
Abstract
Background and aims:
Per oral endoscopic myotomy (POEM) has become an established treatment for achalasia, but no Scandinavian studies with long-term follow-up exist. This study from a tertiary referral center in Norway investigates the short-, mid-, and long-term feasibility, safety, efficacy, and complications of POEM.
Methods:
Prospective data from the first 84 patients who underwent POEM from 2014 to 2019 were analyzed. The median follow-up time was 44 months. Clinical success was defined as the Eckardt score (ES) ⩽3, and reflux as pathological if the acid exposure time (pH < 4) was more than 6%. ES was used for symptom evaluation before, and at 6, 12, and up to 64 months after POEM.
Results:
A total of 50 males and 34 females were included. A total of 43 (51%) were treatment naïve, 24 (28.6%) had been previously treated with botulinum toxin, pneumatic balloon dilatation, or both, and 17 (20.2%) were previously treated with Heller’s myotomy. The median post-POEM ES at 12 months was 1 (0–9), compared to pre-POEM 7 (4–12) (p < 0.01). At 12 months after POEM, clinical success persisted in 74 patients (88.1%). Clinical success was the highest for patients who were naïve to treatment, 41/43 (95%), and lower for those previously treated with Heller’s myotomy 12/17 (70.6%). Long-term follow-up at 5–6 years of 42 patients showed a clinical success rate of 94%. We experienced adverse events in five patients (6%). Post-POEM pathological reflux was found in 46% (28/61). After 3–4 years, the median ES was 1, and after 5–6 years, it was 2.
Conclusion:
POEM was safe and relieved the symptoms of achalasia significantly and persistently. The procedure had a better outcome in treatment naïve than previously treated patients. However, POEM is associated with significantly increased esophageal acid exposure.
Twitter summary
Norwegian single-center study: POEM had a clinical success rate of 94% after 5–6 years since its introduction at the center in 2014, providing a safe and effective treatment for achalasia.
Keywords
Context and relevance
Since peroral endoscopic myotomy (POEM) was first introduced in 2010, it has become an established treatment modality for achalasia. Several studies have documented excellent short- and mid-term results. Long-term follow-up studies are limited, and there are no Scandinavian studies available to this date. This study from a Norwegian tertiary center shows that POEM effectively relieves symptoms of achalasia after 5–6 years with few adverse events. However, the study revealed a higher post-POEM gastroesophageal reflux rate than other studies. We believe that this study is valuable to the surgeons and endoscopists when navigating the emerging field of interventional endoscopy.
Introduction
Achalasia is a rare motility disorder of the esophagus. Current therapeutic options include pneumatic balloon dilatation (PBD), botulinum toxin (BTX) injection into the lower esophageal sphincter (LES), and laparoscopic Heller’s myotomy (LHM). Since per oral endoscopic myotomy (POEM) was first described in 2010 by Inoue et al., 1 it has gradually become an established treatment option for hypercontractile esophageal motility disorders in all age groups. 2 Short- and mid-term results are excellent, but long-term results beyond 4 years are limited and have yet to be investigated in the Scandinavian population.3–8 The POEM procedure was introduced at our center in early 2014, as the first center in Norway.
Patients with achalasia often report dysphagia, sometimes weight loss, retrosternal pain, and regurgitation. These symptoms are the basis for the Eckardt score (ES), which is used to evaluate the severity of achalasia and results of therapy. 9 High-resolution manometry (HRM) is the gold standard in achalasia diagnostics and allows subdivision of achalasia into three subtypes according to the Chicago classification. This classification may also be useful for selecting treatment and predicting outcome. 10
The primary endpoint of this study was the clinical outcome of POEM in short-, mid-, and long-term evaluated by ES, with the clinical success defined as ES ⩽ 3 after POEM. The secondary outcomes were the effects of procedural parameters such as the myotomy direction and selective circular or full-thickness myotomy, frequency of adverse events (AEs), the difference in LES integrated relaxation pressure before and after POEM, and post-POEM gastroesophageal reflux (PGER).
Patients and methods
Subjects and study design
Eighty-four consecutive patients who underwent primary POEM for achalasia at Haukeland University Hospital were prospectively registered and evaluated for a quality assurance study between February 2014 and June 2019. Redo-POEM was performed in three patients during the same period. The Regional Committee for Medical and Health Research Ethics in Western Norway was consulted and waived the study as POEM was already established as a clinical treatment method internationally. Hence, the study was not registered in a clinical trial database. The inclusion criteria and indication for POEM were patients older than 16 years with HRM-confirmed achalasia, ES ⩾ 5 who could give informed consent. Patients who were previously treated with PBD, BTX, or LHM, without intended effect or with relapse of symptoms were also included. Exclusion criteria consisted of pregnancy, inability to provide informed consent, and patients unfit for general anesthesia. Before POEM, we assessed all patients with ES, performed HRM (ManoScanESO®, Medtronic Inc., Minneapolis, MN, USA), pH impedance monitoring (Ohmega®, MMS BV, Leiden, the Netherlands), and timed barium swallow in standardized projections—anterior-posterior, lateral, and oblique, with minimum 6 s films and esophagogastroduodenoscopy.
Procedure
All POEM procedures were performed by a single operator (K.D.-C.P.) with the patient under general anesthesia. The patients received prophylactic topical anti-fungal therapy for 7 days, and a single dose of intravenous Metronidazole and Cefalotin during POEM. A high-definition endoscope (HQ190, Olympus Inc., Tokyo, Japan) was used. Two different types of diathermic knives were mainly used: TriangleTip Knife® (KD-640L, Olympus Inc.) and Erbe T-type (Erbe, Tübingen, Germany) in combination with an electrosurgical unit (VIO300D, Erbe). The setting for the electrosurgical unit for the TriangleTip knife was Endocut–Q, effect 2 for mucosal incision and myotomy, and spray coagulation 50 W, effect 2 for submucosal dissection. For the Erbe T-type knife, the setting on the electrosurgical was Endocut-Q, effect 2 for mucosal incision, and swift coagulation for submucosal dissection. For the hemostatic forceps, the setting was soft coagulation 80 W, effect 5. Sterile water was used for irrigation, CO2 gas was used for insufflation. We injected 2–3 mL of saline with indigo-carmine to create a submucosal lift 2–3 cm proximally to the intended myotomy tract and incised the mucosa. A submucosal tunnel was created until 2–3 cm into the cardia. Gentamycin 80–160 mg was routinely sprayed in the submucosal tunnel before myotomy in the first 70 cases but was discontinued thereafter. The length of the myotomy was chosen individually according to the Chicago subtypes of achalasia found on HRM and modified timed Barium swallow. The direction of the myotomy (anterior: 12–2 o’clock, posterior: 5–7 o’clock with the patient in the supine position) was selected at the discretion of the operator, but patients previously treated with LHM were treated with posterior myotomy. Selective myotomy of the circular muscle or full myotomy was done in the esophagus and 3 cm into the cardia (Fig. 1). The procedure was finalized by closing the mucosal entrance with hemostatic clips. The procedure time and any intra-operative AEs were recorded. After POEM, the patients fasted for 24 h before repeated timed barium swallow. Subsequently, the patient could start oral intake, increasing consistency from liquid to normal food over 7 days. Proton-pump inhibitors (PPIs) were given routinely for 2 weeks and on-demand thereafter.
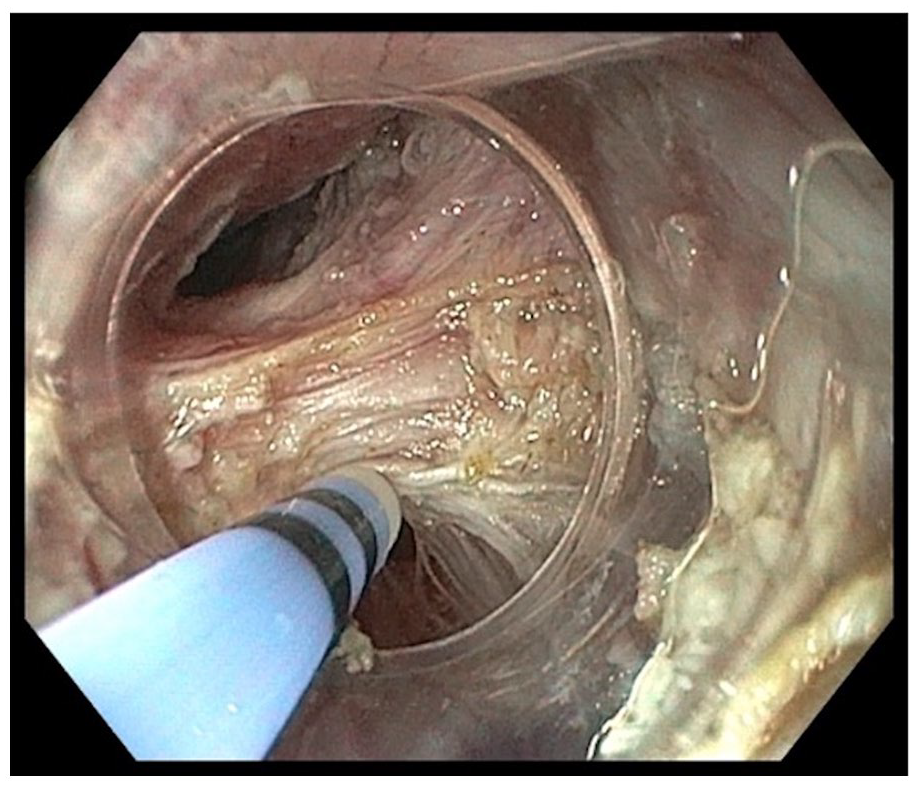
Myotomy of the lower esophageal sphincter during POEM.
Measured outcome and follow-up
The ES was re-evaluated at 6 and 12 months, and 2, 3–4, and 5–6 years after POEM. Patients were also evaluated with 24-h pH impedance monitoring for PGER. The patients were asked to stop PPI 1 week before the examination. Pathological reflux was defined when the acid exposure time was more than 6% in 24 h, according to the definition from 2017 by the International Working Group for Disorders of Gastrointestinal Motility and Functions. 11 The patients were also followed up with HRM and timed barium swallow around 12 months after POEM in three standardized projections. AE were classified according to the Clavien–Dindo classification, which defines AE as an event that is considered to be any deviation from the normal post-operative course. 12
Statistical analysis
Continuous variables are presented as mean values and standard deviations (SDs) or as medians and min–max or range unless stated otherwise. Normality was tested with QQ plots and Shapiro–Wilk’s test. Continuous variables before and after POEM were compared with paired Student’s t-test or Wilcoxon’s test as appropriate. Associations with clinical outcomes were analyzed with univariate and multivariate logistic regression models, including univariate (unadjusted), fully adjusted, and final models. The final models were made by stepwise, backward exclusion of covariates with a <90% probability (p ⩾ 0.10) of association with clinical outcome, including forced entry of age and male gender. A p-value of <0.05 was considered statistically significant.
Results
We included 84 patients (50 males, 34 females). The baseline and procedural characteristics are shown in Table 1. POEM was performed successfully in all 84 patients (100%). The myotomy length median was 11 cm (range = 4–20). Full-thickness myotomy of the LES was performed in 66/84 (77.4%), and selective myotomy of the circular muscle was performed in 19 (22.6%). Fifty-four (64.3%) received posterior myotomy, while 30 (35.7%) had anterior myotomy. The procedure time was median 120 min (50–250). A coagulation forceps was used to treat active bleedings or seal vessels in 34 procedures (40.5%) prophylactically. The mean length of admission was 3 days. In three patients, a second POEM procedure was performed after 16–32 months due to relapse of symptoms. All three redo-POEMs achieved a post-procedural ES ⩽ 3.
Patient characteristics and procedure parameters.
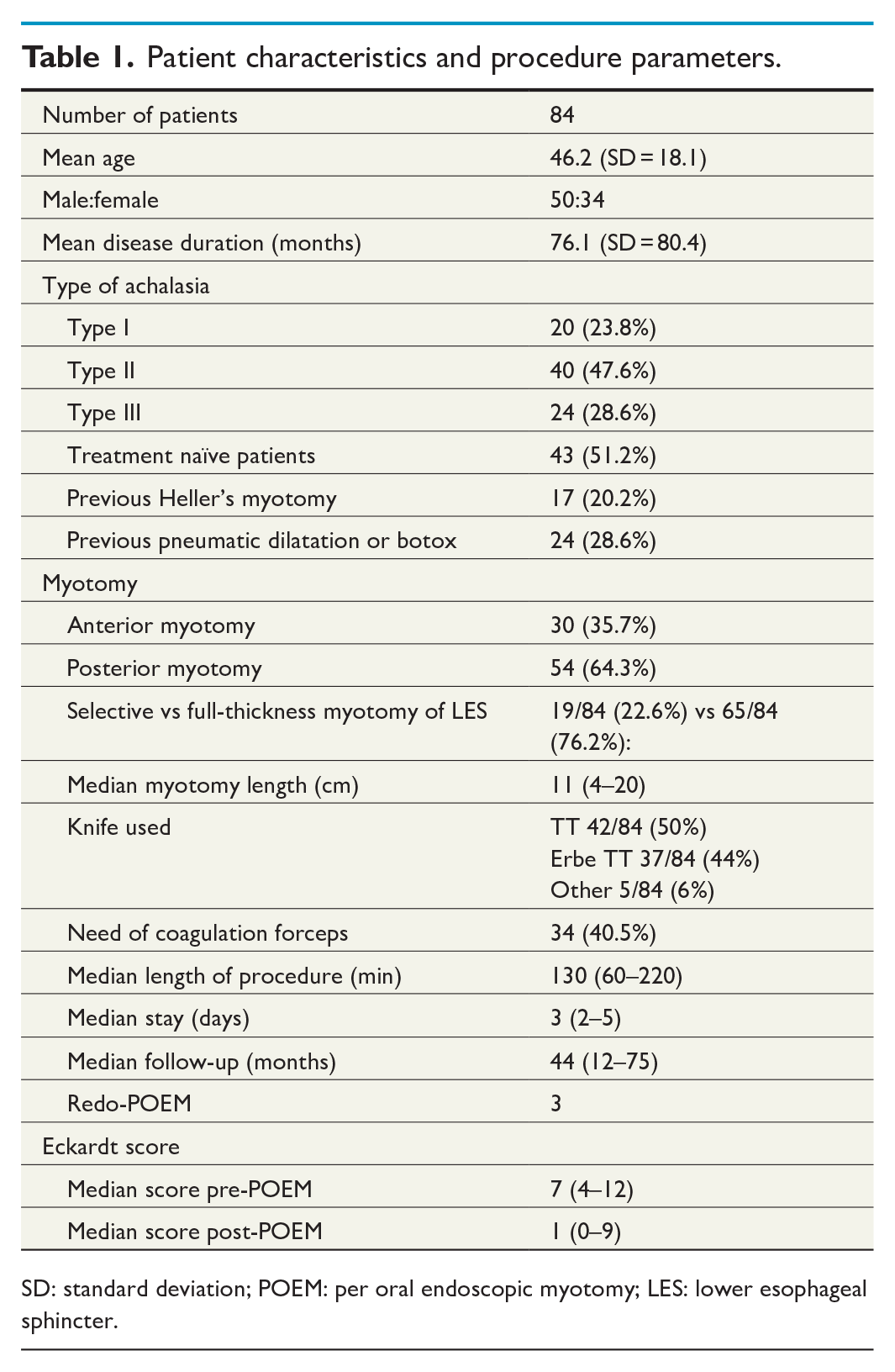
SD: standard deviation; POEM: per oral endoscopic myotomy; LES: lower esophageal sphincter.
Follow-up
Follow-up data were obtained for all patients at 12 months, including ES (100%) and timed barium swallow (100%), whereas HRM and impedance could be obtained in 71 patients (85%) and 24-h pH measurements for 61 (72.6%) patients. The number of patients followed up at 12 months, 2, 3–4, and 5–6 years was 84 (100%), 68 (80%), 54 (64%), and 42 (50%), respectively. The median post-POEM ES at 12 months was 1 (0–9), compared to pre-POEM 7 (4–12), p < 0.01. At 12 months after POEM, clinical success was achieved in 74 (88.1%) patients when defined as ES ⩽ 3, while 63 patients (75%) had ES ⩽ 2. Clinical success was the highest for patients who were treatment naïve, 41/43 patients (95%). For patients previously treated with PBD or BTX, the clinical success rate was somewhat lower 21/24 patients (87.5%). For the previously treated patients with Heller’s myotomy, the clinical success rate was significantly lower 12/17 (70.6%, p = 0.02) (Fig. 2 and Table 2). For all achalasia subgroups, the symptoms improved significantly after POEM, although at 12 months, type III achalasia had a higher median ES, the 75 percentile was still at ES 3. There was no significant difference in ES between the achalasia types after 12 months. For patients who were followed for more than 4 years, there was a tendency to increase in ES after 2–3 years, although the median ES after 12 months and at 3–4 years was 1 (0–6), and after 5–6 years, the median ES was 2 (1–6) (Fig. 3). Forty-two patients were followed up for more than 5 years, during which one patient with achalasia type II and one with type III (6.3%) had recurrence with ES > 3. One patient who had failed LHM with fundoplication, POEM, PBD, and BTX was treated successfully with retrograde endoscopic myotomy. 13 In univariate and multivariate logistic regression models for associations with clinical failure defined as ES > 3 and reflux based on 24-h pH measurement, we found that full-thickness myotomy reduces the risk of reflux (odds ratio (OR) = 0.12, 95% confidence interval (CI) = 0.02–0.63), but increase the risk of clinical failure (OR = 3.94, 95% CI = 1.00–15.57), while the different manometric subtypes, the direction of the myotomy, and smoking did not affect the clinical outcome nor PGER (Table 3).
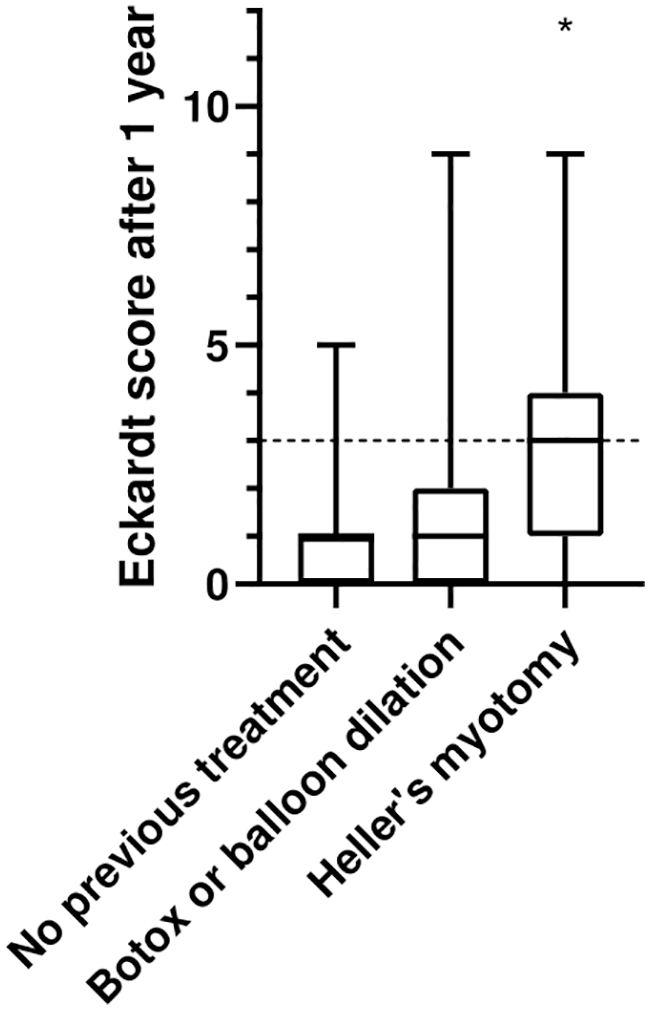
Comparing the Eckardt score after 1 year for the different pre-POEM treatments.
Association between previous treatment and clinical success defined as the Eckardt score ⩽3 after 12 months.
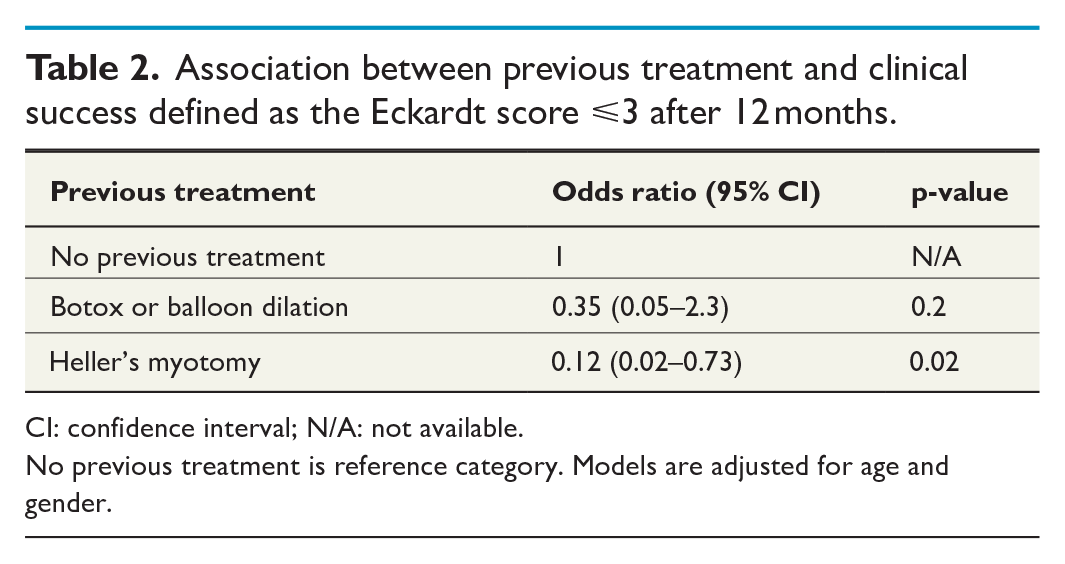
CI: confidence interval; N/A: not available.
No previous treatment is reference category. Models are adjusted for age and gender.
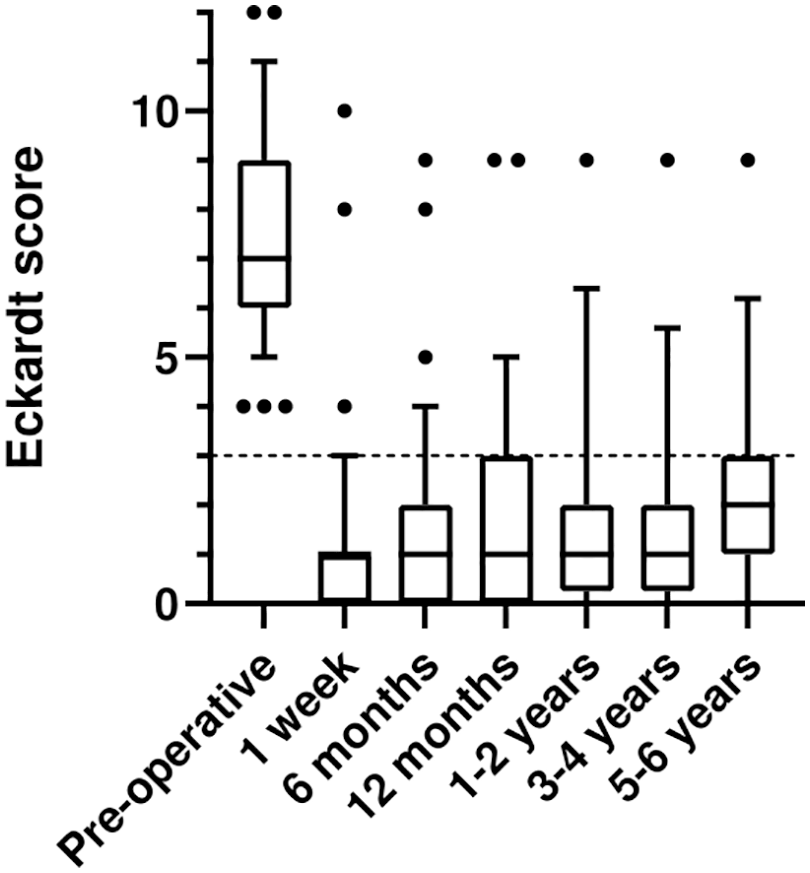
The development of the Eckardt score over time after POEM.
Univariate and multivariate logistic regression models for associations with clinical failure defined as the Eckardt score > 3.
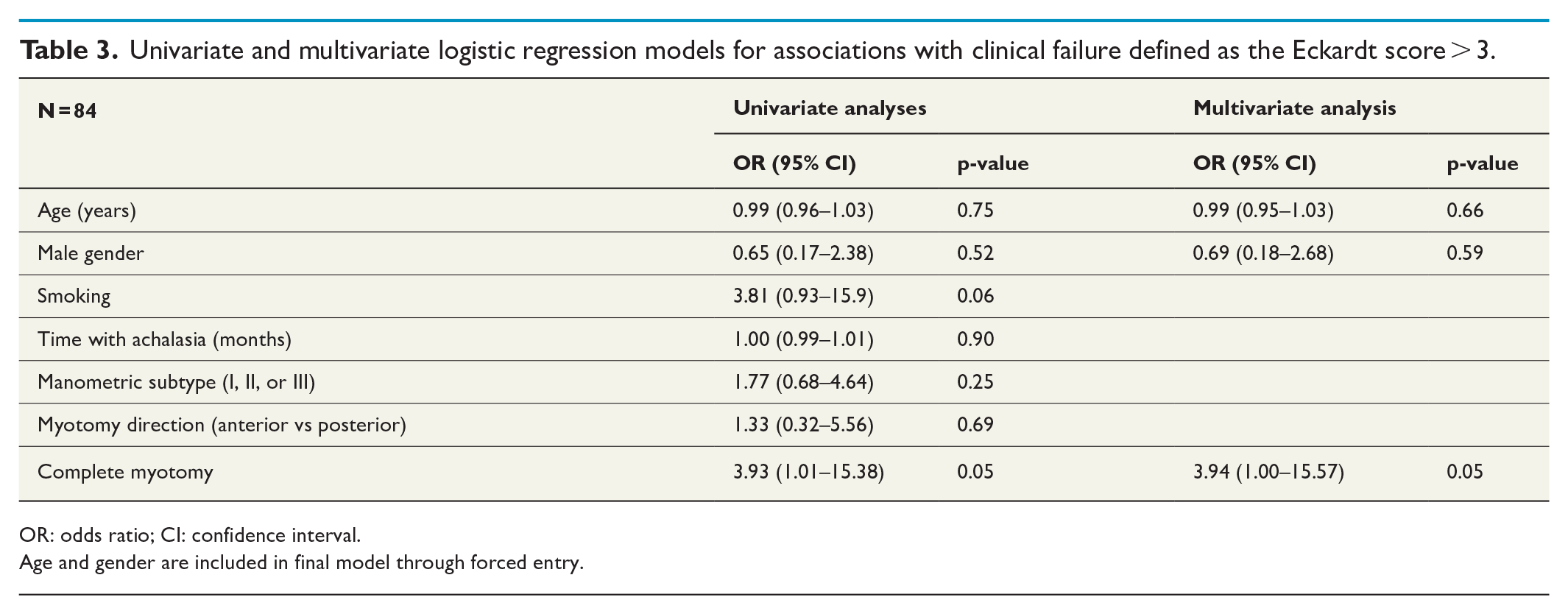
OR: odds ratio; CI: confidence interval.
Age and gender are included in final model through forced entry.
HRM
Control HRM (n = 70, 83%) showed a significant reduction of the LES integrated relaxation pressure after POEM (mean = 27.8 mmHg vs 7.6 mmHg, p < 0.0001).
24-h impedance pH-metry
A total of 33 patients (39%) had symptomatic reflux, while 30 (36%) reported that they were using PPI daily or on-demand. 24-h pH measurements were obtained for 61 patients (72%), of these, 28 (46%) had a pathological acid exposure time of more than 6%/24 h. The percentage of patients with PGER in our cohort varied depending on their previous treatment. Albeit not statistically significant, pathological post-POEM acid exposure time >6%/24 h was found in 18% of patients previously treated with LHM, in 54% in treatment-naïve, and 46% in post-BTX and PBD-treated patients.
Adverse effects
Post-operative capnoperitoneum and capnothorax were observed in 11 patients (13%) on X-ray, of which three patients (4%) required intra-operative peritoneal decompression. Five patients (6%) developed subcutaneous emphysema around the neck during POEM and were treated with forced intra-operative hyperventilation (Grade 1). One case of mucosal injury was treated with clips during POEM. None developed post-operative infections. All perioperative complications were treated endoscopically or by forced respiration in the first session, without further endoscopy sessions. Bleedings were managed most frequently with the diathermic knife. The coagulation forceps was only used in 40% of bleedings.
Discussion
In this study, we present the largest series of achalasia patients in Scandinavia treated with POEM. It confirms that POEM is an effective treatment for achalasia of all types with few adverse events both in treatment-naïve patients and in patients previously treated, with long-lasting effect.
The strength of this study is the high follow-up rate and its relatively long follow-up time. Compared to other larger series,14,15 where a considerable number of patients were lost to follow-up, our data were collected prospectively, with relatively high adherence to the follow-up protocol. In our cohort, we have follow-up data for long-term ES and timed barium swallow (100%), HRM (83%), and 24-h pH measurements (70%). One publication suggests that in order to improve the evaluation of the outcome of POEM, the follow-up rate should be higher than 80% and should include symptom scoring, HRM, timed barium swallow, the treatment goal, and evaluation of reflux. 16 All the procedures were performed by one endoscopist, which limits inter-operator variability. This study is limited by the small number and the geographical spread of our patients, as it was not always possible to perform follow-up 24-h pH measurements and HRM at our center. In addition, complete data for pH measurements were only available in 70%, which may influence the results.
Furthermore, we have not taken the endoscopists learning curve into account. Our cohort is very heterogeneous with respect to age, sex, geography, duration of disease, and previous treatment. As we have included patients consecutively, the material represents the real-world experience of achalasia patients in a reference center. Nearly half of the patients had received other treatments, including surgery, and some had undergone multiple treatments before POEM. In this group, the anticipation of symptom relief after POEM would be lower. Nevertheless, the short- and long-term results for most patients are good. Our clinical success rate in the short- and mid-term is consistent with other series.3,17 The most challenging group to treat were those who had previous LHM, where the success rate was only achieved for 12/17 patients (70.6%) at 12 months, compared to patients who had been treated with PBD (87.5%) and BTX (95.3%). We do not fully understand why our success rate is lower than previously reported for POEM after LHM. 18 One possible explanation is that patients who relapse with symptoms after LHM represent a selection of patients who originally had type III or diffuse esophageal spasm, in which LHM is known to be less effective.19,20 The current consensus is that type III and diffuse esophageal spasm should be treated with long myotomy. 21 In Norway, LHM is usually combined with concomitant fundoplication, which may cause mechanical obstruction in the lower esophagus, despite efficient myotomy.
Surprisingly, full-thickness myotomy of the LES reduced the clinical success and at the same time reduced the risk of PGER in our logistic regression model. This finding is contrary to what we would expect and may be explained by a low number of patients who received full-thickness myotomy and residual confounding. In this study, the majority (65/84 patients) had full-thickness myotomy. However, further studies are needed to verify this result. A previous meta-analysis on risk factors for PGER did not find significant differences between circular nor full-thickness myotomy. 22
PGER is the most frequent side effect of POEM. The reflux rate reported in the studies depends on how gastroesophageal reflux was assessed and the follow-up rate. In the early and larger case series, the reflux rate was reported to be lower; 13%–21.3%,15,23 but with increased numbers of POEM performed, PGER is also seen more frequently. There is no formal and standard definition of PGER, but a recent expert review recommends that the definition of gastroesophageal reflux from the Lyon consensus should be used, 24 to which this study complies. Based on acid exposure time >6%, Brewer Gutierrez et al. 4 reported 47.5% reflux, while Martinek et al. 18 found 41.5% in a study including 155 patients where 72% underwent 24-h pH measurements. In the same study, 37.8% used PPI, while we found 36.6% PPI users in our series. The majority of patients with PGER respond to PPI therapy. 25 Therefore, our result for PGER at 46% measured with acid exposure time >6% seems reliable. Recent publications indicate that the prevalence of PGER is most likely in the order of 44%–58% in mid- and long-term follow-up.25–27 Although based on a small number of patients, it seems that POEM is a god alternative after failed LHM with regard to PGER. This may be due to the fact that all the patients who were treated with LHM had also a fundoplication.
The dominant symptom among the non-responders was pain. In our experience, pain was also the most difficult symptom to relieve and a high pain score in ES may represent a prognostic indicator for non-responders. Three patients with type II + III achalasia, who did not experience clinical improvement after primary POEM, were treated successfully with posterior redo-POEM, extending the myotomy to the proximal part of the esophagus. In these patients, the common findings were hypercontractile segments in the mid and proximal esophagus. This suggests that a longer myotomy should have been performed during the first POEM procedure. Redo-POEM was performed in three patients in our cohort. However, if we include the second POEM, the overall clinical success rate increases to 91% (77/84). Other authors have also reported high clinical success rates for redo-POEM, 28 confirming that redo-POEM is an efficient treatment for failed primary POEM in patients in whom symptoms remain or relapse early, and where high-pressure zones can still be detected in the esophagus on HRM.
The definition of long-term follow-up after POEM is controversial, and it ranges from 2 to 7 years in various studies. Data on long-term effects of POEM surpassing 4 years are scarce.3–8 Three of the studies with the longest follow-up after POEM include a series of 32 patients from China and a large single-center series from the United States with 610 patients, who were followed over 7 and 10 years, respectively.5,8 These studies show a success rate between 88% and 95% at 4–5 years, reflux symptom rate at 20.5%–38%, and a positive pH study of 57.1%. Our long-term data of 42 patients with 5–6 years follow-up show similar results with clinical success of 94% and reflux rate at 40%. All recurrences in our series happened within the first 24 months, similar to results reported by Werner et al. 26 Type II and Type III achalasia tend to recur, and there were no redo-POEMs with type I achalasia in our series.
POEM is a safe procedure without serious AE in our series. Capnoperitoneum and capnomediastinum are common, and usually do not need treatment. However, after introducing prophylactic forced hyperventilation and hypocapnia, we observed a marked reduction in CO2-related AE. The first 70 POEM procedures were performed with prophylactic submucosal gentamycin spray prior to myotomy. The discontinuation of gentamycin in routine practice did not increase our infection rate nor change the response in inflammatory parameters after POEM. Submucosal lavage with gentamycin is no longer recommended in the guidelines from 2020 set by the European Society of Gastrointestinal Endoscopy (ESGE). 29
One advantage of POEM is the possibility to use it as salvage where other treatments have failed, including POEM. The POEM procedure has reduced the load on surgical capacity at our center since it can be performed in an endoscopy room. Another advantage compared to LHM is that it induces less post-operative pain, 2 but still offers a similar resolution of dysphagia at 2 years follow-up.26,30 However, the post-POEM reflux condition is still the main concern. This study supports the view that POEM is a valid alternative for treatment of achalasia and also efficient in type III achalasia/hypercontractile esophageal motility disorders.
Conclusion
POEM is safe and efficiently relieved achalasia symptoms in the short- and long-term for the first 84 patients from Norway. The efficiency and complication rates were comparable to other reports, even with a heterogeneous cohort that included many patients who had undergone previous treatments. However, we found a higher PGER rate than previously reported.
Footnotes
Acknowledgements
The authors are grateful to Professor Lars Birger Nesje, Professor Georg Dimcevski, Roy Cato Solheim, the nurses from the Department of Medicine, and Terje Stokke (ret.) at the Department of Radiology, Haukeland University Hospital.
Author contributions
K.D.-C.P. has performed all the procedures, collected the data, included, and followed up the patients and drafted the manuscript. S.S.L. has written sections of the manuscript and revised the manuscript, R.F.H. has participated in several procedures, contributed to the statistical work and figures as well as revision of the manuscript. E.T. has contributed to the statistical work and figures as well as revision of the manuscript. J.G.H., and O.H.G. have revised the manuscript. J.A did counseling on statistical analysis.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.D.-C.P. has received lecture fees, travel, and education support from Olympus. O.H.G. has received speaker honoraria from AbbVie, Bracco, Almirall, GE Healthcare, Takeda AS, Meda AS, Ferring AS, Janssen-Cilag, and Allergan. He has served as consultant for Bracco, GE Healthcare, Takeda, and Samsung. R.F.H. has received lecture fees from Bristol-Myers Squibb.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.