
Abstract
Background and aims:
Esophageal perforations are life threatening. Since the 1990s, placing of covered esophageal stents has become an alternative to surgery. Theoretically, this minimally invasive approach has several benefits; however, little data are available on long-term outcome in these patients. We aimed to evaluate how patient-reported outcome differed between full surgery and placement of self-expanding metallic stents when treating primary benign esophageal perforations.
Material and methods:
Of 48 patients treated at our hospital in 2000–2015, 23 were alive and asked to answer three questionnaires. We used a short clinical questionnaire, the QLQ-OG25 from the European Organization for Research and Treatment of Cancer and a simplified quality-of-life instrument, the Check Your Health. Non-parametric statistics were used to evaluate differences between the two groups.
Results:
In all, 20 (87%) individuals (13 men, 64 years of age) responded. At survey, surgical patients had lost 13 kg of initial weight, compared to no weight loss in the self-expanding metallic stents group (p = 0.01). This involuntary weight loss worried patients according to the QLQ-OG25; otherwise patient-experience measures did not differ between groups. For quality of life, surgical patients scored significantly lower physical health, emotional well-being, social functioning, and overall quality of life after treatment, but after stenting no differences were seen.
Conclusions:
In contrast to stenting, surgical treatment was associated with involuntary, and worrisome, weight loss as well as reduced quality of life. We therefore believe that self-expanding metallic stents should be used when possible in treating benign esophageal perforations.
Keywords
Introduction
Perforation of the esophagus remains a potential medical emergency of the first order (1). The risk of severe morbidity and mortality is considerable (2) and patients depend on swift (3) and proper treatment (4) to stand the best chance of survival and minimal complications (1, 5). Besides the classical Boerhaave syndrome (6), iatrogenic perforations, occurring in connection with, for example, dilatation of strictures or endoscopic exams have become more frequent (7).
Several treatment options in the management of esophageal perforation are available (8, 9). Surgical treatments include drainage and repair with interrupted sutures, with or without supporting tissue flaps, and immediate resections of the damaged area with an end-cervical esophagostomy, to be followed by later reestablishment of alimentary continuity (3, 10). At our department, the latter treatment regime has been preferred because it stops the mediastinal leakage immediately. Since the 1990s, placement of self-expanding metallic stents (SEMS) has become a treatment for primary esophageal perforations. Initially, there were some concerns regarding the outcome, but during the past 20 years, stenting has become an established way of treating even very ill patients (11–13). Little data are, however, available on long-term outcome in patients given a SEMS on this indication.
In the present study, we wanted to compare patient-related long-term outcome between initial end-cervical esophagostomy and SEMS placement in the treatment of benign esophageal perforations.
Material and Methods
We retrospectively examined our database for patients having received SEMS or an esophagostomy during the years 2000–2015 at Uppsala University Hospital, excluding esophageal cancer and anastomotic leakages. The diagnosis was validated by studying the medical charts, from which background data (age, gender, weight, presentation of disease, treatment, and outcome) were collected. Living patients at the time of the study were asked to complete a three-part questionnaire, as follows.
Questionnaires
The first part of the questionnaire contained clinical questions about weight at survey, use of proton-pump inhibitor drugs (PPIs), and instability of the left shoulder (due to the resection of the left part of the manubrium sterni and collar bone when later expanding the operative field to restore the esophageal continuity). Weight loss was calculated.
Second, the validated QLQ-OG25 instrument from the European Organization for Research and Treatment of Cancer (EORTC), intended for use in patients with cancer of the esophagus or gastro-esophageal junction, contains 25 questions on various common symptoms or problems in the gastro-esophageal tract (14). Responders indicate the extent (not at all, a little, quite a bit, and very much) to which they have experienced these symptoms or problems during the past week. According to the scoring procedure, six scales (dysphagia, eating restriction, reflux, odynophagia, pain and discomfort, and anxiety) and 9 single items (trouble eating with others, dry mouth, trouble with taste, body image, trouble swallowing saliva, choked when swallowing, trouble with coughing, trouble talking, and worry over weight loss) are calculated. The only invalid question (#25), on hair loss post radio/chemotherapy, was omitted in the distributed questionnaires (being one of the single items, this did not affect scoring on other points). All scores were linearly transformed to a 0–100 score according to the EORTC scoring manual (15).
Finally, using a simplified quality of life (QoL) instrument, Check Your Health (16), patients were asked to rate their physical health, emotional well-being, social functioning, and overall QoL on a visual analogue scale (0–100) at the time of the survey as well as how they imagined it if the perforation had not occurred.
Statistics
Data are presented as median and range, and in absolute number and percent (%), when applicable. Statistical differences between the two treatment groups were studied by Chi-square test, and Wilcoxon and Mann–Whitney U-test due to the small numbers. A p < 0.05 was considered statistically significant. The study was approved by the regional ethical committee in Uppsala (Dnr 2016/259). All included patients gave written informed consent.
Results
Of 48 patients fulfilling our inclusion criteria, 23 were alive when the study was done, of which 20 (87%) answered our questionnaires. Median follow up was 7 (2–16) years.
As demonstrated in Table 1, demographics did not differ between the two groups (10 surgical treatment and 10 stent), nor did the etiology or diagnostic delay of the esophageal perforation. All perforations occurred in the distal part of the esophagus, and in surgical patients an end-cervical esophagostomy (with resection of the damaged part of the esophagus) was performed. Surgical patients reported a significant weight loss of 13 kg at the time of survey (p = 0.018) as well as compared to no weight loss in the stent group (p = 0.011). Both groups use PPIs to the same degree (50%), and no difference was seen in shoulder instability, 40% versus 20% (p = 0.329).
Demographics and results of the short clinical questionnaire.
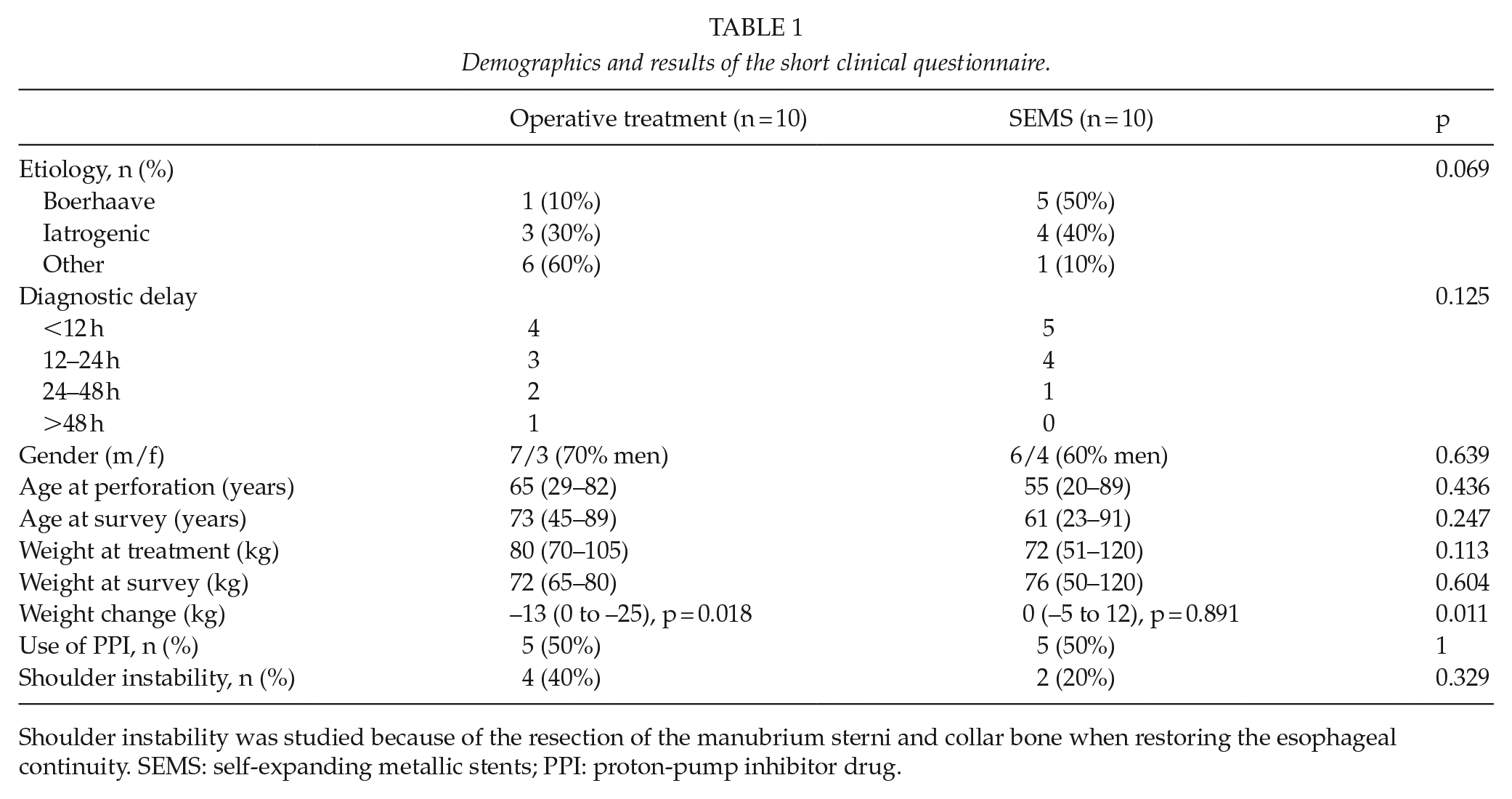
Shoulder instability was studied because of the resection of the manubrium sterni and collar bone when restoring the esophageal continuity. SEMS: self-expanding metallic stents; PPI: proton-pump inhibitor drug.
In the QLQ-OG25, worry about involuntary weight loss was scored higher in the surgical group (p = 0.033), but there were no other differences (Table 2).
Results of the EORTC QLQ-OG25 according to the standardized protocol. All responders (N = 20). Scale 0–100, higher score is worse.
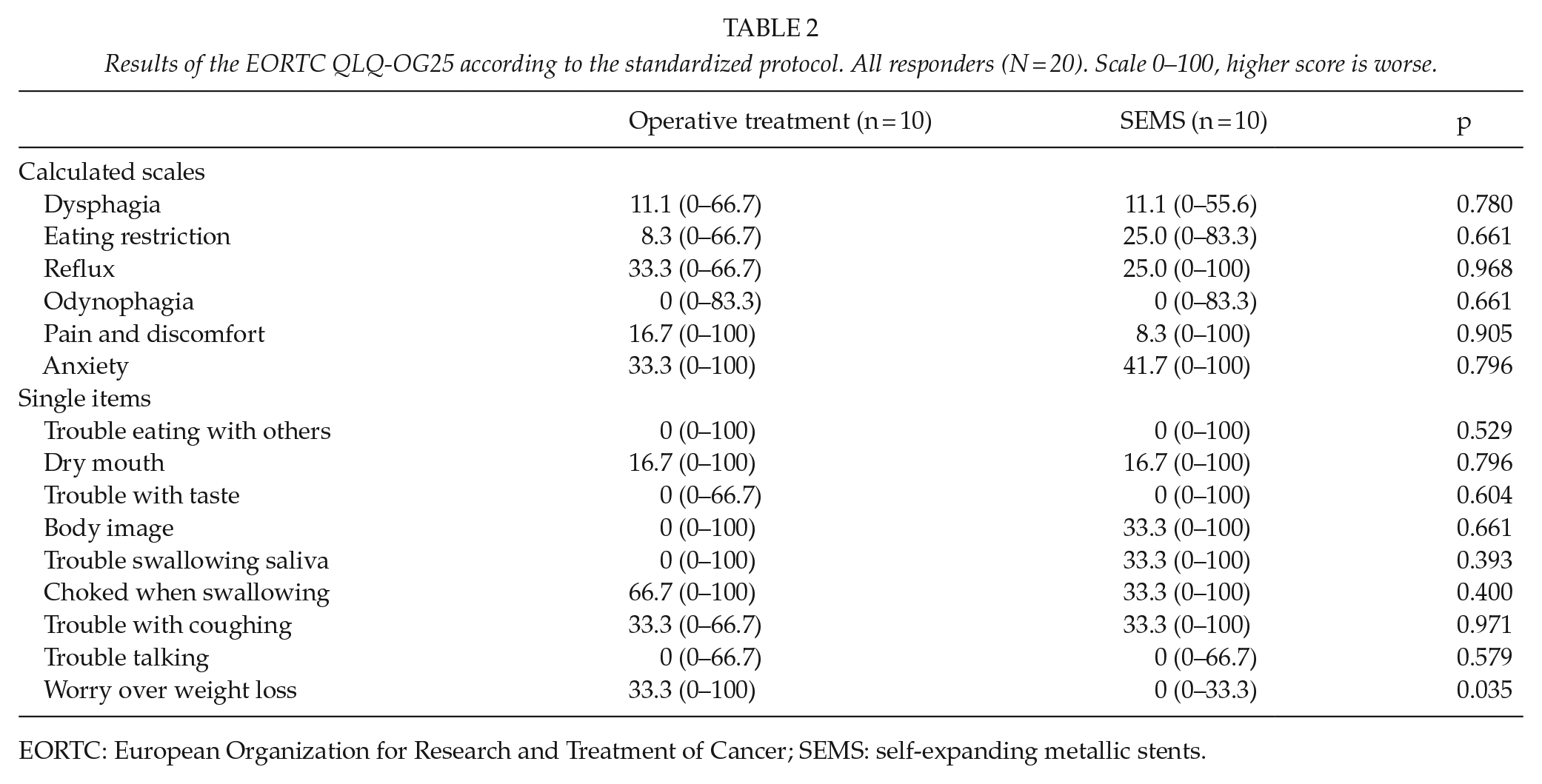
EORTC: European Organization for Research and Treatment of Cancer; SEMS: self-expanding metallic stents.
For QoL, surgical patients scored almost halved physical health, emotional well-being, social functioning, and overall quality-of-life scores after treatment, but there were no differences after stent grafting. Table 3.
Patient reported QoL today versus their imagined score, if not suffering an esophageal perforation. Results from the Check Your Health questionnaire. Scale 0–100, higher score is better.
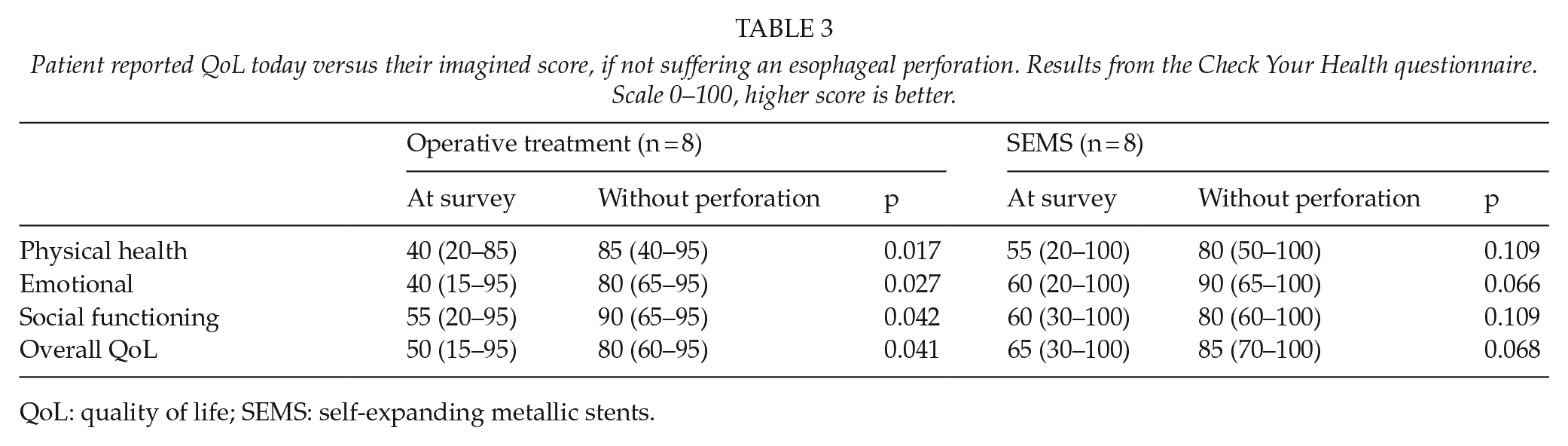
QoL: quality of life; SEMS: self-expanding metallic stents.
Discussion
In contrast to stenting, patient-reported outcome after surgical treatment led to involuntary, and worrisome weight loss, as well as reduced QoL. The etiology of perforation as well as age and gender are similar between the groups in our present study and typical for the condition (17). It seems reasonable to assume that there has been a “natural” selection of patients: those with small, probably iatrogenic, perforations will be better suited for stent treatment whereas those with an esophageal rift and gross contamination of the mediastinum will require surgery (2, 12). This assumption is not, however, borne out by the data. In fact, almost all Boerhaave patients among responders had received stent treatment. However, in line with the literature, our overall early mortality rate in all patients with an acute esophageal perforation was high, 30.4% and 31.8%, respectively.
Although beyond the scope of this article, it is important to mention that stent-treated patients often need repositioning of their stent, particularly during the first few days, and adequate drainage of the pleural cavity. In a systematic review of treatment options in patients with a leaking esophagus, the use of SEMS was successful in 88% of 371 patients (18). If an end-cervical esophagostomy is performed, the patient will need a second procedure to restore the alimentary continuity, when in good shape (10). Two possibilities exist, reconstruction with a gastric tube as used in malignant resections (10) or a colonic interposition (19). In this study, a gastric pull-up was used in all cases, but one.
The present questionnaire comprised of three parts as described above: questions on typical aspects of life that are often affected by esophageal injuries and their treatment (weight loss, use of PPIs, post-operative shoulder instability); second, a validated questionnaire (QLQ-OG25); and third, a QoL instrument in which responders are asked to rate their current QoL on four points versus how they imagined it without their illness.
Both our groups used PPIs to the same degree (50%). Patients operated for esophageal cancer, typically having a gastric tube connected to the cervical esophagus, usually suffer from acid reflux to a larger extent, while the use of SEMS should leave an intact gastro-esophageal sphincter. The high use of PPI in the stent group could depend on the underlying disease, for example, hiatal hernia with distal esophageal stenosis due to severe reflux, leading to an iatrogenic perforation. Moreover, the use of PPI is common in the general population. PPI has been prescribed to 17.5% of all Swedes between 60 and 69 years according to the Prescribed Drug Registry, kept by the National Board of Health and Welfare (20) and different PPIs are also available over the counter. Finally, the rate of shoulder instability (40%) was somewhat lower in the operated patients than we expected after removal of the bone structures and stabilizing ligaments around the left sternoclavicular (21).
In the QLQ-OG25, the two groups responded similarly, except that the weight loss in the surgical patients caused them concern (score 33.3 vs 0, p = 0.035). The weight loss is not surprising because most patients having a gastric pull-up or similar reconstruction, for example, after resection of a cancer in the esophagus or gastro-esophageal junction, often lose up to 10% of their total body weight due to changed eating habits (22). In line with this, no patient in the surgery group gained weight after treatment, whereas patients in the stent group gained up to 12 kg body weight. In comparison with the general Swedish population, the present scores are higher in both groups, both when compared to an age-matched cohort (23) and a group without known malignancy (n = 4497) (23). In patients diagnosed with cancer of the esophagus or gastro-esophageal junction (n = 214), the intended use of the questionnaire, all individual scores were higher than in our patients (14).
In QoL terms, the surgery group is more pessimistic on all counts: they feel a significant loss of physical health, emotional well-being, social interactions, and overall QoL. Because both groups rated their imagined current QoL (if not having an esophageal perforation) similarly, this implies that a gastric pull-up affects life negatively, even after many years. In a recent study from Norway on iatrogenic esophageal perforations, the 10 patients alive (47.6%) after median of 82 months still reported reduced health-related QoL as well as fatigue, when compared to a reference population (24).
Limitations
Despite covering 15 years, our study included only 48 patients, of which 23 were alive at the time and 20 responded to the questionnaire. Such small numbers of patients give limited strength to any statistical measures, although the response rate to the questionnaire was high. However, a large meta-analysis found that studies in this field have on average 39 included patients (17) and to find additional differences in the present study, much larger groups would be needed. Moreover, in a sensitivity analysis on our initial 43 patients, the included patients and non-survivors did not differ significantly for etiology, gender, and age at the time of the esophageal perforation. When studying the original questionnaires, it appears that some patients found the final QoL questions difficult. However, despite the small number of responding patients (n = 8 in each group), both groups rated their imagined current levels of QoL, if they had not fallen ill, very similarly.
Conclusion
In contrast to stenting, surgical treatment was associated with an involuntary, and worrisome, weight loss of 13 kg as well as significantly reduced QoL. SEMS should therefore be used, when possible, in treating benign esophageal perforations to obtain better long-term results.