
Abstract
Background and Aims:
The aim of the study was to ascertain changes in the incidence, etiology, treatment, and outcomes of pleural infections over a decade in a Finnish University Hospital.
Materials and Methods:
All patients treated for pleural infections in Tampere University Hospital during 2000–2008 and 2012–2016 were included. The incidence rates and the epidemiologic data and medical history of patients, etiology of infection, and treatment trends and outcomes were compared between the cohorts.
Results:
The incidence of pleural infections increased from 4.4 during 2000–2008 to 9.9 during 2012–2016 per 100.000 patient-years, p < 0.001. The patients in the latter group were older, 63 versus 57 years, p = 0.001, and the prevalence of chronic lung disease, hypertension, heart failure, dyslipidemia, and immunosuppressive medication were higher. The causes of infection remained similar and pneumonia accounted for 70% of all cases. The identification rate of the microbe pathogens increased from 49% to 64%, p = 0.002, while the distribution of identified pathogens was unchanged. More patients in the latter cohort were treated operatively, 88.3% versus 80.9%, p = 0.005, and, in these, the proportion of thoracoscopic surgery was higher, 57.4% versus 8.0%, p < 0.001, and the delay to surgery shorter, 5 versus 7 days, p < 0.001. Radiologic outcomes were similar. The 30-day mortality rate was 3.1% during 2000–2008 and 5.1% during 2012–2016, p = 0.293.
conclusion:
The overall incidence of pleural infections has increased significantly while the causes of pleural infections and the distribution of pathogens remain unchanged. Contemporary patients are older with higher prevalence of comorbidities and more frequently undergo thoracoscopic surgery.
Introduction
Pleural infections are a significant cause of patient morbidity and health care costs, and associated with inferior long-term survival. Furthermore, the worldwide incidence of pleural infections has been increasing (1–4). Pneumonia is the most common etiology of pleural infections. Other common causes include thoracic malignancies, trauma, and complications of invasive intrathoracic procedures. Advanced age, male sex, alcoholism, and low socioeconomic status, as well as malignancies and other common comorbidities are associated with higher risk for the development of pleural infections (3, 5–7). The most common pathogens are streptococci in community-acquired pleural infections, and staphylococci and enterococci in hospital-acquired cases. Hospital acquired cases are associated with worse prognosis (8, 9).
The goal of treatment for pleural infections is to control the infection and to allow the re-expansion of the affected lung. The treatment options include antimicrobial therapy, pleural drainage, possibly combined with intrapleural fibrinolysis, and surgery. While less invasive methods may suffice, surgical treatment, either traditional open surgery or video-assisted thoracic surgery (VATS), is often required (3). Several studies have shown similar treatment outcomes with open surgery and VATS, though the latter is associated with faster recovery (10–13).
The objective of the present study was to ascertain the trends in the incidence, etiology, patient profiles, bacteriology, treatment, and outcomes of pleural infections in a Finnish University Hospital over a decade.
Materials and Methods
The Study Population and the Incidence of Pleural Infections
The study included all consecutive patients treated for pleural infections in Tampere University Hospital, Tampere, Finland, between January 2000 and December 2008 (group 1) and between January 2012 and December 2016 (group 2). The patients for both study groups were identified from the institutional database by retrieving all cases associated with the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10), code “J86” or any subclass of “J86,” and the diagnosis of pleural infection was confirmed by reviewing the medical records and laboratory results of each case. Patients treated in the pediatric department were excluded. The relevant epidemiologic data and medical history were recorded in each patient. Yearly incidence rates were calculated according to the number of residents at the hospital district obtained from Statistics Finland.
The Diagnosis and Classification of Pleural Infections
The study comprised patients with pleural infections (stage II or III) according to the American Thoracic Surgery classification (14). Clinical signs of infection together with a pleural effusion of significant volume and detection of infection in the pleural fluid analysis or intra-operatively were required for the diagnosis. Positive bacterial culture, stain, or polymerase chain reaction (PCR) test result, pH < 7.2, lactate dehydrogenase level >1000 IU/L, and/or glucose <2.2 mmol/L in the pleural fluid analysis were considered indicative of infection. The pleural infections were further classified as complicated effusions, when loculated effusions with fibrin deposits but no pus was detected, and empyemas, when clear pus was present in the pleural space, in concordance with the Light criteria (14). The identified pathogens were recorded. The results of the most important laboratory examinations were collected. The cause of pleural infection was classified into the following categories: pulmonary infection, trauma, complication of a procedure, malignant disease, other, and unknown.
Trends in the Treatment of Pleural Infections and Treatment Outcomes
The type of treatment given, the intervals between important points of patient care such as the delay between hospitalization and the initiation of chest tube drainage or surgery, and treatment outcomes were compared between the study groups. The course of treatment in both groups was decided by the attending physician and was classified as either conservative, drainage only, or operative. Surgical treatment was classified as VATS or traditional open surgery. The conversion rates for VATS procedures were recorded. The procedure performed, either by VATS or traditional surgery, was classified as canalization, canalization together with decortication, or extended procedure, when, for example, pulmonary resection, pleurectomy of the parietal pleura, thoracoplasty, and/or fenestration was performed. The length of hospitalization at our institution—that is, until discharge home or referral for follow-up treatment in another institution—the number of reoperations, radiologic outcomes, and short-term mortality rates were compared. Radiologic outcomes were analyzed by a single radiologist. The presence of intrathoracic abscesses and/or multi-loculated effusions, and the maximal thickness of the pleural effusion during admission were recorded. The surface area of the ventilating lung in the postero-anterior chest radiograph, lined by the chest wall, diaphragm, mediastinum, and pleural effusions and/or thickening, on the affected side was measured preoperatively and 1 to 6 months postoperatively. Also, the development of diaphragmatic elevation, diagnosed when the right hemidiaphragm was at least 3 cm higher than the left or the left hemidiaphragm was higher than the right, and the loss of the costodiaphragmatic recess were recorded. The 30-day mortality rates following the day of hospital admission were obtained from the National Population Register Center.
This study followed the ethical principles of the Helsinki Declaration and was approved by the institutional review board. Statistical analysis was performed with IBM SPSS for Windows statistical software, version 24.0, using the chi-square test and Fisher’s exact test to compare categorical data and the Mann–Whitney U test to compare scale variables. The mean incidence rates between the study groups were compared using the chi-square test. Values of p < 0.05 were considered statistically significant.
Results
Patient Profiles, Disease Presentation, and the Incidence of Pleural Infections
The incidence rate of pleural infections significantly increased throughout the study period (Fig. 1). The overall incidence was 4.4/100.000 patient-years between 2000 and 2008 and 9.9/100.000 patient-years between 2012 and 2016, p < 0.001. The demographic information and the medical history of study patients as well as the etiology and presentation of pleural infection in both groups are shown in Table 1. The patients in group 2 were slightly older and the prevalence of chronic lung disease, hypertension, heart failure, dyslipidemia, and immunosuppressive medication were somewhat higher in these patients. There were no significant differences in the proportions of the most important causes of pleural infections between the study groups. Pulmonary infection was the most common etiology accounting for approximately 70% of all cases. Of more rare causes, intra-abdominal infections and esophageal perforations were significantly more frequent in group 2. A significant proportion of patients with pleural infections following a procedure, 49%, also had a malignant disease. There were no differences in the radiologic presentation of the disease between the groups (Table 1). The disease was classified as a complicated effusion in 33% and as an empyema in 67% of patients in group 1, while the corresponding rates in group 2 were 61% and 39%, p < 0.001, respectively. The detection and identification rate for the microbe pathogens increased from 49% in group 1 to 64% in group 2, p = 0.002. There were no statistically significant differences in the distribution of identified bacteria between the study groups, and the most important pathogens are shown in Fig. 2. In patients whose pleural infection was a complication of a procedure, the most common identified pathogens were Staphylococcus aureus in 21%, other Staphylococci in 21%, Streptococci in 10%, while 31% had a polymicrobial infection. In the latter group, bacterial PCR test was obtained from 43 (16%) patients and in 8 (3%) cases yielded information not obtained by other means.
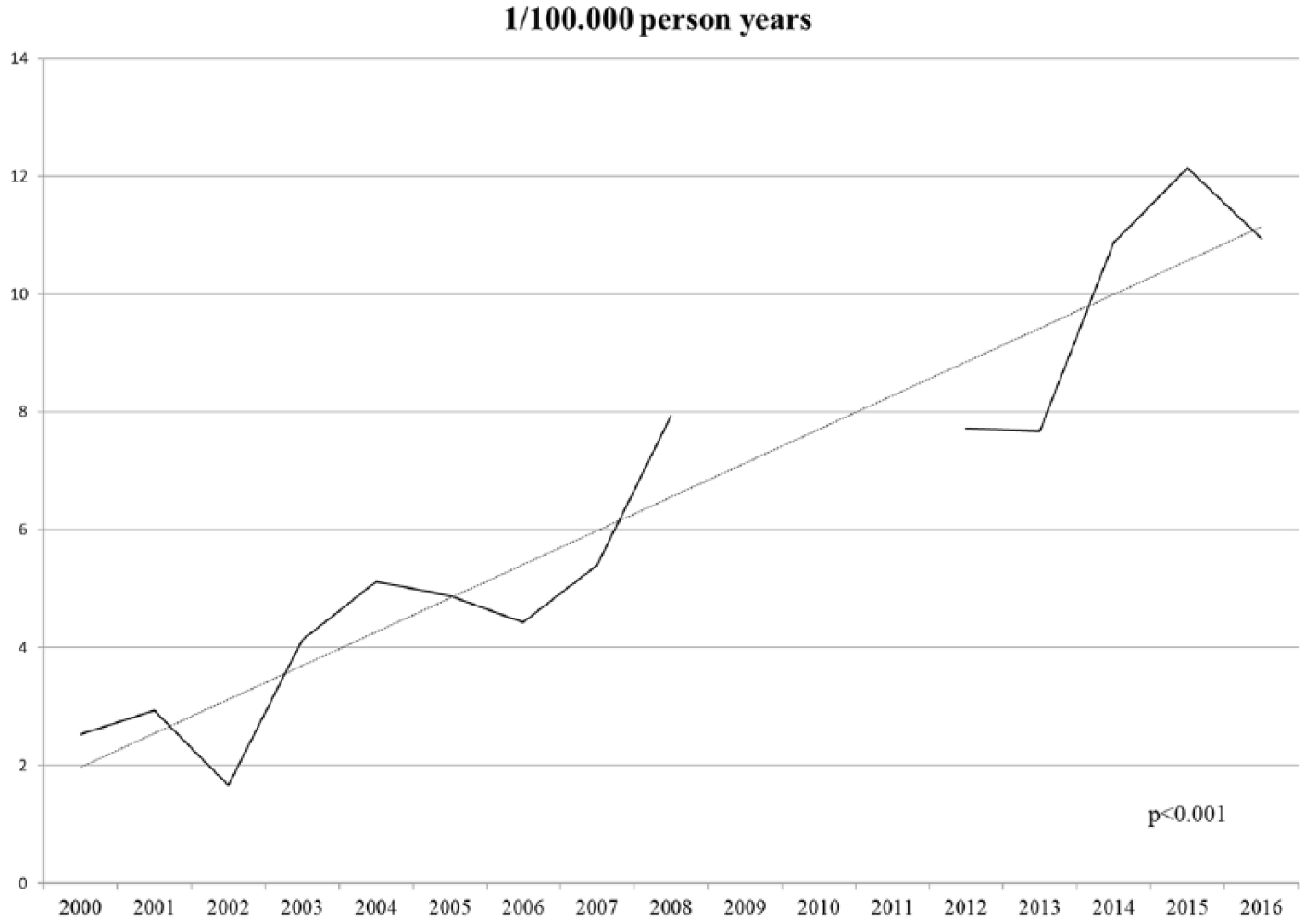
The annual incidence of pleural infections. The number of residents in the hospital district area increased from 474.599 to 529.898 during the study period.
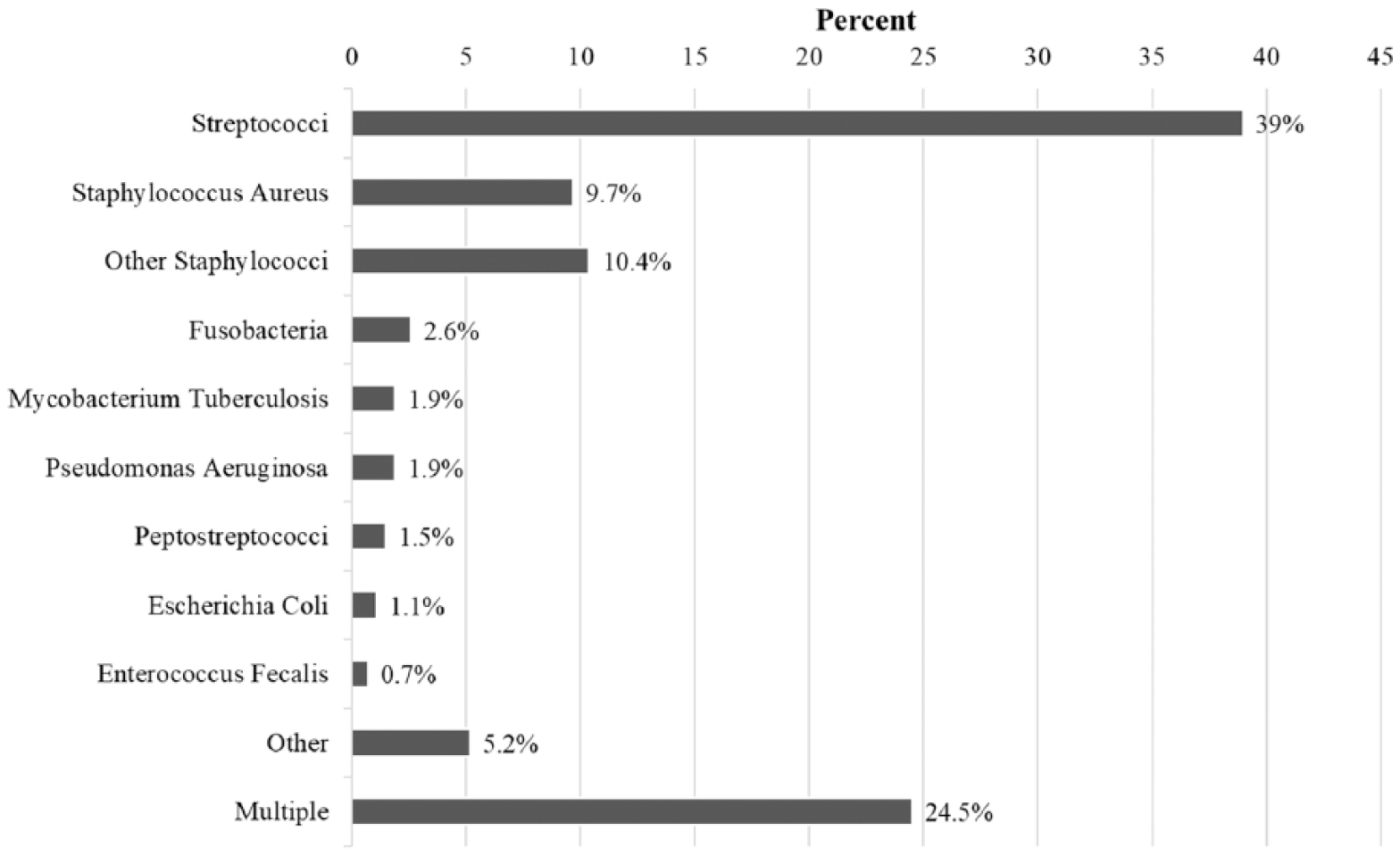
The distribution of identified microbe pathogens in patients with pleural infections.
The demographic information and medical history of study patients as well as the etiology and radiologic presentation of pleural infections.
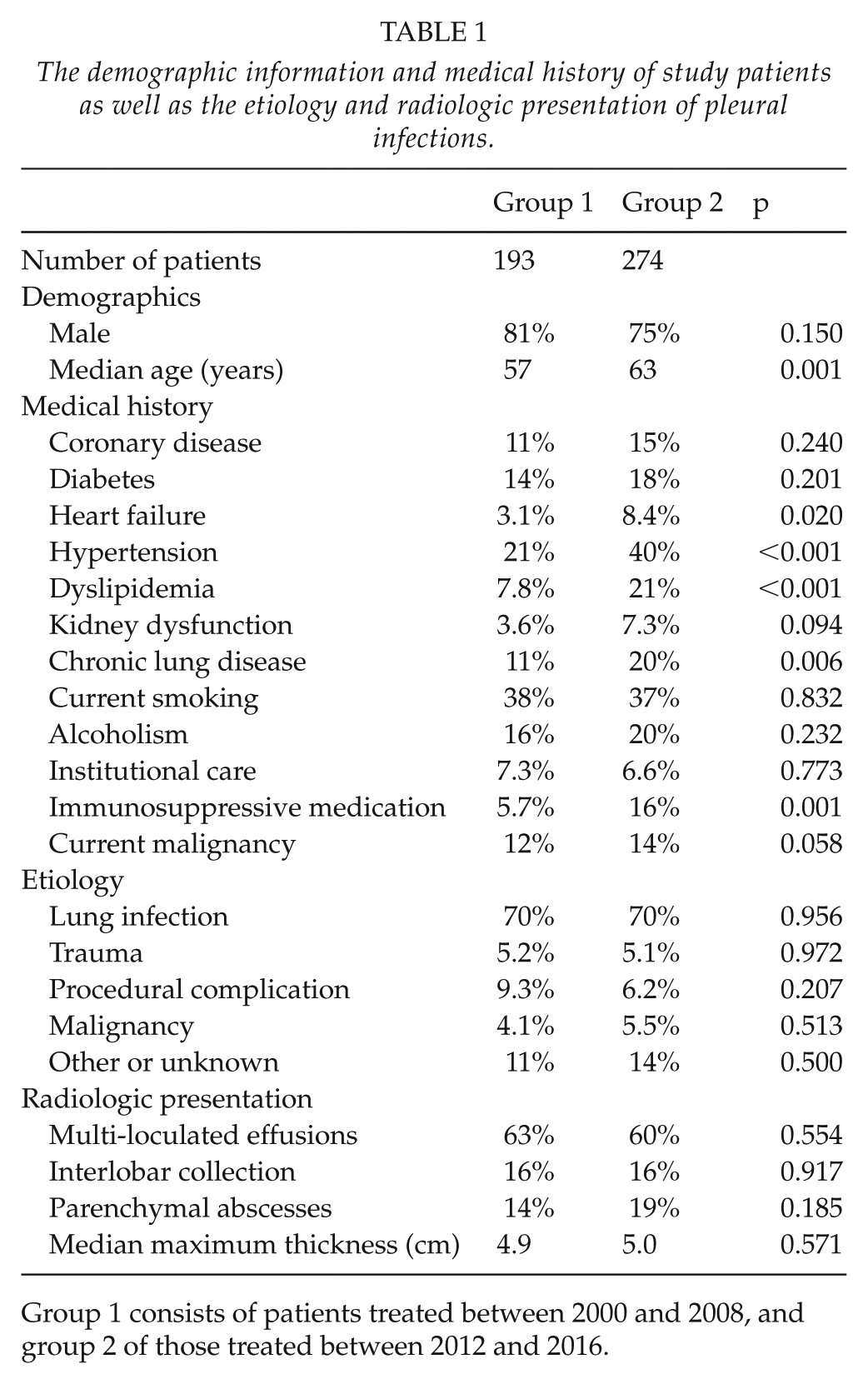
Group 1 consists of patients treated between 2000 and 2008, and group 2 of those treated between 2012 and 2016.
Treatment and Outcomes
Trends in the treatment of pleural infections are described in Table 2. Most patients underwent surgery, but the proportion was significantly higher in group 2, as was the rate of VATS and the less extensive canalization procedures. In patients who were operated, drainage was attempted prior to surgery in 55% of patients in group 1 and 49% in group 2, p = 0.239, with a median interval of 4 days between chest tube insertion and surgery in both groups. The decortication rate was similar in both groups. The need for reoperations and intensive care unit (ICU) treatment were significantly higher in the later cohort. There was no delay in the initiation of antibiotic therapy in either group, but both pleural drainage and surgery were undertaken significantly earlier for patients in group 2. The median length of hospitalization was 14 days with no statistically significant differences between the groups. There were no significant differences in the C-reactive protein, blood leukocyte, hemoglobin, or creatinine concentrations during hospitalization between the groups. The 30-day mortality rates in groups 1 and 2 were 3.1% versus 5.1%, p = 0.293, in all patients; 3.0% versus 4.2%, p = 0.563, in patients with pulmonary infection as the cause of pleural infections; and 2.0% versus 4.5%, p = 0.179, in surgically treated patients, respectively. Altogether 60% of deaths occurred in patients with pulmonary infection as the etiology of pleural infection and 70% in patients who had undergone surgery, and, of these, 57% had required extended procedures. The prevalence of significant comorbidities was high in the non-survivors; 30% had a malignancy, 30% were alcoholics, 30% had a chronic lung disease, and 10% were in institutional care. The median increase of ventilating lung surface area after 1- to 6-month follow-up was 59 cm2 and did not differ between the groups. Diaphragmatic elevation during follow-up was significantly more common in group 1 than in group 2, 60% versus 34%, p = 0.003, respectively, while the rates for the loss of the costodiaphragmatic recess were similar, 85% versus 79%, p = 0.165, respectively.
The treatment of pleural infections.
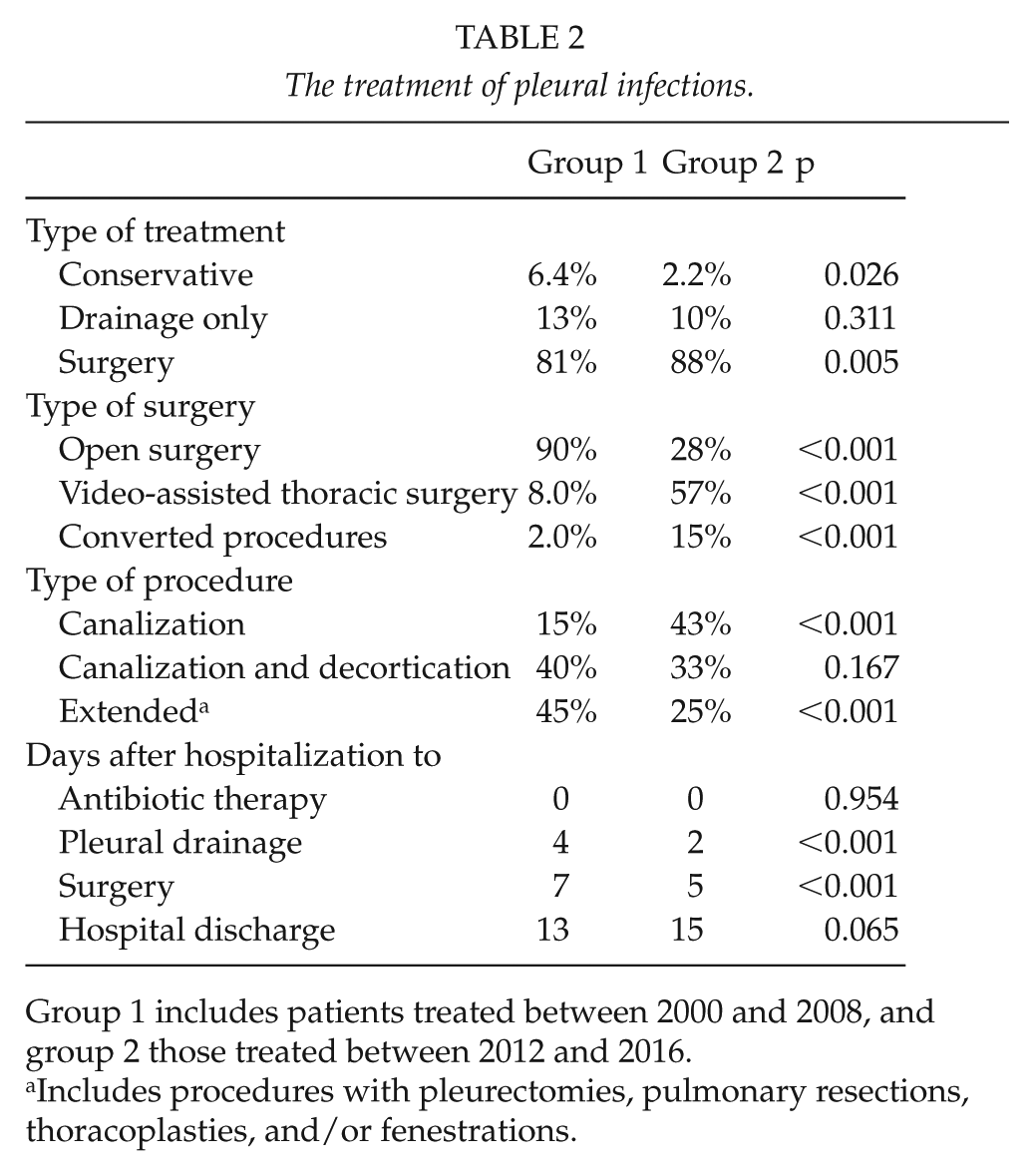
Group 1 includes patients treated between 2000 and 2008, and group 2 those treated between 2012 and 2016.
Includes procedures with pleurectomies, pulmonary resections, thoracoplasties, and/or fenestrations.
Discussion
The aim of the current study was to describe possible changes in the incidence, etiology, patient characteristics, and microbial causes, as well as treatment trends and outcomes, of pleural infections in a Finnish University hospital district. A significant increase in the incidence of the disease throughout the study period was reported, while the etiology and microbial causes of the infections have remained relatively unchanged. Contemporary patients are older, and the prevalence of significant comorbidities is higher. Despite this, operative treatment, increasingly mini-invasive, is offered for a larger proportion of patients and the short-term outcomes have remained similar.
The reasons for the growing incidence of pleural infections are somewhat unclear, but similar findings have been reported by other authors as well (1–3, 15). An actual increase of the disease may be due to changes in the age distribution of the population, as older age groups are becoming more prominent in many developed countries and advanced age is associated with several other diseases—as well as invasive diagnostic workup and treatment—that may predispose to the development of pleural infections in addition to being an independent risk factor for infections of the pleura. For example, hospitalizations due to pneumonia—the most common cause of pleural infections—are more frequent (16, 17). In the present study, patients in the latter cohort were significantly older, which could suggest that the age structure and the corresponding disease burden of a population play an important role. In addition, as diagnostic and mini-invasive therapeutic measures are more readily available, the awareness and identification rate of pleural infections may have increased, and concurrently the threshold to refer increasingly morbid patients may have decreased. Also, the diagnosis was possibly obtained sooner in the later cohort as the disease stage was earlier in many patients. Contemporary patients are older which probably explains the higher prevalence of comorbidities. The causes of pleural infection throughout the study were similar to those in the literature (6, 18).
There was a significant increase in the proportion of identified microbial pathogens over the study period, possibly influenced by the evolution of culture techniques and the inclusion of PCR methods, as well as by the fact that as invasive treatment was undertaken more frequently and earlier, more representing samples with shorter duration of prior antibiotic therapy were obtained. The number of cases with identified microbial pathogens was comparable to other studies though identification rates up to 75% have been reported when PCR tests have been routinely used. The pathogens detected were similar than elsewhere reported although polymicrobial infections were more common in the present series (8, 9, 19, 20).
The proportions of pleural infections treated operatively and less invasively have been increasing worldwide, and a similar finding was observed in the current study [3]. There was a trend toward less extensive procedures in the latter group, possibly due to earlier surgery and stage of the disease. Virtually no patients were treated by intrapleural fibrinolytics in our series. Their role in the treatment of pleural infections is still controversial in the literature (21, 22). The short-term outcomes—including mortality, disease resolution, and the length of hospitalization—were comparable over the study period. There was a non-significant trend toward longer hospitalizations in the latter group which was mostly caused by the termination of district hospital specialized in pulmonology in 2007, where, until that, a significant number of patients were referred for follow-up treatment. Diaphragmatic elevation after treatment was common, especially in the earlier group in which open and extended procedures were more common. Its significance, and the impact of pleural infections on pulmonary function in general, warrants further research. Some important factors possibly favoring VATS, such as postoperative pain and mobilization (23), were not, however, compared, and overall the present study was not designed to compare surgical methods. Even in the current era with mini-invasive therapeutic options, conservative treatment of some patient groups, for example, those with malignant etiology for the pleural infection or those in institutional care, remains reasonable considering the dismal prognosis of these patients (4).
The main limitations of the present study include its single-center setting and the non-randomized retrospective design. The proportion of patients undergoing surgery was higher than in many other studies which may reflect local treatment protocols and differ from other institutions. In most cases that underwent surgery, however, conservative treatment with antibiotics and pleural drainage was attempted before referral to surgery. It is possible that earlier or longer drainage or more active use of fibrinolytics could have resulted in a higher number of non-operatively treated patients and that earlier thoracoscopic surgery could have reduced the need for open surgery. A part of the increase in the prevalence of comorbidities in the later period may be due to more accurate reporting. The classification of disease stage was in many cases based on the surgeons’ descriptions of intra-operative findings, which were non-structural and a potential source of bias. There was insufficient statistical power for some subgroup analyses, such as the comparison of very complicated cases and, for example, the use of different surgical and vacuum-assisted (24) methods for late closure or management of empty space. While the clear majority of patients with pleural infections at our region were admitted to our institution, some cases were treated at other hospitals and the number and the clinical course of these patients are unknown, possibly causing some bias in the results. Patients not referred may, for example, represent extremely morbid and inoperable cases. The authors, however, believe that the proportion of these patients has remained similar throughout the study period and should not significantly impact the results. However, we report a relatively large material of consecutive patients and also included patients who were treated non-operatively when many authors report only surgical cases.
In conclusion, we report a clear increase in the incidence of pleural infections over two decades. The etiology and bacterial causes of the infections have remained similar. Contemporary patients are older, have more comorbidities, and undergo less invasive surgery. Treatment outcomes have remained similar.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants from the Tampere Tuberculosis Foundation, the Foundation of the Finnish Anti-Tuberculosis Association, and the Emil Aaltonen Foundation.