
Abstract
Background and Aim:
Talc poudrage has been used since many years for sclerosing chronic pleural effusion. Several reports have shown good results managing chronic seromas after breast, vascular, and incisional hernia surgeries. The purpose of this study is to determine the utility of talc seromadesis for the management of chronic seromas after incisional hernia surgery
Materials and Methods:
Multicentric prospective observational study including patients diagnosed of chronic seromas after incisional hernia surgery. Under local anesthesia and ultrasonographic control, two percutaneous trocars were placed in the seroma, washing the seroma cavity with 0.9% saline solution and aspirating the remaining liquid. A sample of 4 g of talcum powder was introduced in the seroma cavity, and a 15-F drain was left in place. Patients were followed each week during at least 4 weeks after drainage removal.
Results:
Between January 2013 and December 2016, a total of six patients were enrolled in the study. Talc poudrage was performed without any complications. Drains were pulled out in a mean time of 3 (range: 2–4) weeks. One case of the chronic seromas was efficiently sclerosed with talc without recurrence in time. In three cases, the seroma recurred, and the final solution was surgical decortication of the seroma. In the other two cases, seroma also recurred and were managed with instillation of ethanol and iodine povidone.
Conclusion:
In our experience, the management of chronic seromas after incisional hernia repair with talc seromadesis is ineffective and is associated with a high rate of seroma recurrence.
Introduction
Seroma is one of the most common local complications in abdominal wall surgery. It is typically related to the use of permanent mesh for incisional hernia repair (1). Seroma is defined as an identifiable collection of serous fluid in any tissue, potential space, or cavity after an operation. Its etiology remains unknown (2).
Seromas can be asymptomatic or symptomatic due to expansion or local compression. One of the most common complications is infection that might require urgent drainage. Most seromas will never be diagnosed and will disappear spontaneously. Other seromas will persist and develop a pseudocapsule lined by fibrous tissue that lacks a proper epithelium (3). A persistent seroma will usually require additional procedures for its treatment, including needle aspiration, percutaneous drain placement, sclerosing agent perfusion, or even surgical decortication (4, 5).
Seroma is considered a mild local complication included in the group of “Surgical Site Events” (6), but it can become an annoying entity for both the patient and surgeon. It increases the number of visits and procedures that must be performed in the outpatient clinic and therefore increases the total costs in the patient’s follow-up (7).
Talcum powder was first used in 1935 to produce pleurodesis before performing a lobectomy (8). Since then, talc poudrage has been consistently used to sclerose chronic pleural effusion. Several reports indicated that this treatment produces adequate management of chronic seromas after breast, vascular, and incisional hernia surgery (9–11).
Due to our successful use of talc poudrage for managing a chronic seroma after groin hernioplasty (12), we developed a prospective multicentric study. The aim of our study was to evaluate the outcomes of the management of chronic seromas with talc poudrage after incisional hernia surgery that is refractory to standard treatments.
Materials and Methods
This multicentric prospective study included adult patients diagnosed with subcutaneous chronic seroma after incisional hernia repair that was refractory to percutaneous standard treatments. We defined chronic seroma as any fluid collection palpable or evident with ultrasonography in the subcutaneous tissue beneath a surgical scar with more than 6 weeks persistence after the initial abdominal wall surgery.
Patients were included if they underwent a midline incisional hernia operation with an open approach and mesh insertion. The seroma had to be confirmed and measured with ultrasonography and refractory to the standard percutaneous treatments (needle aspiration and percutaneous drain insertion). We excluded those patients who underwent any instillation of sclerosing agents after the initial percutaneous management. The local ethics committee approved the study, and written informed consent was obtained from all the patients before they entered the study.
Talc Poudrage Procedure
A sample of 2 g of cefazoline was administered 30 min before the procedure. Under local anesthesia and ultrasonographic control, a 10-mm trocar was introduced in the seroma cavity. After aspiration of the serous fluid, a 0° scope was introduced in the seroma cavity with pneumoperitoneum pressure up to 8 mmHg. Another 5- or 10-mm trocar was then introduced in the seroma cavity, the fibrinous debris was removed, and the cavity was washed with 500 cc saline solution. After complete aspiration of the liquid, 4 g talc powder (STERITALC® F4, Novatech, France) was sprinkled in the seroma cavity with a cannula. A 15-F drain was left in place through one of the trocar incisions, and the other wound was closed with staples (Figs 1 to 3). The patients were discharged the same day of the intervention, and the drainage was occluded for 24 h following surgery.

Trocar placement for the seroscopy.
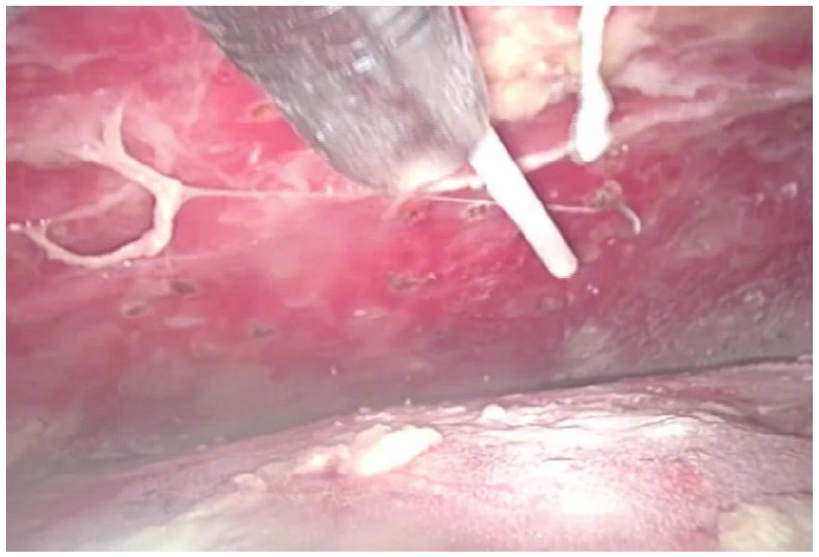
Seroscopy with the view of the cannula placed through the assistant trocar during talc instillation.
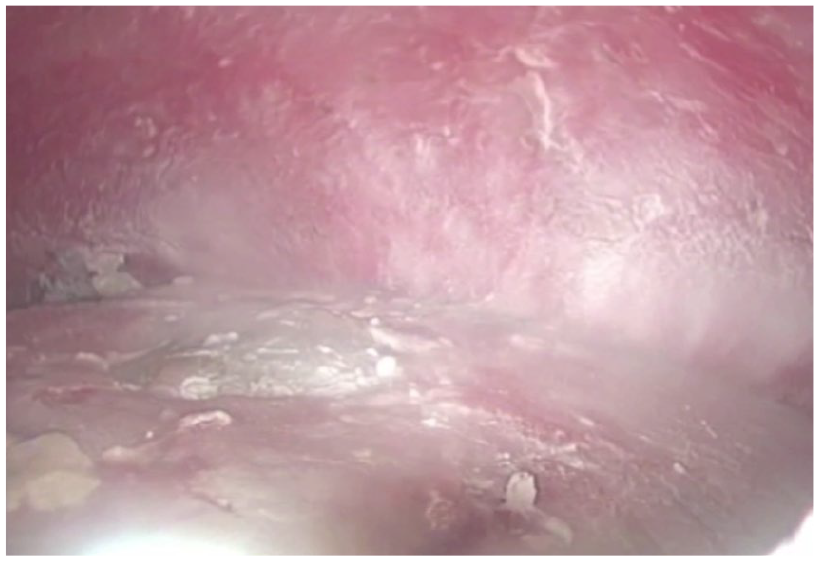
Final view of the seroma cavity after complete aspiration of the seroma fluid and the instillation of 4 g of talcum powder.
Outpatient Clinic Follow-Up
The standard follow-up protocol consisted of physical examination in the outpatient clinic each week until complete seroma resolution. The patients were instructed to connect the drain aspiration 24 h after the hospital discharge and to quantify daily the volume released from the drain. The criterion to remove the drain was a volume less than 25 cc per day. Physical examination and clinical ultrasonography were weekly performed on the patients during the month following drain removal in order to confirm the absence of seroma recurrence.
Statistical Analysis
Quantitative variables are expressed as mean and range and categorical variables as absolute numbers and percentages. All statistical analysis was performed using SPSS, version 22.0 (IBM Corp, Armonk, NY, USA).
Results
Between January 2013 and December 2016, a total of six patients were enrolled in the study. There were three men and three women, with a mean age of 62 (range: 52–72) years. In all cases, the initial abdominal wall surgical technique was a retromuscular Rives-Stoppa. In two cases, it was necessary to add an anterior component separation (ACS). In the remaining cases, a posterior component separation (PCS) with transversus abdominis release was performed in order to obtain complete closure of the midline. All patients presented symptomatic seromas and referred discomfort and bulge subjacent to their surgical incision. All seromas were confirmed with ultrasonography and found in the subcutaneous tissue.
Before their inclusion in the study, all patients underwent a mean of 3.8 needle aspirations (range: 2–6) and a mean of 1.7 percutaneous drainages. The mean volume aspirated in the first needle aspiration was 351.7 (range: 250–450) cc. None of the patients presented important co-morbidities (Table 1). The mean time from the initial surgery to the start of the talc treatment was 6.7 (range 6–8) weeks.
Demographic characteristics and procedures of the patients included in the study.
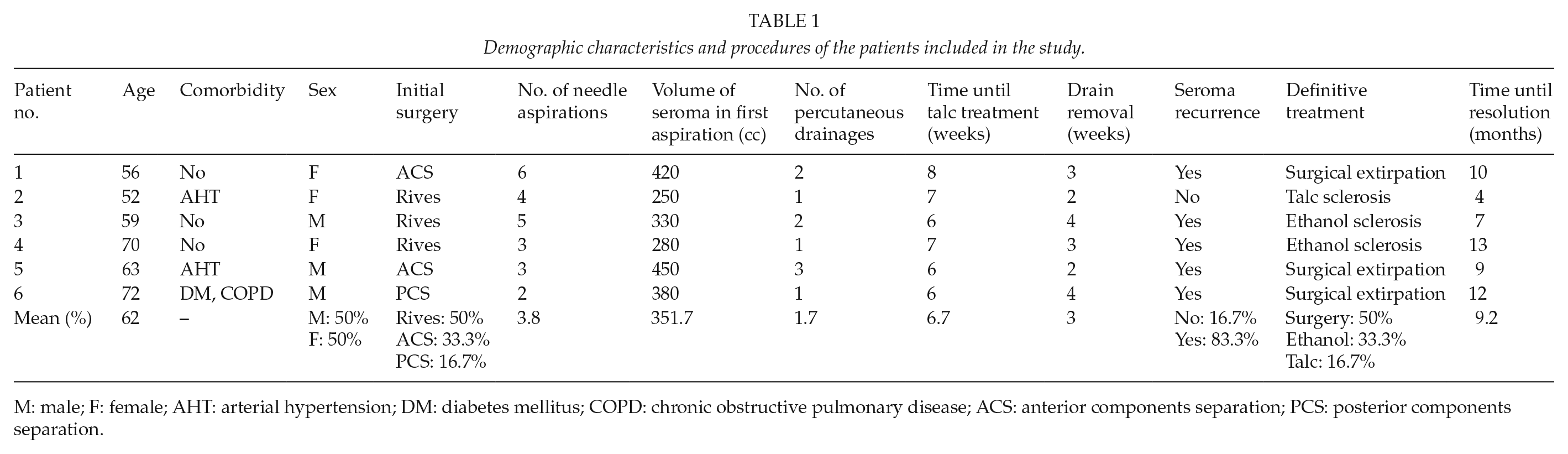
M: male; F: female; AHT: arterial hypertension; DM: diabetes mellitus; COPD: chronic obstructive pulmonary disease; ACS: anterior components separation; PCS: posterior components separation.
The six procedures were performed without any surgical complications, and all patients were discharged the same day of the surgery. Drains were pulled out after a mean time of 3 (range: 2–4) weeks.
One chronic seroma was efficiently sclerosed with talc without recurrence. In three cases, the seroma recurred between 1 and 3 weeks after drainage removal. After new percutaneous drain placement, the final solution for all three cases was surgical decortication. Subsequently, there were no delayed recurrences over time. In the other two cases, there was recurrence in the second and third weeks after drain removal. These two cases were managed with the placement of a new percutaneous drain and the instillation of a 1:1 mixture of ethanol and iodine povidone. After three weekly sessions for the first case and four sessions for the second one, there were no late recurrences.
No episodes of seroma infection appeared during the procedures. In our series, the mean time from the initial incisional hernia surgery until the complete resolution of the seroma was 9.2 (range: 4–13) months.
Discussion
Seroma is one of the most common complications related to surgery. The incidence of this surgical site occurrence is even higher when dealing with incisional hernia repair because the use of synthetic mesh increases the rates of seroma and haematoma formation, chronic inflammation, infection, chronic pain, and mesh migration (1). Most seromas are asymptomatic and will resolve spontaneously even before the patient becomes aware of its presence, and thus there is no need for intervention. Some authors proposed that if asymptomatic or uncomplicated, seromas can be considered a natural part of the healing process related to surgery (13). Park et al. (14) suggested that a seroma should be considered a complication only if it persists for more than 6 weeks, presents continuous growth, or becomes symptomatic. According to these concepts, we considered “chronicity” to be the persistence of the seroma for more than 6 weeks and the presence of symptoms and refractivity to standard percutaneous treatments.
Despite the apparent benignity of this entity as a surgical complication, the persistence of a seroma over time will become a major problem both for the patient and the surgeon. Seroma persistence truly impairs the patient’s quality of life until its complete resolution. Indeed, it increases the number of visits to the outpatient clinic and the associated postoperative costs related to its management. In our study, the mean time for complete seroma resolution was 9.2 months from the initial abdominal wall surgery, with nearly one clinic visit per week during this time.
There is no consensus about the best treatment for chronic symptomatic seromas. There have been myriad publications since the early 1950s (15), but the vast majority are isolated cases or short series, with an obvious lack of comparative studies. The most extended technique is percutaneous repeated needle aspiration followed by mild local compression. Nevertheless, aspiration is associated with a higher risk of seroma infection and has a high recurrence rate (16). Percutaneous placement of an aspiration drain or open drainage of the collection represent alternative options proposed for the management of this pathology. However, these procedures are also associated with high recurrence rates (17).
Lehr and Schuricht (11) described a laparoscopic approach for the treatment of persistent seromas after laparoscopic post-incisional hernia repair. This group proposed a laparoscopically controlled evacuation of both the serous fluid and the fibrinous debris followed by argon beam scarification of the seroma pseudocapsule in order to produce an irritative reaction. When seroma develops a thick surrounding capsule, it is considered to be cystic. In this situation, capsule removal might be the only curative option (18, 19).
Several sclerosing agents have been described in the literature for the management of chronic seromas. In 1983, Nichter et al. (20) preconised the use of tetracycline sclerotherapy for the treatment of persistent seromas. More recently, a case report described the use of doxycycline as another sclerosing agent (21). In 2006, Saeb-Parsy et al. (10) described the application of talc in an 8-month recurrent chronic seroma after breast surgery. They sprinkled 4 g of talc inside the seroma cavity and observed complete wound healing 10 weeks after its application. Using this clinical scenario, other groups obtained similar results (22). In 2012, our group published a case of groin chronic seroma after inguinal hernioplasty that was resolved after talc poudrage in the seroma cavity with no complications (12). In 2013, Metcalfe et al. (9) presented the first reported case of a persistent high-output groin seroma after endovascular abdominal aortic aneurysm repair that was successfully managed with intraoperative application of sterile talc. Throckmorton et al. (5) published their experience with ethanol and povidone iodine as sclerosing agents for the treatment of postmastectomy chronic seromas. In that work, 18 seromas were treated with an 83% rate of success.
In this study, we experienced an 83% of seroma recurrence rate after talc seromadesis; this rate should be considered unacceptable. Despite our promising result with this technique in a chronic seroma after inguinal hernioplasty, five of six chronic seromas after incisional hernia repair recurred. Other techniques were used to solve these recurrences: ethanol and iodine povidone sclerosis in two cases and surgical decortication in three.
Conclusion
In our experience, the management of chronic seromas after incisional hernia repair with talc seromadesis is ineffective and associated with an unacceptable rate of seroma recurrence. Therefore, this technique should not be recommended for the treatment of this pathology.
Footnotes
Author Contributions
J.L-.M. and M.A.G.U. took part in the study conception and design of this study. LB, J.G., and M.A. contributed in acquisition of data. Analysis and interpretation of data were performed by J.L-.M., J.L.L., and A.R. Drafting of manuscript was by J.L-.M., C.S-.M., M.A., and J.M.M. Critical revision of manuscript was given by M.A.G.U., J.L.L., and J.M.M.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from all individual participants included in the study.