
Abstract
Background and Aims:
Because chronic limb-threatening ischemia (CLTI) is often associated with multilevel arterial disease, it usually requires revascularization at different sites of the limb vasculature. We aim to assess the outcome of the hybrid interventions including open surgical revascularization together with outflow segment percutaneous transluminal angioplasty (PTA) in patients with chronic limb-threatening ischemia.
Material and Methods:
This study included all hybrid outflow-PTA interventions (n = 80) on patients suffering from CLTI performed in Helsinki University Hospital between 2003 and 2015. Follow-up ended on 31 December 2019. Patient data were prospectively collected into our vascular registry and scrutinized retrospectively. Thirty-one patients (39%) suffered from rest pain (Rutherford category IV) and 49 patients (61%) had ischemic ulcers (Rutherford category V–VI). The most common open surgical procedure was femoral endarterectomy (n = 63, 79%) and the most common endovascular procedure was superficial femoral artery percutaneous transluminal angioplasty (n = 65, 81%). Mean follow-up time was 56 months (range: 4 days–183 months).
Results:
Limb salvage was at 30 days—92%, at 1 year—91%, and at 5 and 10 years—86%. Survival and amputation-free survival were at 30 days—93% and 86%, at 1 year—80% and 76%, at 5 years—51% and 48%, and at 10 years—21% and 21%. Wound healing at 3, 6, and 12 months was 48%, 71%, and 87%. Freedom from target lesion revascularization was at 30 days—97%, at 1 year—88%, at 5 years—72%, and at 10 years—66%.
Conclusion:
Hybrid outflow revascularization is an important tool in the vascular surgeon’s armamentarium for treatment of patients with multilevel arterial disease causing chronic limb-threatening ischemia.
Keywords
Background and Aims
Despite advances in risk factor management, patients suffering from chronic limb-threatening ischemia (CLTI) are at risk of significant morbidity and mortality due to cardiovascular events. Patients with CLTI have a 25% mortality rate in the first year after presentation and without revascularization the risk of major amputation is 25% (1). Therefore, big efforts have to be made to revascularize patients suffering from CLTI. There is limited high-quality data about the most suitable revascularization method for treatment of CLTI (2, 3). Traditionally, it has been a choice between endovascular (percutaneous transluminal angioplasty -PTA-) and open surgery. Over the last decade hybrid interventions, which comprise endovascular and open surgery done during the same session, have increasingly been used for treatment of multilevel arterial occlusive disease (4–6). Hybrid interventions combine the strengths of open and endovascular procedures, that is, the superior patency of surgical intervention at the femoral bifurcation and the minimal invasiveness of treating occlusive lesions endovascularly (7–9). Hybrid interventions allow prompt revascularization as opposed to the delay in staged procedures.
A hybrid intervention can be characterized by the location of the endovascular target compared to the open surgery site (10). Outflow PTA refers to a procedure in which endovascular intervention is performed distally to the open surgery, while inflow-PTA refers to a procedure in which endovascular intervention is performed distally to the open surgery.
The knowledge about the outcome after hybrid outflow interventions for treatment of CLTI is scarce. So far the majority of publications on hybrid procedures have focused primarily on femoral endarterectomy combined with aortoiliac PTA (inflow-PTA), and some reports on results on both, inflow- and outflow-PTA procedures (6, 8, 10–15). Moreover, most studies present series of cases with a wide spectrum of etiologies and it is not uncommon to see results on claudicants and CLTI patients presented together. As known, no study has focused on CLTI patients undergoing hybrid outflow interventions. The purpose of this article was to evaluate the long-term results of hybrid outflow revascularization for treatment of CLTI.
Material and Methods
Inclusion Criteria
All hybrid outflow revascularization procedures on CLTI patients (Rutherford IV–VI) (16) with an outflow-PTA component (n = 80) done in Helsinki University Hospital between 1 January 2003 and 31 March 2015 were included in the study.
Hybrid Outflow Technique
All patients had, if not contraindicated preoperatively, a magnetic resonance angiography (MRA). In the case of multilevel disease, including proximal lesions, which are best treated with open surgery, and distal lesions suitable for endovascular treatment, a hybrid outflow procedure was planned. Open surgery was performed prior to the outflow endovascular component. The outflow endovascular procedure was done through an antegrade puncture. First, an angiography was done to assess the lesions in need for endovascular procedures according to preoperative MRA. Thereafter, PTA was done using conventional methods. Stenting was performed only if the result was inadequate (residual stenosis) or if the artery was dissected (bailout-stenting) except in crural arteries.
Methods
Clinical characteristics, operative data, immediate postoperative outcome, and follow-up information including re-interventions, hemodynamic measurements, evolution of ischemic ulcer, and leg salvage were prospectively collected into our institutional vascular registry (HUSVASC) and scrutinized retrospectively. The last follow-up datum collected was from 31 December 2019. Follow-up included clinical assessment, ankle-brachial index (ABI), and toe-pressure (TP) measurements and ultrasound investigation when needed at 1, 6, and 12 months or until the patient was free from any CLTI-symptoms, that is, no rest pain and the ischemic wound had healed. Survival data were retrieved from the Finnish national population registry, Statistics Finland.
Endpoints
The main outcome of the study was limb salvage. Secondary outcomes were patient survival, amputation-free survival (AFS), freedom from target lesion revascularization (TLR), wound healing, and postoperative complications.
Major amputation was defined as any amputation of the lower limb above ankle level. Wound healing was defined as complete epithelization of all ischemic wounds of the leg. The wound was considered unhealed if the patient had a major amputation due to ischemic foot-ulcers or a re-revasularization with bypass was performed for treatment of occlusions in the endovascularly treated segment. Technical success of the endovascular procedure was classified as good (residual stenosis 0%–20%), acceptable (20%–50%), or insufficient (>50%) based on blood flow measurement (volume per minute) and completion angiogram. TLR was defined as the re-revascularization procedure performed either with balloon angioplasty alone or by the means of a secondary bypass on those patients that had CLTI-symptoms due to re-occlusions or re-stenosis after the primary operation. Criteria for re-intervention included rest pain or clinical deterioration of the ischemic wound based occlusion or stenosis. Re-stenosis was defined as a lesion with more than three-times-increase in the peak systolic velocity detected with ultra sound scanning or angiographic diameter reduction of >50%. Postoperative complications (within 30 days from the hybrid intervention) include myocardial infarct diagnosed by ischemic changes in the electrocardiogram together with acute troponin elevation, stroke causing a new neurological symptoms and diagnosed by brain computer tomography scan, acute renal failure demanding dialysis, and sepsis diagnosed by positive blood cultures. Deep wound infection was defined as an infection at the open surgery site during the follow-up requiring surgical debridement.
Statistics
Categorical variables are shown as percentages. Continuous variables are expressed as means and range. All data were gathered using EXCEL version 2016 and the statistical analyses were performed using SPSS version 22.0 (17) and R version 3.6.0 (18). Kaplan–Meier method was used for the analysis of leg salvage, survival, AFS, TLR, and ulcer healing. We use the weighted median of medians as core technique in aggregate data meta-analysis to compare our sample’s ulcer healing time with that of the literature using the weighted median function in the spatstat package.
The study protocol was approved by the Institutional Review Board of Helsinki University Hospital (Department of Surgery).
Results
In total, 80 outflow-PTA hybrid procedures were performed on patients suffering from CLTI. Demographic characteristics of the cohort are shown in Table 1. Mean follow-up was 55.9 months (range: 4 days to 182.7 months). The most common open surgical procedure was femoral endarterectomy (n = 63, 79%) and the most common endovascular procedure was superficial femoral artery PTA (n = 65, 81%). Surgical interventions and endovascular target arteries are presented in Table 2.
Demographics..
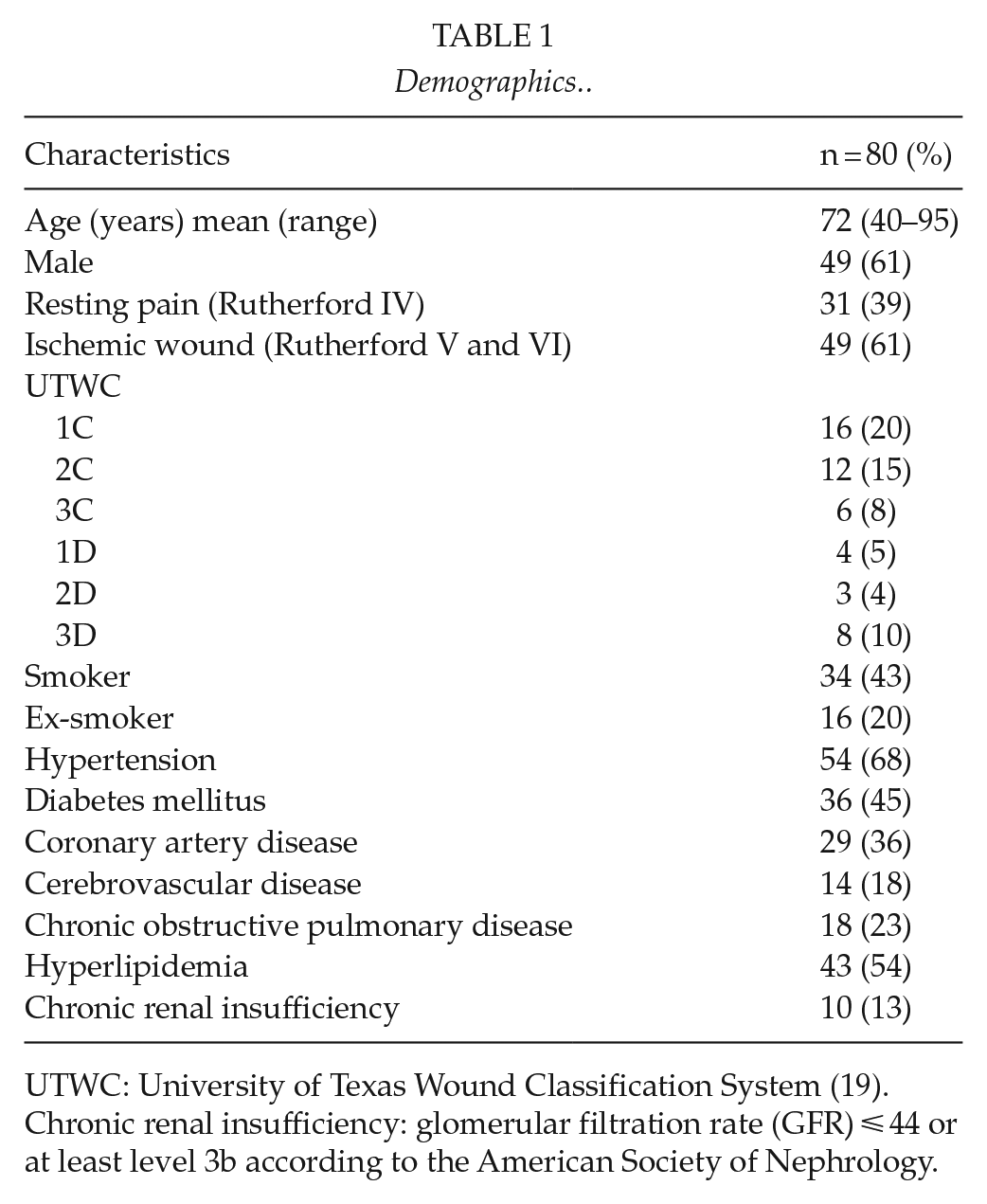
UTWC: University of Texas Wound Classification System (19).
Chronic renal insufficiency: glomerular filtration rate (GFR) ⩽ 44 or at least level 3b according to the American Society of Nephrology.
Open surgical and endovascular procedures with their frequency.
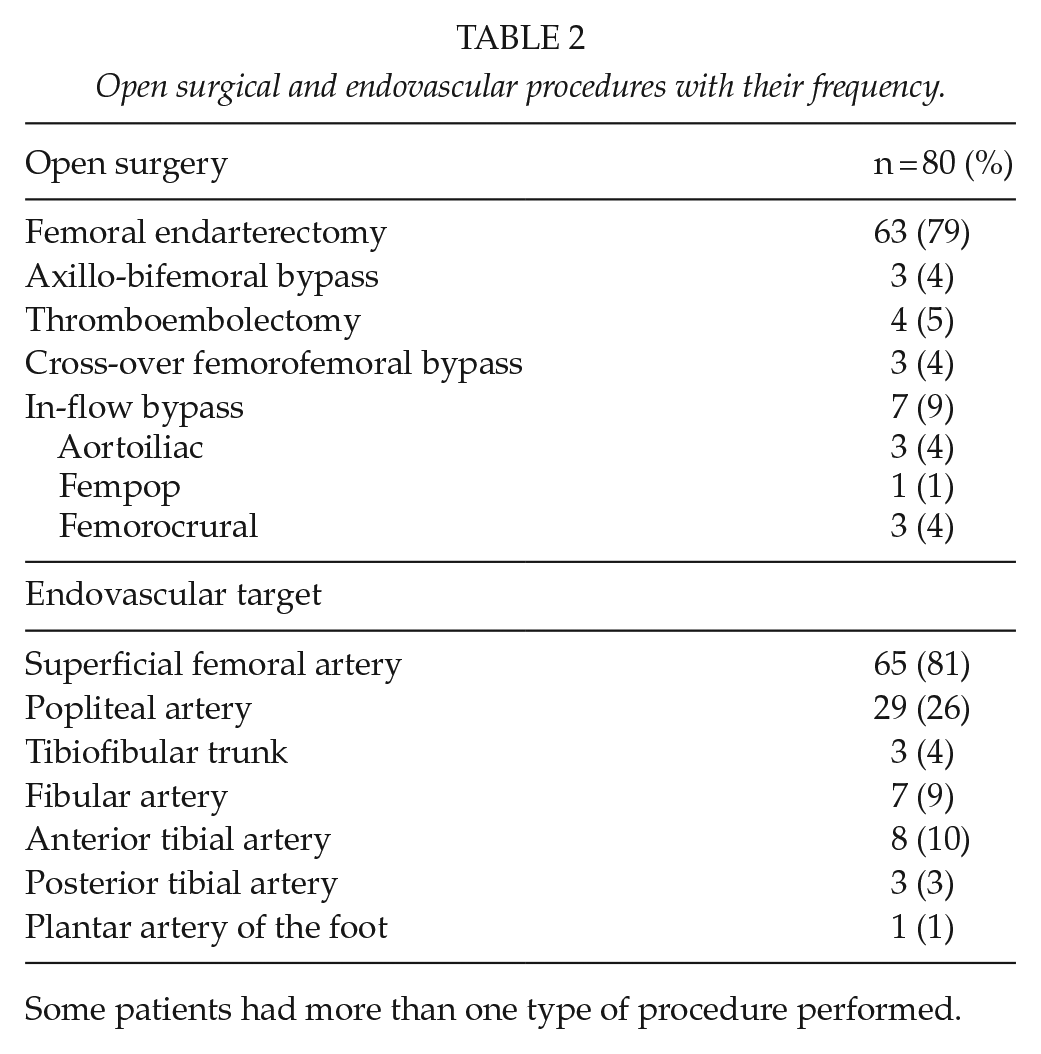
Some patients had more than one type of procedure performed.
Limb salvage was at 30 days—92%, at 1 year—91%, and at 5 and 10 years—86% (Fig. 1). The reasons for the ten major amputations that happened during the follow-up were in three of the cases, occlusion of the treated segment or graft with no further possibility of re-revascularization. Five patients had extensive tissue loss that led to amputation despite of successful hybrid outflow operation. And finally, two patients with ischemic wounds that healed after revascularization had an amputation later on due to relapsing of CLTI.
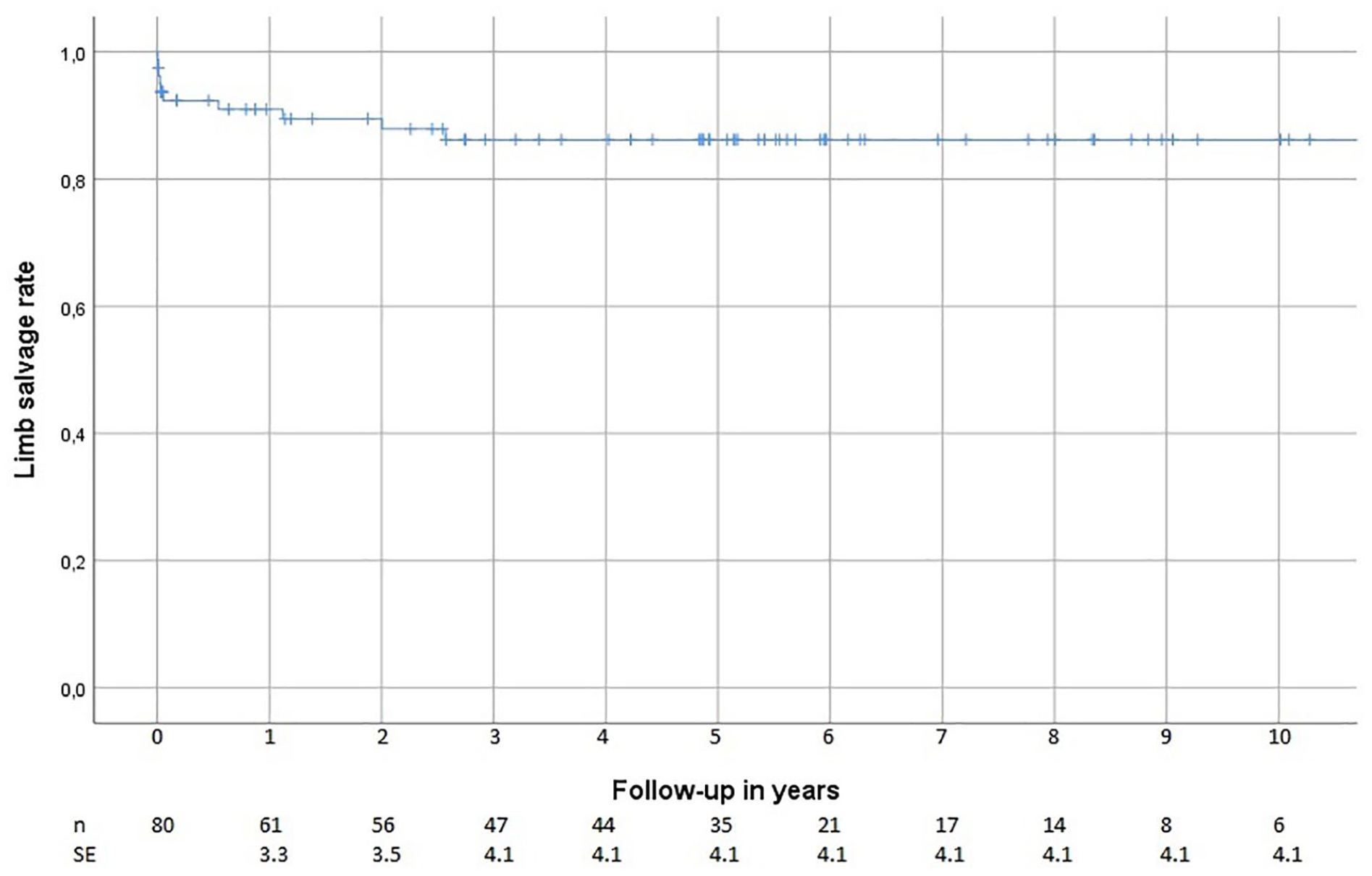
Kaplan–Meier estimator of limb salvage after hybrid outflow revascularization.
Patient survival was at 30 days—93%, at 1 year—80%, at 5 years—51%, and at 10 years—21%. The correspondent values for AFS was 86%, 76%, 48%, and 21% (Fig. 2). Two patients (2.5%) suffered from an acute myocardial infarction, three patients (3.9%) had a stroke, two (2.5%) developed acute renal failure, and two (2.5%) had positive blood cultures and symptoms of sepsis within 30 days of the hybrid procedure.
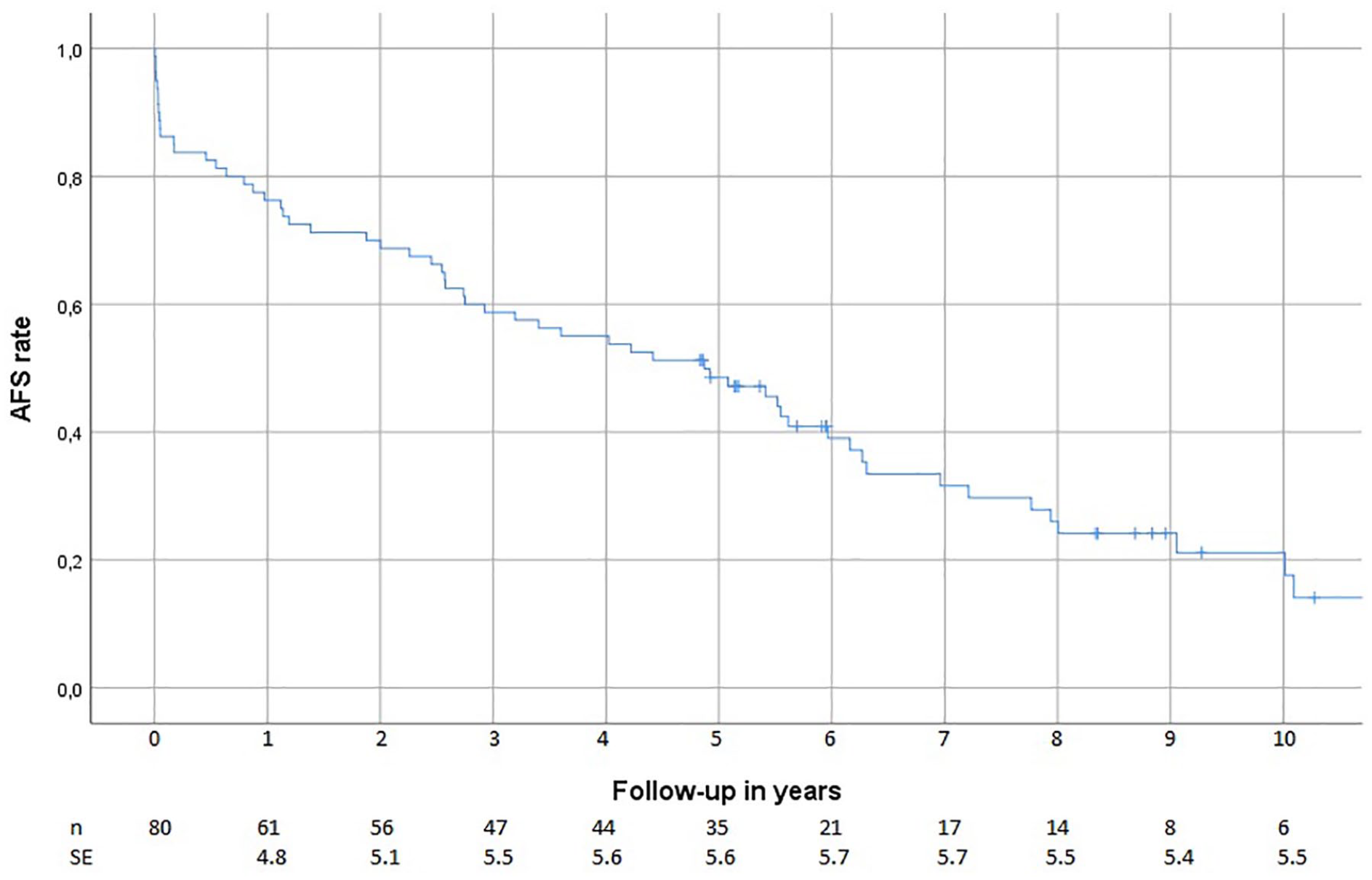
Kaplan–Meier estimator of the amputation-free survival (AFS) after hybrid outflow scularization.
Freedom from TLR was at 30 days—97%, at 1 year—88%, at 5 years—72%, and at 10 years—66% (Fig. 3). In total, 16 (20%) patients developed new critical limb ischemia (CLI) symptoms during the follow-up and had a re-intervention. Of them, 10 (12.5%) were treated with endovascular re-revascularization of the target outflow tract, whereas another 6 (7.5%) underwent secondary open repair due to occlusion of the outflow segment.
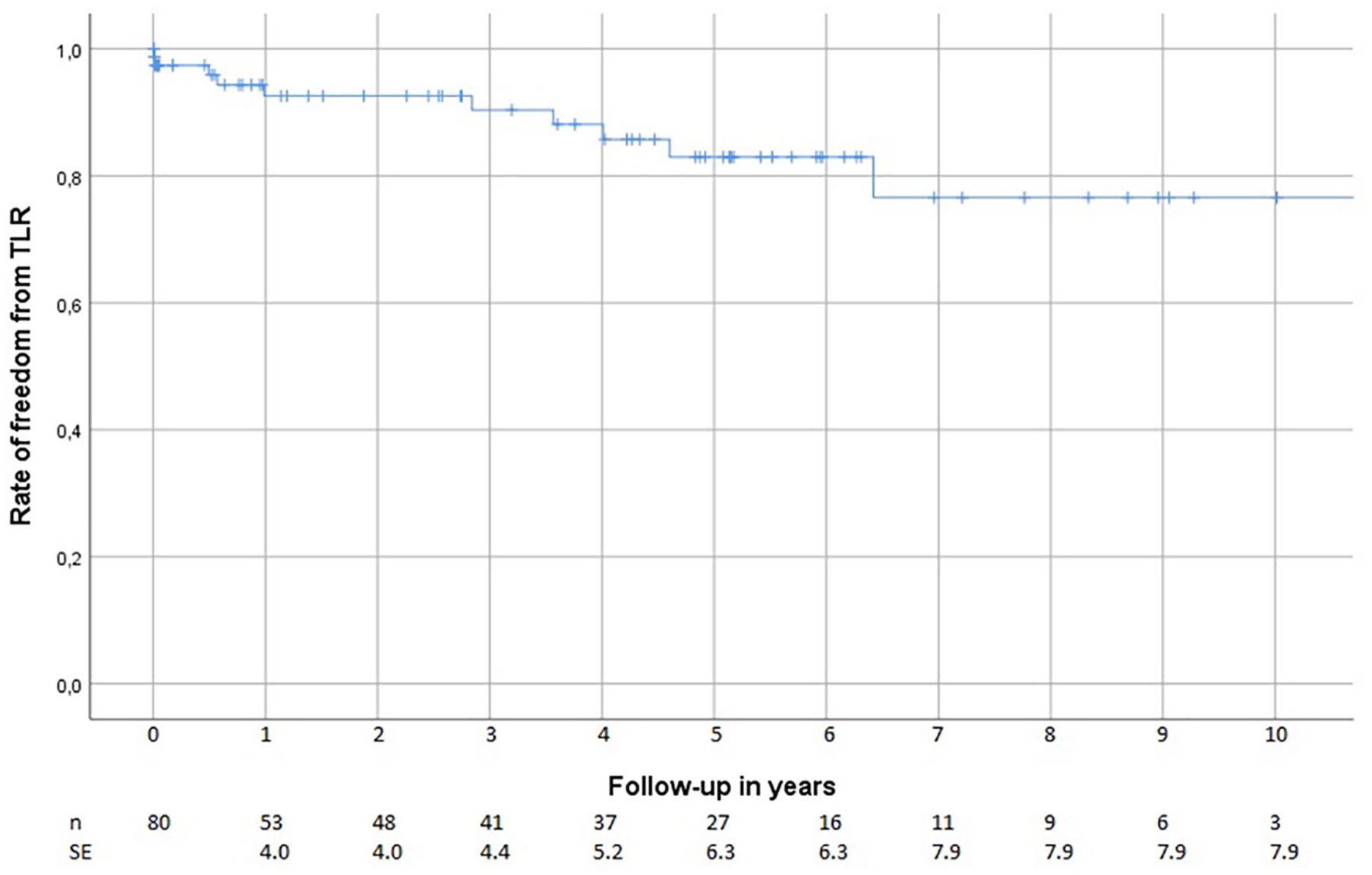
Kaplan–Meier curve of the freedom from target lesion revascularization (TLR) after hybrid outflow revascularization.
The operating surgeon defined the initial success of the endovascular procedure based on blood flow measurement (volume per minute) and perioperative angiography and as “good” in 79% operations (n = 63), “acceptable” in 16% (n = 13), and “insufficient” in 5% (n = 4).
Preoperative mean ABI was 0.45 (range: 0–1.72), postoperative mean ABI was 0.9 (range: 0–2.19), and the postoperative increase in mean ABI was 0.43 (range: 0–1.36). Mean preoperative TP was 27 mmHg (range: 0–69 mmHg), postoperative mean TP was 60 mmHg (range: 0–128 mmHg), whereas the mean TP increase was 33 mmHg (range: −26 to 128 mmHg).
Rutherford category V accounts for most of the wounds (n = 43), whereas six patients suffered from more extensive tissue loss corresponding to Rutherford VI.
Wound healing at 3, 6, and 12 months was 48%, 71%, and 87%, respectively (Fig. 4). Of the 13 patients whose ischemic lesions were not confirmed healed, five died within 6 months of the operation and two were lost to follow-up before complete healing of the wound was documented. No amputation or vascular operation was performed on them ever after. Five underwent major amputation for irreversible ischemia, and finally one had an infrainguinal bypass. Median wound healing time was 111 days after the hybrid outflow procedure.
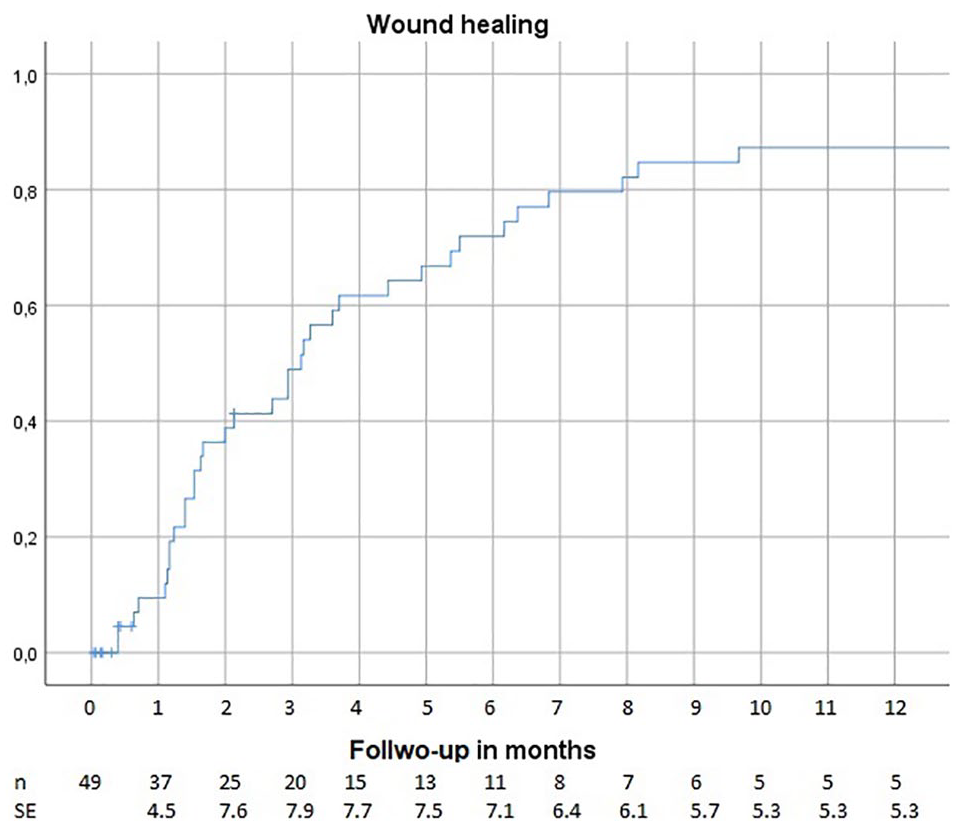
Estimated wound healing rate over time after hybrid outflow treatment.
One (1.3%) of the patients had a deep surgical wound infection during the follow-up period.
Discussion
The use of vascular hybrid procedures has been reported to increase constantly during the last years (6, 20, 21). In order to extract more concrete conclusions from the data, we focused on a cohort made entirely of CLTI patients that underwent lower limb revascularization including outflow endovascular procedure. We did not find any publication focusing solely on CLTI patients undergoing hybrid outflow interventions.
The largest series published on hybrid operations including outflow PTA to our knowledge is from Baroi et al. (22), who reported results of 94 hybrid procedures. In their study, 11 major amputations during 3.6 years were performed on a cohort of 94 patients with a mix of claudicants and other stages of peripheral artery disease (PAD). They reported separately the limb salvage in patients suffering CLI: after 44 months of follow-up, the limb salvage rate was 73% compared to the estimation of 86% in our cohort. Joh et al. (23) analyzed open versus hybrid revascularization of multilevel lower extremity arterial disease. They found an overall limb salvage of 97% and an overall survival rate of 93% in a mean follow-up of 10 ± 9 months. Our cohort exclusively composed by CLTI patients had worse limb salvage and survival rates at 10 months: 91% and 84%. The difference can be explained by the fact that Joh and colleagues included a significant proportion of claudicants (24%) in the hybrid group, which represent a less advanced state of the PAD disease than CLTI and is associated with a better prognosis (1, 2). Dosluoglu et al. (12) classified hybrid surgery as simple when the endovascularly treated segment was TASC A or B and complex when it was TASC B or C according to the TransaAlantic InterSociety Consensus. In the simple hybrid group, the 1-year limb salvage was 94% and the 3-year limb salvage rate was 80%. However, in the complex group, there were no amputations. A majority of the endovascular procedures were suprainguinal in the study by Dosluoglu et al. compared to our study where all patients had infrainguinal occlusive atherosclerotic lesions.
The long-term limb salvage rate was good in our study, 86% at 5 and 10 years. Almost no amputations were performed after 1 year. Once the ischemic wound has healed, tissues need of blood supply decreases to normal baseline and re-occlusion of the outflow does not necessary lead again to CLTI. This might explain also the low rate of re-revascularizations. The high long-term leg salvage and freedom from target lesion revascularization in our study may also reflect the importance of revascularizing the profunda femoris artery. Femoral endarterectomy is known to be a durable revascularization procedure (6, 8, 9). Even if the infrainguinal arteries re-occlude later on, a patent femoral profunda artery may provide sufficient blood flow to maintain the viability of the leg avoiding amputation.
A remarkable finding in our study was that the median ulcer healing time was 111 days and almost 90% achieved complete ulcer healing at 12-month follow-up. Few publications about limb revascularization report complete healing of the ischemic wound (24). As known, no study has reported wound healing rate after hybrid outflow revascularization. Okazaki et al. (25) published their results after surgical or endovascular revascularization of ischemic limbs: 64% ulcer healing at 12 months and their median ulcer healing time was 144 days. Azuma et al. (26) published in 2014 a thorough review of the literature on ulcer healing after revascularization. Among the many studies reporting limb salvage, they found only 17 (0.1%) reporting data on wound healing. In these, 1-year wound healing rates vary between 47% and 87%, we calculated the weighted median healing time of them to be 186 days ranging from 64 to 267 days (26). Wound healing is dependent on several factors including patient comorbidities and local ulcer factors as depth, size, localization, and presence of infection. This explains the large variations in wound healing time noticed in different studies (27). Neither hybrid procedure was included in Azuma’s review nor did we find in the literature any publication about hybrid procedures reporting complete ulcer healing as an outcome.
According to our findings, the treatment of CLTI patients with hybrid outflow procedures yields good limb salvage, but the AFS is compromised due to the high mortality rate and global atherosclerotic burden that accompanies CLTI (28). The epidemiological baseline of our cohort including elderly people, 63% with a smoking history, 45% diabetics, and 36% patients diagnosed with coronary artery disease represent a fragile population with high mortality according to current reported epidemiological characteristics of CLTI patients (29–31). In the BASIL trial, the AFS at 3 years was 52% in patients randomized to the infrainguinal bypass group and 57% in patients assigned to endovascular treatment for severe limb ischemia (3). This compares to 60% in our patient sample. The perioperative morbidity was low and 30-day mortality rate was 7% which is equal or better than bypass procedures reflecting the mini-invasive nature of hybrid outflow interventions (14).
Our results indicate that hybrid outflow procedures are an important option in individuals with multilevel PAD. Fluoroscopic interventions are not risk-free, radiation hazard to patient and staff, as well as potential reactions to contrast exist. Patient selection and detailed preoperative planning are essential to achieve good results. All patients suffering from CLTI may not be suitable for hybrid outflow revascularization, that is, due to very widespread arterial occlusions. For some, the surgeon must make the choice between open and endovascular procedure. BASIL-2 and BESTCLI studies seek further evidence on the treatment of patients suffering from CLTI, but neither of these two trials focus on hybrid interventions. Now, treatment modality should still be chosen according to patient characteristics and expected gain of the revascularization.
Limitations of The Study
The weaknesses of the study include its retrospective nature and the relatively small number of patients. There were several combinations of open and endovascular outflow procedures including femoral and crural PTA as well as distal bypasses to different levels, again the small sample does not allow subgroup analyses.
The influence that the characteristics of the ischemic wounds have on the outcome was not analyzed due to the limited number of patients with ischemic wounds. Also the small size of our patient’s sample precludes meaningful analyses of comorbidities or factors impacting the outcome.
The arterial occlusive lesions were not classified as there is no classification comprising lesions from iliac to the crural arteries. Direct comparison hybrid outflow interventions with other revascularization methods are to be cautious. Randomized trials on hybrid outflow operations and other revascularization methods have not been done and would be difficult to execute as this group of patients have severe limitations on the kind of treatment they can endure. Comparison of staged versus simultaneous or hybrid versus only open operations has not been addressed here; such an approach might be ethically questionable as it would mean performing sub-optimal and/or delayed revascularization in critically ischemic limbs.
Conclusion
Open revascularization combined with endovascular outflow procedures is a tempting alternative in the management of multilevel PAD in CLTI patients. Hybrid outflow interventions seem to be particularly promising in saving critically ischemic limbs and promote healing of ischemic wounds.
Footnotes
Acknowledgements
The authors would like to thank Pablo Valledor Pellicer for his technical assistance with statistics and the analysis using R.
Author contributions
J.S.S., M.S., R.H., and K.H. were involved in the collection of data; J.S.S., M.S., and R.H. were involved in writing; and J.S.S. and M.S. were involved in data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.