
Abstract
Background and Aims:
Patients who develop infections of the pleura have several risk factors for malignancies, particularly lung cancer, and the infections might even be caused by undiagnosed intra-thoracic neoplasms. The aim of the study was to compare the occurrence of lung cancer and other malignancies between patients treated for pleural infections and controls during long-term follow-up.
Materials and Methods:
All consecutive patients treated for pleural infections between January 2000 and June 2016 at the Tampere University Hospital were included. Ten matched controls and data regarding later cancer diagnoses were requested from national registries. The cancer types and rates, the diagnostic delays, as well as survival were compared between patients and controls.
Results:
The material comprised 506 patients and 5022 controls (78% was male and median age was 60 years in both groups) with a median follow-up time of 69 months. In total, 74% of pleural infections were related to pneumonia. The occurrence of lung cancer during follow-up was 3.0% in all patients, 2.2% in pneumonia-related cases, and 0.6% in controls, p < 0.001 when compared with controls. The overall rate of non-pulmonary malignancies did not differ. Lung cancer was diagnosed within 3 months in 73% of patients versus in 6.9% of controls, p < 0.001. The survival in patients with later lung cancers or other malignancies was inferior to that of controls with similar neoplasms.
Conclusion:
The rate of lung cancer diagnoses was significantly increased in patients treated for pleural infections when compared with matched controls and the prognosis of patients with subsequent malignancies was impacted.
Introduction
Infections of the pleura are increasingly common and a substantial burden for health care as the disease often necessitates long hospitalization, lengthy antimicrobial regimens, pleural drainage, and even surgery (1–4). Most cases are related to pulmonary infections, but malignancies and other causes play a role as well (1). The overall long-term survival of these patients is impacted, and the authors have previously reported that the rate of cancer-related deaths was approximately twofold in these patients when compared with that of age- and gender-matched controls (5, 6). Particularly risk factors for lung cancer, such as smoking and chronic pulmonary disease, are frequent in these patients. Furthermore, pulmonary infections and subsequently those of the pleura may be caused by undiagnosed intra-thoracic malignancies that become apparent later.
The authors hypothesize that the occurrence of malignancies, particularly lung cancer, is increased in patients treated for pleural infections. The primary aim of this study was to compare the occurrence of lung cancer between patients treated for pleural infections to that of controls and the secondary aim of the study was to compare the incidence of other malignancies, respectively.
Methods
The study comprised patients treated for pleural infections in the Tampere University Hospital, a tertiary referral clinic and the second largest University Hospital in Finland, and included all consecutive cases, both surgically and conservatively treated, that were hospitalized between January 2000 and June 2016. The patients were retrospectively identified from the institutional database by reviewing all cases that were associated with the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10), diagnosis code or any subcode of “I86.” The criteria for the diagnosis of pleural infection consisted of a pleural effusion of significant size that was associated with clinical signs of infection as well as those in the pleural fluid analysis, that is, frank pus or positive bacterial culture, stain, or polymerase chain test, elevated lactate dehydrogenase (LD) (>1000 IU/L), low pH (<7.2), and/or low glucose (<2.2 mmol/L). Pediatric patients were excluded.
The demographics and relevant medical history of each patient were recorded. Prior malignancies were classified as present when they had not been definitely treated or had recurred and as previous when curatively aimed treatment had been given and no signs of recurrences had occurred prior to the onset of pleural infection. The etiology of pleural infection was classified as pneumonia, traumatic, iatrogenic, malignant, or other/unknown according to disease history and clinical findings during the treatment period. If an ipsilateral intra-thoracic malignancy had been previously diagnosed or was detected during the treatment period of pleural infection and there was no other apparent cause for the infection the case was classified as malignancy associated. The treatment of pleural infections was classified as either conservative, drainage only, or surgical. Surgical treatment was performed by either open thoracotomy or video assisted thoracic surgery (VATS). The length and course of the hospitalization, as well as the results of the most important laboratory and imaging studies were recorded. Chest computed tomography was routinely obtained in the diagnostic work-up. Bronchoscopies were not habitually performed except to treat mucus retention and pulmonary atelectasis in select cases.
Ten individual controls for each patient matched for age, gender, and the location of residence at the time of the patients’ study inclusion, that is, the hospitalization date for the pleural disease, as well as the survival data of all patients and controls were requested from the Finnish Population Register Center. Less than ten controls were obtained for altogether seven patients who were included in the analysis. The details of later lung cancers, that is, malignant neoplasms associated with the code or any subcode of “C34,” and other malignant diseases reported after the hospitalization date of the treatment episode for pleural infections in patients and the corresponding date in controls that had been reported until the end of 2016 were obtained from the Finnish Cancer Registry, the national registry that contains robust data of all diagnosed cancer cases in Finland. In the statistical analysis, the cancers were categorized according to the organ of origin in accordance with the ICD-10 classification of malignant neoplasms.
The rates of occurrence of lung cancer and other types of malignancies, the disease grades, as well as the delay for the diagnoses of malignant diseases was compared between patients and controls using statistical methods. When more than one malignancy was diagnosed in a study subject, the delay was calculated for the earliest one and in cases with multiple cancers, the highest cancer grade was reported, separately for pulmonary and other malignancies. The survival rates were calculated for patients and controls with complete follow-up at each time point.
The study was performed according to the Helsinki declaration and institutional review board approval was obtained. The statistical testing was performed using IBM SPSS version 23 (IBM corp, Armonk, NY, USA). Categorical variables were compared using the Chi-square and Fishers Exact test, while non-parametric variables were compared using the Mann–Whitney U-test. Kaplan–Meier graphs and the Log-Rank test were used to compare the occurrence of cancer during the follow-up. Statistical significance was set at p < 0.05.
Results
The Occurrence of Lung Cancer
The study material is presented in Table 1. The median follow-up time was 69 (range 6–202) months and the overall mortality during the follow-up was 40% in patients and 17% in controls, p < 0.001. The rate of lung cancer diagnoses was significantly higher in patients treated for pleural infections than in controls during follow-up (Table 2). The malignancy was reported within 3 months after study inclusion in 73% of all patients, in 63% of patients with pneumonia-associated disease, and in 6.9% of controls, p < 0.001 and p = 0.002 when compared with controls, respectively (Fig. 1). Most lung cancers—83% of cases with available data regarding laterality—were reported on the same side as the pleural infection had occurred. Altogether 80% of patients and 73% of controls with lung cancers had a locally advanced disease with regional lymph node involvement or distant metastases and/or tumor invasion to adjacent organs present at the time of diagnosis, p = 0.999. Patients in whom lung cancer was diagnosed had statistically inferior early survival when compared with that of controls with lung cancer (Fig. 2). Lung cancer was more frequently reported in patients with immunosuppressive medications, 10% versus 2.2% in other patients, p = 0.002, and there was a high-significant trend for more advanced age in those patients that later developed lung cancer when compared with other patients, median 67 years versus 59 years, p = 0.053, respectively. There were no other statistically significant associations between the recorded patient characteristics, including smoking history, pulmonary and cardiovascular diseases, or the history of malignant diseases, with the later diagnosis of lung cancer. The proportion of non-surgical treatment—that is, conservative or drainage only—for the pleural infection was higher in patients that were later diagnosed with lung cancer—33% versus 15% in other patients, p = 0.047.
The patient and control demographics and the medical history, disease classification, and outcomes of patients.
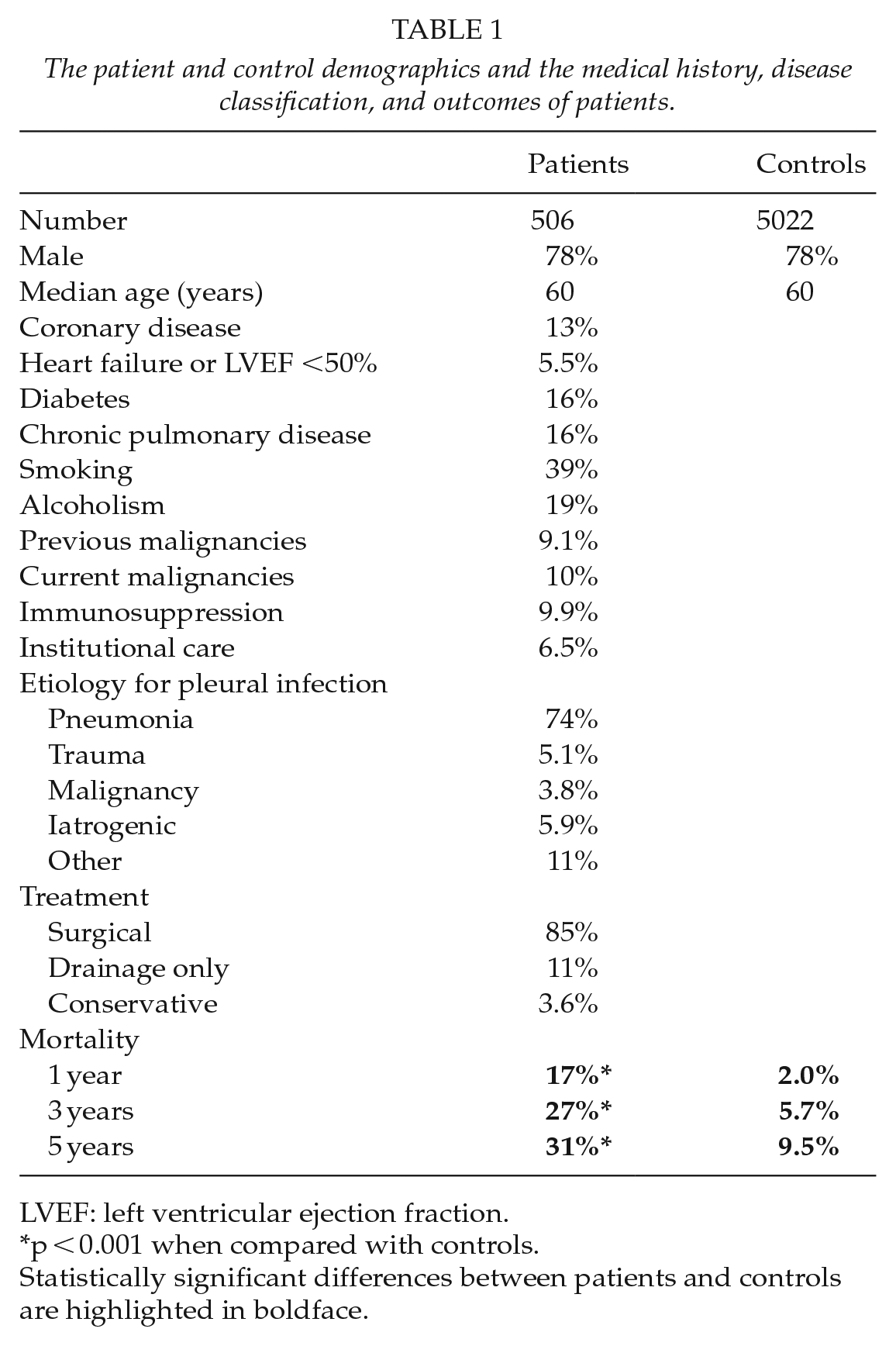
LVEF: left ventricular ejection fraction.
p < 0.001 when compared with controls.
Statistically significant differences between patients and controls are highlighted in boldface.
The occurrence of lung cancer and other malignancies during follow-up in all patients, patients with pleural infections due to pneumonia, and controls. Statistical analyses were made comparing the respective occurrence to that of the controls.
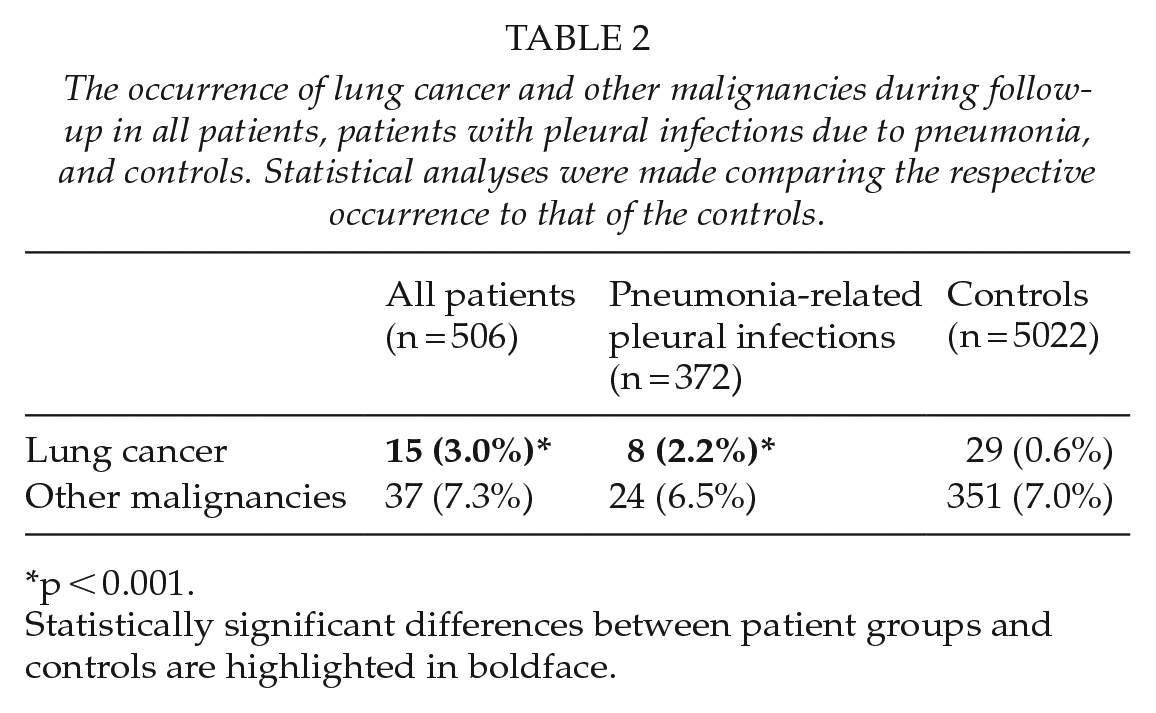
p < 0.001.
Statistically significant differences between patient groups and controls are highlighted in boldface.
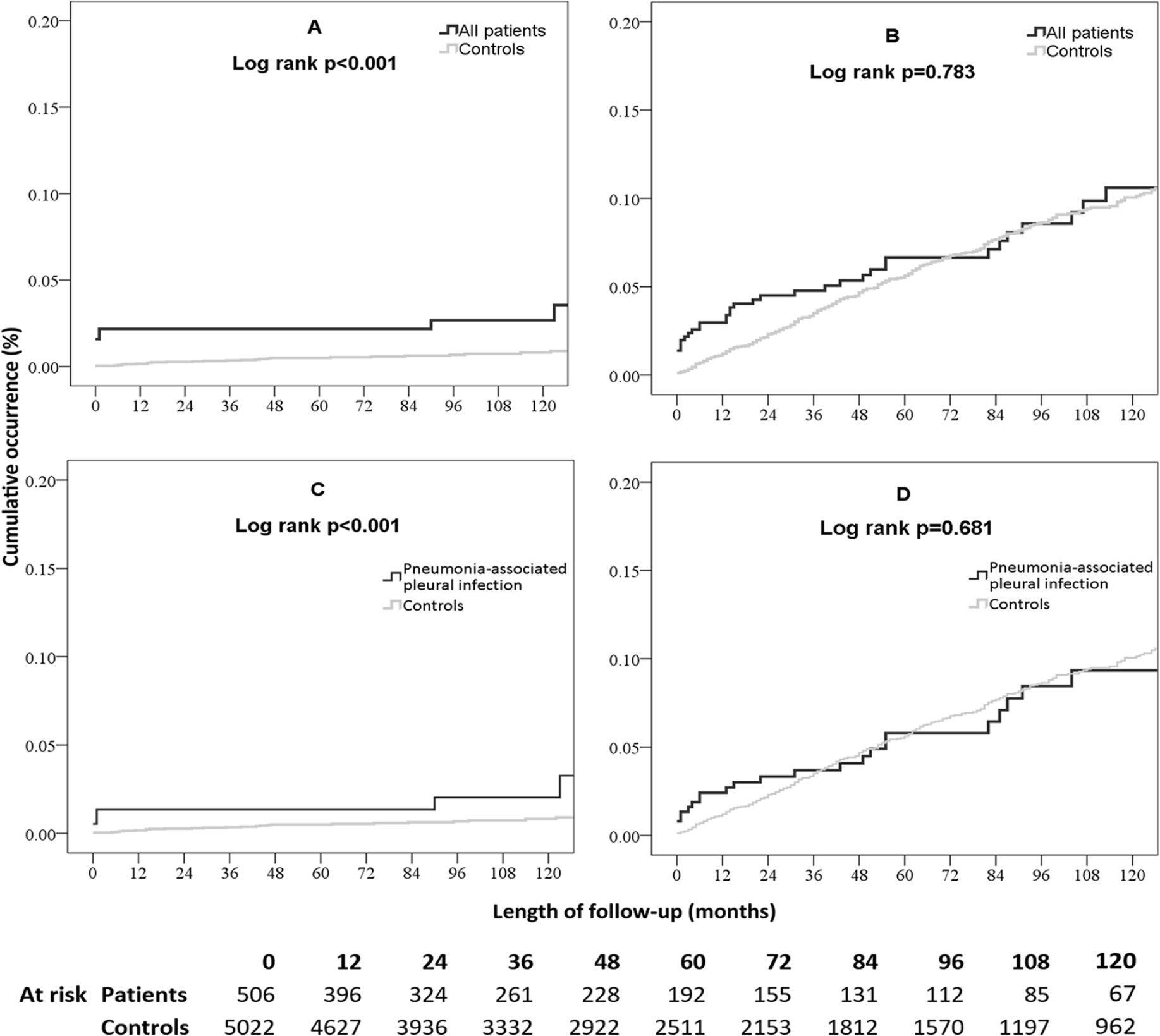
The occurrence of lung cancer and other malignancies in patients with pleural infections compared with controls (A and B, respectively), and in patients with pneumonia-associated pleural infections compared with controls (C and D, respectively).
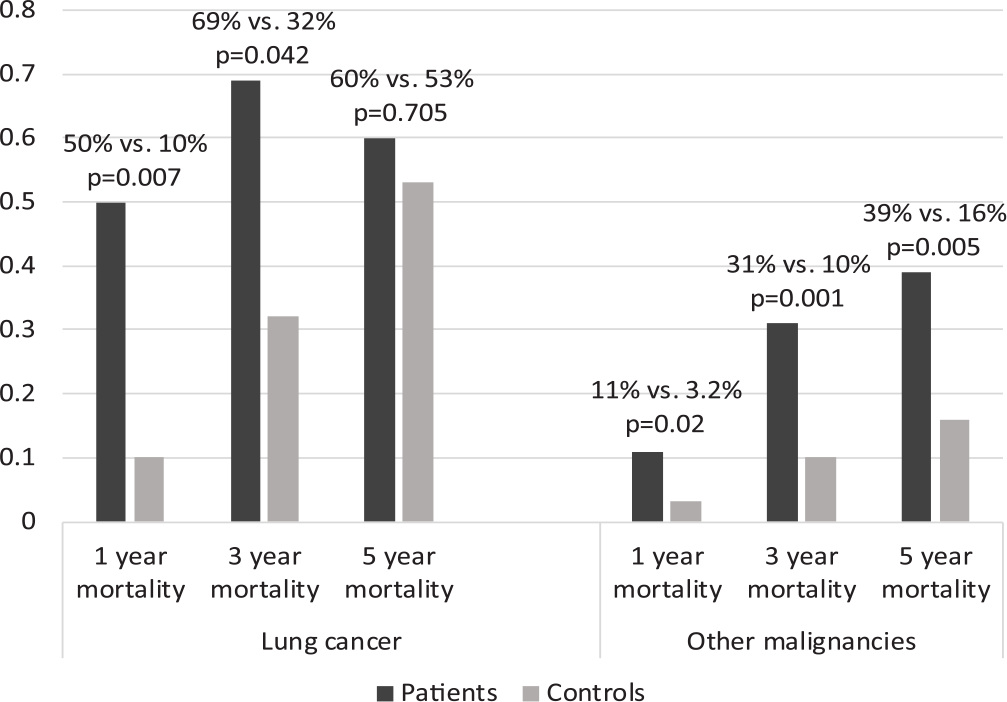
The long-term all-cause mortality rates of patients and controls with lung cancer (left) and other malignancies (right) during follow-up. Cases with insufficient follow-up time at each time point were excluded respectively.
Other Malignancies
There were no statistically significant differences between the overall frequencies of non-pulmonary cancer diagnoses between patients and controls during the follow-up (Fig. 1 and Table 2). However, when analyzing malignancy subgroups, male genital cancers—of which all but one case were prostate cancer—appeared more common in controls than in patients. The types of malignancies detected are shown in Fig. 3. The cancers were reported earlier in patients treated for pleural infections; altogether 30% of the diagnoses were obtained within 90 days of the treatment episode in the patient group, when the corresponding rate in controls was 3.4%, p < 0.001. In study subjects with non-pulmonary malignancies, the long-term mortality rates were higher in patients than in controls (Fig. 2). There were no statistically significant differences in the cancer stages between patients and controls.
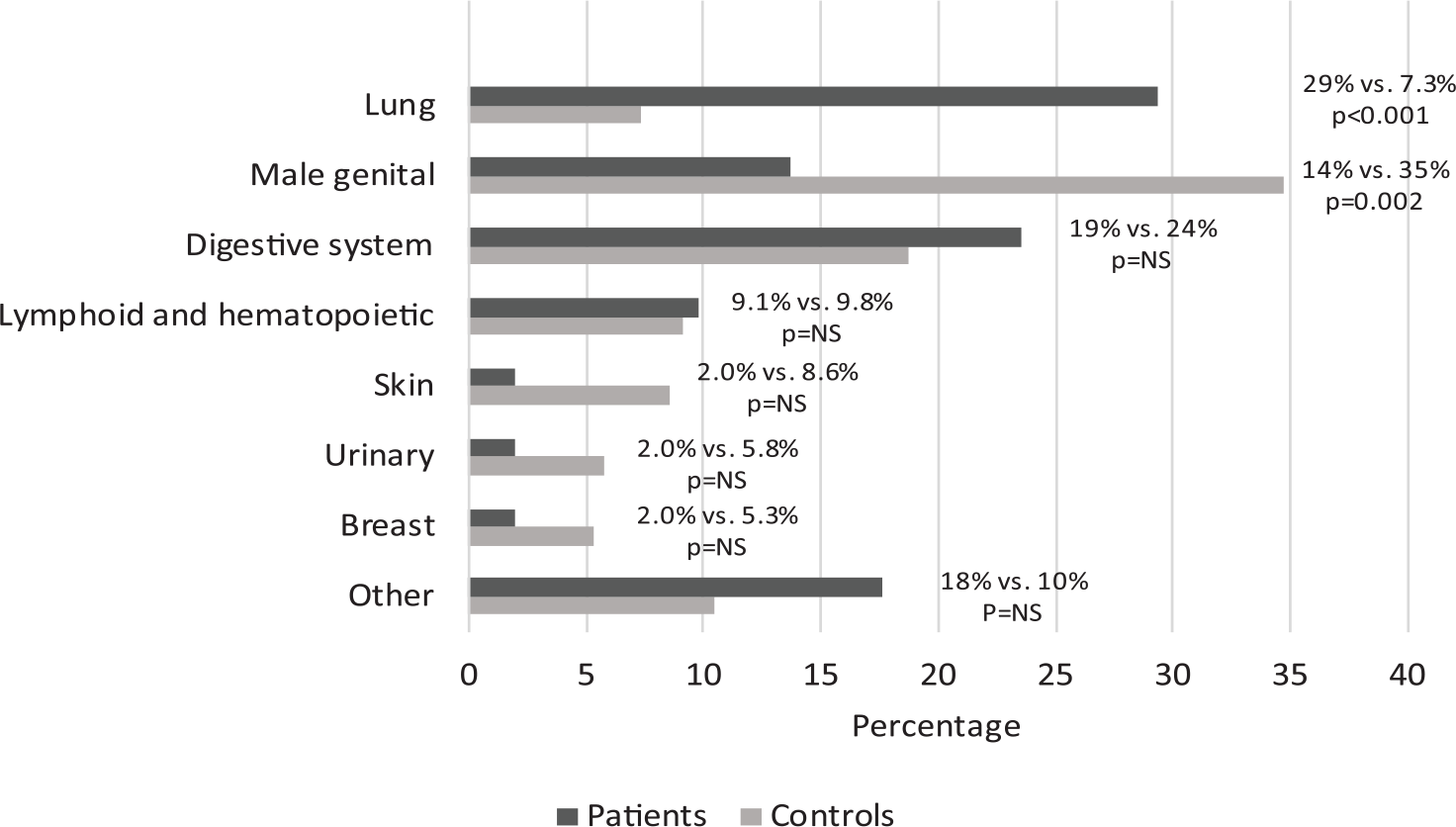
The distribution of the most frequent origins of cancers in patients and controls during follow-up.
Discussion
The occurrence of malignant diseases, particularly lung cancer, significantly impacts both the prognosis and the quality of life of inflicted patients (7). Identifying those at high risk may enable earlier detection and treatment of cancer and result in improved outcomes. Patients that develop pleural infections have been reported of having inferior long-term survival partly due to increased risk of cancer-related deaths. In this study, the authors sought to determine whether the occurrence of lung cancer as well as other malignancies is increased in patients treated for pleural infections and report a statistically significantly higher incidence of pulmonary malignancies as well as inferior early survival in these patients when compared with matched controls, even when considering only cases whose pleural infections were thought to be caused by pneumonias initially. The results of this study agree with the only previous study with similar aims, in which the authors describe a higher incidence of several malignancies, including lung cancer, during follow-up in a registry-based analysis comprising a Taiwanese population (8).
There are several possible explanations for the greater incidence. First, patients that develop pleural infections probably represent a somewhat frailer and perhaps more immunocompromised population with relevant risk factors and consequential comorbidities, though the statistical power of this study did not allow reliable subgroup analyses. Particularly, the prevalence of active smoking was high—almost 40%—in patients. While the exact rate of smoking in the control group was unknown, the proportion of smokers in the general population during the study period was significantly smaller and decreased from less than 30% to about 16% in males aged 20–64 years between 2000 and 2016 and was significantly lower in older men and females (9). Chronic pulmonary diseases were also frequent and may be associated with increased risk for lung cancer (10). It is interesting that in several patients with pleural infections—that were thought to be pneumonia-associated—lung cancer was soon diagnosed, yet not during the initial treatment for the pleural disease. It has been previously reported that a pleural disease at the time of imaging may impede the detection of concomitant pulmonary malignancies (11). Furthermore, despite the recognized association, the exact proportion of patients with pleural infections related to primary lung cancers is inconclusively described in this literature but possibly represents only about 0.1%–3.3% of all patients (12, 13). Whether there was a causal relationship with lung cancer and the onset of pleural infection in these cases remains uncertain but seems likely as the majority of lung malignancies were detected on the ipsilateral lung and shortly following the pleural disease. Pulmonary malignancies may cause immunodeficiency increasing the overall risk for infections and also directly induce pleural infections through several mechanisms including pneumonia caused by bronchial obstruction, infection of necrotic tumor tissue, and cancer invasion to the pleural space. It is also plausible that the conditions were independent and the diagnostic work-up and the follow-up of patients with pleural infections eventually led to the recognition of the co-existing neoplasm. The finding that pulmonary malignancies may, in relevant numbers, be heralded by or at least concomitant with pleural infections emphasizes the need for follow-up and re-imaging in these patients which has not been extensively discussed in the literature previously. Based on the results of this study, the authors propose that thoracic re-imaging, preferably by computed tomography, should be considered in all or most patients after disease resolution—for example, after 3 months—to exclude or identify tumors that might have been missed in the initial imaging studies. As both false negative and false positive results may be caused by disease- and treatment-related residual findings with significant implications, the optimal time for control imaging merits further discussion. The reason for inferior survival in patients with lung cancers compared with that of controls with similar neoplasms reported in this study is not known. There was no apparent association with a more advanced disease stage at the time of diagnosis between patients and controls. It could be postulated that, as the diagnosis was, in many patients, obtained soon after the onset of pleural infection, the disease or its treatment could have restricted or otherwise negatively affected the treatment of the respective malignancy, particularly the use of chemotherapy and the feasibility of radical resections (13, 14). Another possibility is that the other comorbidities, frailty, and immunodeficiencies of these patients negatively impact their prognosis (15).
While the overall incidence of non-pulmonary malignancies did not significantly differ between patients and controls, the number of male urologic cancers, that is, those of the prostate, was significantly higher in controls. Prostate cancer is common in men of advanced age with a reported age-adjusted incidence of approximately 50 per 100,000 patient years and the authors suspect that the difference is at least partially explained by better survival rates and hence higher number of subjects at risk for the respective malignancy in the control group (7). The non-pulmonary malignancies also occurred or at least were detected earlier in patients than in controls and were associated with a somewhat inferior life expectancy. This was possibly due to the comprehensive diagnostic evaluation and the follow-up associated with the pleural disease as well as the comorbidities and the cancer-associated risk factors of these patients. Overall, when comparing the cancer rates between patients and controls and when interpreting the results of this study, the differences in the early and long-term survival and subsequently in the time at risk per patient must be regarded. In the literature, the disease-related mortality rates in patients with pleural infections range from 6% to 27% and the long-term prognosis of these patients appears to be affected as well, probably due to the high rate of relevant comorbidities such as smoking and alcoholism, similar to our results (3, 5, 6, 16–18).
The most important restrictions of the study include its single center setting, the relatively small number of patients with malignancies limiting subgroup analyses, and the realities associated with registry-acquired data. While virtually all cases of pleural infections in which thoracic surgery was contemplated within the University hospital district were referred to our institution, some cases, particularly those in which operative treatment was not considered, might have been treated elsewhere, causing some selection bias, as suggested also by the high percentage of surgical treatment in the series. The proportion of actively smoking patients was high in the study, which was probably a significant reason for our findings, but our material might not be representative to those of others. Exactly how the diagnosis was acquired and was there a difference between the treatment given for the malignancies between patients and controls is not known. The strengths of the study comprise a relatively large cohort of consecutive patients with documented comorbidities and disease-related specifics that were treated over a time period of nearly two decades and the comprehensive national registries available in our country. Furthermore, the study included all patients, when some authors describe only surgically or conservatively treated patients, or pleural infections caused by a single etiology.
In conclusion, we report a significantly higher rate of lung cancer in patients that were treated for pleural infections during follow-up when compared with that of matched controls. Most cases were identified within a few months after the treatment period. The overall incidence of other malignancies did not significantly differ. The survival of patients with lung cancer as well as those with non-pulmonary malignancies was inferior to that of controls with similar diagnoses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants from the Tampere Tuberculosis Foundation, the Emil Aaltonen Foundation, and the Finnish Anti-Tuberculosis Association.