
Abstract
Background and objective:
The growing number of identified intraductal papillary mucinous neoplasm (IPMN) patients places greater pressure on healthcare systems. Only a minority of patients have IPMN-related symptoms. Thus, more precise surveillance is required.
Methods:
In this retrospective single-center cross-sectional study, patients with an active diagnosis of branch duct IPMN (BD-IPMN) and >6 months of surveillance were classified as follows: presence/absence of worrisome features (WF) or high-risk stigmata (HRS), newly developed WF/HRS, under/over 15 mm cyst, growing/not growing <15 mm cyst, and elevated serum carbohydrate antigen 19-9 (CA 19-9).
Results:
In all, 377 patients with BD-IPMN were followed for a median of 5.4 years, 28% with WF at diagnosis, and 14% who developed WF/HRS during surveillance. Half had a <15 mm primary cyst, 40% of which did not grow during surveillance. CA 19-9 was elevated in 12%. None of the patients with normal CA 19-9 levels developed cancer or high-grade dysplasia (HGD).
Conclusions:
No carcinomas or HGDs appeared with normal CA 19-9 levels. Patients with <15 mm cysts that do not grow and have no WF/HRS could undergo imaging less frequently.
Keywords
Introduction
The number of pancreatic cysts detected has increased alongside the increasing availability of higher resolution abdominal imaging. 1 The prevalence of pancreatic cysts in a healthy population was 49.1% in a 2017 study by Kromrey et al., with only 6% presenting with cysts over 1 cm in size. 2 Cyst prevalence and size increase during one’s lifetime. 2 Intraductal papillary mucinous neoplasms (IPMNs) constitute the largest group of pancreatic cysts. 3 In addition, IPMN can progress to cancer.3,4 Based on the high prevalence of IPMN and low incidence of pancreatic cancer, only a minority of IPMNs progress to invasive carcinoma.5,6 IPMNs fall into three types: main duct IPMN (MD-IPMN), branch duct IPMN (BD-IPMN), and mixed type (MX-IPMN). 3 Among these, MD- and MX-IPMN carry the highest risk of progressing to malignancy. 4 In BD-IPMN, the risk of malignant transformation during follow-up stands at approximately 3%–15%. 7
Due to the risk of malignancy, IPMN patients remain under surveillance. Little evidence exists in the literature to guide the frequency, duration, and type of surveillance for IPMNs.1,8 In 2015, American Gastroenterological Association (AGA) guidelines advocated for ceasing surveillance after BD-IPMN patients remained asymptomatic for 5 years. 9 By contrast, European guidelines recommend lifelong surveillance of patients fit for surgery. 4 At Helsinki University Hospital, IPMN surveillance adheres to European guidelines. Such surveillance includes magnetic resonance imaging (MRI) and laboratory testing, including monitoring of serum carbohydrate antigen 19-9 (CA 19-9) levels.
However, the growing amount of IPMN patients under surveillance requires identifying a subpopulation of patients that are at the lowest risk of developing malignancy and who thus do not need annual follow-up. 8 In 2020, Ciprani et al. demonstrated that cysts <15 mm at the time of diagnosis had a very low risk of malignant transformation, with that risk decreasing over time. 10 Furthermore, they argued that a size increase of ⩾2.5 mm/year represents the strongest predictor of malignancy. 10
This study aimed to analyze long-term outcomes among patients with BD-IPMN presenting without worrisome features (WF) and/or high-risk stigmata (HRS) at the beginning of surveillance. In addition, we aimed to find patients that are at lowest risk of developing a malignancy.
Methods
Patient selection, and inclusion and exclusion criteria
We retrospectively identified 521 patients diagnosed with pancreatic cystic lesions in the Department of Gastrointestinal Surgery, Helsinki University Hospital from 2014 through 2016. The inclusion criteria for this study were as follows: a working diagnosis of BD-IPMN made by study observers, 1 and a minimum 6-month-long surveillance. We excluded patients with (1) a previous pancreatic carcinoma, (2) no MRI or computed tomography (CT) after the initial diagnosis, and (3) a working diagnosis other than IPMN (e.g. serous cystadenoma, mucinous cystic neoplasm, cystic neuroendocrine tumor, solid pseudopapillary tumor, chronic pancreatitis, or pseudocyst). This resulted in 377 BD-IPMN patients (Supplementary Figure 1).
This retrospective study was registered and approved by the Surgical Research Committee of Helsinki University Central Hospital (HUS/333/2019, extended HUS/155/2021). Because of the retrospective nature of this study and the Act on the Secondary Use of Health and Social data (552/2019), the written informed consent of the patients was not demanded.
Follow-up
Follow-up was first performed according to the 2006 International Consensus Guideline (Sendai), 11 according to the Fukuoka Guidelines from 2012, 3 and according to European guidelines from 2018. 4 Indications for surgery relied on these guidelines.3,4,11 The study observers did not participate with the actual patient follow-up or with the operation decisions. The duration of follow-up was recorded as beginning with the first evaluation of cross-sectional imaging evaluated by the pancreatic surgeon through one of the following endpoints: date of operation, date of initial discovery of a malignancy upon imaging for patients who underwent neoadjuvant treatment or who had an unresectable tumor, or the date of the last evaluation or a patient’s death without progressing to pancreatic cancer.
Statistical analysis
In our analysis, we report categorical variables as frequencies and percentages, and continuous variables as means and 95% confidence intervals (CIs) or medians and interquartile ranges (IQRs) if data were skewed. We compared categorical variables using the chi-square or the Fisher’s exact tests as appropriate. Continuous variables were compared using Student’s t-test or the Mann–Whitney U-test. We detected no statistically significant differences between patients whose surveillance started before or after 1 January 2014, and thus, the entire population was analyzed as a whole. Patients whose serum CA 19-9 levels were not measurable during the entire surveillance period were considered Lewis antigen–negative and we considered the CA 19-9 information missing in all analyses involving CA 19-9. This included 35 (9.3%) patients, in agreement with the literature. 12 Mural nodules considered unclear by study radiologists were categorized a “not mural nodules” in the statistical analyses. All tests were two-sided, and we considered p < 0.05 statistically significant. All statistical analyses were performed using SPSS, version 27.0 (IBM SPSS Statistics, version 27.0 for Mac; SPSS, Inc., Chicago, IL, USA).
Data collection
Laboratory and patient history
We collected data on patient demographic characteristics, clinical presentation, and comorbidities. Serum CA 19-9 levels at the beginning and at the highest point were collected upon diagnosis and during follow-up. The upper reference limit for CA 19-9 was 26 kU/L based on the routinely used upper reference limit in our hospital as recommended by the manufacturer of the assay used by the hospital laboratory.
Imaging modalities and analysis
Imaging data were retrospectively analyzed by two radiologists experienced in pancreatic imaging (K.J. and E.L., with 5 and 20 years’ experience, respectively). The imaging modalities used in this study consisted of MRI and/or magnetic resonance cholangiopancreatography (MRCP), CT, and ultrasound (US). MRI examinations were performed using 1.5 Tesla (1.5 T) and 3 Tesla (3T) systems. The MRI/MRCP protocol was long, including volumetric interpolated breath-hold (VIBE) before- and after-contrast agent and diffusion-weighted imaging (DWI) sequences, or short without enhancement and diffusion sequences. CT images were enhanced or unenhanced. Results from US images were collected from radiological reports and US information was only collected at the first instance of a pancreatic abnormality, after which US was not included in further surveillance.
The following imaging timelines were applied to each patient:
Retrospectively observed first imaging where the pancreatic abnormality was detected (by a radiologist or by a study observer);
The initial imaging evaluated by the surgical unit;
The final image completed (final IPMN follow-up or other final CT or MRI scan); or
Preoperative scans for patients who underwent a pancreatic resection.
The parameters evaluated from the datasets appear in Supplementary Table 1.
At the time of diagnosis and during surveillance, patients were categorized according to clinical and radiological WF/HRS characteristics: 1 cyst ⩾30 mm, main pancreatic duct (MPD) size ⩾5 mm, thickened enhanced cyst walls, abrupt change in the MPD caliber with distal pancreatic atrophy, lymphadenopathy, elevated CA 19-9 level, and obstructive jaundice in a patient with a cystic lesion of the pancreatic head. We also took into account all mural nodules (some of the images were unenhanced). Endoscopic ultrasound (EUS) was performed following the guidelines and cyst fluid was evaluated when needed.
Results
Altogether, we included in our analysis 377 patients with a working diagnosis of BD-IPMN, 61.3% female and a mean age of 65.3 years (range: 31.1–87.0 years). The mean follow-up time was 5.4 years (range: 0.5–15.8 years). The initial diagnosis was based on MRI/MRCP in 89.1% and CT in 10.9% of cases. EUS was performed at some point during surveillance on 11.4% and fine-needle aspiration (FNA) on 9.0% of patients. Abdominal images prior to the beginning of surveillance in which the radiologist or study observer retrospectively could see a pancreatic abnormality were available for 361 patients, US for 78 (21.6%), MRI for 69 (19.1%), and CT for 207 (57.3%) patients. The mean time between these images and the beginning of surveillance was 1.1 years (range: 0–12.68 years). The mean cyst size at diagnosis was 17.7 mm (95% CI: 16.7–18.6), with an MPD width of 2.7 mm (95% CI: 2.6–2.8). In 39 (10.3%) patients, the cyst size exceeded 30 mm. At the end of surveillance, 90.7% of patients had MRI images as final completed images and 9.3% had CT. At the end of surveillance, the cyst size had increased in 246 (65.3%) patients, with a mean cyst size for all patients of 19.7 mm (95% CI; 18.5–20.9). MPD widened during surveillance in 103 (27.3%) patients, whereby we observed a final mean width of 3.0 mm (95% CI: 2.9–3.1) in all patients. WF was present in 106 (28.1%) patients upon diagnosis. A new WF or HRS during surveillance emerged in 39 (14.4%) patients. Table 1 summarizes additional patient characteristics.
Patient characteristics.
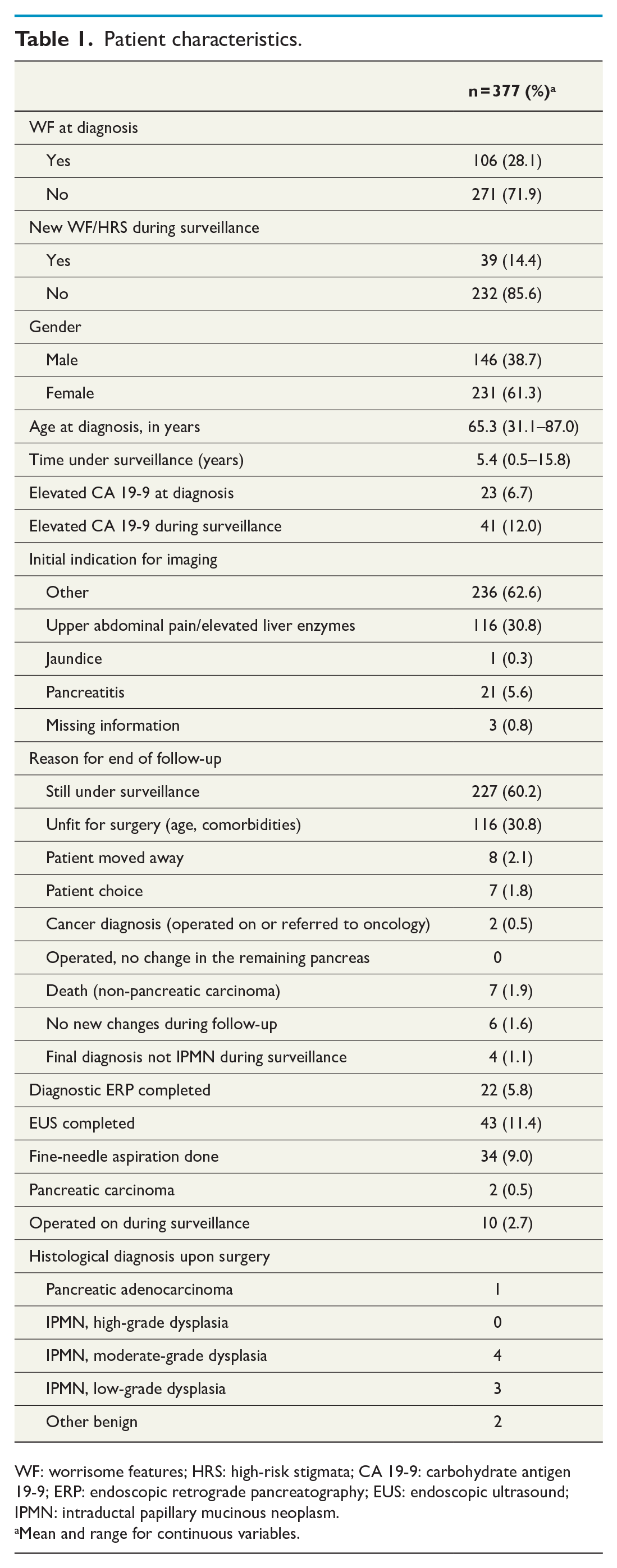
WF: worrisome features; HRS: high-risk stigmata; CA 19-9: carbohydrate antigen 19-9; ERP: endoscopic retrograde pancreatography; EUS: endoscopic ultrasound; IPMN: intraductal papillary mucinous neoplasm.
Mean and range for continuous variables.
WF at diagnosis
At diagnosis, no one had HRS, but 28.1% of patients had WF. The cysts among patients with WF were 24.3 mm compared to 15.1 mm (p < 0.0001) identified in patients without WF/HRS; furthermore, MPD was wider as well (2.9 mm vs 2.6 mm; p < 0.004). We detected no difference in age, although patients with WF had a slightly shorter surveillance period. During surveillance, we found no difference in cyst growth or in MPD widening between groups. Patients with WF at diagnosis underwent surgery more often during surveillance compared to those without WF/HRS at diagnosis (6.6% vs 1.1%; p < 0.006). The development of carcinomas or HGD during surveillance only emerged in two patients with no WF/HRS at diagnosis (Table 2).
Worrisome features at diagnosis.
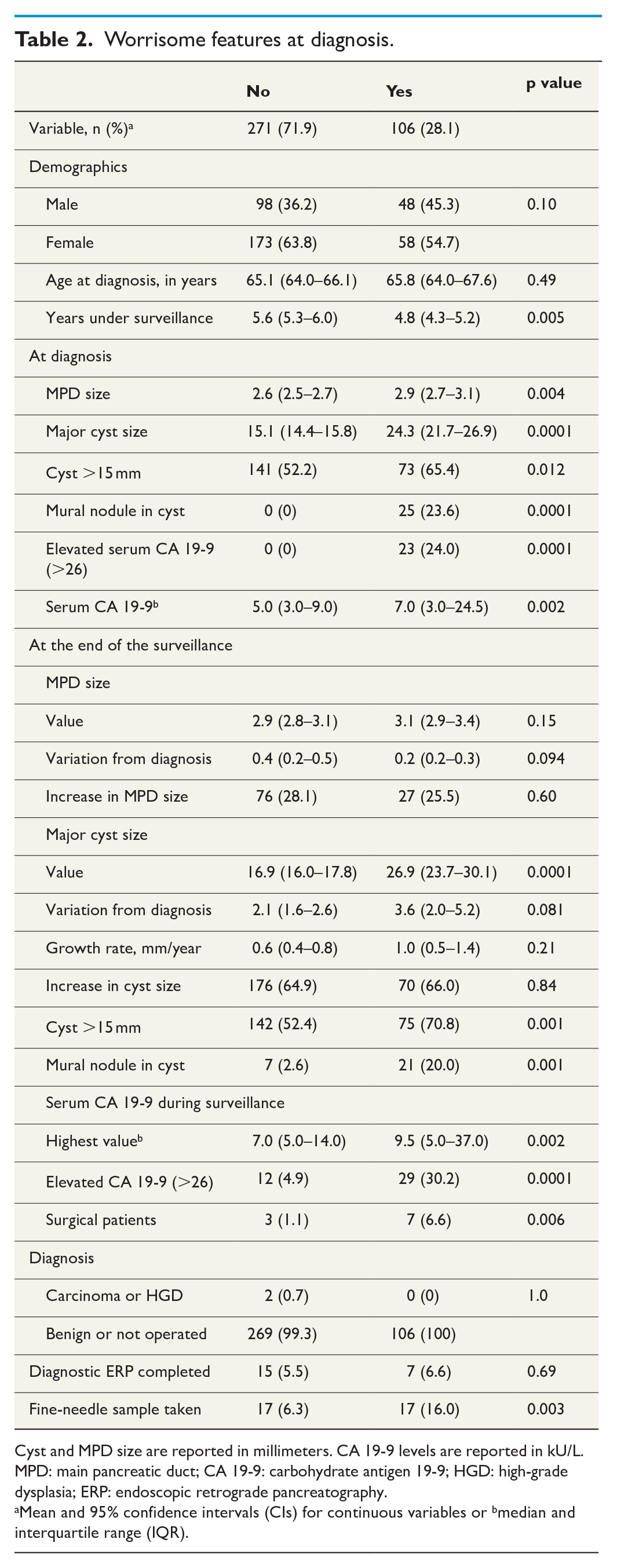
Cyst and MPD size are reported in millimeters. CA 19-9 levels are reported in kU/L.
MPD: main pancreatic duct; CA 19-9: carbohydrate antigen 19-9; HGD: high-grade dysplasia; ERP: endoscopic retrograde pancreatography.
Mean and 95% confidence intervals (CIs) for continuous variables or bmedian and interquartile range (IQR).
New WF/HRS during surveillance
A new WF/HRS developed in 39 (14.4%) patients during surveillance. At diagnosis, their cysts were slightly larger compared to those found in patients with no new WF/HRS (17.7 mm vs 14.6 mm; p < 0.011). We detected no differences based on patient age or gender. During surveillance, patients with new WF/HRS exhibited a significantly larger growth rate per year (1.2 mm vs 0.5 mm; p = 0.013), and a greater total growth in the cyst (4.9 mm vs 1.6 mm; p = 0.001), leading to significantly larger cysts (21.6 mm vs 16.1 mm; p = 0.004). In addition, MPD widening was greater (1.2 mm vs 0.2 mm; p = 0.002), leading to a significantly wider MPD (3.9 mm vs 2.8 mm; p = 0.001). Furthermore, patients with a new WF/HRS had higher mean CA 19-9 levels at diagnosis (10.1 vs 6.2; p = 0.003). Among patients who developed a new WF/HRS, three patients underwent surgery, one of whom had a histologically confirmed carcinoma. In addition, one patient had a pancreatic carcinoma based on radiological findings, but was not fit for surgery. Altogether, 232 patients did not a have WF/HRS at diagnosis or during surveillance, among whom 57% had a cyst <15 mm at diagnosis falling to 50% at the end of surveillance (Table 3).
New worrisome features or high-risk stigmata during surveillance.
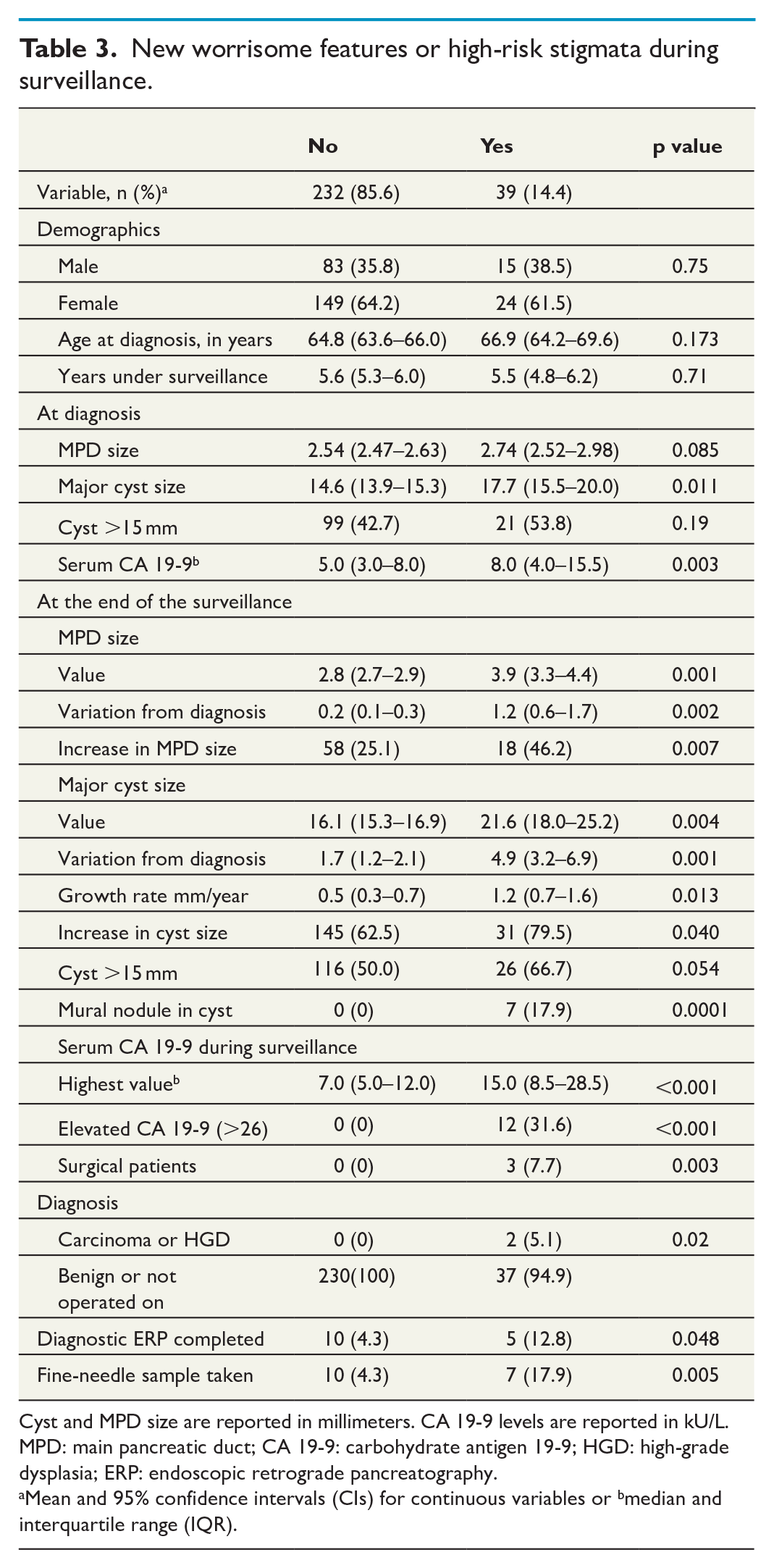
Cyst and MPD size are reported in millimeters. CA 19-9 levels are reported in kU/L.
MPD: main pancreatic duct; CA 19-9: carbohydrate antigen 19-9; HGD: high-grade dysplasia; ERP: endoscopic retrograde pancreatography.
Mean and 95% confidence intervals (CIs) for continuous variables or bmedian and interquartile range (IQR).
Small versus large cysts at diagnosis
More men (63.7%) had a large cyst >15 mm at diagnosis compared to women (42.0%; p < 0.001). In addition, patients with a large cyst were older (67.1 years vs 63.5 years) than those with smaller cysts (p < 0.0001). We observed no association between MPD width and cyst size. However, patients with a large cyst at diagnosis were more likely to have a mural nodule (9.5% vs 3.7%; p = 0.025) or WF (36.8% vs 19.3%) at diagnosis (p < 0.001). During surveillance, large cysts grew more quickly (annual growth rate 1.0 mm vs 0.4 mm; p < 0.001), and were more often the target of FNA (p < 0.001; Table 4). Two carcinomas developed during surveillance in the group of patients with cysts <15 mm, cysts which grew during surveillance. Yet, we found no statistically significant difference in the risk for malignant transformation between small and large cysts.
Cyst size at diagnosis.
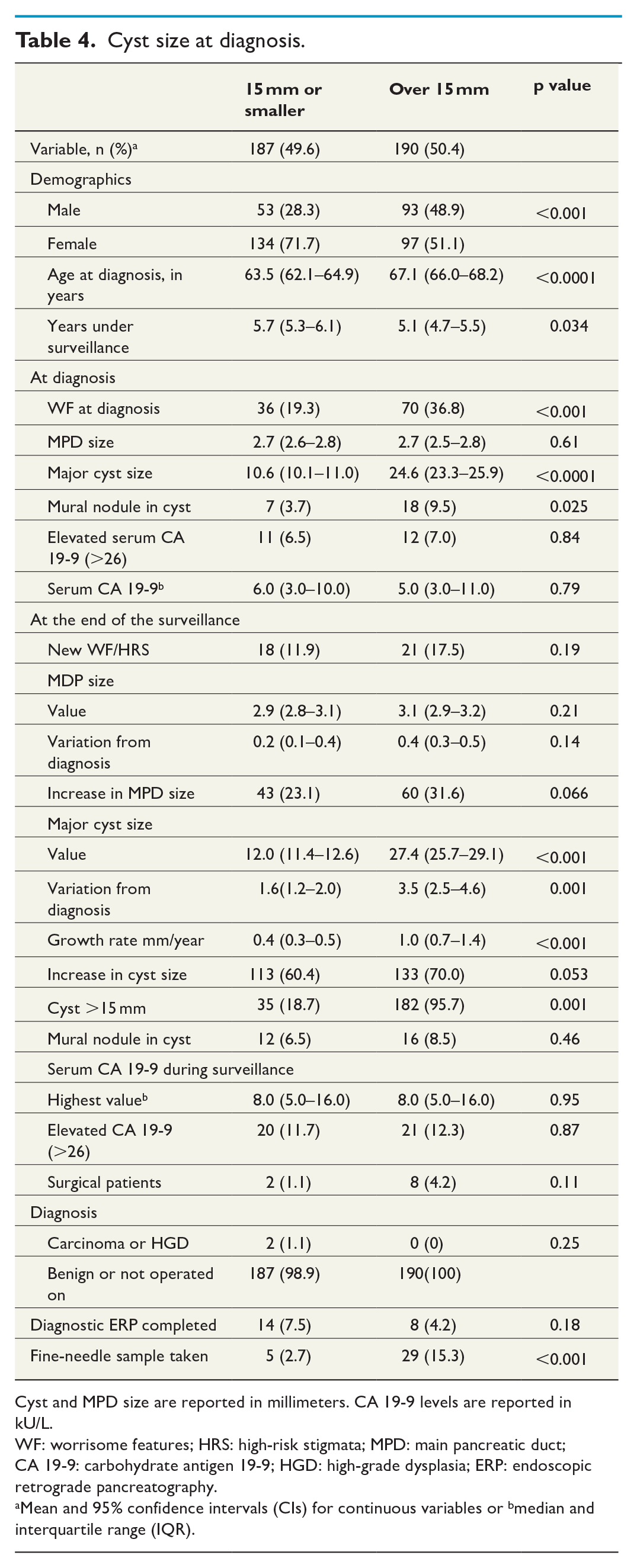
Cyst and MPD size are reported in millimeters. CA 19-9 levels are reported in kU/L.
WF: worrisome features; HRS: high-risk stigmata; MPD: main pancreatic duct; CA 19-9: carbohydrate antigen 19-9; HGD: high-grade dysplasia; ERP: endoscopic retrograde pancreatography.
Mean and 95% confidence intervals (CIs) for continuous variables or bmedian and interquartile range (IQR).
Patients who had a <15 mm cyst at diagnosis were dichotomized based on cyst growth or no cyst growth, whereby 39.5% of cysts <15 mm did not grow during surveillance. Patients with cysts that did not grow during surveillance were older (65.4 vs 62.4 years; p = 0.037). Those whose cysts grew during surveillance exhibited a wider MPD (3.0 mm vs 2.7 mm; p = 0.043) and larger cysts (13.7 mm vs 9.3 mm; p < 0.001) at the end of surveillance. They also more often developed new WF/HRS (16.2% vs 5.3%) during surveillance (p = 0.043). Patients with cysts that did not grow had no HRS during surveillance. Cysts that did not grow appear to have shrunk: mean size of 10.2 mm at diagnosis, shrinking to 9.3 mm at the end of surveillance (Table 5).
Growth in small cyst (<15 mm) during surveillance.
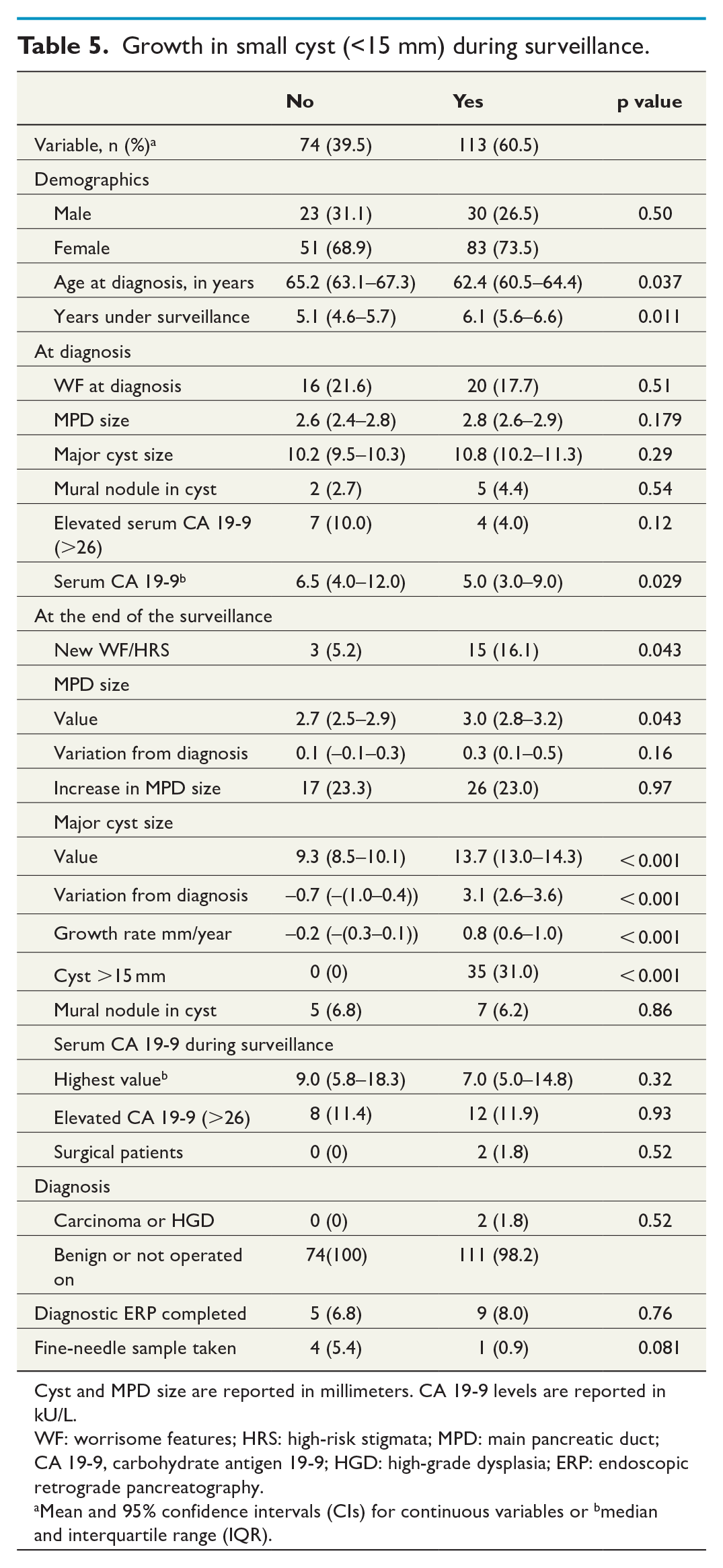
Cyst and MPD size are reported in millimeters. CA 19-9 levels are reported in kU/L.
WF: worrisome features; HRS: high-risk stigmata; MPD: main pancreatic duct; CA 19-9, carbohydrate antigen 19-9; HGD: high-grade dysplasia; ERP: endoscopic retrograde pancreatography.
Mean and 95% confidence intervals (CIs) for continuous variables or bmedian and interquartile range (IQR).
CA 19-9 level during surveillance
We detected an elevated CA 19-9 level in 41 (12.0%) patients at some point during surveillance. Among those with an elevated CA 19-9 level, 70.7% had a WF at diagnosis compared to 22.3% of those with a normal CA 19-9 level (p = 0.0001). During surveillance, 12.2% of patients with an elevated CA 19-9 level underwent surgery compared to only 1.7% of those with normal CA 19-9 levels (p < 0.003). No carcinomas or HGD were detected in patients who never had an elevated CA 19-9 level compared to two patients with an elevated CA 19-9 level (4.9%; p = 0.014; Table 6).
Serum CA 19-9 during surveillance.
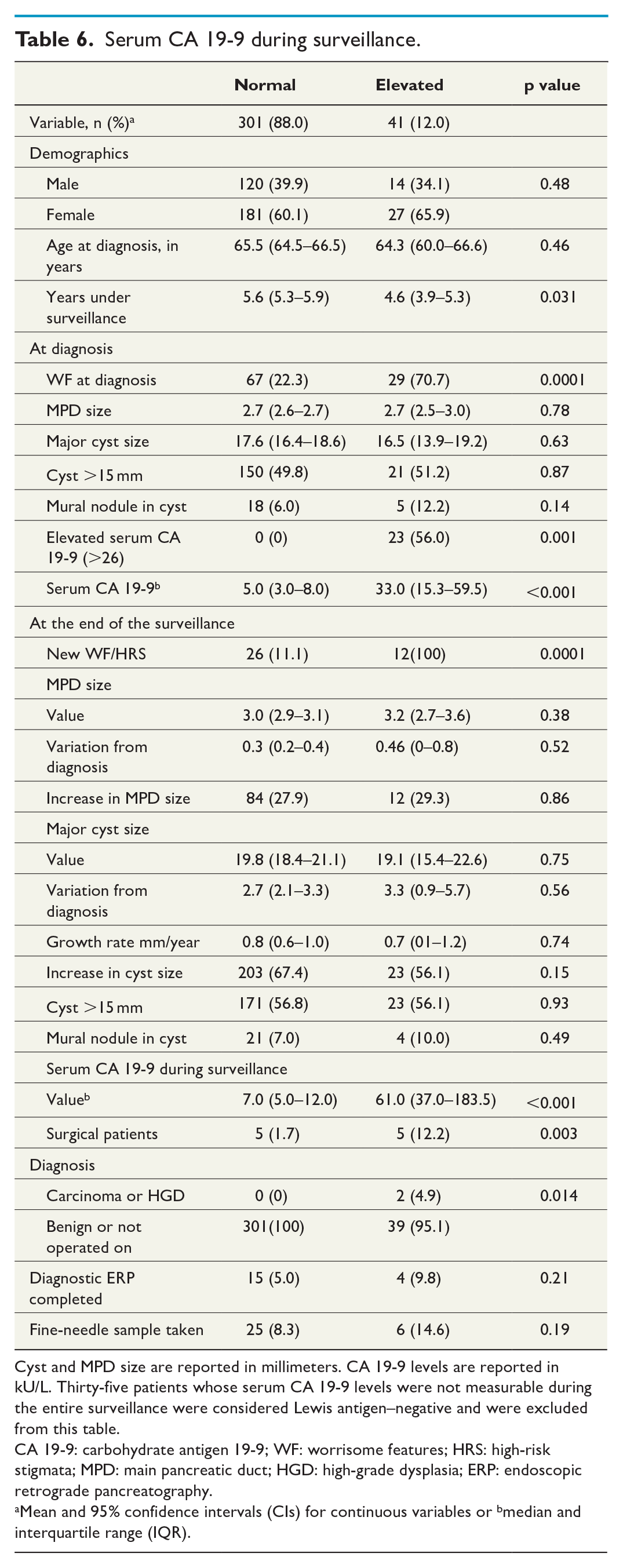
Cyst and MPD size are reported in millimeters. CA 19-9 levels are reported in kU/L. Thirty-five patients whose serum CA 19-9 levels were not measurable during the entire surveillance were considered Lewis antigen–negative and were excluded from this table.
CA 19-9: carbohydrate antigen 19-9; WF: worrisome features; HRS: high-risk stigmata; MPD: main pancreatic duct; HGD: high-grade dysplasia; ERP: endoscopic retrograde pancreatography.
Mean and 95% confidence intervals (CIs) for continuous variables or bmedian and interquartile range (IQR).
Surgical patients
In total, 10 (2.8%) patients underwent surgery during surveillance. The median time from beginning of surveillance to surgery was 3.2 years (IQR: 2.0–4.6). Two pancreatic carcinomas emerged during surveillance, both in patients with cysts <15 mm at diagnosis, but whose cyst grew during surveillance. The other patient underwent surgery and PAD revealed an adenocarcinoma. Another patient was too fragile for surgery, but a metastatic carcinoma was identified radiologically. Four patients had a moderate-grade dysplasia and three had a low-grade dysplasia. Two patients had also main duct involvement and was diagnosed to have mixed-type IPMN at the time of surgery. In one patient, PAD was serous cystadenoma but also BD-IPMN cysts were seen in imaging (Supplementary Table 2).
Discussion
Given the increased use of abdominal imaging, a greater number of IPMNs are detected, most of which are incidentally discovered causing no symptoms. We observed similar findings in our series, where only 5.9% of patients exhibited symptoms related to IPMN. At diagnosis, 28.1% of patients with BD-IPMN had WF. In addition, a new WF/HRS appeared in 14.4% of patients during a mean 5.5 years of surveillance, agreeing with recent reports from other patient series.13,14 The cross-over of 2.7% to resection was similar to some reports,15,16 while significantly higher numbers have also been reported. 5 The development of pancreatic cancer was 0.5% during surveillance, which also agrees with previous studies.15,16 However, our follow-up time of malignant transformation was shorter than in the previous study of Oyama et al. (2020) which reached up to 15 years. 7
Patients with WF at diagnosis were more likely to undergo surgery as expected and to have larger cysts, but during surveillance they did not exhibit indicators of a more aggressive natural course of disease such as a faster cyst growth or MDP widening compared to the remainder of the study population. This underscores the need to identify new biomarkers to better recognize subpopulations requiring alternate surveillance protocols. Patients who developed new WF/HRS during surveillance had a larger cyst at diagnosis with a mean size of 17.7 mm, similar to results previously reported. 17 Furthermore, higher CA 19-9 levels at the time of diagnosis appeared in patients who eventually developed WF/HRS. These patients also had larger cysts at the end of surveillance as expected, as well a wider MPD. The mean growth rate annually in their cysts was 1.2 mm compared to growth rate of 0.5 mm in patients who did not develop WF/HRS.
During surveillance, 232 patients (62%) exhibited no WF or HRS, and had no carcinoma nor HGD. In this population, 57% of patients had cysts <15 mm at diagnosis, decreasing to 50% at the end of surveillance. None of these patients were operated during surveillance nor had elevated CA 19-9. This group could possibly be monitored less frequently in the future.
We also found that elevated CA 19-9 levels during surveillance associated with WF at diagnosis. Overall, 41 patients exhibited elevated CA 19-9 levels at some point during surveillance, 23 of whom had elevated CA 19-9 levels already at diagnosis. During surveillance, 18 more patients had elevated CA 19-9 levels. Among these 18 patients, 4 had a radiological WF finding at diagnosis and 7 more developed radiological WF/HRS in addition to elevated CA 19-9 levels during surveillance. Patients with elevated CA 19-9 levels were more likely to undergo surgery and more likely had a carcinoma or HGD. Interestingly, no carcinomas or high-grade dysplasia were observed among patients with normal CA 19-9 levels. Because IPMN surveillance is targeted at preventing cancer and a lesion featuring a high-grade dysplasia indicates surgery, CA 19-9 measurements could possibly replace some imaging surveillance in very low-risk patients. Interestingly, 5%–10% of the Caucasian population is Lewis antigen–negative and produce no CA 19-9 at all. When no CA 19-9 levels are detected, CA 19-9 screening cannot be used to detect cancer among such patients.
Smaller (<15 mm) cysts at diagnosis appeared not to grow as much as larger cysts during surveillance, exhibiting an annual average growth of 0.4 mm following diagnosis compared to larger cysts that increased by 1.0 mm annually. This result mirrors a previous study by Han et al. from 2018, which found that smaller (<20 mm) cysts grew 0.7–0.8 mm/year compared to larger cysts (>20 mm) that increased by 1.1–1.2 mm/year. 14 In our study, almost 40% of major cysts <15 mm at diagnosis did not grow during surveillance, instead seeming to shrink slightly. Given that the mean difference reached only 0.9 mm between measurements, it may be that the cyst shrinkage originated from a difference in the measurement direction or image plane. Thus, we assume that these cysts remained essentially stable. Furthermore, these cysts also accompanied fewer new WF during surveillance compared to other small cysts that did increase in size. Thus, among the patient group with smaller cysts, if no WF/HRS features emerge, less frequent imaging could be possible in future BD-IPMN surveillance. For instance, in 2020 Ciprani et al. demonstrated that cysts <15 mm without WF/HRS at the time of diagnosis carry a very low risk of malignant transformation, with the risk diminishing over time. 10 In their study, 55% of patients experienced no increase in cyst size. 10
In our study, 62% of patients exhibited no WF or HRS during medium of 5.6 years of surveillance. Of these 50% had <15 mm cyst at the end of surveillance. Almost 20% of our study population had <15 mm cysts that did not grow and had no HRS during surveillance. Since we aimed to find a specific IPMN population which is at the lowest risk of developing malignancy, and thus, a potential target for follow-up discontinuation these patient populations could be target for fewer follow-up in the future. This warrants for further studies reaching over 10 years of surveillance. In our study, the surveillance was still ongoing for 227 patients. It will take an additional 5 years to see the 10-year results for this population.
It remains essential that patients undergo surgery at the right time when they have a high-grade dysplasia—that is, before progression to carcinoma. Operating too early when only mild or moderate dysplasia exists results in surgical-related morbidity, since not all IPMN patients with mild or moderate dysplasia progress to carcinoma. In our study, a total of 10 patients (2.8%) underwent surgery during surveillance. Among them, only one had an adenocarcinoma in histology. This patient did not have WF/HRS at the time of diagnosis. The patient did, however, exhibit elevated CA 19-9 levels (67,500 kU/L) during surveillance and the cyst increased to 3.9 cm in size, exhibiting a growth rate of 6.7 mm/year. The other patient in our study had metastatic carcinoma and was too fragile for surgery, but also had no WF/HRS at the time of diagnosis. After 1.5 years of surveillance, the patient exhibited an elevated CA 19-9 level, up to 9300 kU/L. During subsequent imaging, an unresectable pancreatic tumor with liver metastasis was identified and the patient was referred to oncology. In this study, no carcinomas or high-grade dysplasia were identified in patients with normal CA 19-9 levels. In the future, CA 19-9 measurements could possibly replace some imaging surveillance among BD-IPMN patients who exhibit no WF/HRS features. This study warrants a validation study regarding CA 19-9 among a larger population to clarify our findings.
We should mention some limitations to this study. First, communication of the cyst with MPD was considered a requirement for a working diagnosis of BD-IPMN. For some patients, only CT images were available, which did not feature high-contrast resolution or a sufficiently high sensitivity to identify a mural nodule compared to MRI.4,18,19 Furthermore, mural nodules were categorized as no, yes, or unsure. Unsure was assigned, for example, when moving sediment or a hemorrhage was more likely suspected than a true mural nodule. Finally, the largest cyst size was measured from one target cyst or from the entire size of a multicystic cluster if such were found.
Conclusion
BD-IPMN patients with cysts <15 mm that do not grow and have no WF/HRS require less frequent imaging in the future. If such cyst <15 mm remains stable following 2 years of surveillance, the next controls could possibly take place, for example, every second year.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969221076792 – Supplemental material for A retrospective study of intraductal papillary neoplasia of the pancreas (IPMN) under surveillance
Supplemental material, sj-docx-1-sjs-10.1177_14574969221076792 for A retrospective study of intraductal papillary neoplasia of the pancreas (IPMN) under surveillance by Katarina Johansson, Tuomas Kaprio, Heini Nieminen, Tiina E. Lehtimäki, Eila Lantto, Caj Haglund and Hanna Seppänen in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-2-sjs-10.1177_14574969221076792 – Supplemental material for A retrospective study of intraductal papillary neoplasia of the pancreas (IPMN) under surveillance
Supplemental material, sj-docx-2-sjs-10.1177_14574969221076792 for A retrospective study of intraductal papillary neoplasia of the pancreas (IPMN) under surveillance by Katarina Johansson, Tuomas Kaprio, Heini Nieminen, Tiina E. Lehtimäki, Eila Lantto, Caj Haglund and Hanna Seppänen in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-3-sjs-10.1177_14574969221076792 – Supplemental material for A retrospective study of intraductal papillary neoplasia of the pancreas (IPMN) under surveillance
Supplemental material, sj-docx-3-sjs-10.1177_14574969221076792 for A retrospective study of intraductal papillary neoplasia of the pancreas (IPMN) under surveillance by Katarina Johansson, Tuomas Kaprio, Heini Nieminen, Tiina E. Lehtimäki, Eila Lantto, Caj Haglund and Hanna Seppänen in Scandinavian Journal of Surgery
Footnotes
Author contributions
Conceptualization, K.J., T.K., and H.S.; Data curation, K.J. and T.K.; Formal analysis, T.K. and K.J.; Funding acquisition, K.J., T.K., C.H., and H.S.; Investigation, K.J., T.K., H.N., T.L., and E.L.; Methodology, K.J., T.K., H.N., and H.S.; Resources, H.N. and H.S.; Project administration, K.J., T.K., and H.S.; Validation, K.J., T.K., and H.S.; Supervision, H.S., C.H., and T.L.; Writing—original draft, K.J., T.K., T.L., C.H., and H.S.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: K.J. (Finska Läkaresällskapet, Svenska Kulturfonden), T.K. (K. Albin Johansson Foundation), C.H. (the Finnish Medical Foundation, Medicinska Understödsföreningen Liv och Hälsa), and H.S. (the Finnish Cancer Foundation, the Sigfrid Jusélius Foundation, The Mary and Georg C. Ehrnrooth Foundation). Open access funded by Helsinki University Library.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.