteria. These patients were included in the pre-MARS and post-MARS cohorts.
MARS study period and ethical approval
The short-term results of the prospective MARS pilot study and a detailed study and treatment plan are reported elsewhere. 7 Briefly, the study aimed to demonstrate safety and feasibility of early postoperative MARS treatment in patients fulfilling the Balzan criteria on postoperative day 5 after major hepatectomy. The study was conducted between 1 December 2012 and 31 May 2015 at Karolinska University Hospital.
Inclusion criteria for MARS were age of 18–80 years and Balzan criteria fulfilled on postoperative day 5 and the willingness and ability to provide informed consent (next of kin was accepted according to the ethical approval). Exclusion criteria for early MARS treatment were age over 80 years, uncontrolled bleeding or sepsis, any relevant and untreated surgical complication such as mechanical bile duct obstruction, hepatic artery, or portal vein thrombosis, and a platelet count of <20 × 109/L.
The study protocol for the prospective MARS pilot study has been approved by the regional ethical board, Stockholm (Dnr 2013/149-31/2) and the present study was approved separately by the national ethical board (Dnr 2020-04493). The initial MARS study was registered at ClinicalTrials.gov (NCT03011424) and performed according to the Helsinki Declaration.
Statistical analysis
Statistical analysis was done using STATA 15.0 (StataCorp, Collage Station, Texas, USA). Categorical data are expressed as frequencies and percentages and compared using Pearson’s chi-square test or Fisher’s exact test. Non-normally distributed continuous data are presented as median values (min, max) and compared using Kruskal–Wallis test. Univariable survival estimates were illustrated with Kaplan–Meier curves and compared using log-rank test. The significance level was set at p < 0.05 and median survival presented with 95% confidence intervals (CIs).
Results
In total, 655 patients were included in the final analysis, 192 patients in the pre-MARS period, 207 in the MARS-study period, and 256 in the post-MARS period. Over the entire study period, 31 patients fulfilled the 50:50 criteria (16 patients classified as ISGLS C, 12 as B, and 3 as A). The groups were similar regarding age, sex, indication for resection, preoperative chemotherapy, preoperative liver volume manipulation, and the extent of resection (Table 1). The need for red blood cell transfusion (⩾3 units packed red blood cells) decreased significantly over the study period, from 30% in the pre-MARS to 9% in the post-MARS period (p < 0.001).
Major complications (⩾Clavien–Dindo 3b), which occurred in 18.3% of all patients, and 90-day mortality (overall 5.3%) were not significantly different between the three defined cohorts. The 90-day mortality of patients with PHLF according to the Balzan criteria was 55% (6/11) in the pre-MARS period, 14% during the MARS study period (2/14), and 50% (3/6) in the post-MARS period (p = 0.084). Patients undergoing major hepatectomy during the MARS study period had significantly better median survival compared to the pre-MARS cohort (57 months (95% CI: 41–76 months) versus 38 months (95% CI: 29–52 months); p = 0.021) but not compared to the post-MARS cohort (39 months (95% CI: 31–51 months); p = 0.067) (Table 2). There was no difference regarding long-term survival between the pre- and post-MARS cohorts (p = 0.902). The Kaplan–Meier estimates displaying long-term survival of these three groups are shown in Fig. 1.
Long-term survival comparing pre-MARS, MARS, and post-MARS patients.

MARS: molecular adsorbent recirculating system; OS: overall survival; CI: confidence interval.
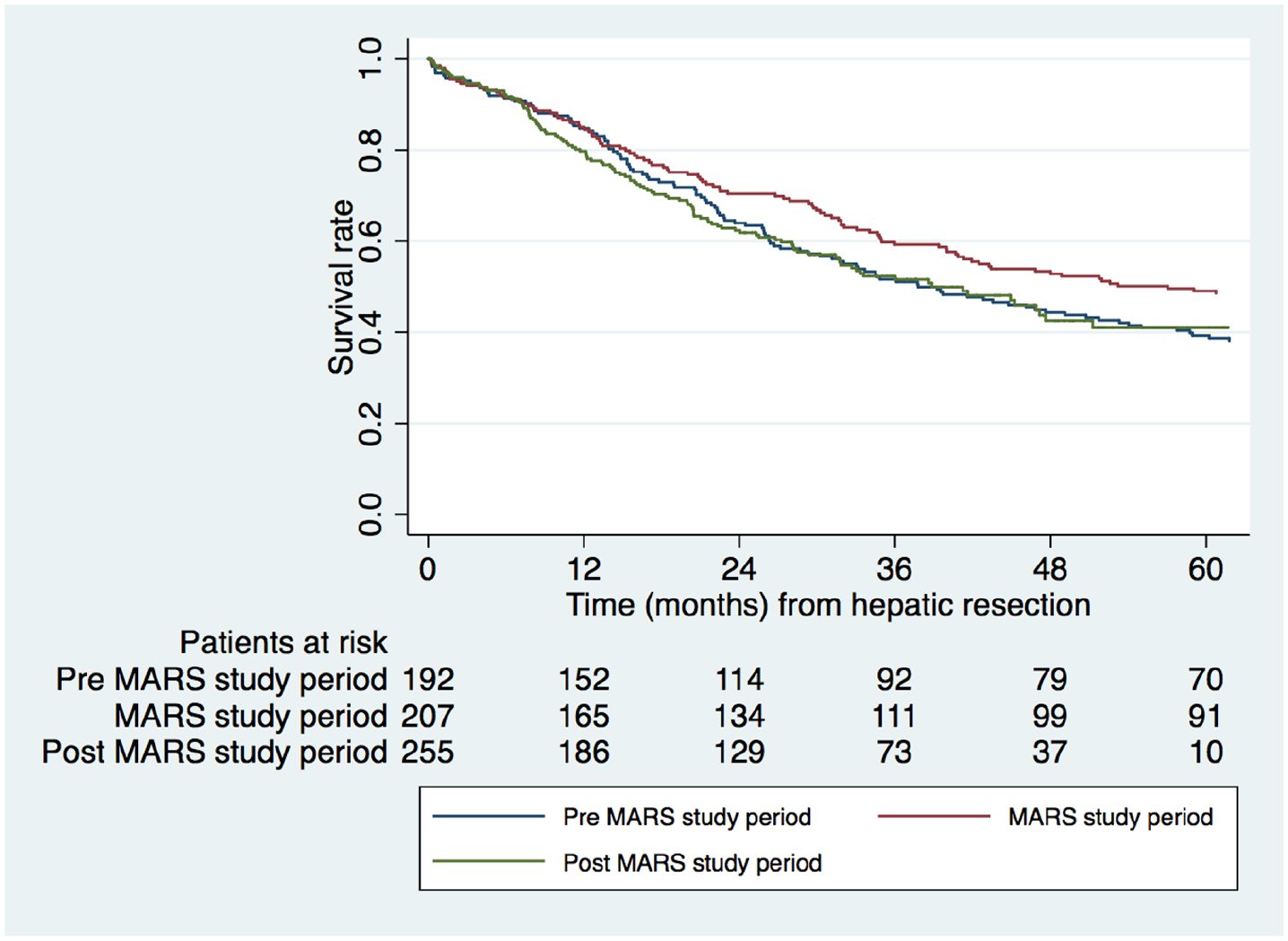
Kaplan–Meier estimates of all patients, stratified for pre-MARS, MARS, and post-MARS period (p = 0.04).
A total of 10 patients were included in the prospective MARS study. The patient selection, treatment, and short-term outcome of this cohort have been described elsewhere. 7 Briefly, the 90-day mortality was 10% and four patients developed a chronic and prolonged liver failure with increasing bilirubin and multiple complications, including sepsis, bleeding episodes due to portal hypertension, and renal failure. Three of these patients had early disease recurrence within 3–4 months after surgery and were treated with palliative intent and survived between 130 and 349 days. Another patient died due to disease recurrence after 18 months, following palliative chemotherapy with normalized liver function. The remaining four patients were alive 5 years post-surgery, and while two were being treated for recurrence, none of them showed signs of impaired liver function.
The 5-year OS and median survival of the 10 patients included in the MARS study were 40% and 12 months (95% CI: 3 to NR), respectively. In contrast, for the remaining 21 patients fulfilling the Balzan criteria but not included in the MARS study, the 5-year OS and median survival were 9.5% and 7 months (95% CI: 0.5–25.9 months), respectively. The difference in OS did not reach significance (p = 0.138). Additional information on all 31 patients with PHLF during the study period is presented in Table 3. The Kaplan–Meier estimates for the assessment of long-term survival comparing all MARS and non-MARS PHLF patients are shown in Fig. 2.
Patients fulfilling Balzan criteria between January 2010 and December 2018, stratified for three time periods (pre-MARS, MARS study, and post-MARS).
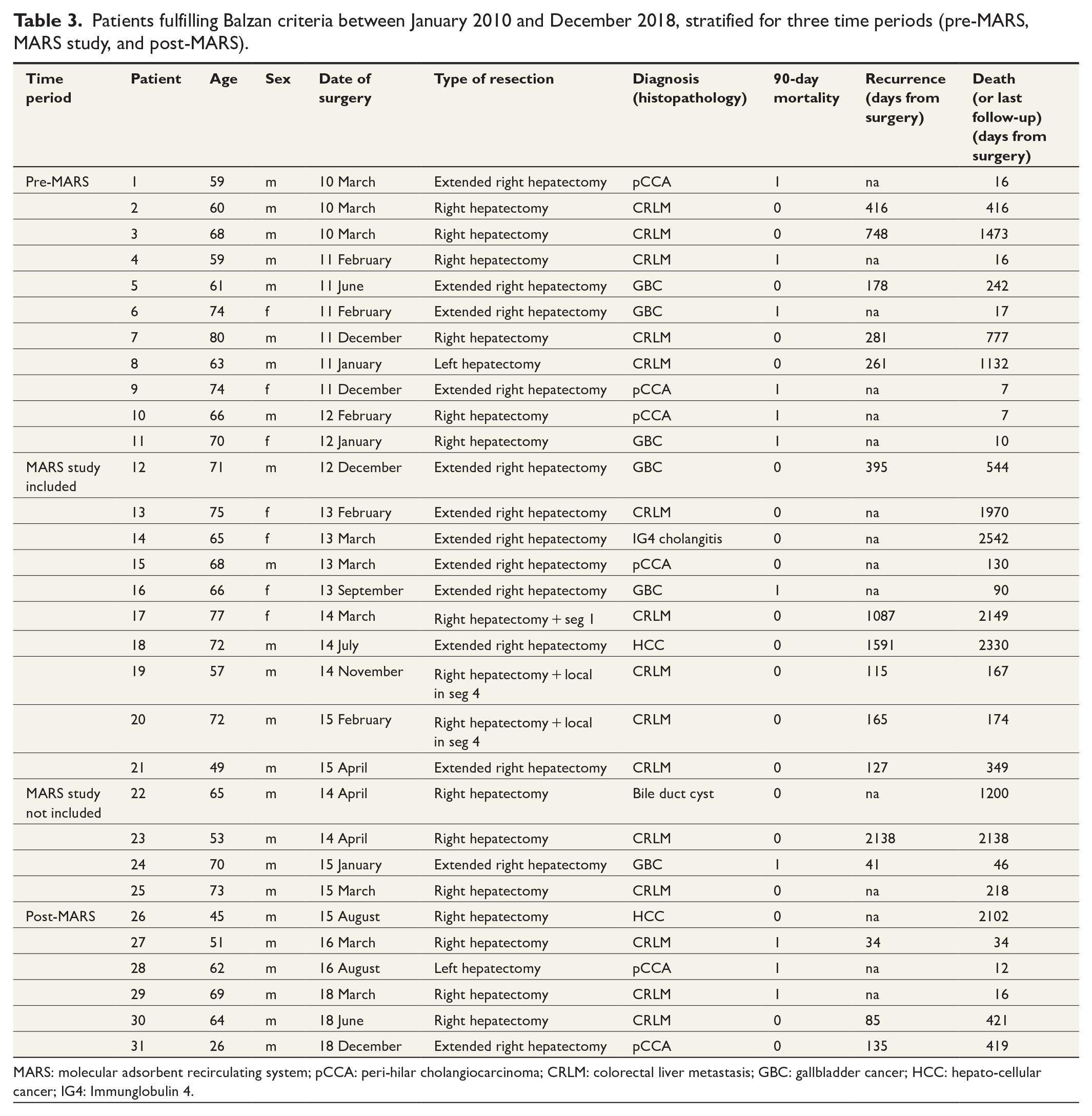
MARS: molecular adsorbent recirculating system; pCCA: peri-hilar cholangiocarcinoma; CRLM: colorectal liver metastasis; GBC: gallbladder cancer; HCC: hepato-cellular cancer; IG4: Immunglobulin 4.
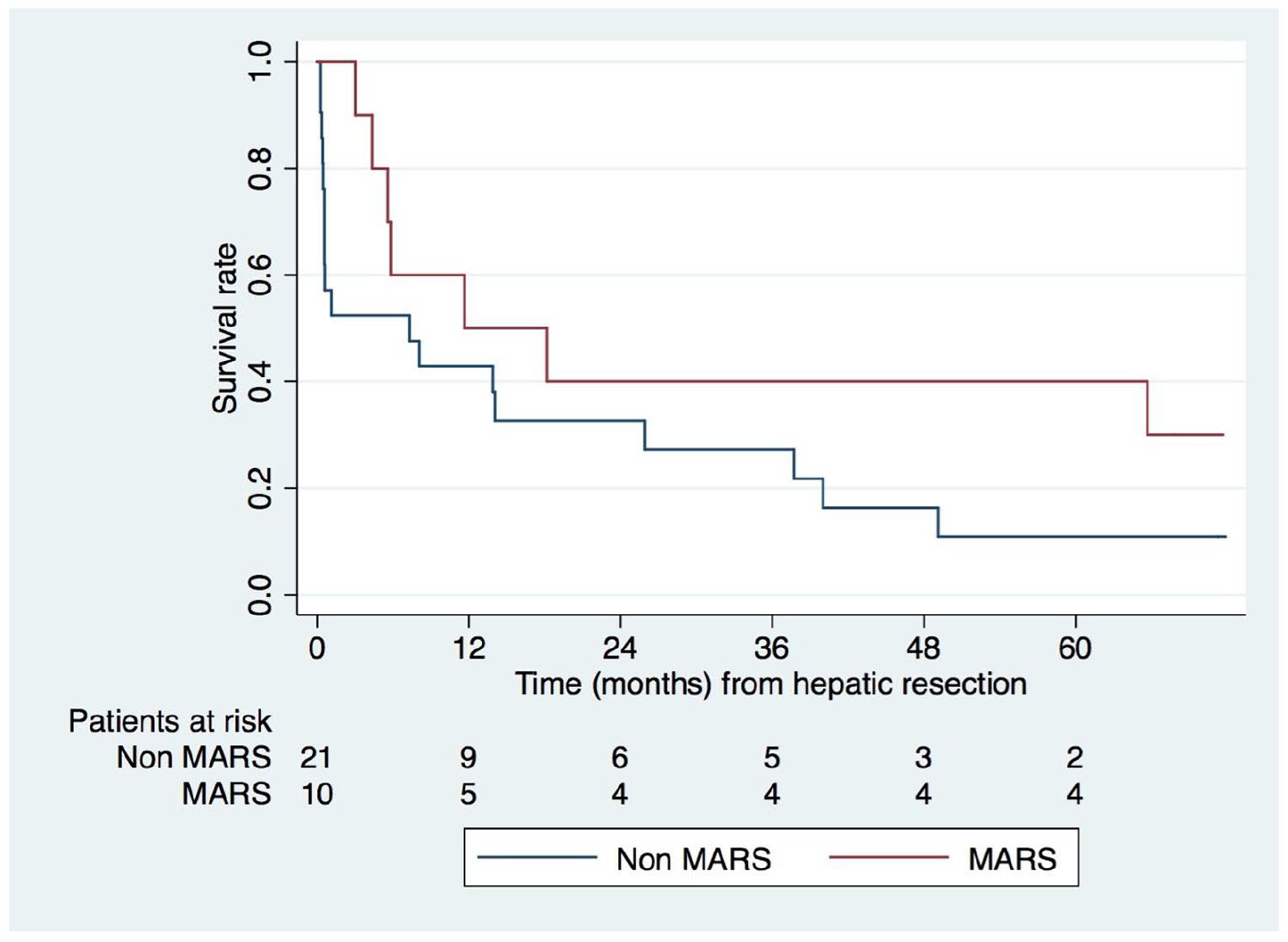
Kaplan–Meier estimates of patients fulfilling Balzan criteria, treated with MARS versus standard of care (non-MARS) (p = 0.14).
Discussion
Long-term survival of patients with PHLF surviving the first 90 postoperative days has not been studied extensively. The few available studies demonstrated a significant negative impact of PHLF not only on short-term but also long-term survival.14–16
To our knowledge, the present study is the first to assess long-term survival following MARS treatment for PHLF. PHLF patients treated with MARS showed a tendency for improved 5-year OS compared to patients with PHLF not treated with MARS. However, the difference did not reach statistical significance. A possible explanation for this is that the small sample size of the original safety and feasibility MARS study was not powered to detect significant improved OS. However, normalizing of liver function following MARS treatment might directly contribute to improved survival, and faster recovery may also allow for adjuvant chemotherapy to be administered in the therapeutic postoperative window. Comparing clinically relevant variables in the three study cohorts, the only significant difference observed was a reduced peri-operative administration of ⩾3 packed red blood cell (PRBC), implying less bleeding complications in the later, post-MARS cohort. This observation is probably related to an improved pre- and peri-operative management over the study period.
In clinical practice, there is no specific treatment for patients with severe PHLF, other than supportive medical treatment and aggressive management of complications. 5 Treatment recommendations are similar to guidelines for the treatment of acute liver failure in general. 17 Thus, guidelines are needed in the future to allow for an appropriate selection of PHLF patients and to determine the optimal timing of MARS treatment. In a systematic review on MARS treatment in PHLF, patients with primary PHLF and early postoperative treatment start demonstrated the most beneficial treatment effects. 18 However, further studies are needed to support such a strategy. Blood markers for early prediction of PHLF and its related morbidity and mortality, for example antithrombin-III activity, micro RNA signatures, or von Willebrand factor, have been investigated but are not routinely used or validated.19–21 Hopefully, such an approach might help to differentiate between PHLF patients with a potential for spontaneous recovery and those at high risk for a lethal outcome at the earliest possible time in the postoperative course. Given the high resource consumption associated with MARS treatment, such a strategy might help in the future to improve patient selection and consequently optimize utilization of medical resources.
The definition of primary and secondary liver failure was not established at the time the MARS study was conducted. However, our strategy to restrict inclusion to patients with primary liver failure seems to be supported by a recent publication. 22 This study on patients with perihilar cholangiocarcinoma found that more than 50% of patients with PHLF developed secondary liver failure, defined as liver failure caused by postoperative complications. Secondary PHLF is associated with surgical or medical complications and without addressing these, specific treatment for PHLF alone is unlikely to improve patient survival.
Another observation in the MARS study group was the conversion of four patients from acute PHLF into a state of chronic liver failure. These patients had similar clinical characteristics with progressively increasing bilirubin, moderately elevated INR (International normalized ratio), anemia, and hypoalbuminemia. Their clinical course was complicated by bleeding complications and recurrent infections leading to premature death. In addition, all of these patients had early disease recurrence and survival was less than 1 year.
The present study has obvious limitations due to its retrospective study design. In addition, the small number of PHLF patients do not allow for profound statistical analysis. Because of the small sample size of the MARS cohort, a multivariable analysis was not considered to be reasonable. From the beginning, the study was not designed to demonstrate improved survival and the results of this study do not provide sufficient evidence for the routine use of MARS in PHLF. However, as this is the first study to evaluate long-term survival following an interventional therapy in PHLF patients, the study results could serve as a basis for power calculations in the planning of future interventional treatment studies. A prospective randomized trial (The Early liver support with MARS in post-hepatectomy liver failure (ELISH trial), ClinicalTrials.gov Identifier: NCT03761238) was planned but not started due to several reasons. First of all, MARS is a resource consuming and expensive treatment applied at intensive care units. In addition, MARS has never gained broad acceptance within the field of Hepatology and Intensive Care medicine as larger prospective trials have failed to provide evidence for improved outcome in patients with acute 23 or acute-on-chronic liver failure. 24 On the contrary, as an alternative treatment in acute liver failure patients, both high-volume plasma exchange 25 and continuous renal replacement therapy 26 demonstrated beneficial effects on patient survival in large trials. As a result, the use of MARS has not become a standard treatment for liver failure patients and nowadays abandoned in many centers, including our own. However, other treatment concepts than MARS have not been evaluated in PHLF patients; yet their efficacy and safety have to be proven in these patients.
In conclusion, the findings in this study, both in terms of short- and long-term results, justify further exploration of early postoperative MARS treatment in patients with severe PHLF.
Footnotes
Author contributions
S.G., E.S., and C.S. designed the study. In addition, J.E. and R.B. did the data collection and J.E. did the data analysis and optical presentation. S.G., E.S., C.S., G.N., E.J., and B.I. contributed to patient inclusion. The study protocol was approved by all authors as well as all authors contributed with a critical revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: E.S. was supported by grants from the Bengt Ihre Foundation, the Center for Innovative Medicine at Karolinska Institutet and Region Stockholm. P.S. was supported by the Stockholm County Council (K2017-4579), Center for innovative medicine, and The Swedish Cancer Society. J.E. was funded by Bengt Ihre Research Fellowship and supported by Region Stockholm (clinical postdoctoral appointment). The funding sources had no involvement in the design or conduct of the study, the writing of the report, or the decision to submit the article for publication.