
Abstract
Background and Aims:
The effect of operation volume on the outcomes of pancreatic surgery has been a subject of research since the 1990s. In several countries around the world, this has led to the centralization of pancreatic surgery. However, controversy persists as to the benefits of centralization and what the optimal operation volume for pancreatic surgery actually is. This review summarizes the data on the effect of centralization on mortality, complications, hospital facilities used, and costs regarding pancreatic surgery.
Materials and Methods:
A systematic librarian-assisted search was performed in PubMed covering the years from August 1999 to August 2019. All studies comparing results of open pancreatic resections from high- and low-volume centers were included. In total 44, published articles were analyzed.
Results:
Studies used a variety of different criteria for high-volume and low-volume centers, which hampers the evaluating of the effect of operation volume. However, mortality in high-volume centers is consistently reported to be lower than in low-volume centers. In addition, failure to rescue critically ill patients is more common in low-volume centers. Cost-effectiveness has also been evaluated in the literature. Length of hospital stay in particular has been reported to be shorter in high-volume centers than in low-volume centers.
Conclusion:
The effect of centralization on the outcomes of pancreatic surgery has been under active research and the beneficial effect of it is associated especially with better short-term prognosis after surgery.
Introduction
The prognosis of pancreatic cancer is poor with an overall 5-year survival rate of 5%. It is noteworthy that if the tumor is detected early, the prognosis improves and 5-year survival as high as 30% can be achieved. Surgery coupled with oncologic therapy is the best option for patients in terms of survival. Pancreatic surgery is, however, high-risk surgery with over 40% postoperative morbidity rates and 0%–15% postoperative mortality rates. In recent years, financial pressure has also reached health care organizers to search more cost-effective ways to take care of patients. The effect of the centralization on pancreatic surgery has been a subject of research worldwide since the 1990s. This review gathers published data on the effects of the centralization of pancreatic surgery on prognosis and cost-effectiveness.
Material and Methods
A systematic librarian-assisted data search in PubMed database was performed covering the time span from August 1999 to August 2019. Both Mesh terms and free text terms in pancreatic surgery, operation volume, and centralization were used as search terms. The search yielded 141 articles which were manually evaluated. Studies comparing mortality, morbidity, complication distribution, pathologic reporting, long-term survival, and/or costs in open pancreatic resections (PRs) (total pancreatectomy, pancreatoduodenectomy (PD) or distal pancreatectomy (DP), or the combined results of these) between different volume groups were included. Studies not available in English were excluded, likewise those which did not involve pancreatic surgery or did not report results in relation to operation volume. No specific criterion was used in defining high-volume center (HVC) or low-volume center (LVC). A PRISMA flowchart was drawn. The results of the studies were summarized in five categories: mortality, complications and failure to rescue, usage of hospital facilities, long-term survival, and quality of pathology.
Results
Included Studies
The systematic search yielded 141 studies. The search history is shown in Supplement 1. After exclusion, 44 studies were included, see flowchart in Fig. 1. Eight studies were published on the Nordic countries and 16 on other parts of Europe. In addition, the search found 1 study from Japan, Taiwan, and Australia and ten 14 from North America. The search found five systematic reviews or meta-analyses of which four concentrated on the outcomes of surgery and one on methodological evaluation.
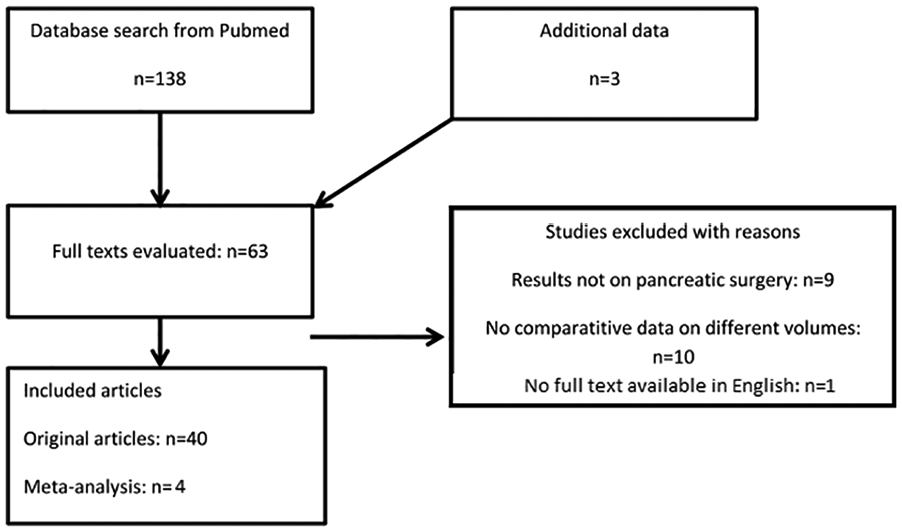
Flowchart of included studies.
Definition of HVC
Several criteria have been proposed in the literature and no consensus has been reached. In studies from the Nordic countries (1–4), LVC has been defined as center performing under 5–10 PDs annually except in one study (5), which analyzed the data with a cutoff of 40 PDs. The definition of an HVC varied between 20 and 40 PDs per year in these same studies. Data on distal resections are sparse, but one study analyzed their centralization with an HVC cutoff of 10 annual distal resections (6). Other European studies (7–19) have set the cutoff for an HVC at 15 to 77 PDs per year and for LVC at under 16 PDs per year. Studies in the United States of America and Canada (20–28) have also presented a wide range for both HVCs and LVCs, from 3 to 22 PDs per year for LVCs and from 16 to 97 PDs per year for HVCs. A recent Japanese study (29) categorized hospitals with at least 18 PDs per year as HVCs and a maximum of 11 PDs per year as LVCs (Table 1).
Reported mortality rates in different volume groups.
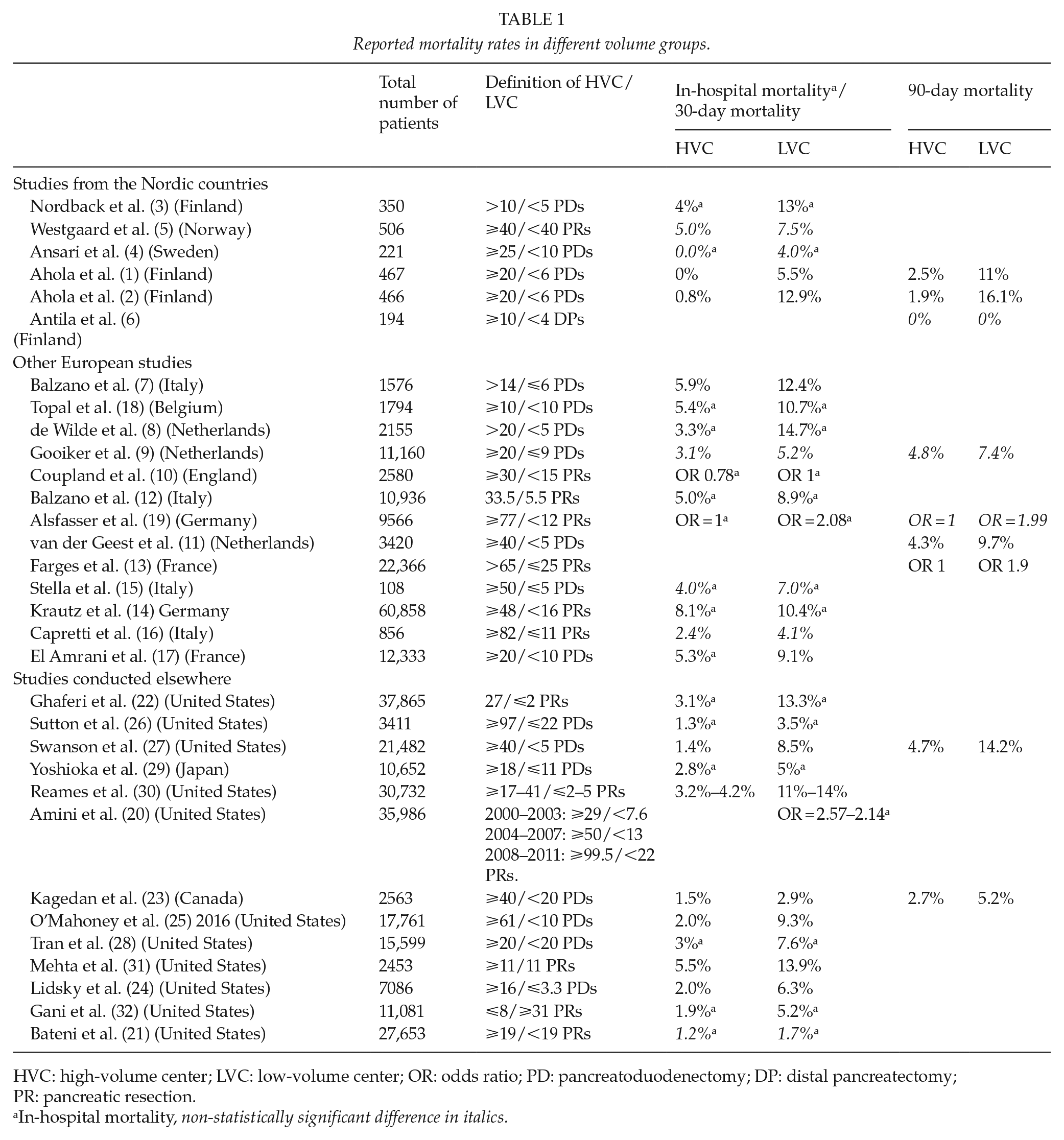
HVC: high-volume center; LVC: low-volume center; OR: odds ratio; PD: pancreatoduodenectomy; DP: distal pancreatectomy; PR: pancreatic resection.
In-hospital mortality, non-statistically significant difference in italics.
Effect of Operation Volume on Postoperative Mortality
The effect of operation volume on mortality has been described in several studies: the data search found 33 studies reporting either mortality rates or hazard ratios for mortality in relation to hospital volume (Table 1). The reported 30-day mortality rate or in-hospital mortality rate was 0%–8.1% in HVCs and 3.5%–15% in LVCs in the published studies. The 90-day mortality rate varied from 0% to 5.3% in HVCs and 9.3% to 16.1% in LVCs. Overall, studies report lower mortality rates in HVCs than in LVCs despite the heterogeneity of the volume criteria, but statistical significance was not reached in all studies on PRs, see Table 1. The mortality rates after PD (see Fig. 2) resemble those for overall mortality after PR, probably due to the high proportions of PDs among the data of PRs. A recent meta-analysis by Hata et al. (33) pooled 13 studies and categorized studies according to different HVC criteria into three groups: HVC > 19 PDs/year, HVC 20–29 PDs/year and HVCs ⩾ 30 PDs/year. Analysis of each group demonstrated a strong inverse association between operation volume and mortality. The pooled odds ratio (OR) in HVC > 19 PDs/year group was 1.94 (1.66–2.26), in HVC 20–29 PDs/year 2.34 (1.81–3.03), and HVCs ⩾ 30 PDs/year 4.05 (1.96–8.34). Van Rijssen et al. (34) studied factors associated with postoperative mortality after PD among patients with suspicion of malignancy. They categorized hospitals not according to the operation volume but according to mortality. They found that male sex, age >75 years, body mass index (BMI) ⩾30, histopathological diagnosis of periampullary cancer, and hospital volume were independent risk factors for failure to rescue.
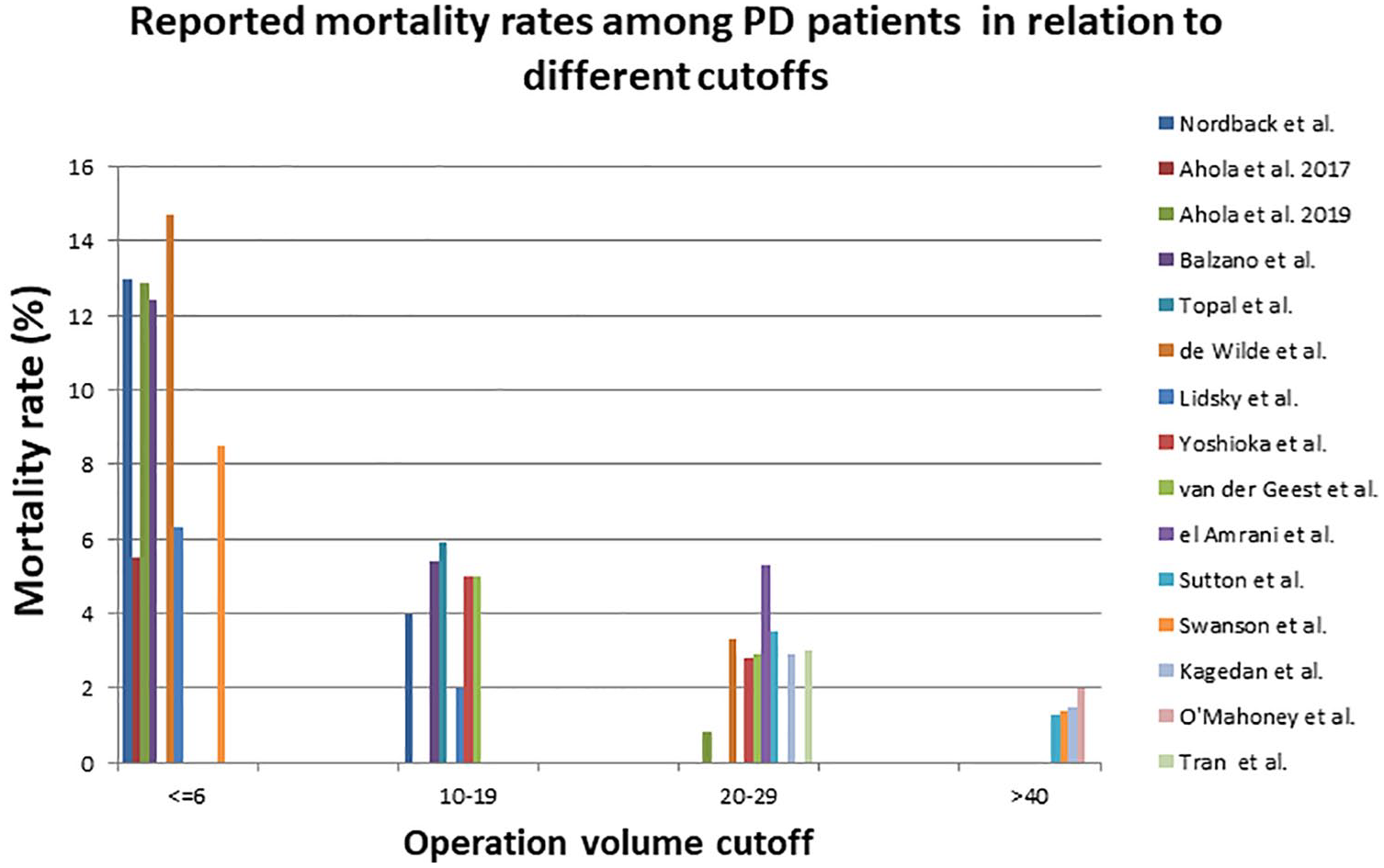
Reported mortality rates among PD patients.
A Swedish study by Derogar et al. (35) described the effect of teaching status and hospital volume on pancreatic surgery results in five operation volume categories. Most of their data comprised PDs (85%), but other pancreatic surgery was also included. They found only one significant difference: a decreased hazard ratio (HR) for 90-day mortality among hospitals performing four to six PRs per year when compared with a group performing a maximum of three PRs per year. They found a strong association between university hospitals and overall mortality favoring university hospitals (p = 0.007). However, the data also included patients from the beginning of 1990, which may have affected the results.
Effect of Operation Volume on Postoperative Complications and Failure to Rescue
High operation volume was associated in several studies with fewer overall complications. Amini et al. (20) gathered data on PRs from the American NIS database (Nationwide Inpatient Sample) covering some 20% of the community and teaching hospitals in United States. They stated that the OR for morbidity was 1.39–1.47 in low or medium volume centers compared with HVCs. Bateni et al. (21) (27,653 patients) and Mehta et al. (31) (2453 patients) analyzed the postoperative results of PRs and concluded that there were significantly more overall complications in LVCs than in HVCs. Mehta et al. (31) added that surgeon volume is also an independent risk factor for 30-day complication rate. A French nationwide study by El Amrani et al. (17) covering 12,333 patients reported that there was more septic, thromboembolic and hemorrhage complications in LVCs than in HVCs after pancreatic surgery. Ansari et al. (4) found the same in a Swedish study comprising 212 patients undergoing PD that hemorrhage complications especially are more common in LVCs than in HVCs and more blood transfusions are needed in LVCs. PDs were also analyzed by Tran et al. (28) in a study of 15,599 patients. These authors added that cardiological, pulmonary, and nephrologic disorders are more likely to occur in LVCs. Antila et al. (6) researched distal resections in a Finnish nationwide study and found that more delayed gastric emptying and grades B/C pancreatic fistulas occur in LVCs than in HVCs.
The series by Ahola et al. (2) (466 PD patients) and Stella et al. (15) (108 PD patients) found no significant difference in the incidence of complications. However, Ahola et al. (2) demonstrated that fatal complications occur more often in LVCs than in HVCs. El Amrani et al. (17) agreed, stating that in addition to the higher incidence of septic and thromboembolic complications, more patients are lost in LVCs than in HVCs if these complications occur. The failure-to-rescue pattern has also been mentioned in American studies reporting results from the NIS database (11,081 PR patients) (32) and Medicare data (3405 PR patients) (22). Gani et al. (32) reported that in HVCs (over 30 PRs/year), 5.4% of the cases presented a failure-to-rescue pattern versus 11.1% in LVCs (under 8 PRs/year). Ghaferi et al. (22) added that the risk of failure-to-rescue is 3.12-fold in LVCs (max five PRs/year) versus HVCs (>27 PRs/year).
Effect of Operation Volume on Long-Term Survival among Pancreatic Cancer Patients
While the beneficial effect of centralization on short-term prognosis has been shown in several studies, the role of operation volume on long-term survival among pancreatic cancer patients has been controversial. The data search resulted in eight studies describing the effect of operation volume on either median survival or survival rates among pancreatic cancer patients. Lidsky et al. (24) concentrated on PDs among 7086 pancreatic cancer patients and Ahola et al. (1) reported survival after PRs among pancreatic ductal adenocarcinoma (PDAC) patients. Both studies resulted in significant differences in the median survival between LVCs and HVCs (16 months in LVCs vs 20–26 months in HVCs). In addition, Gooiker et al. (9) added in their analysis of 11,160 PD patients that 1- and 2-year survival is higher among patients operated on in HVCs than in LVCs (1-year survival 72% vs 57% and 2-year survival 40% vs 31%). Risk for 1-year mortality was also analyzed by Alsfasser et al. (19) in a study covering 9566 patients undergoing pancreatic surgery. They stated that OR is 1.37–1.73 in centers performing fewer than 77 PRs per year, but the data also included benign diseases, which challenges the interpretations of the results. Westgaard et al. (5) showed that 5-year survival among PDAC patients undergoing PD may be higher in HVCs than in LVCs, 26% versus 13%. However, Waterhouse et al. (36) with data on 270 and Derogar et al. (35) with data on 3298 PRs found no association between hospital volume and long-term survival in their survival analyses. Waterhouse et al. (36) reported that patients operated on by surgeons performing fewer than four PRs per year had higher mortality rates and lower survival rates up to 1.5 years after surgery.
Effect of Operation Volume on Pathology Reports
The studies published on the quality of pathology demonstrated the beneficial cumulative effect of high operation volumes on pathological analyses. Four studies reported results on differences in pathological analyses or reporting. Onete et al. (37) reported that less information on tumor size or stage was found in the pathology reports in LVCs than in HVCs. This was corroborated by Ahola et al. (1) and Westgaard et al. (5), who added that tumor margin clearance evaluation was also more detailed in HVCs than in LVCs. These studies were based on data prior to 2010. A more recent study by Lidsky et al. (24) covering the years up to 2012 agreed with these authors that lower number of lymph nodes were detected in LVCs than in HVCs. Standardization of pathology reporting has been shown to improve the quality of the analysis of PRs (38).
Use of Hospital Facilities
The effect of operation volume on the use of hospital facilities has been described in terms of length of hospital stay or stay in intensive care and reinterventions. Studies on PD patients (4) and distal resections (6) have presented that more re-operations are performed in LVCs than in HVCs. However, Ahola et al. (2) studying PD patients in a Finnish nationwide study and Stella et al. (15) concentrating on PRs found no significant difference between volume groups in frequency of re-operations among PD patients. A large study by Bateni et al. (21) comprising 27,653 patients undergoing PR revealed that re-admission is more common among patients operated on in LVCs than in HVCs. This was confirmed by Sutton et al. (26) in a survey of 9805 PD patients. Length of hospital stay was also analyzed in several studies resulting in the conclusion that hospital stay is shorter in HVCs than in LVCs (4, 16, 18, 21, 23–26, 29, 32, 39). In addition, Ahola et al. (2) reported that hospital stay among Clavien-Dindo grade III patients was longer in LVCs than in HVCs. However, the Italian study by Stella et al. (15) found no significant difference between LVCs and HVCs in terms of hospital stay after a PR. However, the comparison of studies is difficult without in-depth knowledge of the health system in each country.
Effect of Operation Volume on Costs
The data search found nine retrospective studies and one meta-analysis on costs after pancreatic surgery. Ke et al. (40) published a systematic review of 19 studies on the effect of operation volume on costs in cancer surgery. The systematic review concluded that high operation volume leads to lower health care costs, but the evidence is inconsistent: 6/10 studies reported an inverse relationship between hospital volumes and costs, 3/10 a parallel relationship, and one study no volume-related relationship. More recently, a retrospective study by Sutton et al. among PD patients (26) reported that high operation volume leads to significant cost savings among pancreatic cancer patients. The association was also apparent in several other studies reporting their results either on pancreatic cancer patients (29, 39) (total of 14,691 patients) or all patients (2, 28, 41) (total of 16,387 patients). Enomoto et al. (45) added in an analysis of 3137 patients from the NIS database that the costs for patients treated by low-volume surgeons at LVCs are higher than those for patients treated by low-volume surgeons at HVCs. On the contrary, large retrospective series by Gani et al. (32) (11,081 PR patients) and Bateni et al. (21) (27,653 PR patients) found no significant association between costs and operation volume.
Cost-benefit has not been widely reported. Ahola et al. (2) analyzed the cost-benefit association among pancreatic cancer patients by dividing costs by survival. The analysis showed that costs per survival are lowest among pancreatic cancer patients operated on at HVCs (Table 2).
Studies on relation of costs and pancreatic resection volume
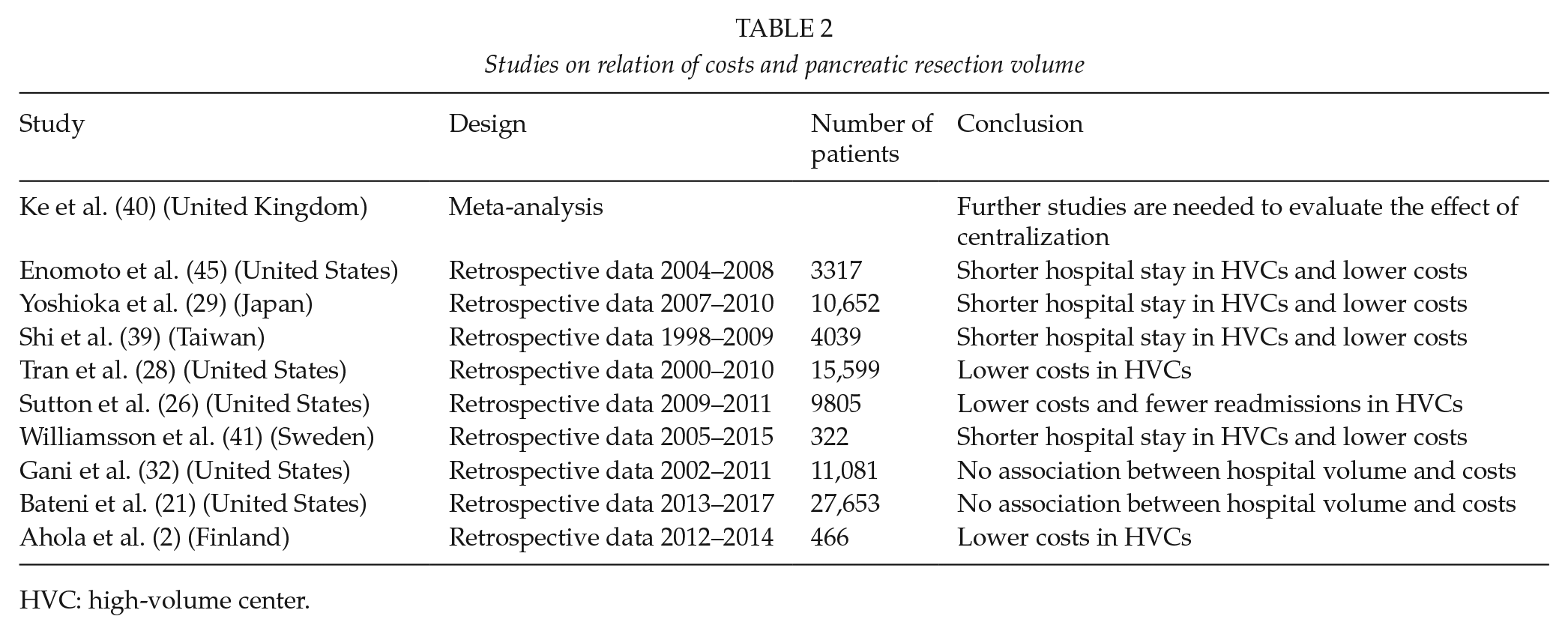
HVC: high-volume center.
Systematic Reviews and Meta-Analyses on Short Term Prognosis after a Pancretic Resection
The search identified four systematic reviews or meta-analyses. Tol et al. (42) screened reviews published between 1980 and 2012. They analyzed data in two categories: adjusted and non-adjusted data and discovered an inverse association between high operation volume and mortality. In addition, adjusted survival data also showed longer survival in HVCs. Hata et al. (33) studied articles published between 2001 and 2014 and analyzed the volume effect on mortality, complications, and hospital stay and agreed on a strong inverse association between mortality and hospital volume. Saulle et al. (43), concentrated on analyzing hospital and surgeon volume. They reported that high surgeon volumes in HVCs result in beneficial outcomes, but that low surgeon volumes in HVCs also result in lower mortality, fewer complications, and shorter hospital stay than in LVCs with low surgeon volumes. Halm et al. (44) performed a critical appraisal of the analysis of volume effect in 2002 and reported the problems of apparent variance in the study methods of different studies. The more recent meta-analysis mentioned above agreed that differences in the study settings limit the interpretations of the meta-analysis and, as shown in this review, still challenge the comparison of different studies.
Conclusion
The effect of hospital and surgeon volumes on the prognosis after a PR has been a subject of active research. The definition of HVC or LVC varies between studies, which complicates the comparison of different studies and no clear uniform criteria can be set. Despite the differences in the cutoffs, the published data highlight the beneficial effect of high operation volumes on mortality and failure-to-rescue. This may mirror the effect of cumulative knowledge, not only among surgeons, but among assisting specialities such as anesthesiology, intensive care, interventional radiology, and pathology in HVCs. It is noteworthy that many high-volume pancreatic surgery centers may also have high volumes in other fields of medicine and surgery. This may result in better availability of resources and personnel. These mechanisms speak for the centralization of high-risk surgery, such as pancreatic surgery.
Supplemental Material
supplement_1 – Supplemental material for Centralization Of Pancreatic Surgery Improves Results: Review
Supplemental material, supplement_1 for Centralization Of Pancreatic Surgery Improves Results: Review by R. Ahola, J. Sand and J. Laukkarinen in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
We thank librarian Jaana Isojärvi for assisting the data search and Virginia Mattila for proofreading.
Declaration Of Conflicting Interests
Authors have work experience in a high-volume center.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.