
Abstract
Keywords
What is critical limb ischemia (CLI)?
Critical limb ischemia (CLI), also known as chronic limb-threatening ischemia (CLTI), is the most severe form of peripheral artery disease (PAD). PAD occurs due to blockages in the leg arteries due to atherosclerosis or plaque build-up. Depending on the location and severity of these blockages, people with PAD may have no symptoms or have pain with walking or foot ulcers that do not heal due to poor blood flow. To learn more about PAD, read the Vascular Disease Patient Information Page on ‘Peripheral Artery Disease’. 1
With CLI, leg artery blockages are so severe that sufficient blood flow cannot reach the legs and feet. This decrease in blood flow can cause a number of symptoms, including pain in the foot or leg even without walking, breakdown of the skin due to decreased blood flow, and inability to heal a superficial or deep injury to the foot. If the skin of the foot cannot heal, then infection or gangrene can develop and eventually lead to amputation. Figure 1 shows an example of a patient with a foot ulcer due to CLI.

Example of a toe ulcer due to critical limb ischemia.
What are the risk factors for PAD and CLI?
The risk factors for PAD and CLI are similar to the risk factors for coronary artery (heart) disease. These include older age, smoking, high cholesterol, chronic kidney disease, hypertension, and diabetes. Smoking greatly increases the risk of CLI due to chronic inflammation in the arteries of the legs. It is never too late to quit smoking – studies have shown that quitting smoking, even after the development of CLI, lowers the chances of leg amputation and death. 2 To learn more about quitting smoking, read the Vascular Disease Patient Information Page on ‘Smoking Cessation’. 3 High cholesterol is a major risk factor for CLI, and all patients with CLI should be treated with statin medications to reduce the risk of heart attack and amputation. Approximately two-thirds of patients with CLI have diabetes. Medical control of blood sugar levels may help decrease the risk of amputation and improve wound healing. 4
What are the typical symptoms of CLI?
Symptoms of CLI frequently involve pain in the foot or leg that is worse at night due to decreased blood flow when lying down. This pain can be so severe that sleeping can be difficult or interrupted. Patients with CLI may actually dangle the leg over the side of the bed while sleeping or need to stand up, because gravity increases the blood flow to the leg. Patients with CLI may also have pain in the legs or calves when walking (claudication), although not every patient with CLI will have claudication. Another symptom of CLI is an ulcer or sore on the foot. Identifying these ulcers early is important for timely diagnosis and treatment. Patients with PAD who develop foot sores or ulcers should immediately schedule an appointment with a vascular specialist for evaluation.
Does an ulcer on the foot always mean CLI?
Not necessarily. There are many categories of foot ulcers, including arterial ulcers, venous ulcers, and neuropathic ulcers. Arterial ulcers are seen in CLI, and they are usually located on the toes, between the toes, or near the edge of the foot or on the outside of the ankle. Venous ulcers are caused by decreased blood return by the veins. These ulcers are typically located on the inside of the ankles, but they can also occur on the front of the leg. Neuropathic ulcers occur because of decreased feeling in the feet (neuropathy) and thus may go undetected. These ulcers usually form at areas of foot injury, including the bottom of the foot. It is important to recognize that these ulcer types can overlap as well. For example, a patient with diabetes and neuropathy might originally develop an ulcer from trauma that is not recognized due to the neuropathy, but decreased blood flow from an artery blockage could make this ulcer worse and prevent healing. The causes leading to a foot ulcer are summarized in Figure 2. For this reason, it is important to have a specialist evaluate every foot ulcer in a prompt manner. 5
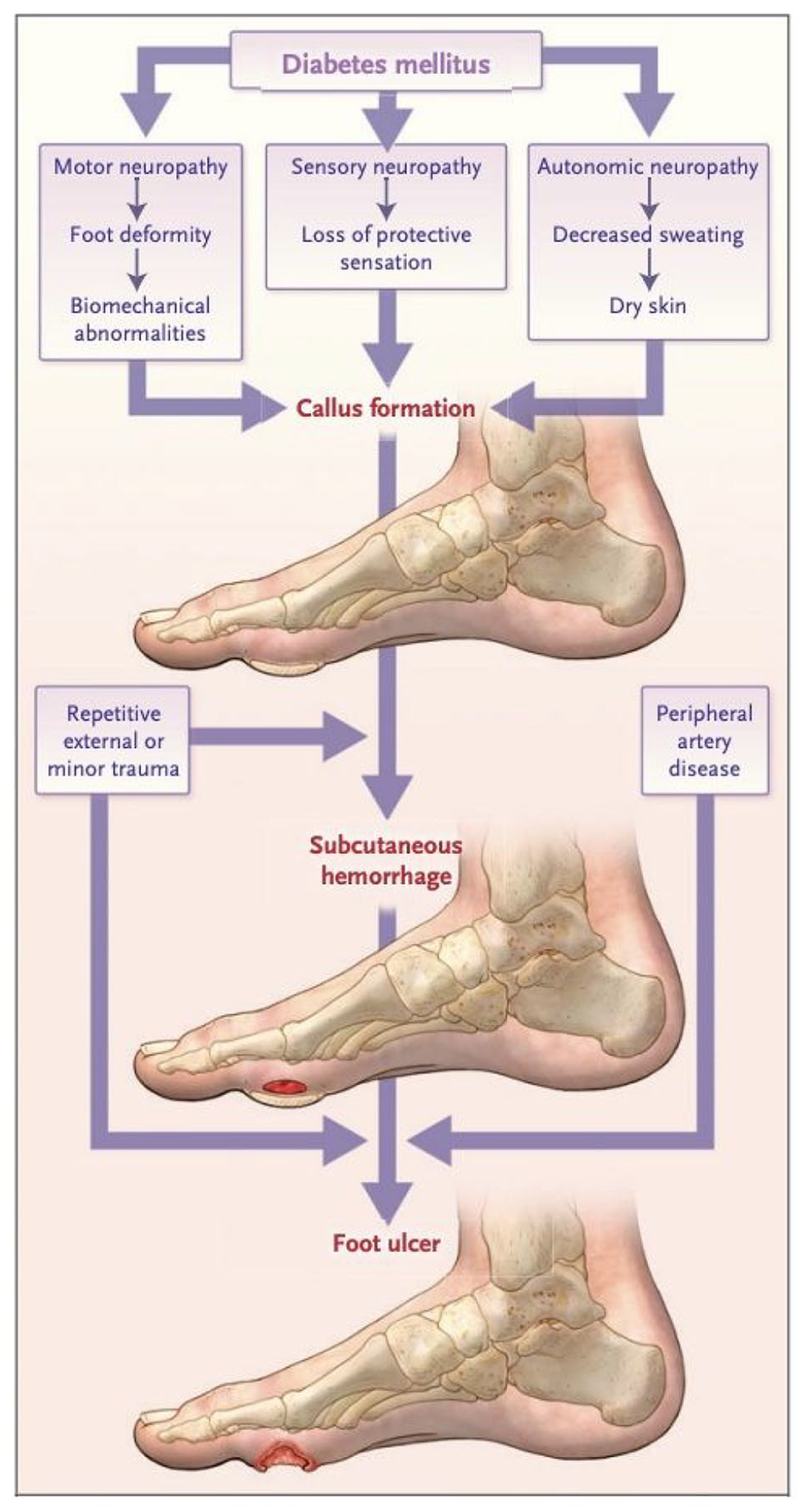
Pathway of diabetic foot ulcer occurrence and recurrence and the effect of critical limb ischemia.
How common is amputation in patients with CLI?
Approximately 200,000 amputations are performed in the United States each year due to CLI. Only a small percentage of patients with PAD develop CLI but having CLI is associated with amputation rates of more than 25% per year. Although some patients with CLI may require amputation due to extensive gangrene or infection of the foot, many of these amputations could be avoided by early evaluation and careful analysis of the blood flow to the leg and foot. Several studies have shown that there are health care disparities in CLI care for minority populations, in part because of delays in diagnosis of the CLI.
What tests are performed to diagnose CLI?
Multiple tests may help verify that leg pains or leg ulcers are the result of CLI. These tests can include the ankle–brachial index (ABI), toe–brachial index (TBI), duplex ultrasound (DUS), computed tomographic angiography (CTA), magnetic resonance angiography (MRA), and diagnostic angiography. The ABI is a noninvasive test that compares the blood pressure in the ankle arteries to the blood pressure in the arm arteries. If there is no blockage in the leg arteries, the ankle blood pressure should be slightly higher than the arm blood pressure. Patients with CLI typically have ankle pressures that are severely reduced to 50% or less than arm pressures. However, it is also possible to have CLI and a normal ABI, due to variations in the anatomy of blood flow to the foot and location of the ulcer. The TBI is similar to the ABI, except that it measures pressure in the great toe. This measurement can help predict wound healing and is also especially helpful in cases of vessel calcification, when the ankle arteries may not be compressible by the blood pressure cuff. DUS uses ultrasound images to assess the blood flow in the leg arteries. DUS is complementary to ABI because it can identify the locations of blockages, which can be helpful with planning a procedure. CTA and MRA are more advanced imaging techniques that also identify the location of blockages and can help with procedural planning. Diagnostic angiography involves inserting a small catheter in the leg artery under local anesthesia. Contrast is then injected through the artery, thereby diagnosing the severity and level of artery blockages. This procedure is often done at the same time as angioplasty of the arteries, which can be performed through the same small catheter in the artery.
Which doctors treat patients with CLI?
The long-term treatment of CLI requires a collaborative approach for optimal care. The healthcare team may include vascular specialists to restore the blood flow (vascular surgeons, interventional cardiologists, interventional radiologists); vascular medicine specialists to help reduce the medical risk of cardiovascular complications; podiatrists and other wound care specialists to manage wound care and minimize the level of amputation; endocrinologists to manage diabetes if present; infectious disease specialists to treat infections of the skin or bone; nephrologists to help manage kidney complications; and prosthetic specialists to help with prosthesis fitting and rehabilitation. 6 Given the importance of managing both the blood flow and foot complications (such as wounds and deformities causing wounds), this team concept has been termed ‘toe and flow’, and is summarized graphically in Figure 3.
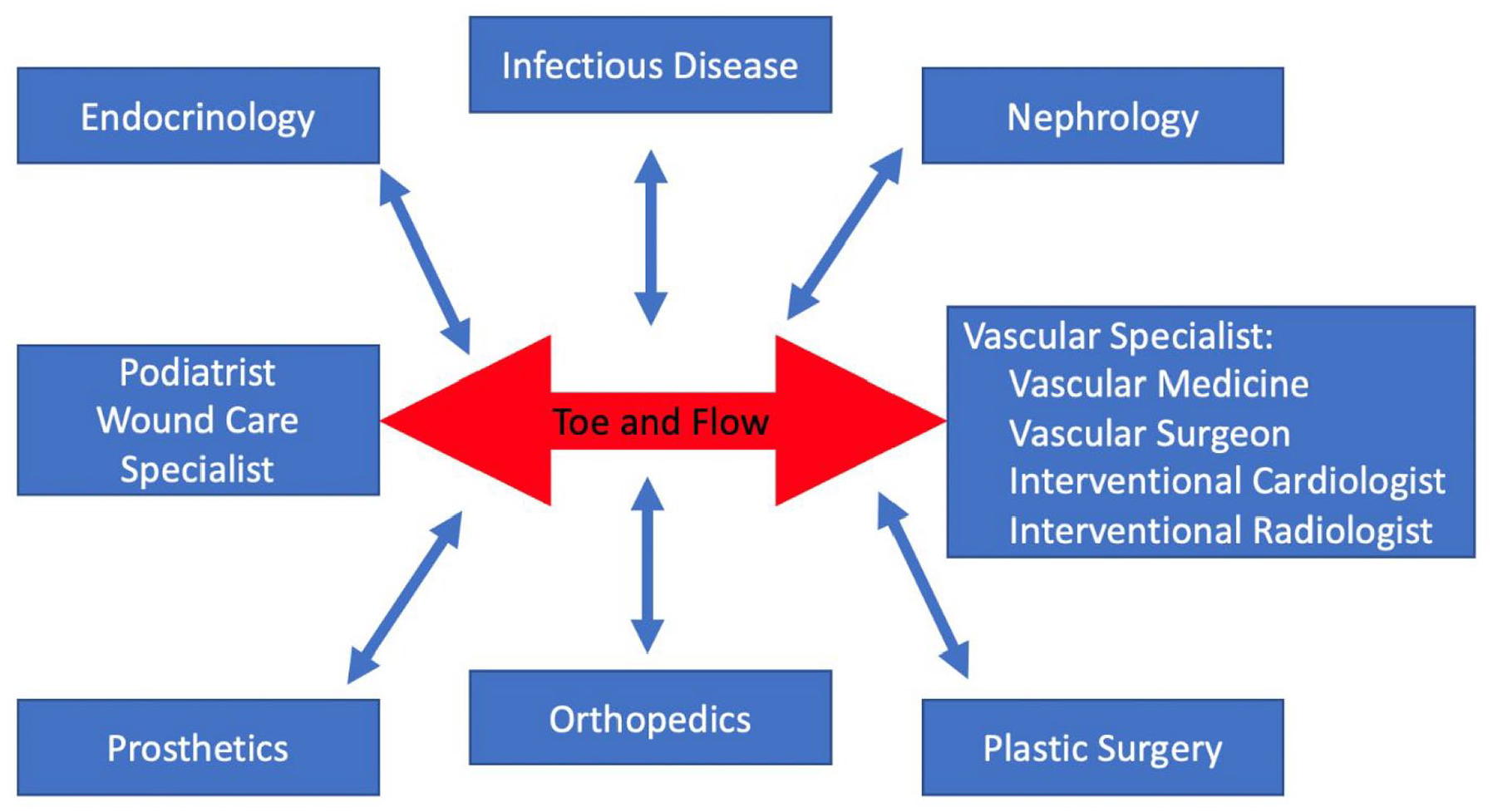
Multidisciplinary care for CLI. Optimal care of CLI focuses on both the ‘toe’ with wound care, and the ‘flow’ by restoring blood flow to the foot. In addition to vascular specialists, several other medical professionals are important to manage the complex medical problems that patients with CLI tend to have.
What are the treatment options for CLI?
The primary treatment for CLI is to restore blood flow to the affected leg in order to relieve symptoms of leg pain and provide enough blood flow to heal any leg and foot wounds. Revascularization (blood flow restoration) can consist of surgical bypass or minimally invasive techniques referred to as angioplasty. Bypass surgery involves rerouting blood flow to ‘go around’ the blockage with either a vein or a prosthetic graft. Angioplasty uses balloons or stents to open blocked arteries from the inside. The decision to perform bypass versus angioplasty is based on several factors, including the location and length of the artery blockages, the risk of bypass surgery, and patient preference. Angioplasty techniques are increasingly used for the treatment of CLI because this approach is less invasive and has a much shorter recovery period. In a typical angioplasty procedure, the patient may be able to go home the same or next day, thereby avoiding a long hospital stay. Ongoing studies are comparing the surgical versus angioplasty-based treatment of CLI. 7
Apart from restoring the blood flow, how can amputation be avoided?
Although revascularization is extremely important to help promote better blood flow and wound healing, wound care after revascularization matters just as much. Typically, wound care involves working with a podiatrist or other wound care specialist to apply adequate dressings and other topical therapies to promote wound healing. Offloading pressure in the area of the wound is also very important, as continued pressure can slow or prevent wound healing. Once a wound is healed, then podiatrists, pedorthists, and orthotists may provide special shoes or other orthotics to help decrease pressure on the area of the wound and reduce the risk of recurrence.
Is it better to amputate a toe or part of the foot instead of a more significant amputation below the knee?
Absolutely. Major amputation (i.e. an amputation above the level of the ankle) may be associated with a risk of death from the surgery, poor quality of life, and higher overall chances of dying. 8 Although walking is often possible with a prosthetic, 50% of patients who undergo major amputation never walk again on a regular basis. In comparison, minor amputations (i.e., a limb-sparing amputation within the foot) allow patients to continue walking long-term. Figure 4 shows an example of a patient who initially had a large ulcer of the foot. After revascularization, wound care, and limited amputation, the patient was able to heal the ulcer and continue walking.

Amputation prevention in a patient with severe critical limb ischemia. These images are from a 52-year-old owner of a landscaping company with diabetes, end-stage kidney disease (on dialysis) with a long-standing heel wound. He underwent multiple procedures to improve blood flow to the foot followed by cleaning (debridement) of the wound back to healthy bone followed by a type of skin graft known as a free-tissue transfer. With this ‘toe and flow’ approach, he was able to avoid an above-knee amputation. He was ultimately able to return to work with close follow-up care, which included customized shoes and work boots.
Are patients with CLI at risk for other complications apart from amputation?
In addition to ulcers on the feet, patients with CLI have a very high risk of heart attack and stroke. In fact, heart attack and stroke are leading causes of death among patients with CLI. For this reason, medical treatment of cardiovascular risk factors is paramount. Every patient with CLI should be treated with a statin medication regardless of cholesterol level. To learn more about statins, read the Vascular Disease Patient Information Page on ‘Statins’. 9 Quitting smoking improves wound healing and decreases the risk of death. Blood pressure-lowering medications, such as angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, also reduce the risk of heart attack or stroke. Finally, every patient with CLI should be prescribed either aspirin or clopidogrel to thin the blood and reduce the risk of cardiovascular events. Recent data also suggest that low dose rivaroxaban, an oral anticoagulant given in addition to an antiplatelet agent, can reduce the risk of amputations and death in patients with CLI. 10
Summary
CLI is a severe form of PAD associated with pain in the legs and feet at rest and ulcers that do not heal due to poor blood flow in the arteries. Any ulcer in the foot should be evaluated promptly by a vascular specialist. Restoration of blood flow, combined with close attention to wound care, can prevent amputation in CLI.
The ‘Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at http://journals.sagepub.com/vmjpatientpage.
The Vascular Disease Patient Information Page is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Declaration of conflicting interests
Ehrin Armstrong serves as a consultant to Abbott Vascular, Boston Scientific, Cardiovascular Systems Incorporated (CSI), Gore, Medtronic, Philips, PQ Bypass, and Shockwave.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.