
Abstract
Background and Aims:
Spondylolysis is a common cause of lower back pain during youth. The aim of this study is to report the bony union rate and risk factors for non-union of the lumbar spondylolysis of pediatric patients treated with a rigid thoracolumbosacral orthosis (Boston brace).
Materials and Methods:
A retrospective review of 68 children (mean age = 13.9 years) treated for spondylolysis with a thoracolumbosacral orthosis. Patient charts and imaging studies were evaluated to identify the bony union rate of the spondylolysis after a minimum of 3 months of immobilization (mean = 4.2 months). Laterality, grade, level, and presence of high signal intensity in the magnetic resonance imaging were evaluated as prognostic factors.
Results:
Sixty-eight patients presented with 110 defects. Of them, 46 (42%) were incomplete fractures, 38 (35%) complete fractures, and 26 (24%) pseudoarthrosis. Of these defects, 38 (82.6%), 11 (28.9%), and 0 (0.0%) had bony union at the end of the treatment (p < 0.001). Unilateral defects healed significantly better than bilateral ones (relative risk = 1.71, 95% confidence interval = 1.16–2.54, 17/26 (65%) vs 32/84 (38%), p = 0.014). High signal intensity in the magnetic resonance images before the treatment predicted healing (relative risk = 13.24, 95% confidence interval = 1.93–91.01, 48/87 (55%) vs 1/24 (4.3%), p < 0.001). The level of the spondylolysis (L5 vs above L5) did not affect the healing rate.
Conclusion:
The union rates of spondylolysis with a thoracolumbosacral orthosis were similar as compared to earlier studies done with a low thoracolumbosacral orthosis. The grade of the defect, laterality, and presence of high signal intensity increased the probability of bony union. A high thoracolumbosacral orthosis (underarm) does not seem to improve the healing rate of pediatric spondylolysis defects.
Introduction
Lumbar spondylolysis is a common spinal disorder affecting 4.4% of children and 6% of adults (1, 2). Its etiology is typically related to a combination of congenital weakness in the pars interarticularis and mechanical stress resulting into a stress fracture (isthmic spondylolysis) (3, 4–6). Using conservative treatment, early-phase lesions may heal without development of spondylolisthesis during further growth (1, 7–9). Various methods of immobilization such as a soft corset or a low rigid overlapping orthosis have been used resulting into healing rate of 62%–94% of the early lesions, 8.7%–80% of the progressive lesions, and none of the terminal lesions (pseudoarthrosis) (7, 8–10). However, it remains unclear if the healing rates of different stages of lesions could be improved using a high rigid thoracolumbosacral orthosis which is more effective in preventing lumbar extension and flexion (11).
We aimed to report the radiographic outcomes of conservative treatment using an individualized, custom-made Boston underarm thoracolumbosacral orthosis (TLSO) for a minimum of 3 months in pediatric spondylolysis. We hypothesized that a high TLSO management would heal the majority of early-phase isthmic lesions while more advanced lesions would heal less often.
Materials and Methods
Patients
A retrospective review of our academic medical center database identified 76 consecutive patients with unilateral or bilateral spondylolysis who were treated with a TLSO (Boston underarm brace) between 2010 and 2018. Inclusion criteria included age under 18 years at the time of the diagnosis, uni- or bilateral spondylolysis treated with a rigid TLSO targeting to bony healing. Exclusion criteria included high energy trauma, systemic illness potentially affecting bony healing or bone density (osteogenesis imperfecta, skeletal dysplasia, primary or secondary osteoporosis or endocrine disorder, that is, hypothyreosis). Of the 76 patients, 8 were excluded from the analyses: 4 patients did not have a fracture line (only a stress reaction in the pars interarticularis); 1 patient had a stress fracture in the sacrum; 1 patient did not have magnetic resonance (MR) images before the treatment; and 2 patients did not have computed tomography (CT) or MR images after the treatment to evaluate bony healing. Thus, 68 patients were included in this study. These patients’ medical history was re-examined, and the imaging studies of these patients were re-evaluated by an independent musculoskeletal radiologist. The aims of this retrospective study were to investigate the bony union rate of the spondylolysis with a rigid TLSO and to find out factors affecting the bony healing.
The 68 patients (mean age = 13.9 years, range = 6.3–17.8 years, 36 (53%) males) with spondylolysis were immobilized with a rigid TLSO (Boston underarm brace) for a minimum of 3 months (mean = 4.2 months, range = 1.4–5.6 months). All (100%) of the patients were active in sports. The most common sport was soccer (26 patients), followed by ice hockey (12 patients), gymnastics (8 patients), and figure skaters (2 patients). All of the spondylolysis were confirmed with magnetic resonance imaging (MRI) in the beginning of the treatment, an additional CT before immobilization was taken from 27 (39.7%) patients, and the plain radiographs were taken from 31 (41.6%) patients. The spondylolysis was noted in these radiographs in 13 (41.9%) patients. Of these 68 spondylolysis, 26 (38.2%) were unilateral and 42 (61.8%) were bilateral. Therefore, a total of 110 defects were seen in these 68 patients. Twenty (18%) of the defects were above L5 (2 in L1, 4 in L3, and 14 in L4 vertebra) and 90 (82%) in the L5 vertebra. The majority of the lesions above L5 were bilateral: only two (10%) of them were unilateral. The fractures were classified into three grades (incomplete fracture/complete fracture/chronic defect = pseudoarthrosis) by an independent musculoskeletal radiologist according to Hollenberg et al.’s (12) MRI grading system. Stress reactions were only reported when they occurred along with a defect elsewhere.
The treatment consisted of restriction on all exercise except walking and a rigid TLSO (Boston underarm brace). Patients were advised to wear the orthosis 23 h a day. The mean immobilization time was 4.2 months ranging from 1.4 to 5.6 months. At the end of the treatment, either MR images (33 patients) or CT images (24 patients) or both (11 patients) were used to evaluate bony healing of the pars defect. In patients with both examinations, the bony healing was evaluated using the CT images.
Statistical Analyses and Ethical Committee Approval
Statistical comparisons were performed with chi-square tests for categorical parameters and unpaired t-tests for continuous variables. p-values of 0.05 or less were considered significant. Relative risks (RRs) and their 95% confidence intervals (CIs) were calculated with the bilateral spondylolysis and no high signal intensity used as the reference.
Ethical committee approval was granted by Turku University Hospital. Due to retrospective nature of the research, no informed consent was requested by the ethical committee.
Results
The main characteristics of the defects and their bony union rates are shown in Tables 1 and 2. There were 46 (41.8%) incomplete fractures, 38 (34.5%) complete fractures, and 26 (23.6%) pseudoarthrosis in 68 patients. Sixty-seven (98.5%) of the patients followed up the recommended treatment protocol. Of these defects, 38 (82.6%), 11 (28.9%), and 0 (0.0%) had a bony union at the end of treatment, respectively (p < 0.001). Unilateral defects healed significantly better than the bilateral ones (RR = 1.71, 95% CI = 1.16–2.54, 17/26 (65%) vs 32/84 (38%), p = 0.014). High signal intensity of the pars interarticularis in the MR images before the treatment also predicted healing (RR = 13.24, 95% CI = 1.93–91.01, 48/87 (55%) vs 1/24 (4.3%), p < 0.001). The level of the spondylolysis (L5 vs above L5) did not affect the healing rate. The effects of level of the lesion, uni- versus bilateral, and stage of the lesion are shown in Fig. 1. This figure demonstrates that the level of the lesion does not affect the healing rate when uni- versus bilaterality and the stage of the lesions are evaluated. Fifty-eight (85%) out of the 68 patients were asymptomatic at the end of immobilization.
Clinical characteristics of the study groups based on the laterality.
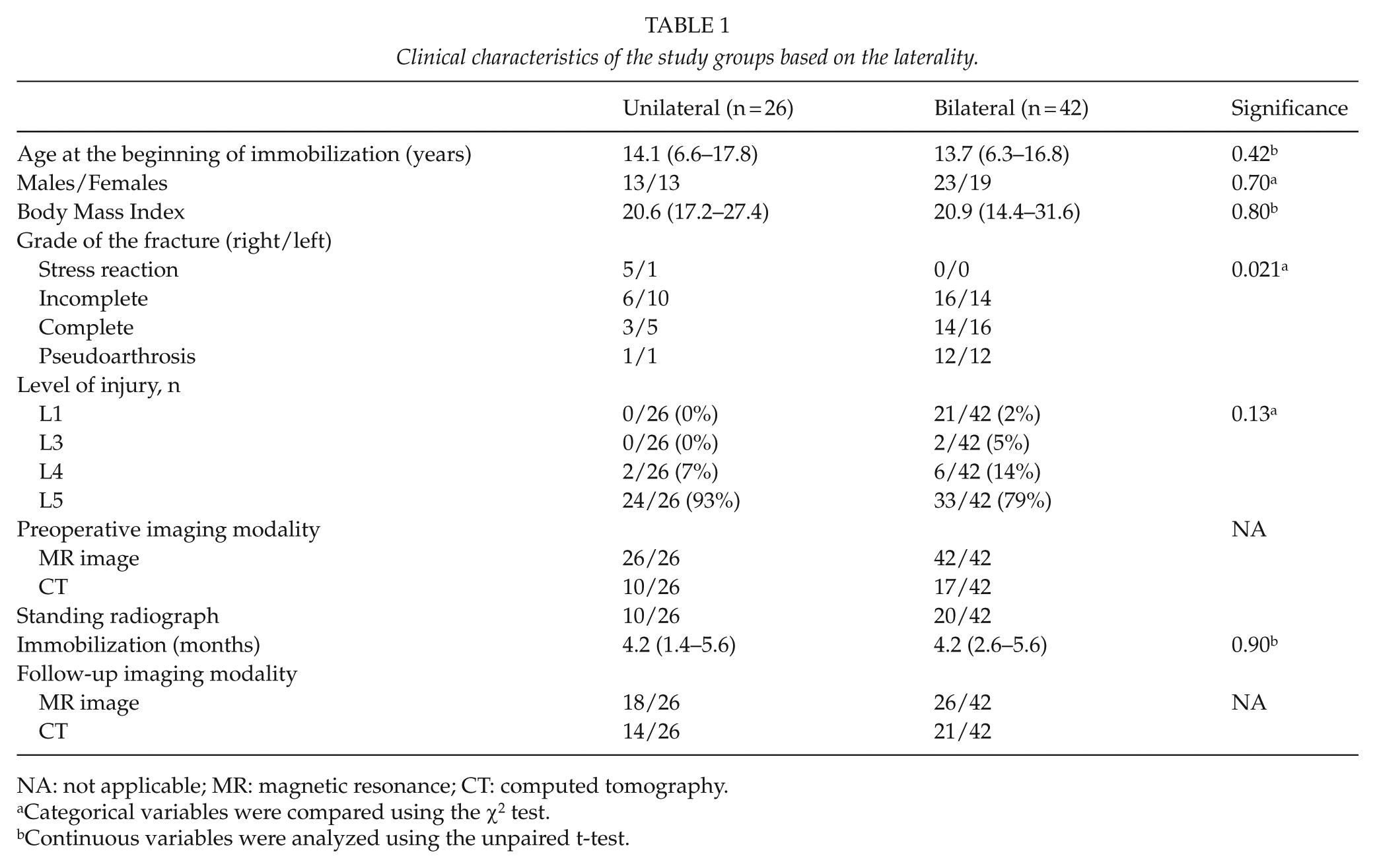
NA: not applicable; MR: magnetic resonance; CT: computed tomography.
Categorical variables were compared using the χ2 test.
Continuous variables were analyzed using the unpaired t-test.
Bony union rates in different groups.
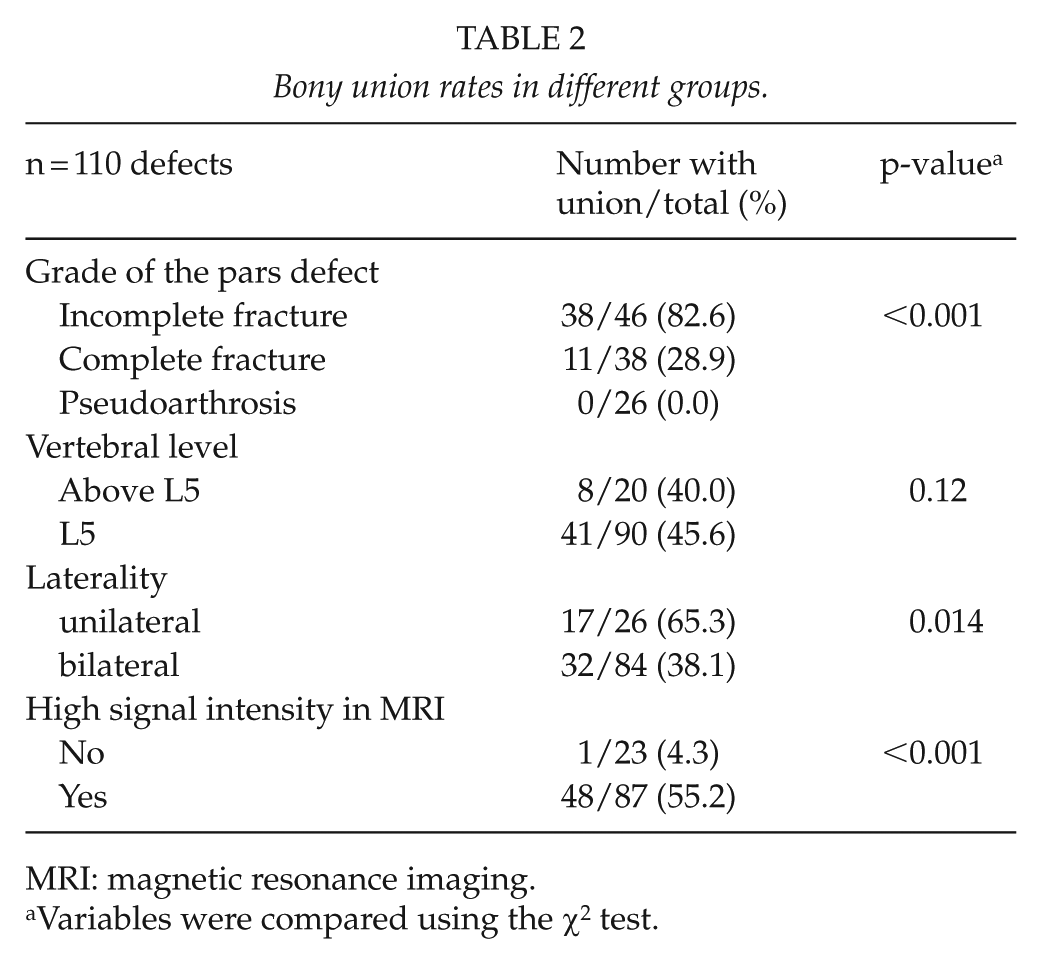
MRI: magnetic resonance imaging.
Variables were compared using the χ2 test.
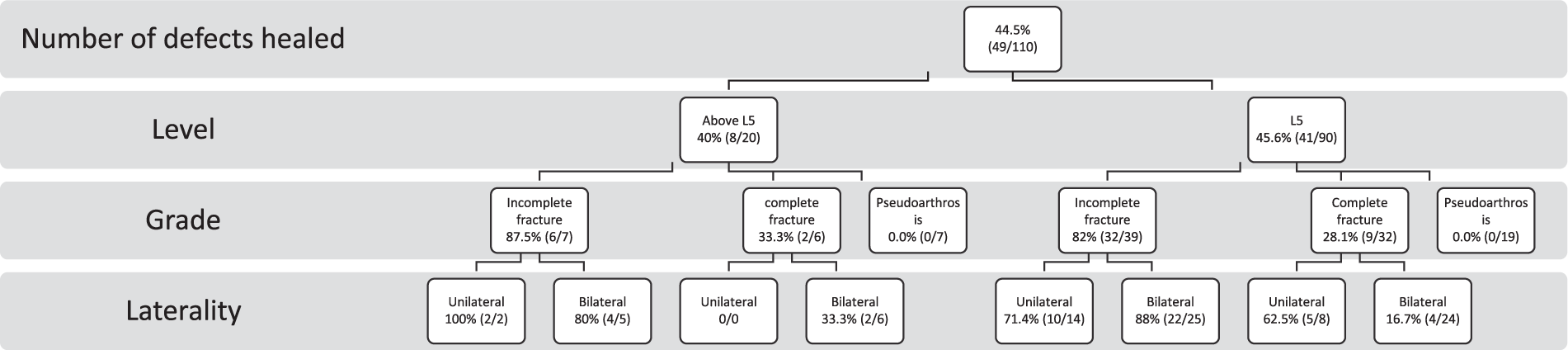
Bony union rates of different skeletal levels, stage of the fracture, and laterality.
Discussion
Validity of the Data
The study was conducted as a retrospective consecutive series. The radiographic analyses were conducted blinded by an independent observer (A.S.). We consider the number of patients (n = 68) to be satisfactory. Follow-up time was 3 months, and our aim was to evaluate bony healing at the end of the treatment. Some of patients may develop a recurrence of the spondylolysis and those not healing a spondylolisthesis during longer follow-up. We did not obtain standing radiographs at the end of immobilization. Bony healing was evaluated using advanced imaging (CT or MR images) done at the end of immobilization in all patients. The correlation of these investigations was generally good. Before treatment, there were two fractures that were classified as incomplete fracture in the MRI and classified as progressive lesions in the CT, while the rest of the incomplete fractures (20 fractures) were also classified as early lesions in the CT. There were two stress reactions seen in the MRI and one did not visualize in the CT. All of the lesions which seemed to be pseudoarthrosis in the MRI were classified as terminal lesions in the CT as well as all of the fractures that were classified as complete fractures in the MRI were graded as progressive lesions in the CT.
After the treatment, there were 11 patients of which both the MRI and CT were taken after the treatment to evaluate the bony healing of the fracture. In one case, the MR image suggested that no bony healing was obtained, while CT showed bony bridges over the fracture line. In the rest of these patients, the CT and the MRI findings correlated well. The patients were advised to wear the Boston brace 23 h a day, but we did not have a sensor in the brace to record the actual use of the orthosis.
Ideally, the effect of high thoracolumbosacral orthosis on the healing rate of pediatric spondylolysis should be confirmed in a randomized clinical trial. However, conducting such a high-level trial is very challenging. For example, the majority of the patients in the Bracing in Adolescent Idiopathic Scoliosis Trial (BRAIST) (13)—comparing the effect of such an orthosis on the progression risk of adolescent idiopathic scoliosis—chose themselves which treatment observation or brace they wanted and the randomized trial arm was ended well before the inclusion requirement was fulfilled.
Comparison with Previous Studies
Spondylolysis is a common cause of back pain in the adolescence, seen in 47% of young athletes complaining lower back pain (14). The bony union of the spondylolysis depends on several factors. The grade of the fracture seems to be an important factor affecting the probability of the union (8–10). The unilaterality and the high signal intensity seen in the MRI prior the treatment seem to increase the probability of osseous healing (9).
Various kinds of rigid orthosis have been used for the treatment of pediatric spondylolysis. In the meta-analysis done by Klein et al. (15), bracing did not seem to affect the clinical outcome of the patients after minimum 1-year follow-up. We could still hypothesize that the higher the bony union rate of spondylolysis, the less lower back problems the patients may have in the long run. Many studies have shown good outcomes with different kinds of braces for the treatment of the spondylolysis. Fujii et al. (8) studied the union rates of 239 spondylolysis defects using a soft Damen corset. The union rate for early lesions was 62%, for progressive lesions 8.7% and for terminal lesions (pseudoarthrosis) 0%. In this study, they also noticed that the L4 spondylolysis had a higher union rate (62.9%) compared to the L5 fractures (8.8%). In our study, the level of the affected vertebra did not have an impact on the union rate and this is not in agreement with the earlier findings by Fujii et al. (8) study, and therefore, further investigations of this subject are needed.
Sairyo et al. (9) used a low hard lumbar brace for immobilization (mean time of immobilization varied from 3.2 months for early and 5.7 months for progressive with low signal intensity group) and noted a bony union in 94% of the early defects, 46% of the progressive-stage defects, and in 0% of the terminal defects. In their study, the treatment time was lengthened up to 6 months if bony healing was not considered to be strong enough after 3 months. In the study of Sakai et al. (10), a low thoraco-lumbo-sacral-type trunk brace (Sairyo-model hard corset) was used to immobilize the patients. They had quite small sample size with only 23 patients with either early or progressive defects (27 had either a stress reaction only or 10 patients a terminal defect) with healing rates 93.8% of the early defects and 80.0% of the progressive defects. In this study, 38 (82.6%) of the early defects, 11 (28.9%) progressive, and none (0.0%) of the terminal defects had a bony union at the end of treatment. Thus, based on this study, a high TLSO does not seem to provide additional benefits as compared with a low rigid brace. Therefore, further studies comparing different kind of braces for the treatment of spondylolysis will be needed to optimize the treatment.
In accordance with the previous studies done by Fujii et al. (8), Sairyo et al. (9), and Sakai et al. (10), none of the pseudoarthrosis/terminal defects had bony union after brace treatment in our study. In this study, the majority of the patients (74%, 14/19) were pain-free after brace treatment. Therefore, the goal of the treatment of the terminal spondylolysis should not be bony healing, but an asymptomatic patient using, for example, a suitable sporting activity level and not a formal immobilization.
Conclusion
Unilaterality, incomplete fracture, and lesions with high signal intensity on MR images predicted healing of pediatric spondylolisthesis. A 3-month immobilization using a high rigid thoracolumbosacral orthosis resulted into following healing rates: 83% of incomplete, 29% of the complete, and 0% of the pseudoarthrosis had a bony union at the end of treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I.H. is a consultant for Medtronic. He has received research grants and funding from Medtronic International and K2M via Innosurge. E.V. has received a research grant from Clinical Research institute HUCH. M.H., K.M., and O.P. declare that they have no conflict of interest.
Ethical Approval
Ethical committee approval was granted by Turku University Hospital. Due to retrospective nature of the research no informed consent was requested by the ethical committee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Medtronic International (Grant No. ERP-2018-11372), K2M via Innosurge (Clinical Research institute HUCH, Project No. 70097).
Informed Consent
This study was a retrospective study and therefore no informed consent was obtained. Individual patients cannot be identified.
Research Ethics
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.