
Abstract
Aim:
Our aim was to evaluate the incidence and type of severe complications in adult primary and incisional ventral hernia surgery reported to the National Patient Insurance Centre in Finland during 2003–2010.
Material and Methods:
The Finnish National Patient Insurance Centre covers the whole country and handles financial compensation for patients’ injuries without proof of malpractice. All the claims concerning ventral hernioplasties in the Centre between the years 2003 and 2010 were retrospectively analyzed. The annual numbers of primary and incisional ventral hernioplasties in Finland were obtained from the National Hospital Discharge Register.
Results:
During the study years, 25,738 ventral hernia operations were performed and 127 claims from the whole country were reported to the Patient Insurance Centre. Overall rate of claims was 4.9/1000 hernia procedures. For primary hernias, 16,243 ventral hernioplasties (817 laparoscopic, 15,426 open) were performed and 41 complications were reported. The most common complication was infection (n = 28, 68%) followed by pain and hernia recurrence (n = 6, 15% in both), large hematoma (7%), bowel lesion (5%), urological injuries (2%), or severe bleeding (2%). In incisional hernioplasties, the rate of claims was 9.1/1000 operations (9495 operations, 86 claims). The most common complication reported was infection (n = 42, 49%) followed by hernia recurrence in 25 cases (29%) and bowel lesion in 24 cases (28%). Major complications (n = 15, 17%) consisted mainly of bowel lesions in laparoscopic operations. There was significantly more claims after laparoscopic than open hernioplasties (p = 0.001).
Conclusions:
The claims for financial compensation for injuries related to primary and incisional hernioplasties are quite uncommon. Major complications, though comparatively rare, are significantly more common after laparoscopic operations.
Introduction
Ventral hernia is a fascial rupture that can occur spontaneously as a primary defect or as a defect at the site of previous surgical incision or other trauma. Primary hernias can be classified as umbilical, epigastric, spigelian, and lumbar (1). Incisional hernias are one of the most common complications after laparotomies, with an incidence of 2%–13% (2). The risk factors for ventral hernia formation are known to be male gender, older age, weakened collagen synthesis, obesity, and smoking. Several ventral operations, operative methods used, and postoperative complications such as wound infections can also predispose to hernia formation (3, 4). Hernioplasties are common procedures: approximately 3200 operations are performed each year in Finland with a population of 5.4 million and over 300,000 operations in Europe (5).
Ventral hernia can be asymptomatic but is often associated with complications such as pain, cosmetic discomfort, bowel obstruction, and incarceration (6, 7). Inspection and palpation are the main diagnostic methods for hernia, but sometimes radiological imaging is needed (5, 8). All hernias causing intense symptoms should be considered for operation because of the risks related to bowel incarceration (6).
Several open and laparoscopic surgical techniques exist for ventral hernia repair. The conventional techniques are open operations where fascial defect is either sutured or repaired with a mesh. During the last decade, laparoscopic methods have become more and more popular. In several studies comparing results of open and laparoscopic operations, it has been shown that the time of hospital stay is shorter, postoperative recovery is faster, and the overall complication rate is lower in laparoscopic procedures (10%–32% vs 29%–48%) (6, 9–11). Furthermore, the incidence of hernia recurrence may be lower after laparoscopic operations though comparative studies have not reached statistically significant differences (2, 12, 13). Overall, incisional hernioplasties carry a morbidity of about 23% (14) and mortality of 0.05% (15). Although there are fewer complications in laparoscopic operations, it has been suggested that the complications can be more severe, like organ injuries and especially enterotomies (5, 6, 9, 15, 16).
The Finnish Patient Insurance Centre covers the whole country and ensures compensation for injuries that are connected to patient’s medical or surgical treatment, for example, whether the injury has arisen as a consequence of examination or treatment, has been caused by an infection, or has been caused by an accident connected to examination or treatment unless considered to be unavoidable or tolerable. No proof of malpractice is required. Every patient is insured by the Centre, to which presumably most of the major surgical complications are reported. Patient insurance compensates costs such as medical treatment expenses, loss of income, pain and suffering, permanent functional defect, or permanent cosmetic injuries after surgery. Minor complications considered as tolerable (e.g. superficial wound infections) or consequences that are considered unavoidable are not compensated and thus not usually reported to the Centre. In this register-based study, we evaluated the incidence and type of reported complications in adult primary and incisional ventral hernia surgery in Finland during years 2003–2010.
Patients and Methods
The retrospective material consisted of 127 complications after open or laparoscopic repair of primary and incisional ventral hernia in adult patients that were reported to the Patient Insurance Centre from January 2003 through December 2010. Primary (n = 41) and incisional (n = 86) hernias were analyzed separately. Major complications were separated from milder ones on the basis of severity and the problems patients had in recovering from them. Severe infections (fulminant cellulitis, septic infections and wound infections that needed revision operations or mesh removal), bowel perforations with peritonitis, and massive intra-abdominal bleedings were considered major complications. Minor complications did not lead to life-threatening events.
The annual number of hernioplasties was acquired from the Finnish Hospital Discharge Register, which gathers information regarding diagnosis, surgical procedures, dates of admission and discharge, of each patient. Finnish communal and private hospitals collect data and automatically send it to the register, which is maintained by the National Board of Health (17). The purpose of this register is for research development, administration, and planning.
The data were collected from the Patient Insurance Centre and analyzed using SPSS for Windows, Release 21.0. Univariate analyses for categorical variables were calculated with the Chi-squared test or Fisher’s exact test, and for continuous variables with the Mann–Whitney U-test. p < 0.05 was regarded as significant for both tests. The independent variables included were as follows: age, body mass index (BMI), method of repair, emergency/elective operation, the use of mesh or sutures in operation, re-operation needed, complications distributed as early/late and minor/major, and deaths during hospital stay or within 30 days. Early complications were the ones noted perioperatively or immediately after the operation and treated during the hospital stay. Late complications appeared after discharging from the hospital during next weeks or months. Because the study design was descriptive no multivariate analysis was done.
Results
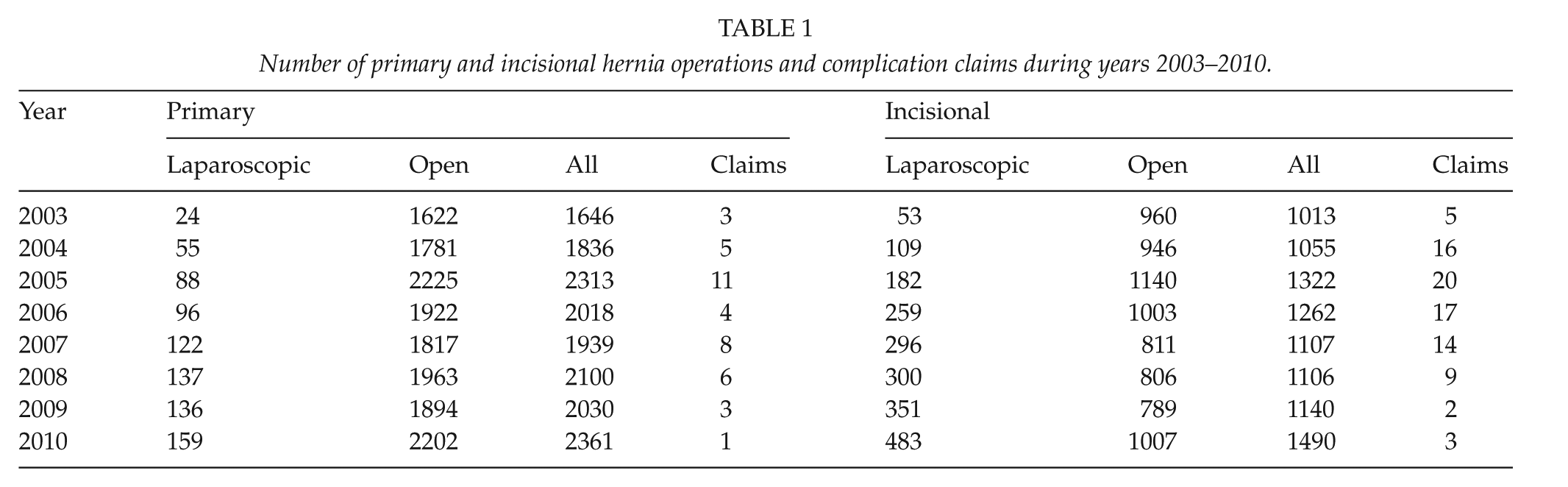
Between 2003 and 2010, 25,738 ventral hernioplasties were performed consisting of 16,243 primary and 9495 incisional hernias. Of primary hernia repairs, 15,128 (93%) were umbilical and 1057 (7%) epigastric. Open techniques were used in the majority of operations; 15,426 (95%) in the primary hernias and 7462 (79%) in the incisional hernias. The annual numbers and types of hernias are shown in Table 1. The amount of open procedures remained stable during the study (Fig. 1A), whereas the frequency of laparoscopic operations increased. The number of claims concerning all hernioplasties decreased over the years with significant difference in laparoscopic group (p < 0.04) (Fig. 1B).
Number of primary and incisional hernia operations and complication claims during years 2003–2010.
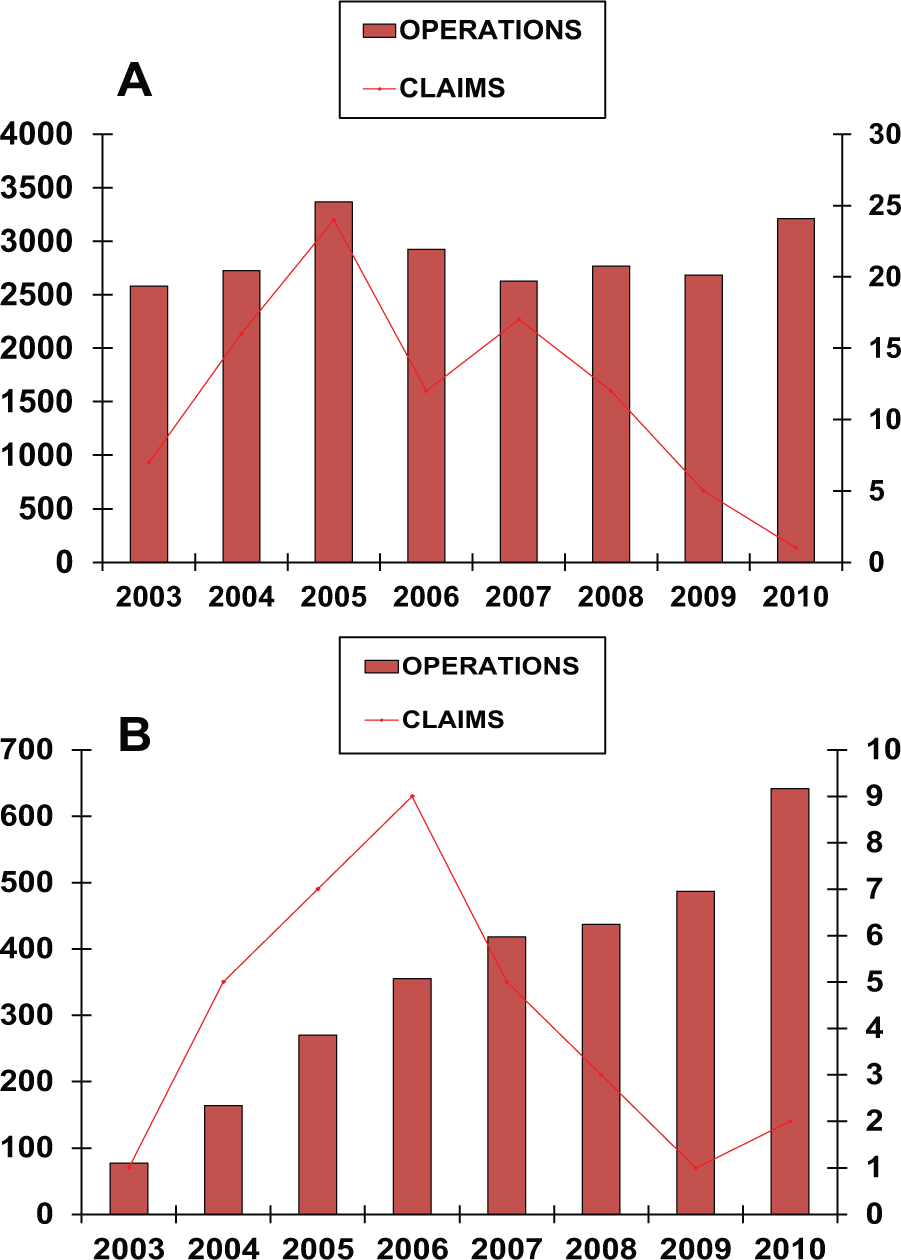
(A) The frequency of claims after open hernioplasties during 2003–2010. (B) The frequency of claims after laparoscopic hernioplasties during 2003–2010.
During this 8-year period, 127 claims were addressed to Patient Insurance Centre concerning all hernia repair operations. Overall rate of claims was 4.9/1000 hernia procedures in Finland. In all, 41 claims were reported after primary hernioplasties, giving the claim rate of 2.5/1000 operations. A total of 86 claims concerned incisional hernioplasties; the rate of claims was 9.1/1000 operations. There were significantly more claims after incisional hernioplasties compared to operations for primary hernias (0.9% vs 0.3% p < 0.001). There were also significantly more claims after laparoscopic operations compared to open operations (11.6 vs 4.1/1000 operations, p < 0.001).
The clinical characteristics of all patients with complications and claims are shown in Table 2. The patients suffering from incisional hernias were more often elderly women than the patients with primary hernias. The majority of the operations were open and elective in both types of hernias. In repairing incisional hernias, mesh was used in 79% of operations compared to only 55% of primary hernia repairs. Patient-related parameters (BMI, age, gender) or surgeon’s experience (resident vs senior) did not show statistical significance when evaluating predictive reasons for complications. In all, 19 major complications were reported consisting of 2 severe infections that led to prolonged recovery and treatment in intensive care unit, 13 bowel perforations with peritonitis and 4 massive intra-abdominal bleedings. There were significantly more major complications after laparoscopic procedures than after open operations (0.5% vs 0.002% p < 0.001). Less than half of the complainers received financial compensation due to complications reported. The reasons for compensation were unreasonable consequences without any proof of malpractice (37%), technical failures (26%), negligence (25%), or delay in the treatment (12%). Other complications reported were considered tolerable or unavoidable considering the patients’ health status.
Clinical characteristics of the patients who claimed for the complications.
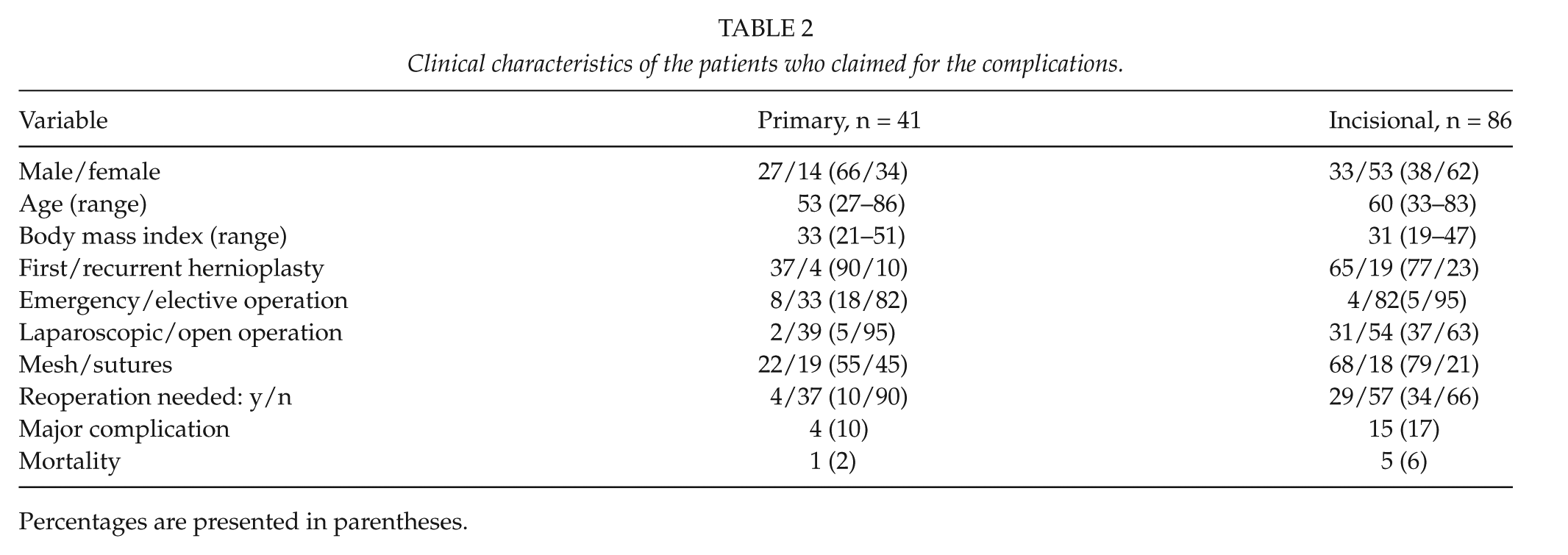
Percentages are presented in parentheses.
Table 3 shows the distribution of complications in claims concerning primary hernia operations, divided into laparoscopic and open groups. Claims concerning open procedures were further divided into sutured or mesh repair. In open technique, the most common complication reported was infection (68%), followed by pain (15%) and recurrent hernia (15%), hematoma (7%), bowel lesion (5%), urological injuries (2%), or bleeding (2%). All reported hernia recurrences (n = 6) occurred to patients treated with open suture repair and in four of them the sutures used were absorbable. All major complications (n = 4, 10%) occurred in open operations consisting of one massive bleeding, one bowel perforation, and two severe infections.
Distribution of complications in primary hernia operations.
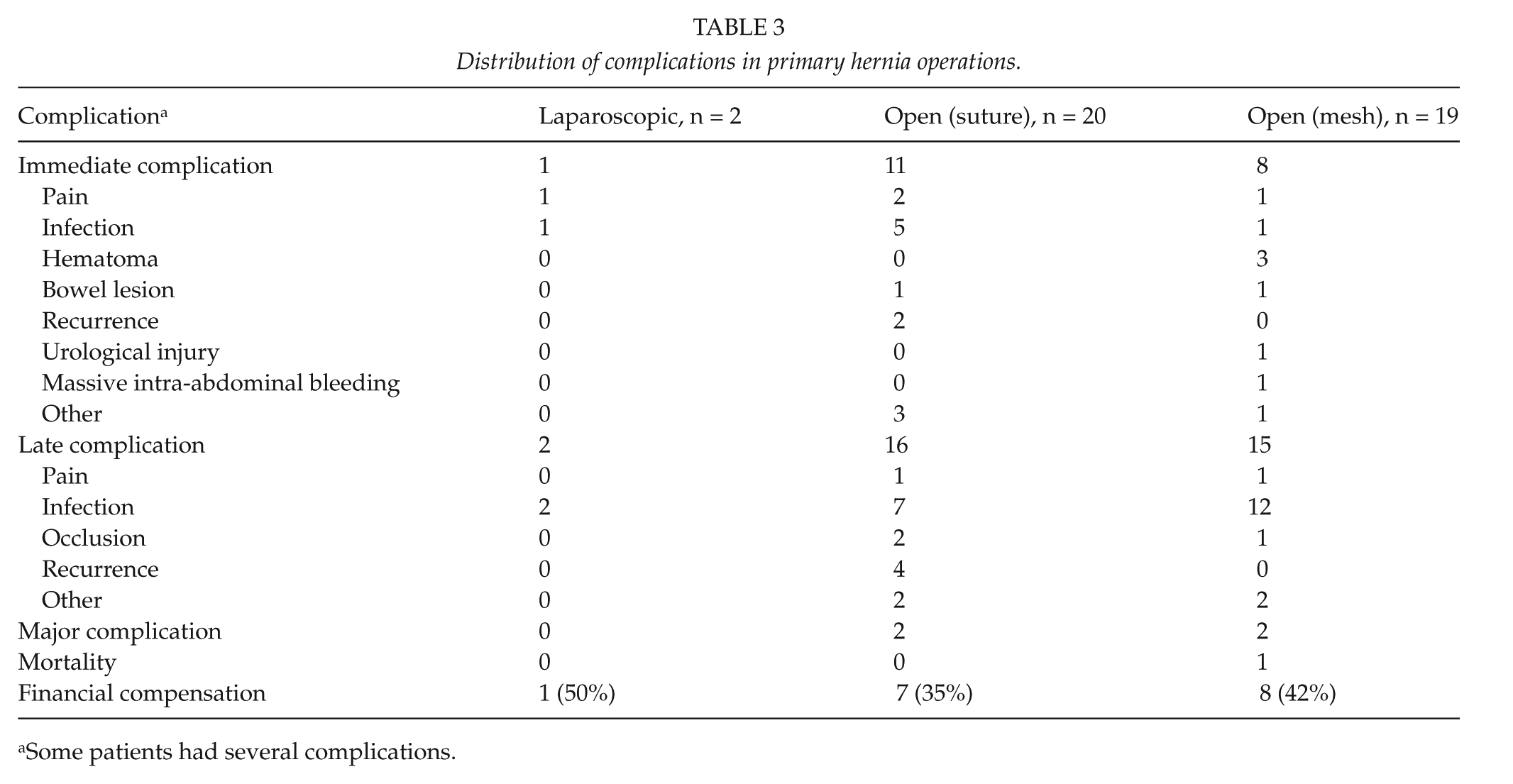
Some patients had several complications.
Table 4 presents the complications reported after incisional hernia operations. Reasons to convert laparoscopic operation into open were bowel lesions (n = 4) and massive intra-abdominal bleeding (n = 2). The most common complication reported was infection (49%), followed by hernia recurrence (29%) and bowel lesions (28%) (Table 4). Other complications were less common (pain 10%, hematoma 6%, urological injuries 2%, bleeding 6%). According to claims, laparoscopic operations were associated with significantly more severe bowel lesions (18 vs 6 p < 0.001) and also overall rate of major complications (13 vs 2 p < 0.001) than open procedures (Fig. 2A and B).
Distribution of complications in incisional hernia operations.
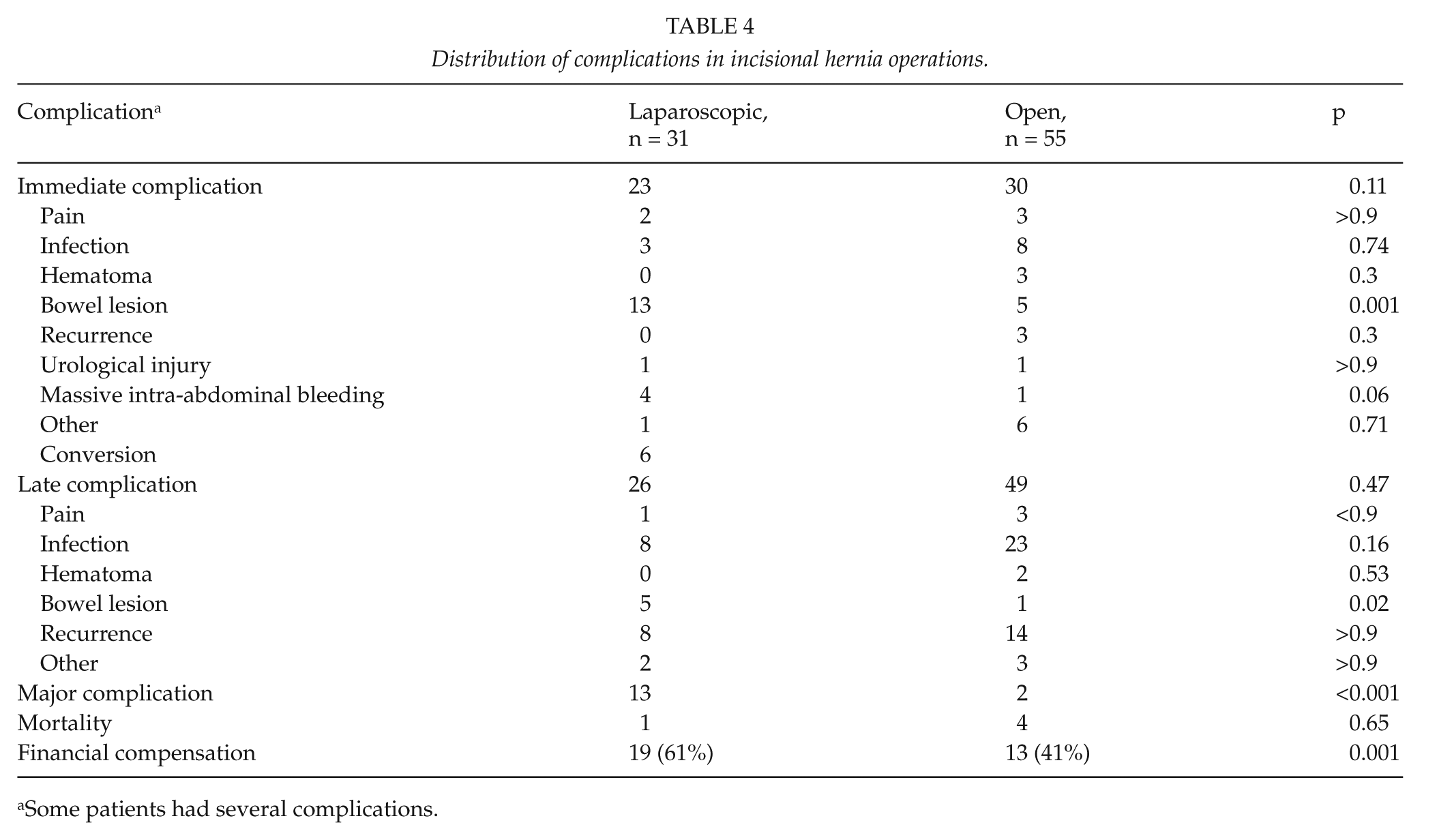
Some patients had several complications.
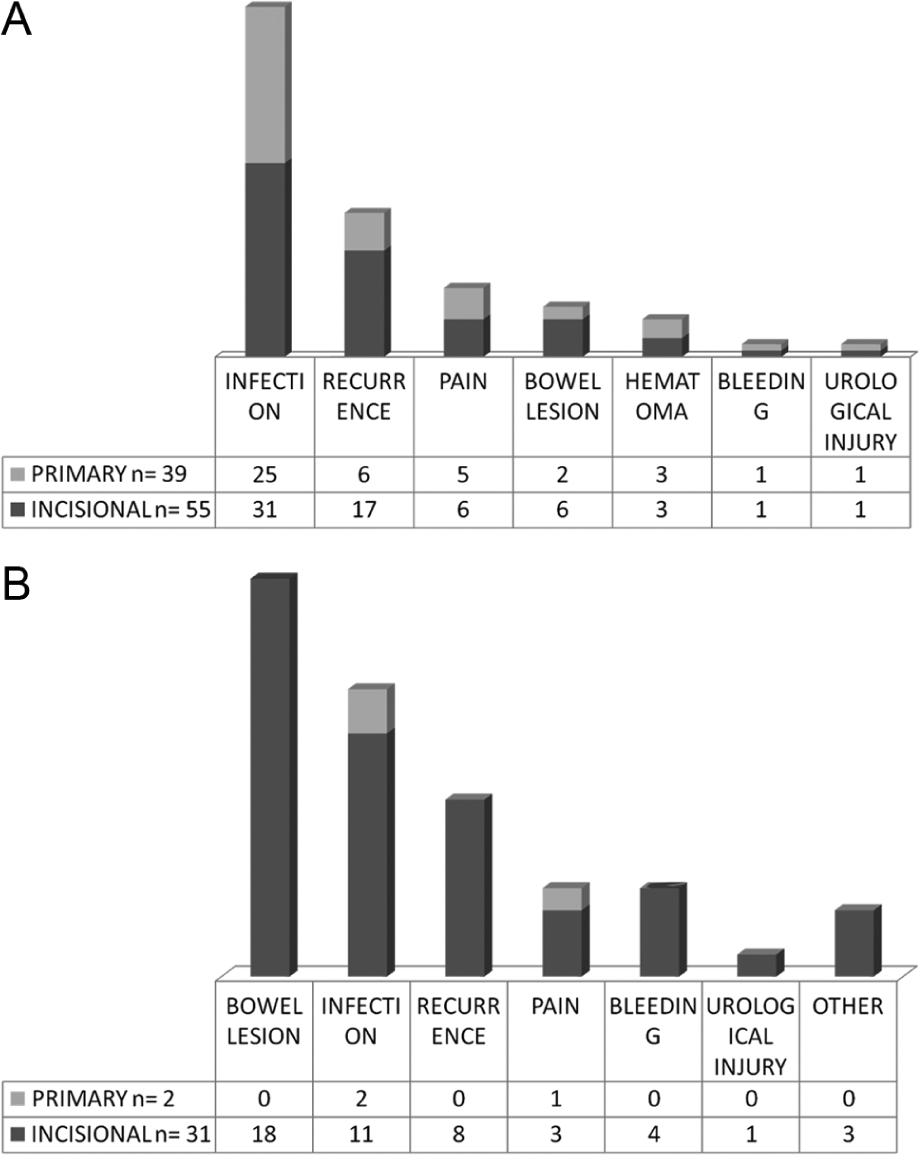
(A) Claims concerning open hernioplasties. (B) Claims concerning laparoscopic hernioplasties.
Discussion
In this retrospective analysis, the incidence of complications that were reported to the National Patient Insurance Centre after ventral hernia repair was only 4.9 per 1000 operations. Based on that, ventral hernioplasty seems to be a relatively safe operation with low rates of severe complications, in line with earlier reports (2, 16). The total number of claims here, however, is much smaller than the expected morbidity rate of some 20% reported in the literature (14). As tolerable or unavoidable complications are not compensated by the Patient Insurance Centre, not all of them are reported either, which is a weakness of this study. Patients are also usually well informed of the risks connected to operations and approve them and consequently, do not see it necessary or useful to report minor problems to the Centre. We assume, however, that similar proportions of complications after different procedures are reported to the Centre, and therefore also comparisons that are made between different hernias and operation types are relevant.
Altogether 48 patients (38% of the claimers) received financial compensation from the Patient Insurance Centre. The remaining claims were considered to be unavoidable or tolerable and were not compensated. Of all complications reported, 15% were considered as major but on a population level that may be an overestimate. The most common complication claimed after was infection followed by hernia recurrence and bowel lesion. It has been shown in the literature that open operations are more frequently associated with postoperative infections (1.3% vs 10.1%) (16) and tend to have more hernia recurrences (3.3–4.3% vs 4.2–12.1%) compared to laparoscopic operations (12, 16). In this study, similar tendency was seen though not with statistically significant differences.
Of the major complications 79% were connected to laparoscopic hernioplasties. In this study, laparoscopic technique was significantly more often used in incisional than primary hernioplasties as primary hernias were more often small and thus repaired by suturing or with special button-shaped ventral patches, which are applied using the open method. The most feared complications after laparoscopic hernia repair are bowel lesions. Especially lesions that remain undetected during the operation are more often connected to laparoscopic than to open repair and are associated with marked morbidity and mortality (18). Extensive adhesions, large hernia size, fistulae, and a prior mesh repair have been reported to be predictive factors for the risk of enterotomy in ventral hernia operations (19, 20). Hernioplasties complicated by enterotomy have a tendency to lead to unplanned bowel resection, sepsis, reoperations, and prolonged hospital stay (19). According to the literature the risk of enterotomy in laparoscopic ventral hernia repair is approximately 2% and in open operations 1% (16). In our study, 0.6% of laparoscopically operated patients appealed for compensation because of consequences of a bowel lesion. The overall incidence of an unrecognized enterotomy is 0.3% (21). In our study, there were five claims for late bowel lesions in laparoscopic group (0.2% of all laparoscopically operated patients). Only one of them was due to unnoticed intestinal lesion, others were caused by fixation material after the patients had been discharged from the hospital. Six patients in this study group succumbed because of complications and another 11 patients ended up with permanently impaired performance ability.
More claims were associated to laparoscopic operations compared to open operations, especially in the early years of this study. It can be presumed that complication frequency was then higher partly due to surgeons’ learning curve as the method was fairly new. Repair of ventral hernia using the laparoscopic technique has become more and more popular during the last decade in Finland as in other Western countries but the complication rate has not increased accordingly. With the increasing experience not only technical skills but also the ability to choose the best operation type for each patient may have improved. When choosing between laparoscopic and open technique many aspects should be considered; for example, patient’s obesity, comorbidities, medication, and the history of previous laparotomies. In our study, however, these patient-related parameters did not show statistical significance when evaluating predictive reasons for complications, probably due to the small number of claims. Of the compensated complications, 63% were due to technical failures, negligence, or delay in treatment. Some of these complications that led to detrimental consequences in this patient cohort may have been avoided by more careful planning and better judgment when choosing the operative technique. Therefore, it is of utmost importance to evaluate not only the frequency but also the backgrounds for the unwanted cause of events. Nationwide registries of complications should be mandatory to get reliable data and to help evaluate and understand the best treatment options for each patient.
Conclusion
To sum up, claims for financial compensation for injuries related to hernioplasties are quite rare. Major complications including death seem to be infrequent but significantly more common after laparoscopic than open operations. Consequently, financial compensation for complications was paid significantly more often after laparoscopic operations.
Footnotes
Acknowledgements
Technical help from Mrs Saija Lehtinen from Patient Insurance Centre is greatly acknowledged.
All authors have contributed equally in acquisition and analyzing of data, drafting, and writing of article.
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.