
Abstract
Background:
We postulated that the preoperative correction of vitamin D levels can significantly reduce the incidence of hunger bone syndrome among patients undergoing parathyroidectomy for primary hyperparathyroidism.
Methods:
We performed a prospective, randomized, open-label study on 102 patients with primary hyperparathyroidism and coexisting vitamin D deficiency who were scheduled to undergo parathyroidectomy. Patients were divided into the following two groups: group I which included 52 patients who did not receive preoperative vitamin D supplementation; and group II which included 50 patients who received cholecalciferol 1000–2000 IU daily or 50000 IU weekly until they achieve vitamin D levels >20 ng/mL (group IIa = 25 patients) or vitamin D levels >30 ng/mL (group IIb = 25 patients).
Results:
The incidence of hunger bone syndrome in group IIb was lower than group I and group IIa (8% versus 16% versus 23%, respectively); however, this difference did not reach the level of statistical significance (p = 0.22). Patients with hunger bone syndrome were significantly younger and had higher serum phosphorus, alkaline phosphatase, magnesium, and bone mineral density at baseline than patients without hunger bone syndrome. On the other hand, patients with hunger bone syndrome had significantly lower 25-hydroxyvitamin D at baseline than patients without hunger bone syndrome (p = 0.001). The ROC curve showed that the baseline level of serum 25-hydroxyvitamin D was not an independent discriminator of hunger bone syndrome (area under curve = 0.21 (95% CI: 0.06–0.34); p = 0.011).
Conclusions:
Preoperative course of vitamin D supplements has no preventive role on the postoperative incidence of hunger bone syndrome among patients with primary hyperparathyroidism and coexisting vitamin D deficiency undergoing parathyroidectomy.
Introduction
Primary hyperparathyroidism is ranked as the third most common endocrinal disorder, which affects up to 1% of the adults’ population, especially elderly patients and postmenopausal women 1 . Owing to recent advances in biochemical screening protocols, the number of patients with primary hyperparathyroidism has increased dramatically in the past few decades 2 . Parathyroidectomy is the only definitive treatment for primary hyperparathyroidism; a cumulative body of evidence shows that parathyroidectomy is effective in correcting hypercalcemia and improving end-organ complications, such as osteoporosis and renal failure 3 . The introduction of new technologies and approaches, such as minimally invasive parathyroidectomy, resulted in a high cure rate and better quality of life in symptomatic patients4,5.
However, parathyroidectomy is not a complication-free procedure. Despite being rare, postoperative hematoma, recurrent nerve injury, superior laryngeal nerve, and hypocalcemia were reported following parathyroidectomy 6 . Hunger bone syndrome (HBS) is a relatively uncommon consequence of suppressed parathyroid hormone (PTH) following parathyroidectomy; the condition is characterized by sudden onset of severe hypocalcaemia, hypophosphataemia, and hypomagnesaemia that persist beyond the fourth postoperative day7,8. HBS usually affects patients with high preoperative bone turnover and presents with tetany-like manifestations, pathological fractures, and eventually coma and death if not promptly corrected9,10. While oral calcium and calcitriol supplementation are the cornerstones for the treatment of HBS, a growing number of published literature has investigated different preventive strategies, especially in high-risk patients11 –13. Preoperative therapy with bisphosphonates and zoledronic acid exhibited a significant decrease in the incidence of HBS following primary hyperparathyroidism11,14. However, the protective role of bisphosphonates is controversial with conflicting published data about its role in the prevention of HBS; short-term preoperative treatment has also been shown to exacerbate postoperative hypocalcemia 15 .
Various risk factors are thought to contribute to the development of HBS, such as old age, high preoperative levels of serum calcium and PTH, high bone turnover, skeletal abnormalities, and a rapid decline in serum PTH levels after surgery7,16. Preoperative vitamin D deficiency is a significant risk factor for HBS in patients undergoing parathyroidectomy. Previous reports showed that a lower preoperative level of 25-hydroxyvitamin D was an independent predictor for secondary hyperparathyroidism and HBS development17,18. A recent report by Rolighed et al. 19 showed that the preoperative dose of vitamin D supplementation improved vitamin status and reduced bone resorption preoperatively. Thus, we postulated that the preoperative correction of vitamin D levels can significantly reduce the incidence of HBS among patients undergoing parathyroidectomy for primary hyperparathyroidism.
Materials And Methods
We performed a prospective, randomized, open-label study on 102 consecutive patients undergoing parathyroidectomy at Cairo University Teaching hospital. Adult patients with primary hyperparathyroidism due to benign adenoma and preoperative vitamin D levels of less than 29 ng/mL were included. We utilized the Horlick classification to categorized the vitamin D status into normal category (>30 ng/mL), insufficient status (21–29 ng/mL), and deficient status (<20 ng/mL) 20 . Only patients with a positive localization by high-resolution parathyroid ultrasound, Tc Sestamibi parathyroid scan, or both were included. We excluded patients with multiglandular, suspected, or proved carcinoma; patients with inadequate fall of intraoperative PTH; patients with renal impairment; and/or pregnancy or lactation at the time of surgery.
Eligible patients were randomly allocated by computer-generated random sequence into the following two groups: group I which included 52 patients who did not receive preoperative vitamin D supplementation; and group II which included 50 patients who received cholecalciferol 1000–2000 IU daily or 50000 IU weekly for variable periods not exceeding 6 months 21 until they achieve vitamin D levels >20 ng/mL (group IIa = 25 patients) or vitamin D levels >30 ng/mL (group IIb = 25 patients).
Surgical Techniques
Parathyroidectomy was done via routine transverse neck incision or by a focused approach according to the results of preoperative imaging results and surgeon preference. In all cases, intraoperative assessment of rapid PTH assay was done to ensure the adequacy of surgery. The decline of more than 50% of the preoperative value within 10 min is considered a successful surgery.
Data Collection
All patients were subjected to full history taking and clinical examination before surgery. The preoperative assessment also included serum calcium level, serum phosphorus level, serum magnesium level, 25-hydroxyvitamin D level, imaging findings, and bone mineral density (BMD) using dual-energy X-ray absorptiometry (DEXA); the simply calculated osteoporosis estimation (SCORE) was used to calculate the BMD T or Z-score depending on patient age with the standard deviation (SD), compared to mean BMD in a healthy young adult 22 . Postoperatively, patients were followed for 4 weeks for the assessment of the changes in laboratory parameters and the occurrence of HBS. The HBS was defined as profound hypocalcemia below 8.2 mg/dL and hypophosphatemia that extended beyond the fourth day postoperative 23 . In the case of HBS, the patient was treated by intravenous (IV), oral calcium, or both together with active vitamin D (calcitriol) 0.25–1 µg according to patients’ requirements until the symptoms of hypocalcemia improved and attain acceptable levels of serum calcium levels 24 .
Study’s Outcomes
The primary outcome in the current study was to assess the effect of the preoperative correction of serum vitamin D levels on the occurrence of postoperative HBS. The secondary outcomes included the cut-off value for vitamin D level, which is associated with a higher incidence of HBS and the association between the preoperative laboratory data and HBS.
Statistical Analysis
The statistical analysis was performed using SPSS version 22.0. The expression of categorical and continuous data was done using frequencies and mean (±SD), respectively. To the test the hypothesis of significant association between continuous variables, we used unpaired T-test or Mann Whitney’s test; while the chi-square was used to test the hypothesis of significant association between categorical variables. The null hypothesis was rejected at probability level of <5%.
Results
The mean age of the included patients was significantly higher in the group IIb (50.8 ± 1.3 years) than group I (47.4 ± 4.4 years) and group IIa (46.5 ± 3.4; p < 0.001); while the majority of the patients were females (p = 0.74). Group IIb had significantly higher preoperative calcium level than group I and group IIa (12.4 ± 0.7 versus 12.5 ± 0.3 versus 13.1 ± 0.4, respectively; p < 0.001). Likewise, group IIb had significantly lower preoperative levels of serum phosphorus and higher serum PTH than group I and group IIa (p < 0.001). Besides, patients in group IIa had significantly lower preoperative levels of serum phosphorus than group I (p < 0.001). Patients in group I had substantially lower preoperative levels of serum alkaline phosphatase than group IIa and IIb (p < 0.001). Before the administration of vitamin D supplement, the group I had a significantly higher level of 25-hydroxyvitamin D than group IIa and IIb (p < 0.001). Table 1 shows the preoperative characteristics of the included patients.
The baseline characteristics of study participants.
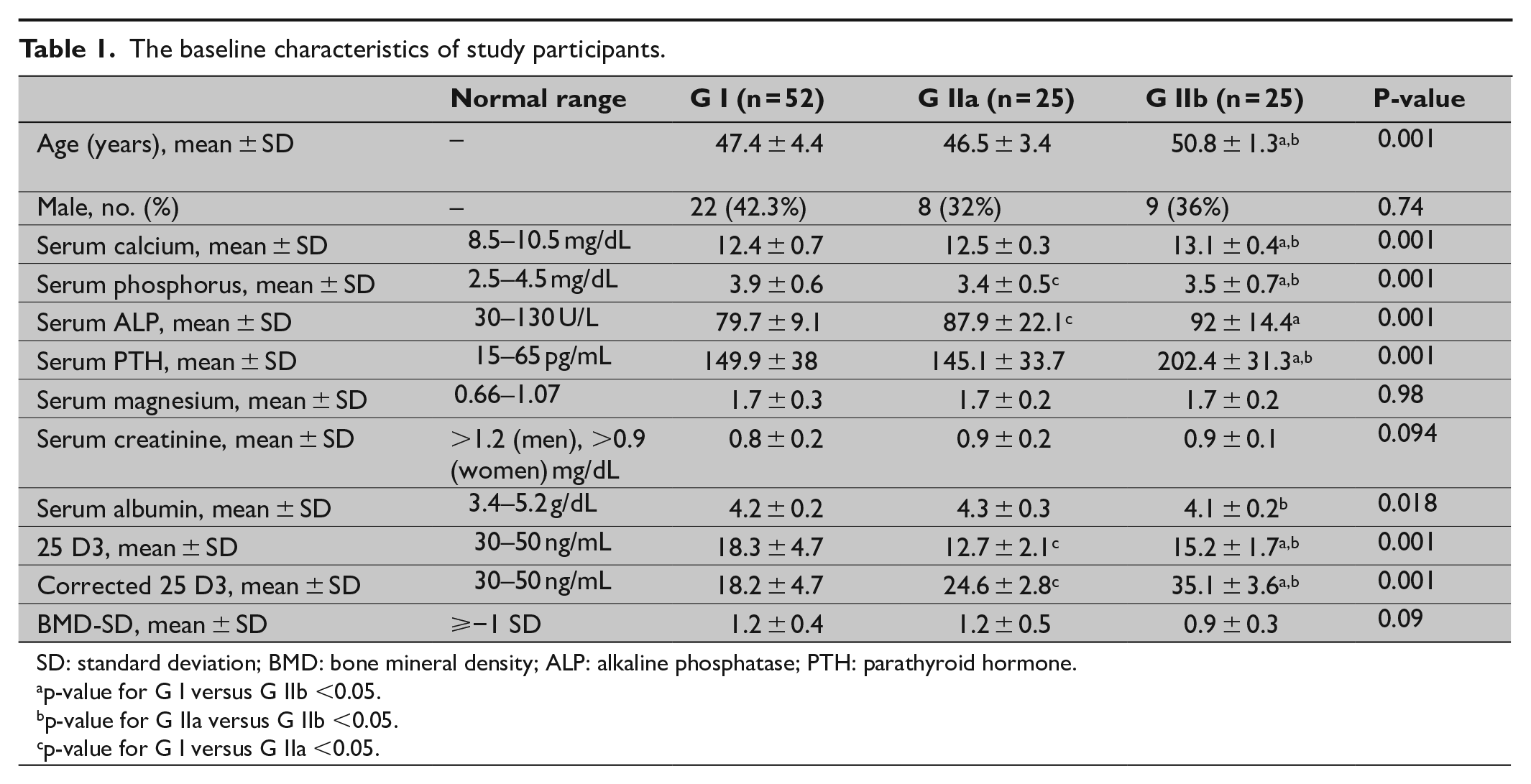
SD: standard deviation; BMD: bone mineral density; ALP: alkaline phosphatase; PTH: parathyroid hormone.
p-value for G I versus G IIb <0.05.
p-value for G IIa versus G IIb <0.05.
p-value for G I versus G IIa <0.05.
Postoperatively, serum calcium showed a significant increase from 7.53 ± 1.2 ng/mL at day 1 to 8.6 ± 0.4 ng/mL at day 30 in group I. Similarly, the serum calcium level increased in group IIa and IIb from 7.7 ± 1.1 and 8.1 ± 0.7 ng/mL at day 1 to 8.8 ± 0.4 and 8.9 ± 0.3 ng/mL at day 30, respectively. On day 30, the serum calcium level was significantly higher in group IIb than group I (p < 0.001). On the other hand, the serum phosphorus increased, and serum alkaline phosphatase level decreased significantly in group IIa and group IIb from day 1 to day 30 (Table 2).
The change in laboratory parameters during follow-up.
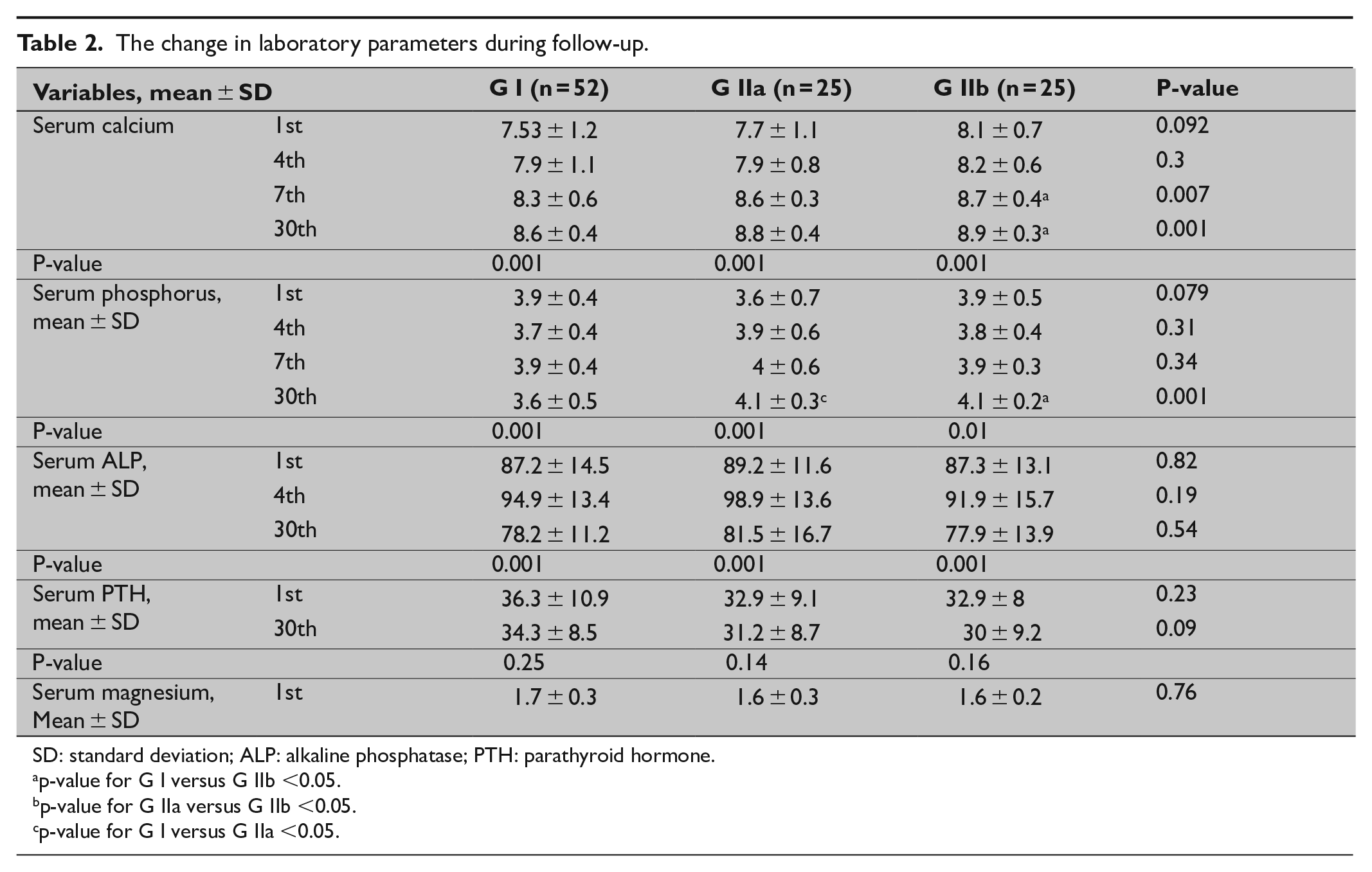
SD: standard deviation; ALP: alkaline phosphatase; PTH: parathyroid hormone.
p-value for G I versus G IIb <0.05.
p-value for G IIa versus G IIb <0.05.
p-value for G I versus G IIa <0.05.
In terms of the primary outcomes of the present study, the incidence of HBS in group IIb was lower than group I and group IIa (8% versus 16% versus 23%, respectively); however, this difference did not reach the level of statistical significance (p = 0.22; Fig. 1). The association analysis showed that patients with HBS were significantly younger and had higher serum phosphorus, alkaline phosphatase, magnesium, and BMD at baseline than patients without HBS. On the other hand, patients with HBS had significantly lower 25-hydroxyvitamin D at baseline than patients without HBS (p = 0.001; Table 3).
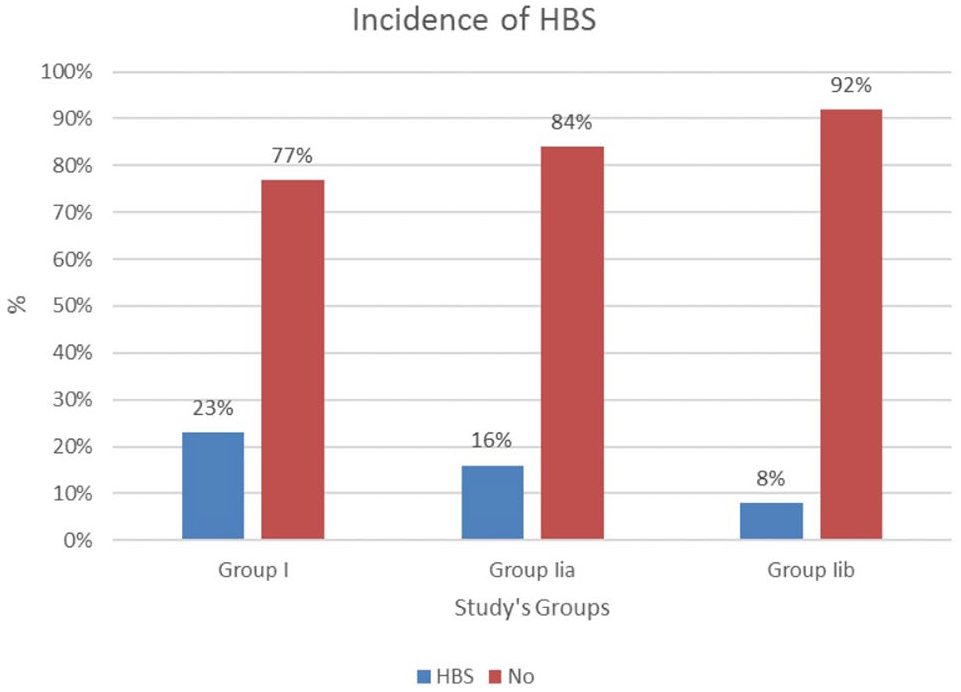
Association between the incidence of HBS and study’s groups.
The association between HBS and preoperative data.
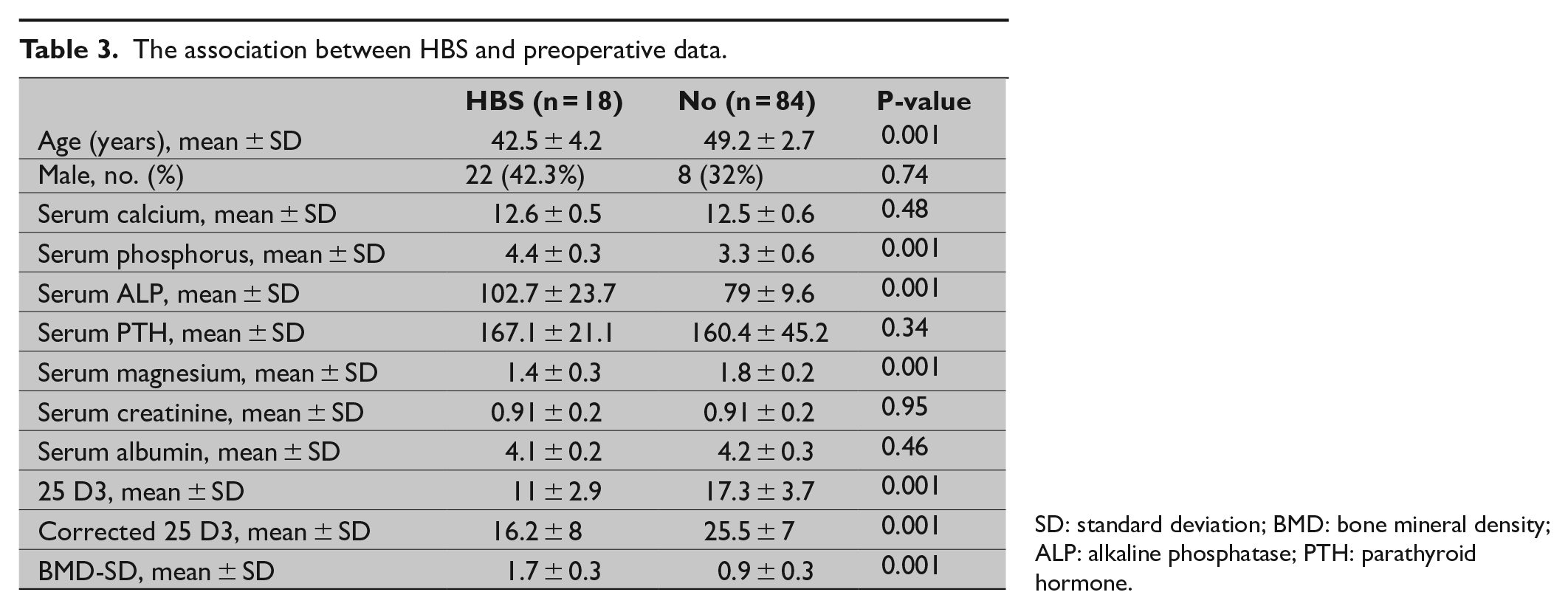
SD: standard deviation; BMD: bone mineral density; ALP: alkaline phosphatase; PTH: parathyroid hormone.
Discussion
The present prospective study assessed the value of preoperative correction of vitamin D levels on the incidence of HBS among patients undergoing parathyroidectomy for primary hyperparathyroidism. Although patients in vitamin D groups exhibited higher serum calcium levels during the postoperative period, we found that preoperative correction of vitamin D did not reduce the incidence of postoperative HBS. On the other hand, patients with HBS exhibited lower levels of preoperative 25-hydroxyvitamin D than patients without HBS; however, the preoperative 25-hydroxyvitamin D was not an independent discriminator of postoperative HBS.
The deficiency in vitamin D has a significant impact on the prognosis and management of primary hyperparathyroidism. While the degree of vitamin D deficiency is closely related to the severity of underlying hyperparathyroidism, vitamin D–deficient patients have higher risks of postoperative hypocalcemia and HBS 25 . Based on these observations, preliminary data suggested that preoperative correction of vitamin D deficiency may improve postoperative hypocalcaemia and decrease the likelihood of HBS 26 . In the present study, patients in vitamin D supplement groups showed better improvement in serum calcium and alkaline phosphatase levels than the control group 1 month after the surgery. Nevertheless, this improvement in laboratory data was not reflected in the incidence of HBS as we found no significant reduction in the incidence of HBS following preoperative correction of vitamin D. However, the incidence of HBS was numerically lower in patients who received oral vitamin D supplements than the control group. To the best of our knowledge, this is the first large cohort study which assessed the preventive role of vitamin D supplement on the incidence of HBS. Owing to the limited number of published evidence, there are no precise data about the potential causes of the lack of protective role of vitamin D supplementation on postoperative HBS. However, it can be postulated that the low sample size and low incidence of HBS in our study might have contributed to these findings. Our findings are also supported by Van’t Hoff et al. 27 report, which showed no significant impact of the preoperative course of vitamin D supplement on the postoperative course of patients treated with parathyroidectomy. On the contrary, another report on six cases demonstrated a significant impact of the preoperative course of l α-hydroxyvitamin D3 on the adverse features of HBS 28 . Thus, further, large-scale, trial is still needed to evaluate the protective role of vitamin D supplementation on postoperative HBS.
As mentioned before, various risk factors are thought to contribute to the development of HBS such as old age, high preoperative levels of serum calcium and PTH, high bone turnover, skeletal abnormalities, depleted vitamin D status, and a rapid decline in serum PTH levels after surgery 7,16. In the current work, we found that patients with HBS were significantly older and had higher serum phosphorus, alkaline phosphatase, magnesium, and BMD at baseline than patients without HBS. On the other hand, patients with HBS had significantly lower 25-hydroxyvitamin D at baseline than patients without HBS. Similar to our findings, a retrospective analysis of 62 patients showed that preoperative levels of serum calcium and alkaline phosphatase were risk factors for HBS development 16 . Despite this finding, preoperative 25-hydroxyvitamin D was not an independent discriminator of HBS in our cohort. In a cohort of 145 patients with primary hyperparathyroidism, Boudou et al. 29 showed that preoperative vitamin D level was not predictive of postoperative hypocalcemia.
This trial has some limitations. The duration of vitamin D insufficiency/deficiency and the history of vitamin D supplementation was not assessed in the present study, which might have influenced the incidence of postoperative HBS. Besides, parameters such as adenoma volume and serum markers of bone turnover were not assessed preoperatively and adjusted among the studied groups; previous reports demonstrated that preoperative adenoma volume and serum markers of bone turnover significantly impact the incidence of postoperative HBS 26 . Another limitation is the young age of the included patients, compared to other reports, and the high level of preoperative calcium level. The lack of pre-determined sample size calculations, data about the preoperative 24-h urinary calcium level and postoperative pathological findings are other limitations.
In conclusion, the present study demonstrated no preventive role of preoperative course of vitamin D supplement on the postoperative incidence of HBS among patients with primary hyperparathyroidism and coexisting vitamin D deficiency undergoing parathyroidectomy. However, patients who received vitamin D supplements showed more stable laboratory parameters than patients who left untreated. Although preoperative depletion of vitamin D status was more prominent in patients with HBS, the preoperative serum vitamin D level was not an independent predictor of postoperative HBS. Owing to the lack of published literature, randomized trials are still needed to assess the role of preoperative vitamin D supplements on the outcomes of parathyroidectomy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consents
Written informed consents were obtained from all participants.
Ethical approval
The study’s protocol was approved and registered by the local ethics committee of Cairo University Teaching hospitals.