
Abstract
Purpose:
To evaluate the effect of vitamin D on the speed and quality of pediatric fracture healing.
Methods:
A 4-year prospective study of healthy children with shaft fractures of the forearm bones (treated with minimally invasive osteosynthesis) or femur (treated by traction or by minimally invasive osteosynthesis). All children had their vitamin D levels examined four times—at the time of the injury, 1, 3, and 5 months after the injury. Also, all children underwent radiograph follow-ups (same time as blood tests) to evaluate fracture healing. Children were, in the beginning, blindly divided into two similarly sized groups—one group was orally administered cholecalciferol throughout the follow-up, the second group was not, and we compared those groups.
Results:
Altogether, 63 children were included in the study—36 supplemented and 27 non-supplemented. In supplemented children, the vitamin D levels increased statistically significantly during the follow-up period, in contrast to the non-supplemented group. The fracture healing on radiographs was also statistically significantly faster and better in the supplemented group. When we divided children according to fracture type, we observed statistically significantly better fracture healing in children with forearm fractures in the supplemented group for the whole study period. In children with femoral fractures, the healing in the supplemented group was statistically significantly better after 3 months; however, after 1 and 5 months, the difference was not statistically significant.
Conclusions:
Based on our results, we recommend vitamin D testing and administration for children treated for forearm and femoral fractures.
Level of evidence:
Level I.
Introduction
Fracture healing is a complex biological process that begins immediately after breaking the bone. It can be divided into four stages, which partly overlap: (1) inflammation stage, (2) formation of the soft (fibrous and later cartilaginous) callus, (3) formation of the hard (bony) callus, and (4) stage of bone remodeling. In cases of anatomical reduction and osteosynthesis with fragment compression, primary healing occurs without callus formation. Secondary healing with all four stages mentioned above is typical for the treatment and healing of children’s fractures.
The speed and quality of healing of skeletal injuries in children and adolescents depend on various factors. The influence of age (younger children heal faster), location of the fracture (shaft fractures take longer to heal than metaphyseal and physeal injuries), and the effect of the treatment method (longer healing after osteosynthesis) are well known. Similar rules apply to the ability to remodel the growing bone (higher ability in younger children and closer to the physis), which we use when deciding whether to treat non-operatively or whether reduction of fragments, or even osteosynthesis, is necessary.
The speed and quality of healing are usually assessed by clinical examination, and mainly by radiographs, on which we follow the presence, size, and quality of the endosteal and periosteal callus. 1
Vitamin D plays one of the key roles in the process of bone mineralization, in regulating calcium metabolism and maintaining bone homeostasis. Bone mineralization is required for (bony) callus formation and bone remodeling.
In humans, vitamin D3 is mainly produced in the skin from 7-dehydrocholesterol due to the absorption of photons of type B UV radiation. The resulting pre-vitamin D3 spontaneously isomerizes to cholecalciferol, which is further transported to the liver bound to the appropriate globulin. From cholecalciferol, calcidiol is then formed in the liver by hydroxylation at position 25, and then in several tissues (mainly in the kidneys), active 1,25-dihydroxycholecalciferol (=calcitriol) is formed. Calcitriol binds to its receptors in the whole body. Its effect is significant in the intestine (increases the absorption of calcium from the lumen), kidneys (increases the reabsorption of calcium by the tubule), parathyroid glands (by activation of the calcium-sensing receptor, it suppresses the production of parathormone), and bones (increases the resorption of older bone tissue and calcium storage into newly formed bone). 2
While the normal physiological role of vitamin D in the regulation described above is relatively well studied, its role in human bone healing is not yet completely clear.
Insufficiency or deficiency of vitamin D has been extensively studied in recent years in relation to autoimmune and other diseases, its significant deficit is associated with rickets in children and osteomalacia in adults. In older age, vitamin D insufficiency can contribute to the development of osteoporosis. 3
In the literature, vitamin D levels in both children and adults are becoming the subject of research more and more often and are, in many cases, associated with fractures and their healing. A study that would compare the healing of fractures in children with and without vitamin D supplementation is, however, still missing in the literature.
A plasma/serum level of 25-hydroxyvitamin D ≥ 30 ng/mL is stated as normal. As insufficiency of vitamin D is considered a plasma/serum level of 20–30 ng/mL, lower levels (<20 ng/mL) are reported as vitamin D deficiency. 4
This applies to all ages; however, the level of vitamin D that, with adequate calcium intake, will still prevent the development of deficient rickets is reported to be above 12 ng/mL.5,6 This means that patients with vitamin D insufficiency and some with vitamin D deficiency may not have obvious skeletal damage. Vitamin D insufficiency may, however, negatively affect the quality of immune processes involved in fracture healing.
The purpose of this study was to investigate whether the level of vitamin D is related to the speed and quality of fracture healing in children and what effect vitamin D supplementation would have. The investigators hypothesize that the initial levels of vitamin D would be generally low, given the described low saturation of the population, including children7,8 and further hypothesized that supplemented children that increase their vitamin D levels would have increased speed and quality of fracture healing on their radiographs.
Materials and methods
The prospective study took place from January 2017 to December 2019, and then from May 2021 to May 2022. It included Caucasian children (up to 18 years of age) with a shaft fracture of the forearm bones (radius, ulna, or both), treated with intramedullary osteosynthesis with Prévot nails according to the ESIN (elastic stable intramedullary nailing) technique, and children with femoral shaft fracture, treated both non-operatively by traction (Bryant’s vertical skin traction or proximal tibial skeletal oblique traction), as well as osteosynthesis according to the ESIN technique. All the children treated operatively were treated by closed reduction and osteosynthesis.
Inclusion criteria were the fracture and the method of its treatment described above, as well as informed consent to participate in the study. We asked all the children (or legal representatives) with those injuries treated at our department during both times of the study to participate. Exclusion criteria were disease or drug therapy known to affect bone quality and/or vitamin D levels and metabolism, or refusal to participate in the study.
The reason why the patient could have been excluded from the study during its course and no further follow-up took place was the patient’s own decision (or legal representative’s) to end their participation, or a refracture during the follow-up. We recorded patient demographics, including age, sex, and race.
All children included in the study had their serum levels of 25-hydroxyvitamin D repeatedly measured, a total of four times—(1) at the time of presentation of injury and enrolment in the study, (2) 1 month after the injury, (3) 3 months after the injury and (4) 5 months after the injury. Radiographs and laboratories were obtained at the stated time points.
The monitored children were randomly divided into two groups, without knowing their initial vitamin D levels. One group was orally administered vitamin D3—cholecalciferol throughout the follow-up (5 months). For supplementation, we used cholecalciferol in the concentration of 0.5 mg/mL (“Vigantol,” manufactured by Merck KGaA), in a dose of 2 drops (1000 IU = 25 µg) per day. The second group was not given vitamin D. Furthermore, it was possible to divide children into subgroups according to whether they had forearm fractures (and again either supplemented with vitamin D or without supplementation) or fractures of the femur (with or without supplementation).
Evaluation of bone healing was carried out by two experienced pediatric surgeons, both independently and completely blinded (the evaluators did not know the laboratory results of the children in question, nor their association into supplemented/non-supplemented groups, they only had the presented radiographs available). To evaluate healing, we chose the RUST (Radiographic Union Scale for Tibial fractures) and mRUST (Modified Radiographic Union Scale for Tibial fractures) schemes, designed specifically to assess the healing of diaphyseal fractures of long bones by evaluating the callus formation (originally on the tibia).9 –12
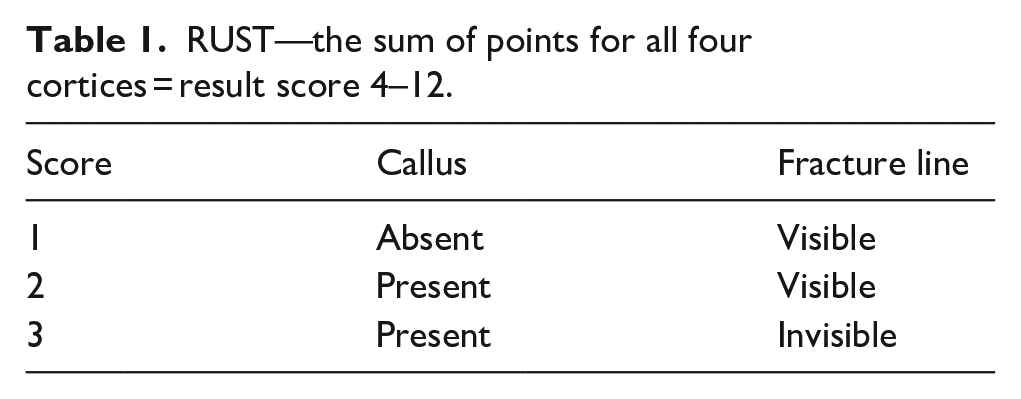
In RUST, each of the four cortices (ventral, dorsal, lateral, and medial—using anteroposterior and lateral radiograph projections) is evaluated and scored 1–3 points according to the presence of a callus and the visibility of the fracture line (Table 1). The result is the sum of points for all cortices (4 × (1–3) = a range of 4–12 points).
RUST—the sum of points for all four cortices = result score 4–12.
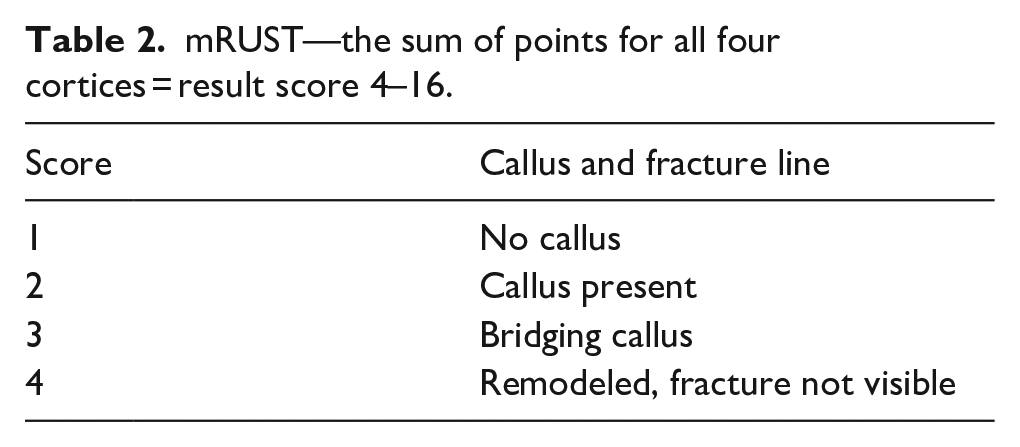
For mRUST, the scheme is modified, and the evaluation is extended to 1–4 points (Table 2). The resulting value is, again, the sum of points for all cortices (4 × (1–4) = a range of 4–16 points).
mRUST—the sum of points for all four cortices = result score 4–16.
Statistical analysis
The data are presented with descriptive statistics (average, median, minimum, and maximum). Due to the nature of the RUST and mRUST bone healing assessment data, non-parametric methods were used. Associations between variables were tested using the Mann–Whitney U test and the Friedman test. Subgroup analysis was tested using the analysis of variance model repeated measures. Statistical analysis was performed using SPSS 29.0 software (SPSS Inc.). It was tested at a significance level of 0.05.
Results
Altogether, 107 children underwent at least one examination of vitamin D levels. Of these, 63 were included in the study and samples were taken according to the study plan. A total of 44 children were excluded during the study—37 of them did not wish to take further blood tests and participate in the study, five were later treated in another hospital, and two children were excluded by study investigators due to refracture during follow-up (Chart 1).
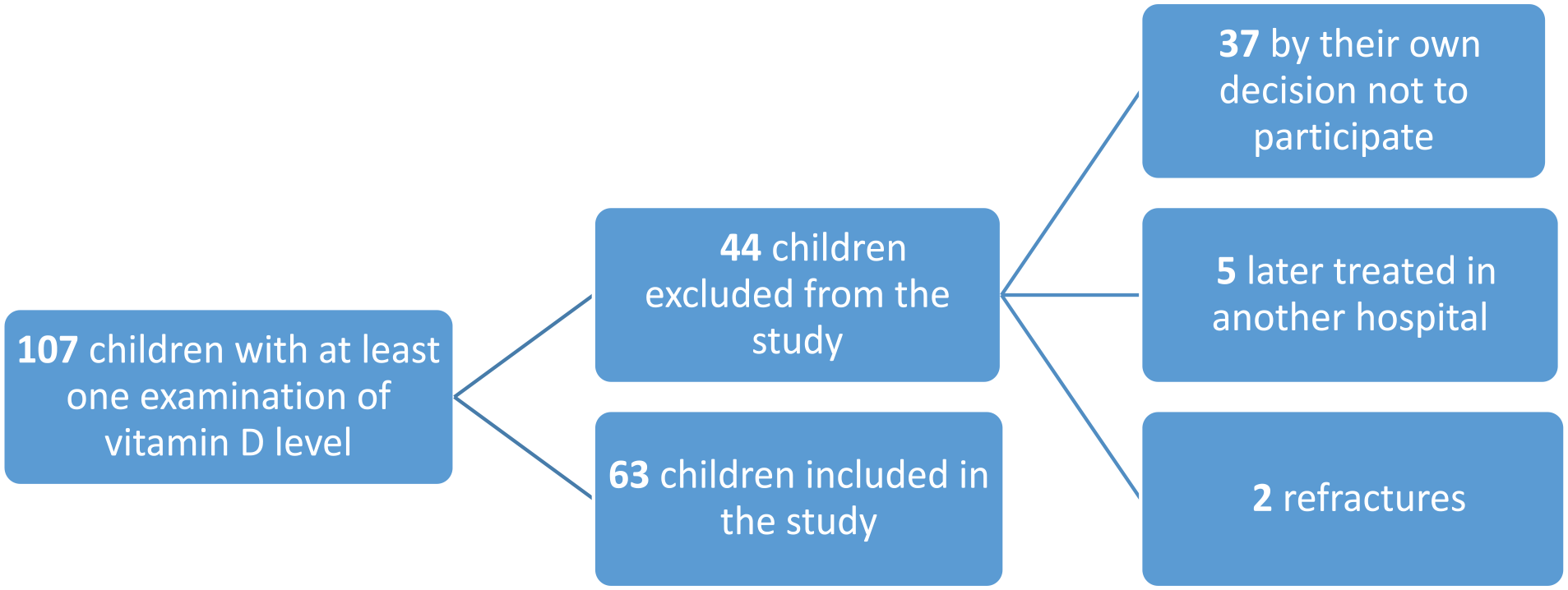
Examined children.
A total of 226 examinations were performed. The serum concentration of 25-hydroxyvitamin D from all these examinations was, on average, 27.0 ng/mL (9.2–72.5, median 24.8). Deficit of vitamin D (<20 ng/mL) was found in 63 examinations (28%). Vitamin D insufficiency (20–30 ng/mL) was present in 92 examinations (41%) and normal levels of vitamin D (≥30 ng/mL) in 71 examinations (31%).
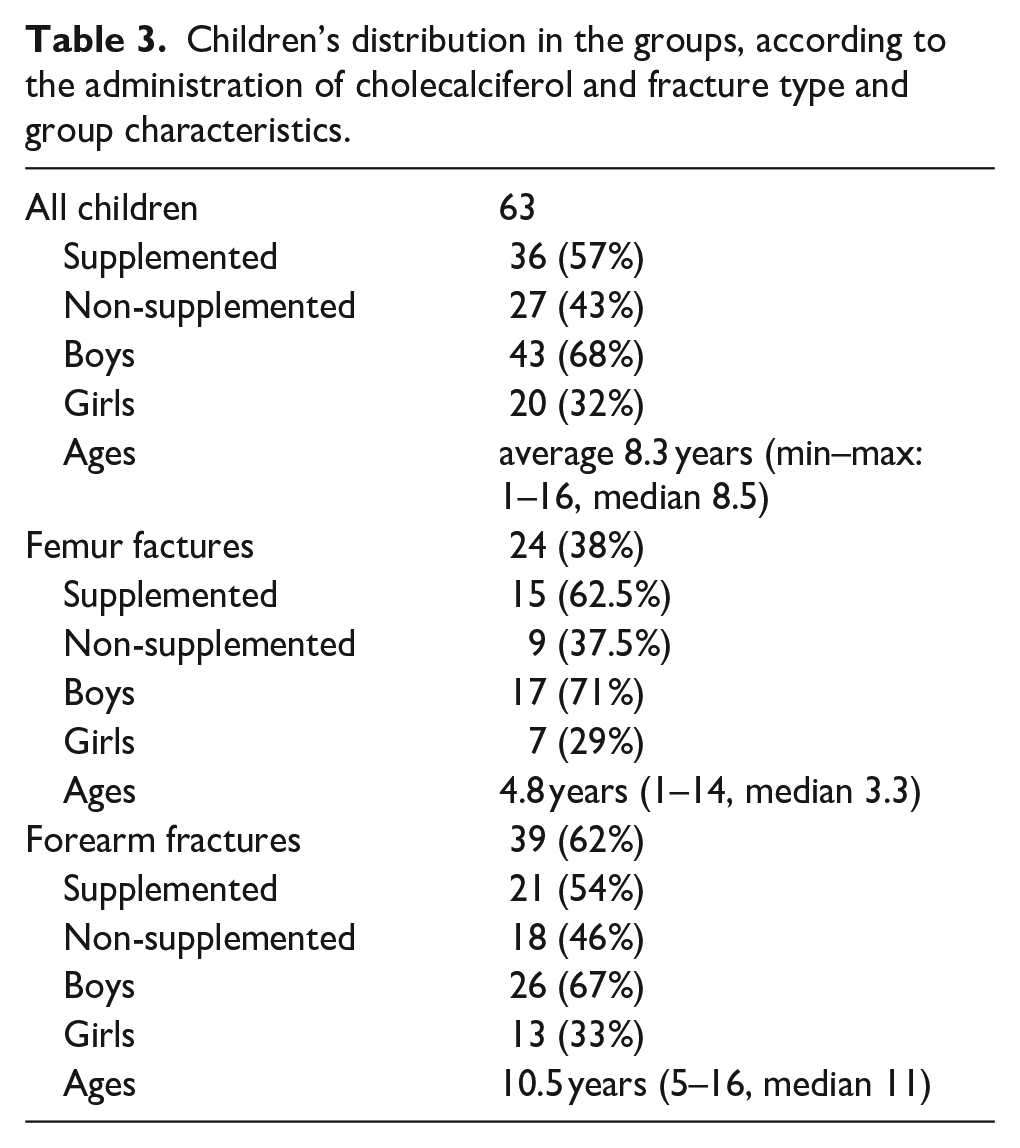
The distribution in the groups according to the administration of cholecalciferol and fracture type and characteristics of those groups are listed in Table 3, including age and sex. All the children in the study were Caucasian.
Children’s distribution in the groups, according to the administration of cholecalciferol and fracture type and group characteristics.
All children
The results of all 63 children, included in the study, and the results when divided in supplemented (n = 36) and non-supplemented (n = 27) groups are listed in Table 4 and Charts 2–4.
Results of all children, included in the study, and the results when divided into supplemented and non-supplemented groups.
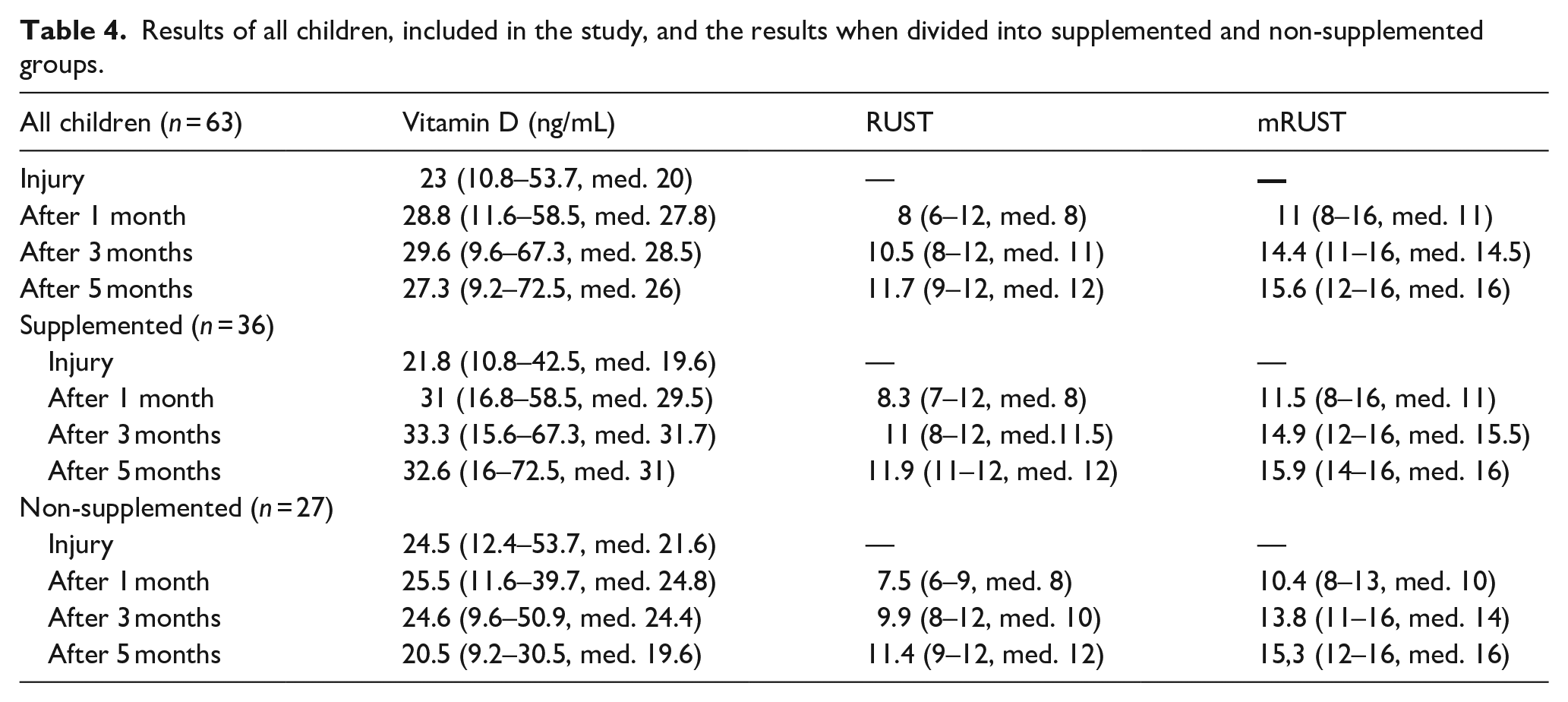
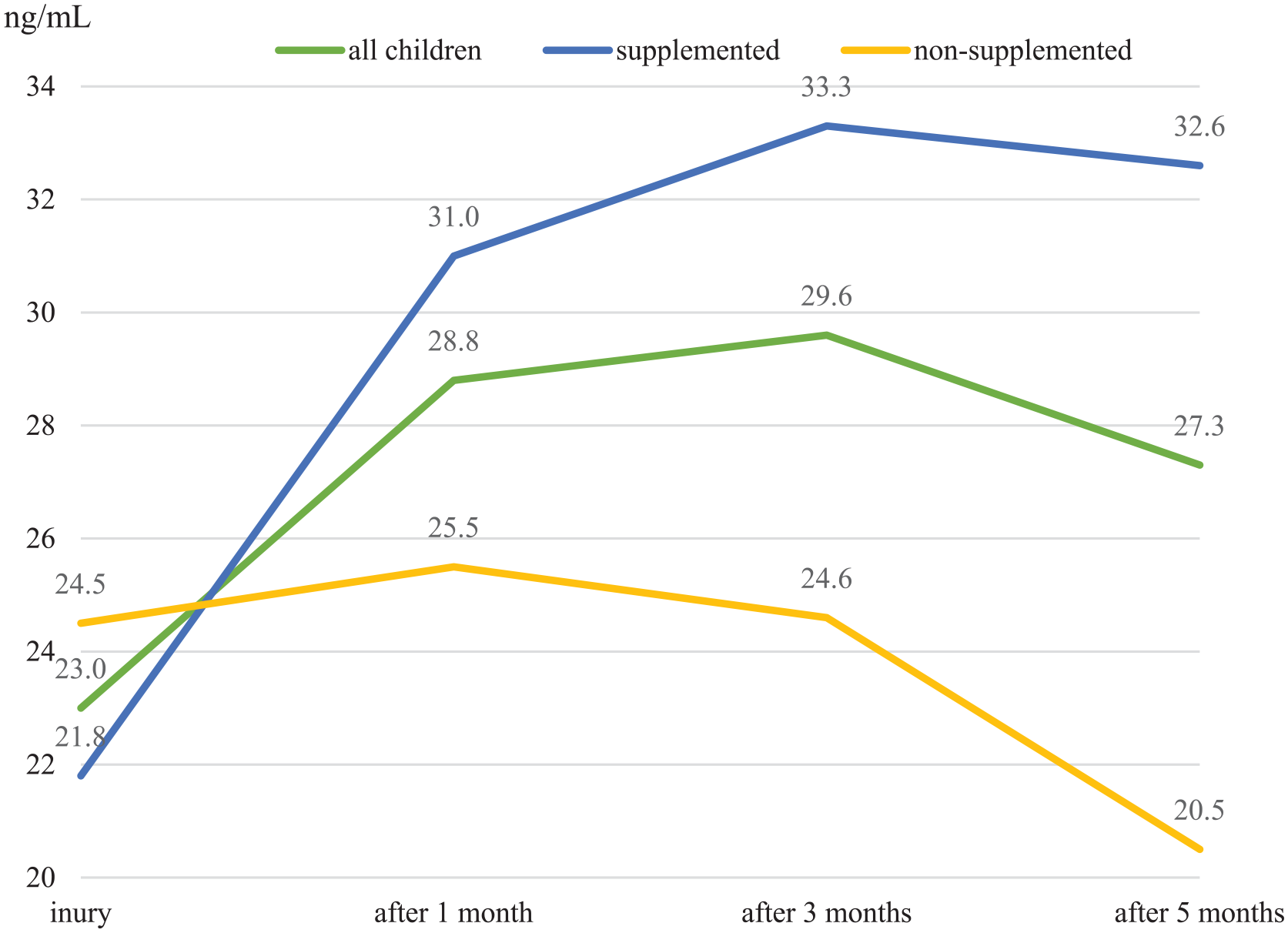
Vitamin D levels.
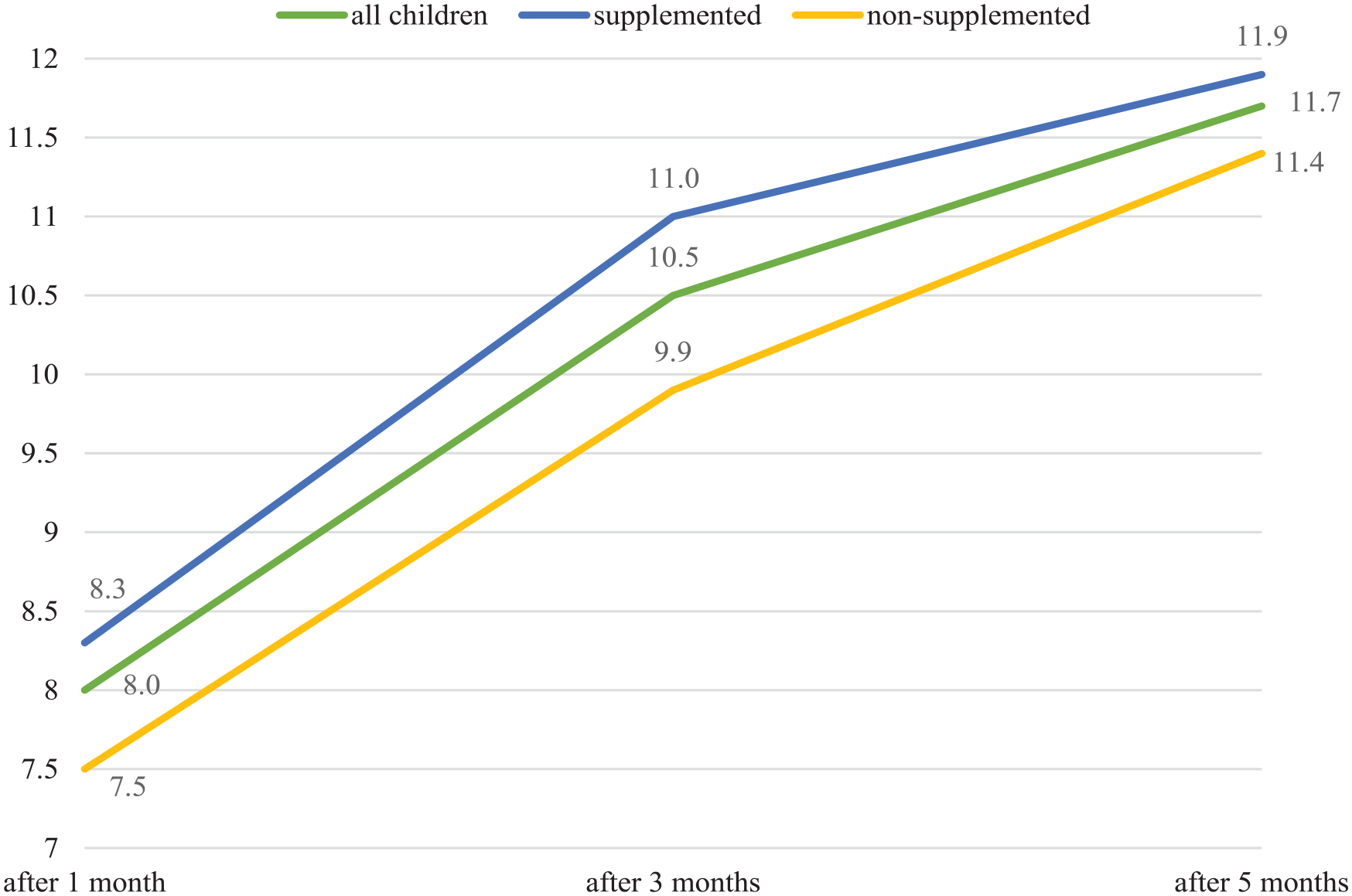
RUST.
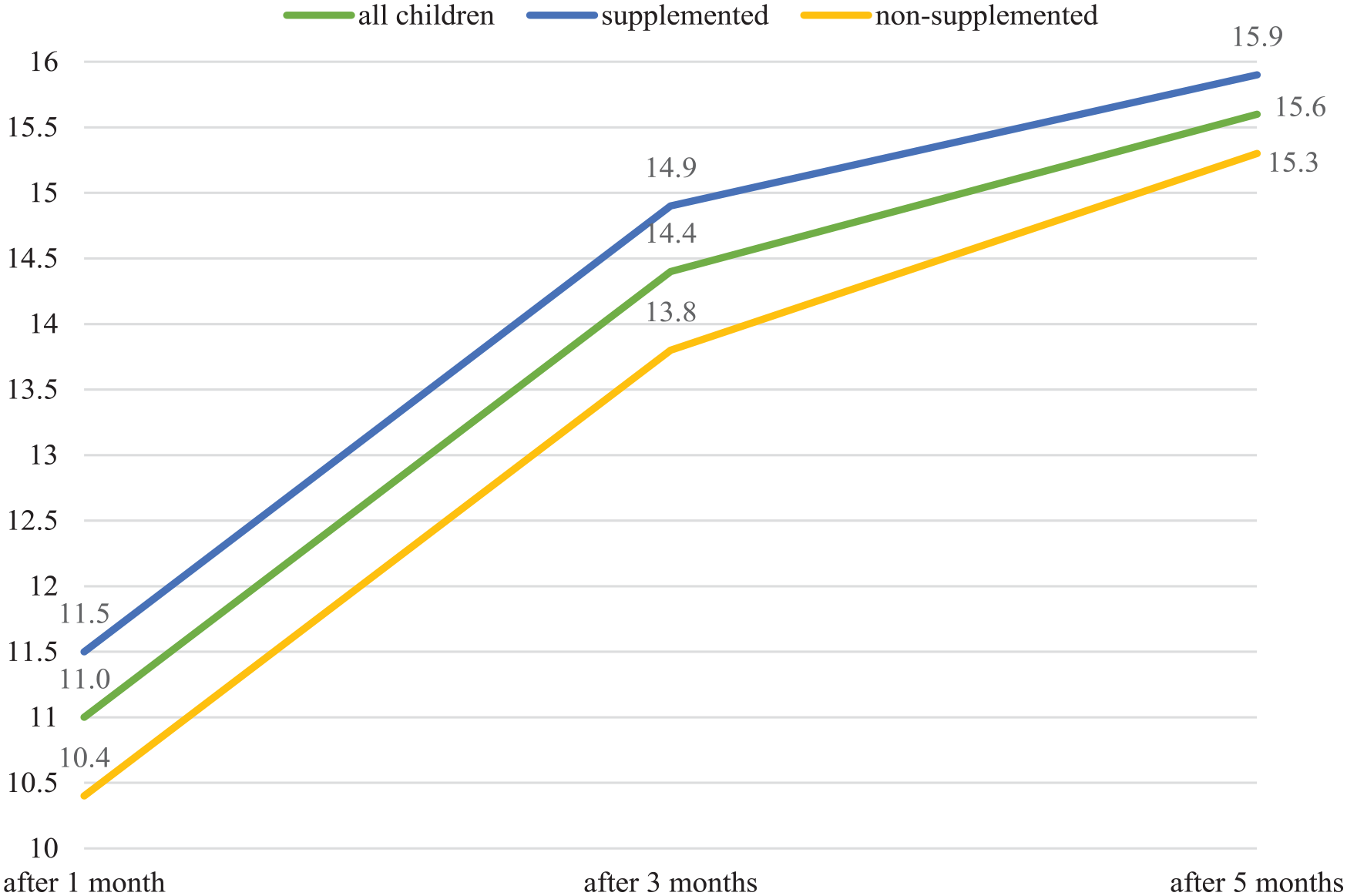
mRUST.
The initial plasma 25-OH vitamin D concentrations did not differ significantly between the study groups (p = 0.550). In the group of children supplemented with vitamin D, the vitamin D level changed statistically significantly during the follow-up period (p < 0.001). Already after 1 month of administration, there was a statistically significant increase (p < 0.001), further changes were no longer statistically significant. In the group without supplementation, the level of vitamin D did not change statistically significantly during the follow-up period (p = 0.328).
The value of RUST increased statistically significantly over time (p < 0.001) and there was also a statistically significant difference between the group of children without supplementation and those supplemented with vitamin D (p = 0.006), where the group of supplemented children achieved higher average scores.
The value of mRUST increased statistically significantly over time (p < 0.001) and there was also a statistically significant difference between the group of children without supplementation and children supplemented with vitamin D (p = 0.045), where the group of supplemented children achieved higher average scores.
Children with femur fracture
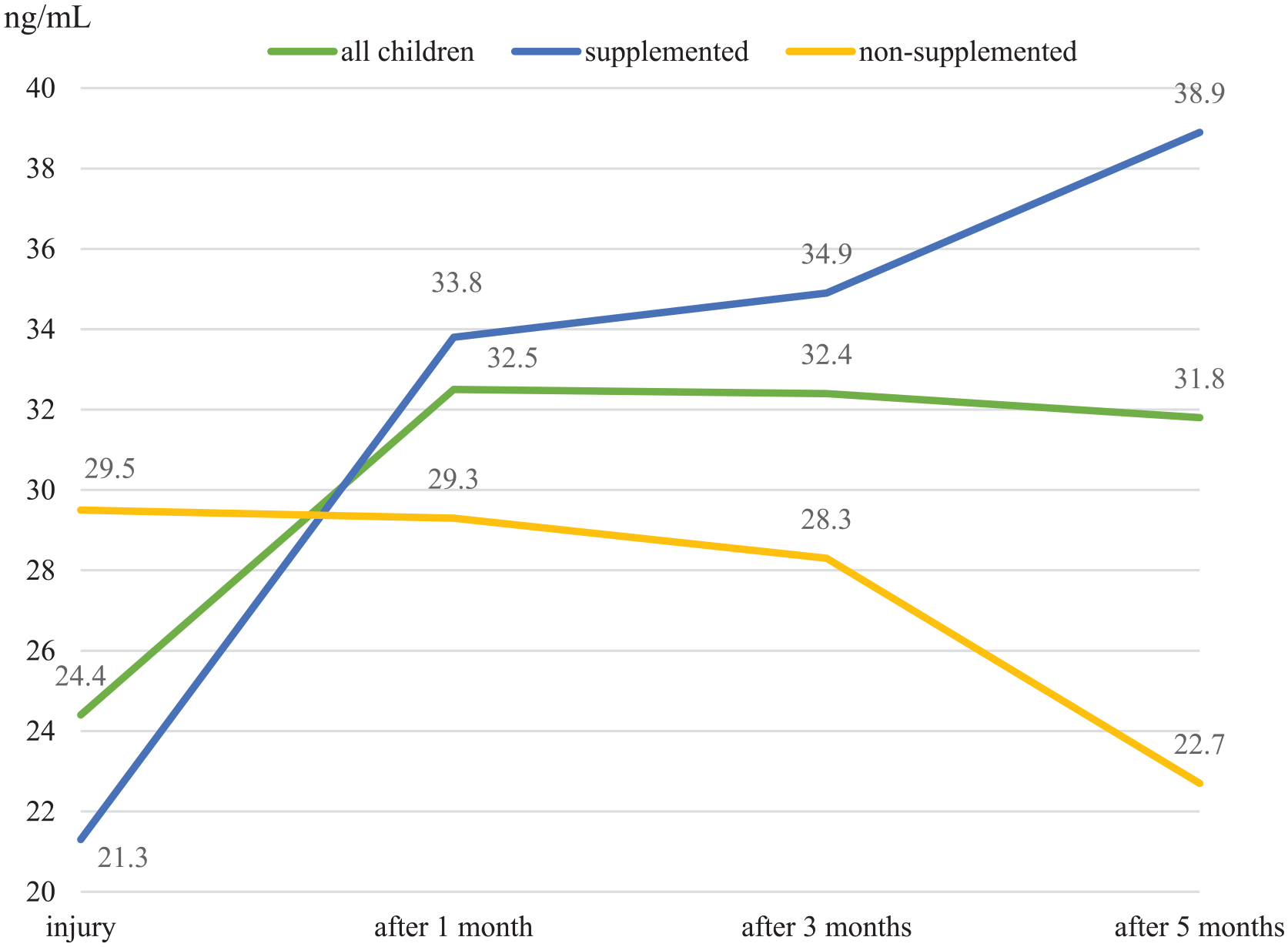
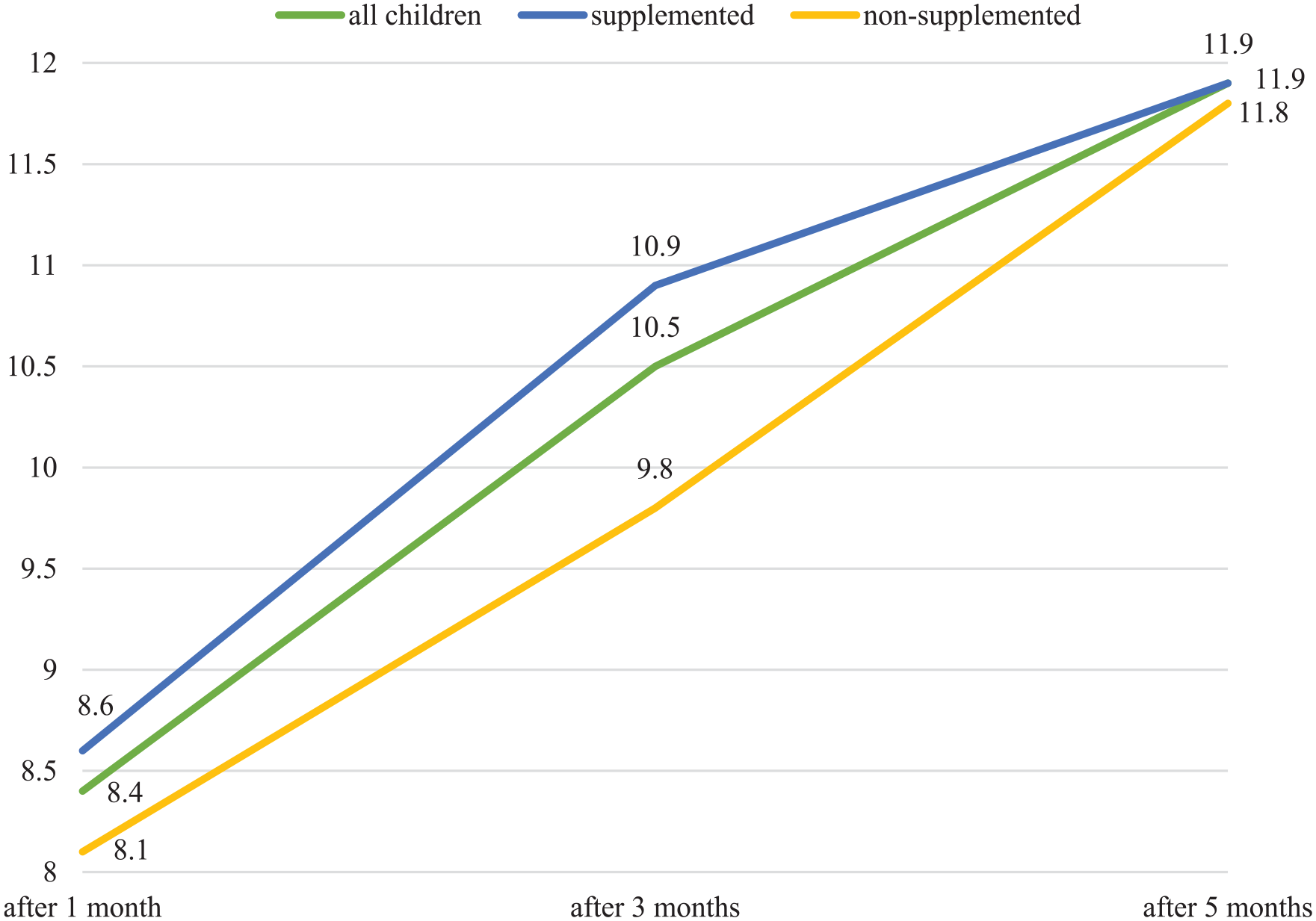
The results of 24 children with femur fracture and the results when divided into supplemented (n = 15) and non-supplemented (n = 9) groups are listed in Table 5 and Charts 5–7.
Results of children with femur fracture and the results when divided into supplemented and non-supplemented groups.
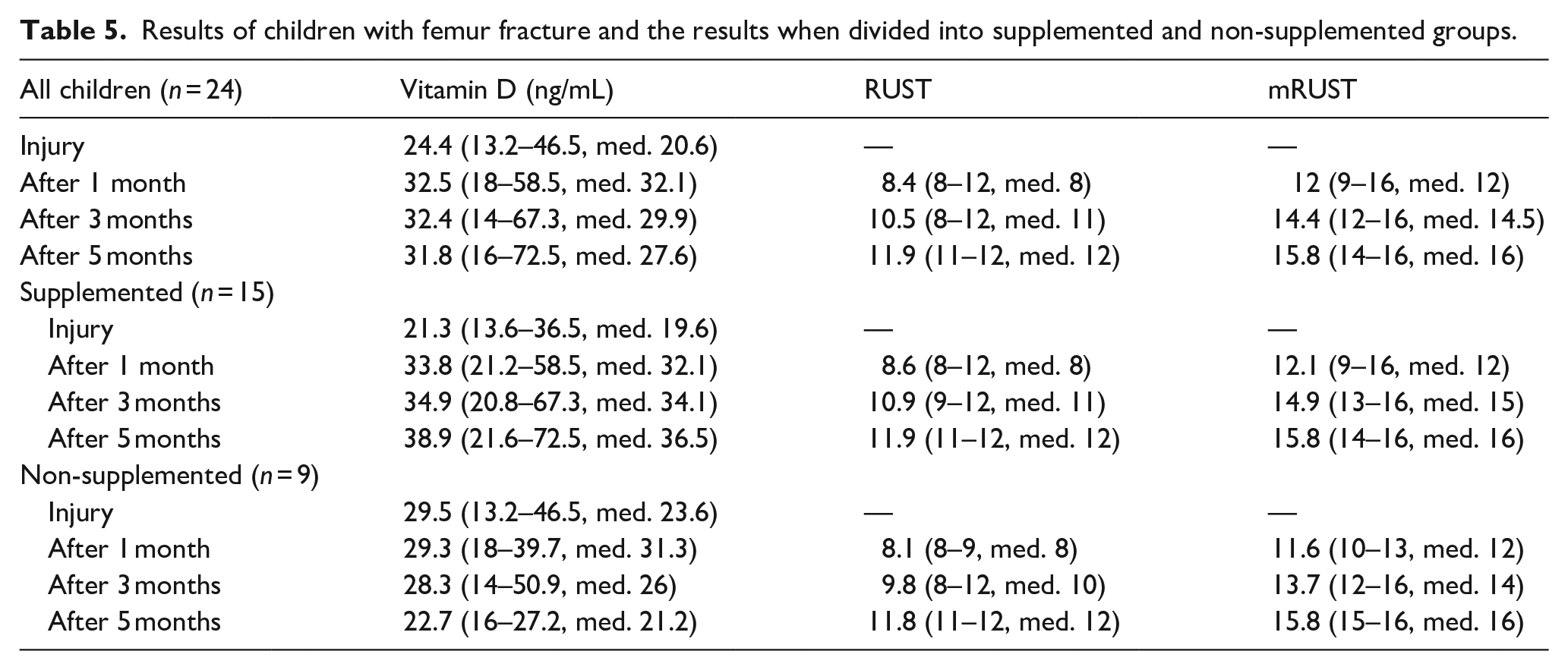
Vitamin D levels, femur fractures.
RUST, femur fractures.
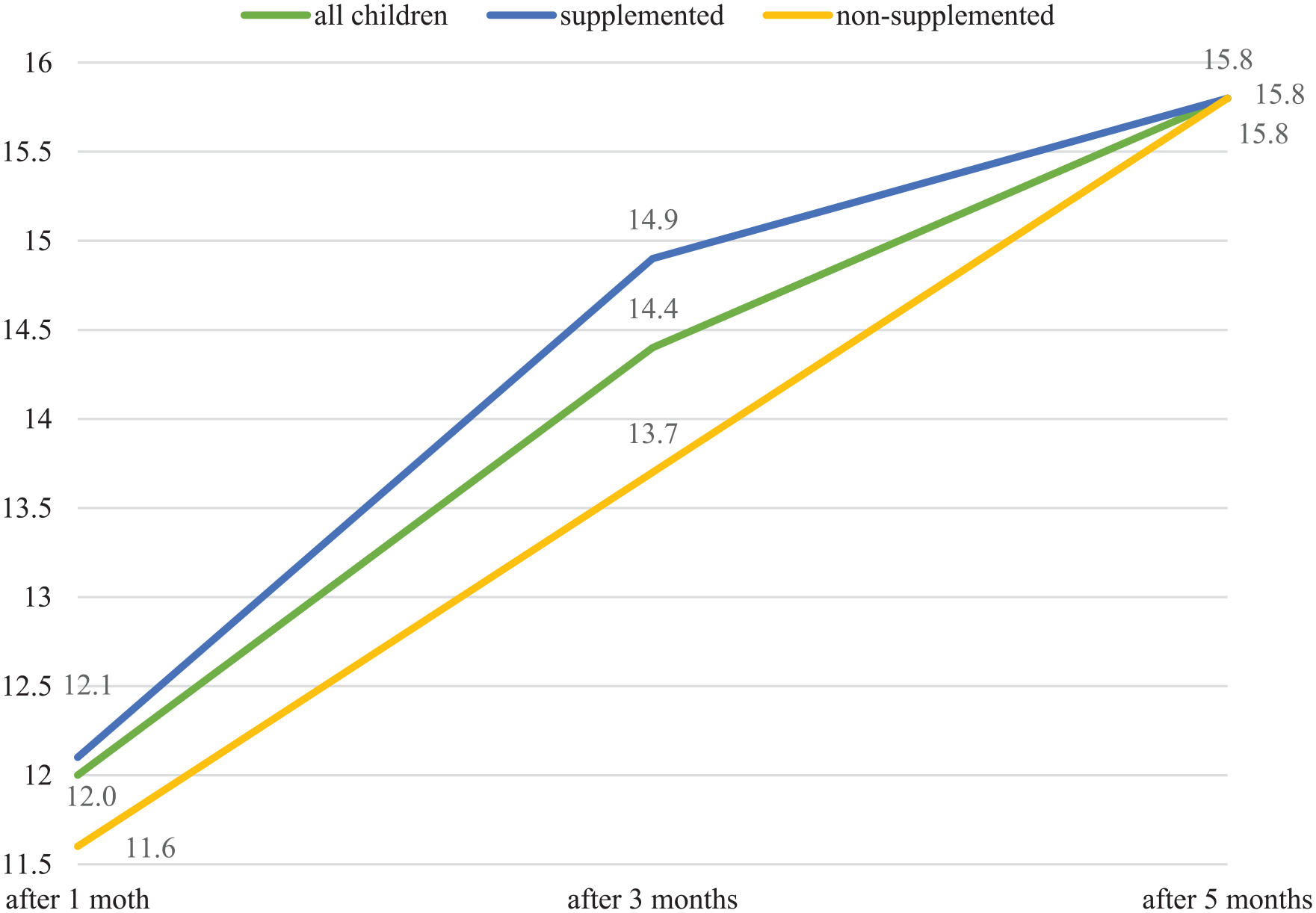
mRUST, femur fractures.
The value of RUST increased statistically significantly over time (p < 0.001), there was no statistically significant difference between the group of children without supplementation and children supplemented with vitamin D (p = 0.429). However, at the 3-month follow-up, the RUST value was statistically significantly higher in the supplemented group compared to the non-supplemented children (p = 0.002).
The value of mRUST increased statistically significantly over time (p < 0.001), there was no statistically significant difference between the group of children without supplementation and children supplemented with vitamin D (p = 0.935). However, at the 3-month follow-up, the mRUST value was statistically significantly higher in the supplemented group compared to the non-supplemented children (p = 0.004).
Children with forearm fracture
The results of 39 children with forearm fractures and the results when divided into supplemented (n = 21) and non-supplemented (n = 18) groups are listed in Table 6 and Charts 8–10.
Results of children with forearm fracture and the results when divided into supplemented and non-supplemented groups.
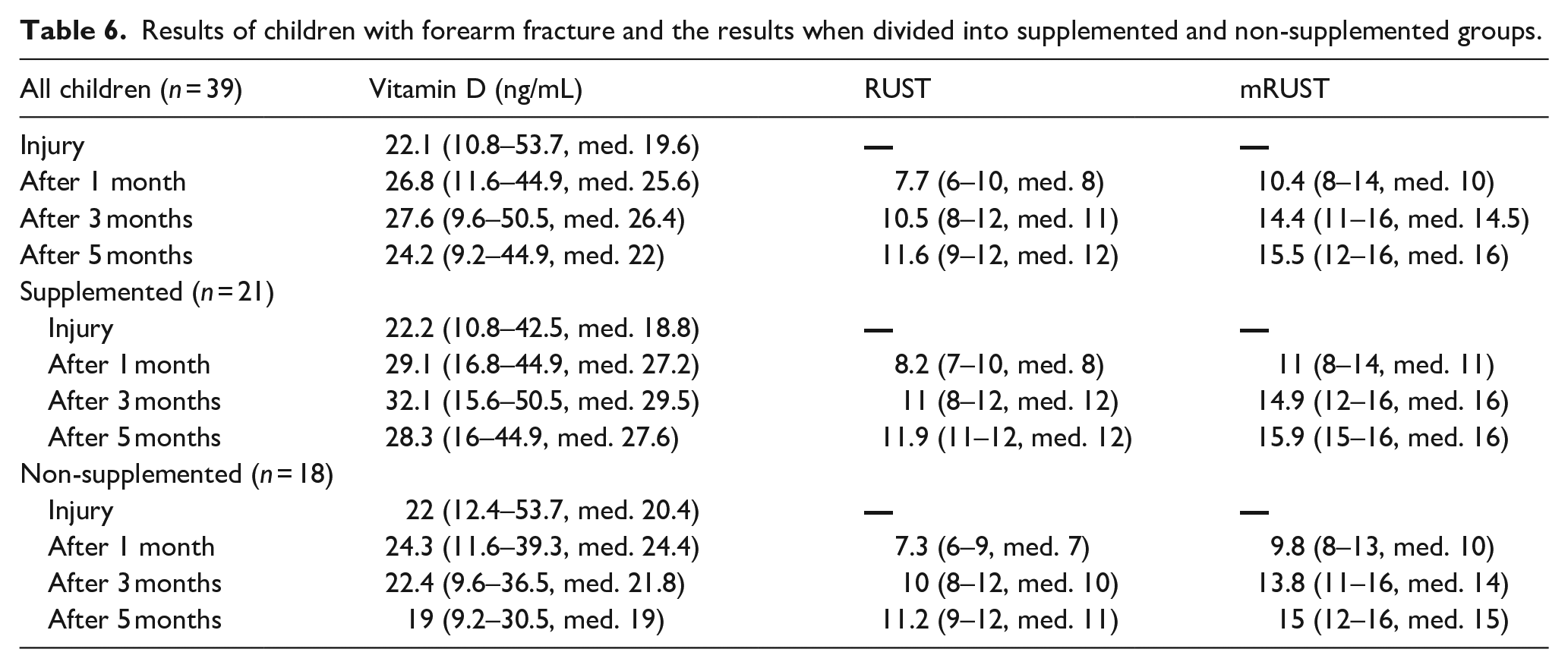
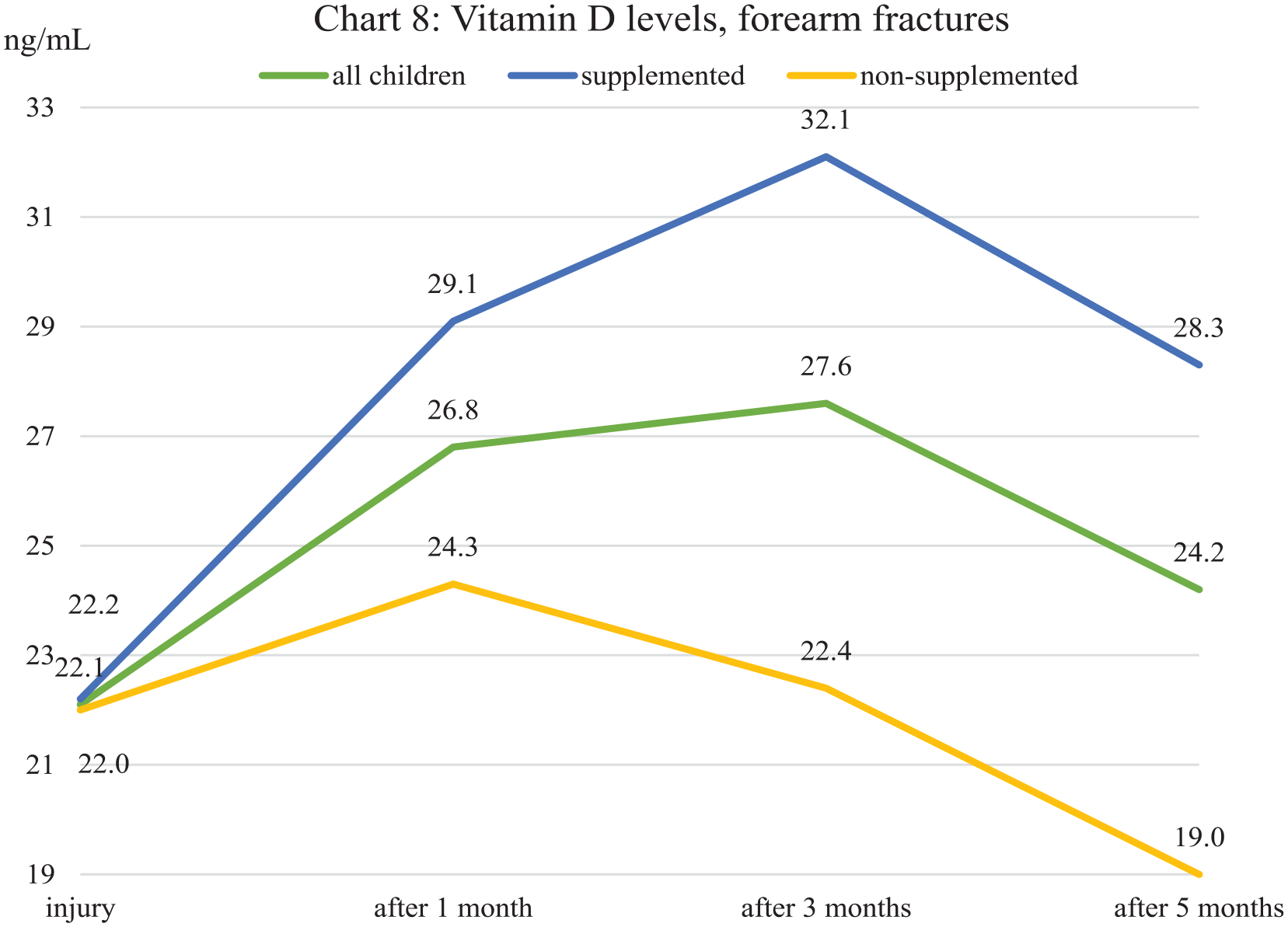
Vitamin D levels, forearm fractures.
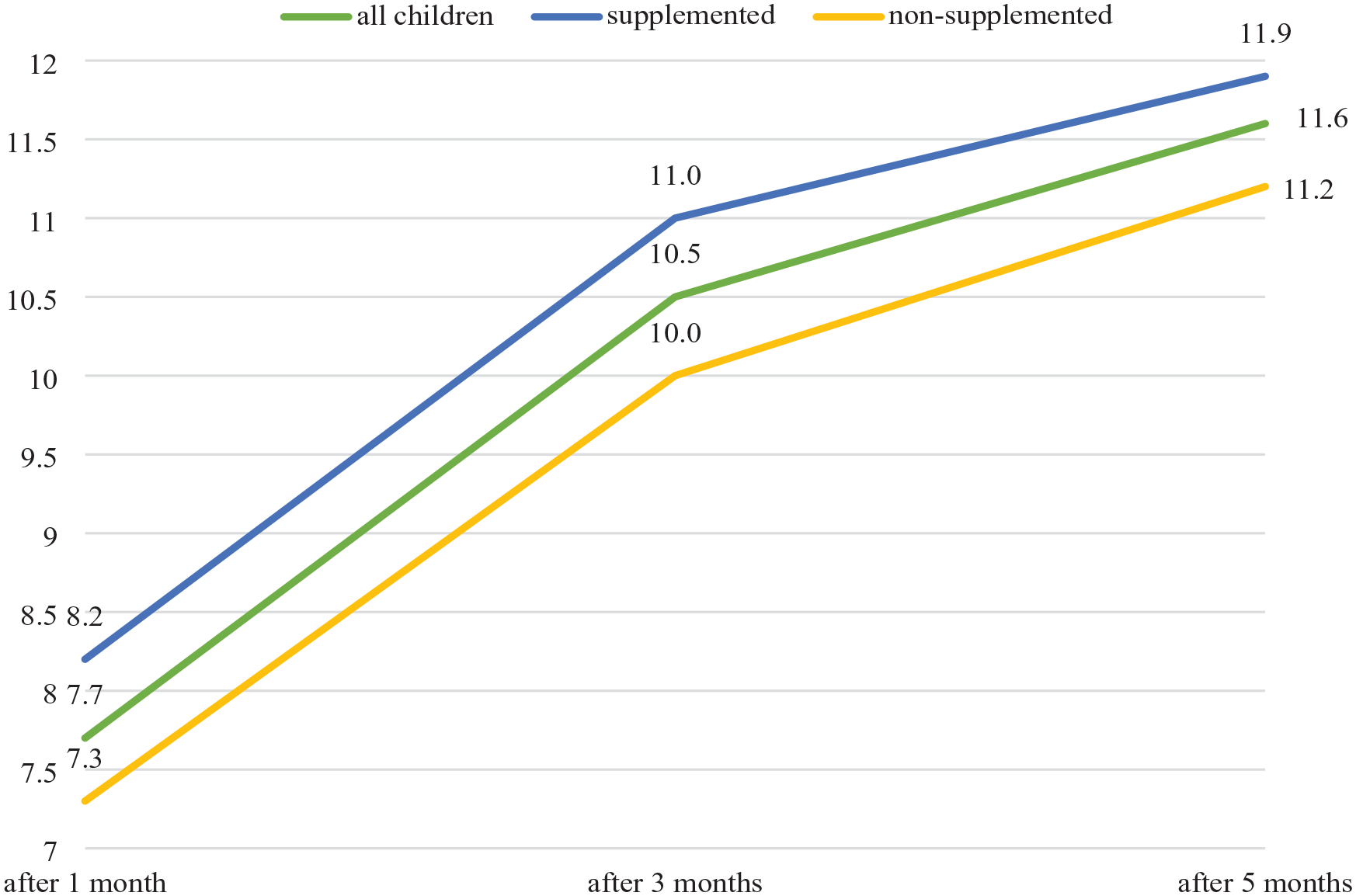
RUST, forearm fractures.
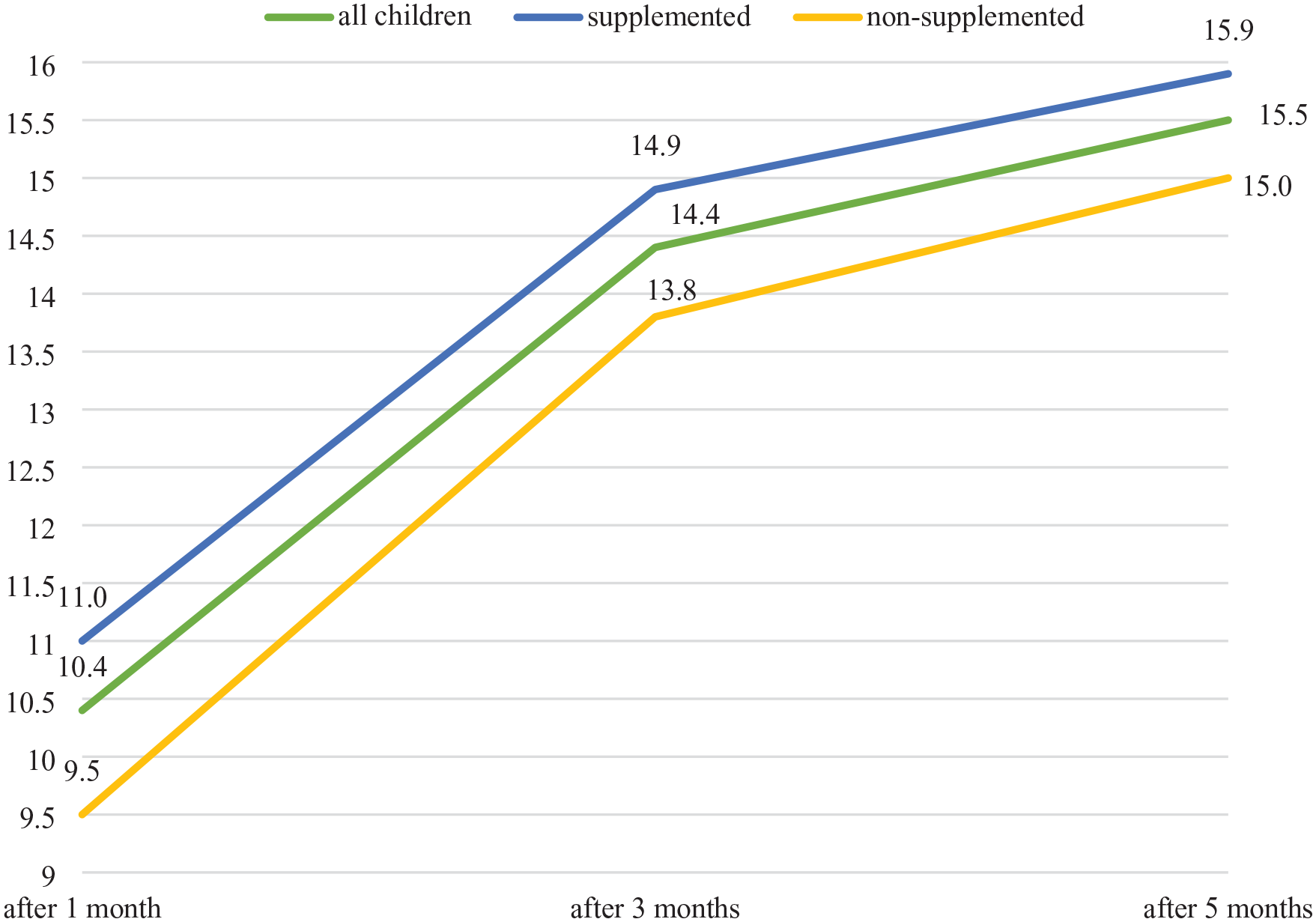
mRUST, forearm fractures.
The value of RUST increased statistically significantly over time (p < 0.001) and was statistically significantly higher in the supplemented group compared to the non-supplemented children (p = 0.005). Statistically significant differences in the average score occurred at the follow-up both after 3 months (p = 0.05) and after 5 months (p = 0.017).
The value of mRUST increased statistically significantly over time (p < 0.001) and was statistically significantly higher in the supplemented group compared to the non-supplemented children (p = 0.019). Statistically significant differences in the average score occurred at the follow-up both after 3 months (p = 0.031) and after 5 months (p = 0.017).
All data are listed in Table 7. Radiographs demonstrating differences between supplemented and non-supplemented children are visible in Figures 1 and 2.
All data.

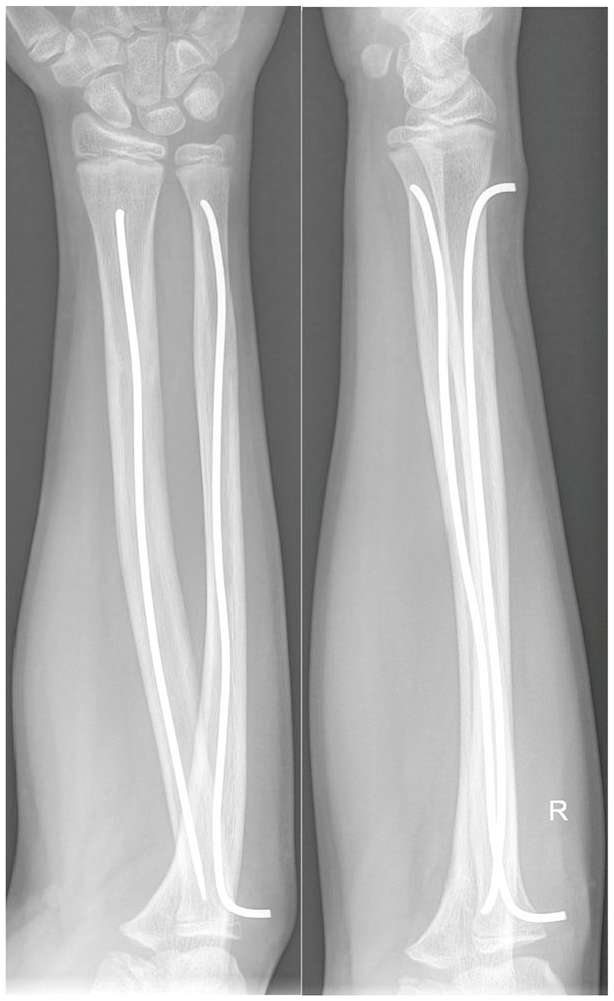
Boy, 12 years old, forearm fracture treated by osteosynthesis. Supplemented with vitamin D. Radiographs from 3 months after the injury. RUST 12, mRUST 16.

Girl, 12 years old, forearm fracture treated by osteosynthesis. Non-supplemented with vitamin D. Radiographs from 3 months after the injury. RUST 8, mRUST 11.
Discussion
The prospective study took place from January 2017 to December 2019, and then from May 2021 to May 2022. We added one more year of study after the COVID-19 pandemic because during an originally planned 3-year period (1/2017–12/2019) we did not have enough children in the study to be able to statistically evaluate the results, especially in some subgroups.
Children with a shaft fracture of the forearm bones, treated with intramedullary osteosynthesis according to the ESIN technique, and children with a femoral shaft fracture, treated both non-operatively by traction, as well as osteosynthesis according to the ESIN technique, were included in the study. We chose these skeletal injuries with these methods of treatment because they allow us to evaluate callus formation, since in the case of femoral fractures they are not fixed with a cast at all, and in the case of forearm fractures when we use osteosynthesis, casting is mainly to reduce pain and swelling after surgery and can therefore be taken off for radiograph examination purposes.
If the hypothesis of a positive effect of vitamin D on the healing of these fractures is confirmed, we would like to propose an investigation also of children treated with other types of fractures.
When evaluating blood tests, we observed a statistically significant difference in vitamin D levels between children supplemented and not supplemented with vitamin D3 already 1 month after the start of cholecalciferol administration (p < 0.001 in the supplemented group, p = 0.328 without supplementation).
Our group of children supplemented with vitamin D had, on average, values getting close to the border of vitamin D deficiency. After only 1 month of administration of cholecalciferol, their levels were within the range of normal values, where they remained also after 3 and 5 months.
In children randomly assigned to the group without cholecalciferol supplementation, the initial levels were, on average, also in the category of vitamin D insufficiency, but significantly higher than in the supplemented group. In the following months, however, stagnation was observed in the non-supplemented group or even decreased close to the border of vitamin D deficiency after 5 months (Chart 2).
When we divided children into subgroups according to fracture type, we observed a similar trend, although the exact values differ.
In children with femoral fractures, there was a greater difference between the initial values, and therefore the difference in the following months was more significant in its difference, as well. In children supplemented with cholecalciferol, there was a permanent increase in average values, while without supplementation, we observed a permanent decrease, at first moderate, then significant (Chart 5).
In children with forearm fractures, on the other hand, the initial values were almost identical. In the following months, when supplementing with vitamin D3, there is a clear increase in the first 3 months, although between the 3rd and 5th months, a further decrease is noticeable. Without supplementation, after a slight increase after 1 month, there is a permanent decrease in the level of vitamin D deficiency after 5 months (Chart 8).
Of all examinations during the study period (n = 226), a deficit of vitamin D was found in 28% of the examinations. A vitamin D insufficiency was found in 41%, and a normal level in 31% of the examinations, and these examinations were already influenced by the supplementation of some children. At the first examination at the time of the injury (and therefore before the possible vitamin D3 supplementation), 49% of children had a deficit of vitamin D, 35% had vitamin D insufficiency, and only 16% had normal levels. Let us remember that these were healthy children—none of them were being treated for a disease that would predict a decrease in vitamin D levels, according to the inclusion criteria.
For evaluating the speed and quality of fracture healing on radiographs, we chose RUST and mRUST schemes. We believe that those schemes are also applicable to the assessment of the healing of other long bones in children (not only the tibia), given that their principle corresponds to how we normally assess the healing of bones in children (presence of a callus and/or fracture line) and these schemes give us the possibility to quantify this. However, we have not yet noticed in the literature that this assessment is commonly used in children.7 –10
When evaluating RUST and mRUST, statistically significant differences were found when comparing the vitamin D3 supplemented versus the non-supplemented group. Average values of RUST increased faster in the supplemented group compared to the non-supplemented group (p = 0.006), and mRUST values showed a similar trend (p = 0.045) (Charts 3–4).
When evaluating children with only a femur fracture, we observe better results when evaluating RUST and mRUST in the supplemented group after 1 and 3 months, but after 5 months the results are similar. In children with femur fractures, as in the only subgroup, there were no statistically significant differences in RUST (p = 0.429) or mRUST (p = 0.935) values when comparing the supplemented/non-supplemented groups. Only at the 3-month follow-up was the value of RUST (p = 0.002) and mRUST (p = 0.004) statistically significantly higher in the supplemented group compared to non-supplemented children (Charts 6–7).
In children with a forearm fracture (as in the evaluation of all children), both RUST and mRUST values are statistically significantly higher in the group with cholecalciferol (p = 0.005, respectively p = 0.019) during the entire follow-up period (Charts 9 and 10).
If we divide children into groups with a forearm fracture and with a femur fracture, it is appropriate to underline the difference between the two groups, especially in age, when the children treated in our group with an injured femur were significantly younger (median 3 years) than those with an injured forearm (median 11 years). This difference was expected due to the inclusion criteria—for femur fractures, we included children treated both with traction treatment (these tend to be younger children) and older children treated with osteosynthesis (of which there were only 20.8%, the remaining 79.2%, were treated with traction). On the other hand, in the case of forearm fractures, only children treated with osteosynthesis (which tend to be mainly adolescents) were included, while children for whom non-operative treatment was sufficient (cast only, or reduction and cast) were not included due to the longer time of cast fixation, and those tend to be younger children, before adolescence.
The effect of age on the healing speed has been repeatedly described, with fractures generally healing faster in younger children and the speed of healing decreasing with age. On the other hand, femur fractures take longer to heal (in a comparable age group) than forearm fractures. 1
Another difference that can affect the evaluation of healing by RUST and mRUST when dividing into groups according to the location of the fracture is the fact that when we evaluate the callus formation and healing of forearm fractures, sometimes two bones (radius and ulna) are covered, or each of these bones can be healed differently. The result is then the average healing of two bones and two fractures. On the femur, however, it was always only an evaluation of one bone and always without covering of another bone, and the evaluation using RUST and mRUST is therefore easier and probably more accurate.
Vitamin D levels were found to stagnate during the latter months of observation. This may be due to the time of year and composition of the child’s diet as well as that there may be hyperconsumption of vitamin D and its metabolites during fracture healing. However, this would need to be further investigated.
We did not encourage children in the study to change their diet and/or sun exposure time during the study period, but it was not monitored if they did so.
Although we warned parents that if the child is not in the supplemented group, he/she should not receive vitamin D, it is possible that to be a good parent, they administered some vitamin D “just in case.” Therefore, we should also assume the possibility of this “Hawthorne Effect.”
Some previous studies on a similar topic were performed on animals: Omeroğlu et al. 13 investigated the effect of a single high dose of vitamin D3 on fracture healing in pigs, when compared to a control group and found improved healing in the supplemented group. Delgado-Martínez et al. 14 compared the mechanical resistance of the fracture healing in a vitamin D-supplemented group versus a non-supplemented group in rats with a femoral fracture. The result was statistically significantly higher bone strength and healing in the supplemented group.
In studies that already investigate children from the available reviews of the literature, it is evident that there is a lack of studies evaluating the effect of vitamin D on fracture healing, and their results are therefore difficult to evaluate. 15 Parry et al. 16 evaluated preoperative vitamin D levels in children undergoing elective orthopedic procedures—90% of these children had vitamin D insufficiency, statistically significantly lower values were observed in African American children and those examined in winter. Older children often had the lowest levels. On the contrary, neither sex nor weight had a statistically significant effect.
Some studies have already directly followed up on the connection between the saturation of the organism with vitamin D and fractures: James et al. 17 retrospectively evaluated vitamin D levels in 181 children treated for an upper extremity fracture. 24% of children had vitamin D deficiency, 41% insufficiency, and 35% normal levels Thompson et al. 18 prospectively compared the levels of vitamin D in a group of children with a fracture and a group without, where they demonstrated a statistically significant higher incidence of low vitamin D levels in the group with a fracture. Clark et al., 19 based on the literature and their own experience with a high incidence of vitamin D deficiency in children, recommend examination of vitamin D in children treated for skeletal injuries and its adequate supplementation. El-Sakka et al. 20 represent a set of Egyptian children 3–10 years old, where 32.6% of them had vitamin D deficiency. Half of the children in the study had a forearm fracture, where 43.5% had a vitamin D deficiency, and the other half were in the control group, where “only” 21.7% had a deficiency. Contreras et al. 21 prospectively assessed vitamin D levels in 100 children with fractures from low-energy trauma and compared them to a population of 100 children without fractures. They found no statistically significant difference between the two groups. The median values for both groups were at the level of vitamin D insufficiency. Ceroni et al. 22 evaluated vitamin D levels in 100 adolescents with a limb fracture compared to 50 adolescents without a fracture. Of the injured, 12% had a deficiency, 36% had insufficiency, and 52% normal level. Of the uninjured, 6% had a deficiency, 34% had insufficiency, and 60% normal level. They therefore pointed to low levels of vitamin D in the population of their adolescents but did not evaluate the further development of laboratory values, nor the healing of fractures. Gorter et al. 23 evaluated the incidence of vitamin D deficiency in children with fractures. Of the 187 children, 34% had a deficit. Of these children, after 4 months of supplementation, 74% already had normal values. They rate older children, the spring season, and non-Caucasian skin type as risk factors. Ryan et al. 24 compared groups of African American children with and without forearm fractures (5–9 years). In their group, children with fractures were statistically significantly more likely to have vitamin D deficiency, lower bone density, and obesity. According to the review by Moon et al., 25 there is insufficient data in the literature to assess fracture risk rates in children in relation to vitamin D levels.
Thus, in all these works, children were examined and followed, but unlike our study, they were not actively supplemented.
Conclusion
In our study, all the children supplemented with vitamin D3 had statistically significantly higher vitamin D levels already after 1 month of administration. The fracture healing (measured by RUST and mRUST values) was also statistically significantly faster and better in the supplemented group compared to the non-supplemented group. When we divided children according to fracture type, we observed statistically significantly better fracture healing in children with forearm fractures in the supplemented group for the whole study period. In children with femoral fractures, the healing in the supplemented group was statistically significantly better after 3 months, however, after 1 and 5 months, the difference was not statistically significant.
We also confirmed a high prevalence of insufficient vitamin D levels in the pediatric population in general—at the time of the injury.
Therefore, based on our results, we recommend vitamin D testing and administration for children healing with femoral (treated by traction or by minimally invasive osteosynthesis) and especially forearm (treated by minimally invasive osteosynthesis) fractures. We assume similar effects on fracture healing in all locations of the pediatric skeleton, treated both operatively and non-operatively, but other studies should be designed to confirm this assumption.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241299624 – Supplemental material for The effect of vitamin D on the speed and quality of pediatric fracture healing
Supplemental material, sj-pdf-1-cho-10.1177_18632521241299624 for The effect of vitamin D on the speed and quality of pediatric fracture healing by Jan Hendrych, Petr Havránek, Milan Bayer, Martin Čepelík and Tomáš Pešl in Journal of Children’s Orthopaedics
Footnotes
Authors contributions
Jan Hendrych—design of the study, getting informed consent, planning and evaluating blood tests, statistics, evaluating results, and writing the article. Petr Havránek—design of the study, radiographs evaluation, and reviewing the article. Milan Bayer—design of the study, planning blood tests, evaluating results, and reviewing the article. Martin Čepelík—blood tests evaluation, statistics, and reviewing the article. Tomáš Pešl—radiographs evaluation, evaluating results, and reviewing the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and informed consent statements
This study was approved by the Ethics Committee of Thomayer Teaching Hospital and IKEM (Ethics Code: G-17-06-03) on June 14th, 2017. All participants (or legal representatives) provided written informed consent prior to enrolment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.