
Abstract
Background and Aims:
The choice of anesthesia method may influence mortality and postoperative urological complications after open groin hernia repair. We aimed to investigate the association between type of anesthesia and incidence of urinary retention, urethral stricture, prostate surgery, and 1-year mortality after open groin hernia repair.
Materials and Methods:
Data were linked from the Danish Hernia Database, the national patient register, and the register of causes of death. We investigated data on male adult patients receiving open groin hernia repair from 1999 to 2013 with either local anesthesia, regional anesthesia, or general anesthesia. In relation to the type of anesthesia, we compared mortality and urological complications up to 1 year postoperatively. We adjusted for covariates in a logistic regression assessing urological complications and with the Cox regression assessing mortality.
Results:
We included 113,069 open groin hernia repairs in local anesthesia, regional anesthesia, or general anesthesia. The risk of urinary retention adjusted for covariates was higher after both general anesthesia (adjusted odds ratio = 1.64, 95% confidence interval = 1.05–2.57, p = 0.031) and regional anesthesia (odds ratio = 2.99, 95% confidence interval = 1.67–5.34, p < 0.0005) compared with local anesthesia. The adjusted risk of prostate surgery was also higher for both general anesthesia (odds ratio = 1.58, 95% confidence interval = 1.23–2.03, p < 0.0005) and regional anesthesia (odds ratio = 1.90, 95% confidence interval = 1.40–2.58, p < 0.0005) compared with local anesthesia. Type of anesthesia did not influence 1-year mortality or the risk for urethral stricture.
Conclusion:
Patients undergoing open groin hernia repair in local anesthesia experience the lowest rate of urological complications and have equally low mortality compared with patients undergoing repair in general anesthesia or regional anesthesia.
Introduction
Open groin hernia repair can be performed in local anesthesia (LA), regional anesthesia (RA), or general anesthesia (GA). Studies have previously demonstrated that the choice of anesthesia may influence post-operative mortality (1), the risk of urinary retention (2–4), and other urological complications (1). Urinary retention is typically treated with catheterization, which is a known risk factor for urinary tract infection (5) and urethral stricture (6–8). Urinary retention can be a sign of an enlarged prostate that may require prostate surgery with the possibility of increased hospital stay, further postoperative complications, and increased mortality. The lifetime risk of inguinal hernia is estimated to be 27% for men and 3% for women (9). On a global scale, approximately 20 million inguinal hernia repairs are performed each year (10). Thus, the choice of anesthesia potentially affects the postoperative course of a substantial number of patients worldwide. A study investigating urological complications and mortality after open groin hernia repair in relation to the type of anesthesia with national data is lacking.
The aim of this study was to investigate the association between LA, GA, and RA during open groin hernia repair and postoperative urological complications and mortality.
Materials and Methods
This nationwide prospective cohort study based on linkage of three registers is reported according to the RECORD statement (11). The study was approved by the Danish Data Protection Agency (journal number: 2012-58-0004), and data were accessed and analyzed on secured servers from Statistics Denmark. Local ethics committee approval was not required according to Danish law. Data were retrieved from three databases, all with nationwide registration: the Danish Hernia Database (12), the Danish National Patient Register (13), and the Danish Register of Causes of Death (14). The aim of data collection in the Danish Hernia Database is to monitor surgical outcomes after groin hernia repair. Utilizations of hospital and health services are registered in the Danish National Patient Register for the Danish Health and Medicines Authority. These data constitute a statistical basis for future healthcare planning (13), and data registration is required in order for hospitals and clinics to receive economic reimbursements. The primary aims of data collection for the Danish Register of Causes of Death are monitoring of the public health and data provision for analysis of outcomes after medical/surgical treatments (14). The databases contain clinical information such as dates of admission, dates of surgery, International Statistical Classification of Diseases and Related Health Problems (10th revision; ICD-10), type of groin hernia repair, and anesthetic method. Age and gender of patients are available, whereas characteristics such as smoking status, alcohol habits, body mass index, and blood pressure are not registered. Unique civil personal registration numbers (15) were retrieved from all three databases and used for linkage between the different registers on an individual level. The data linkage process is illustrated in Fig. 1.
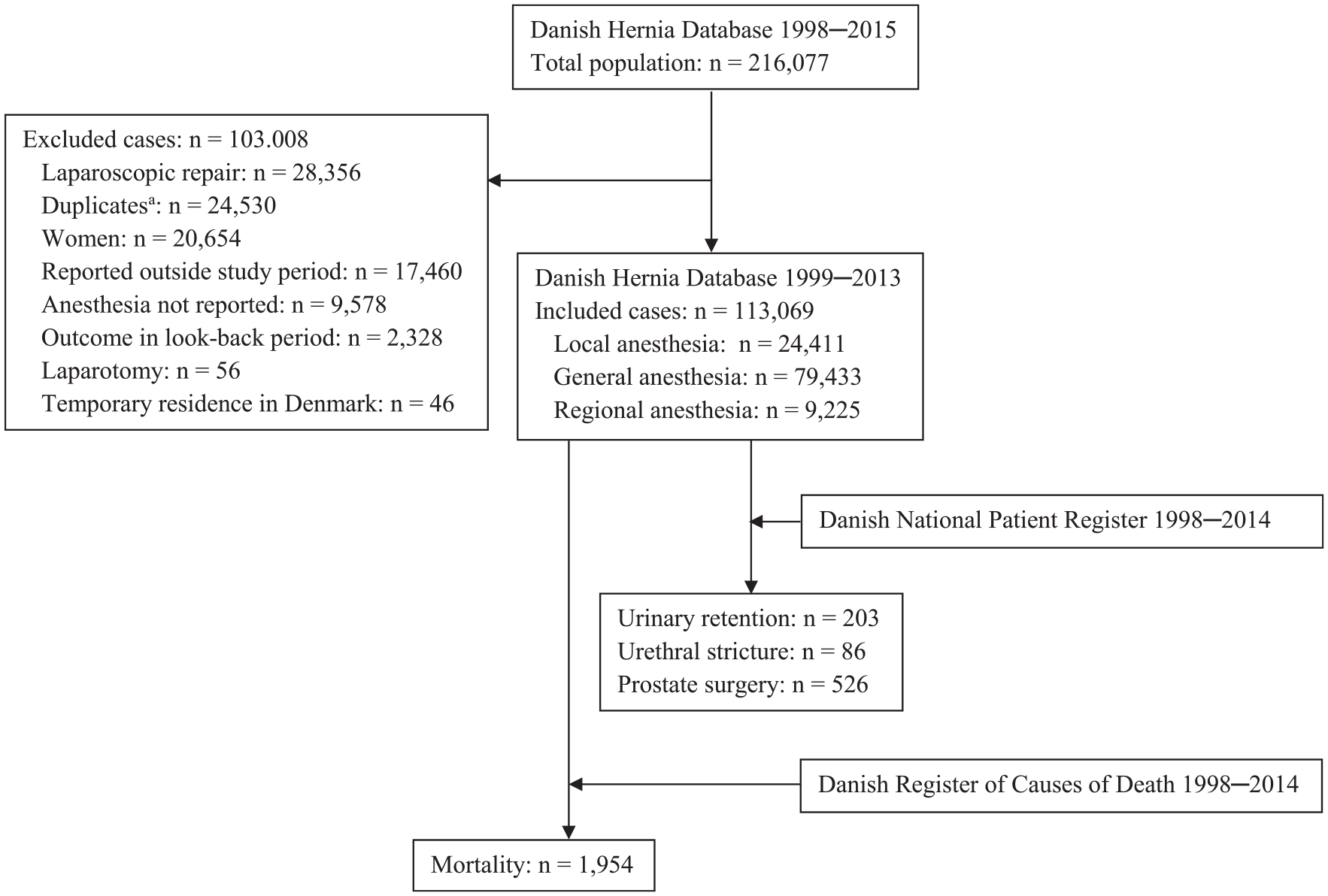
Flow diagram of the data selection and linkage process.
Participants in this study were male patients ⩾18 years of age registered in the Danish Hernia Database. Patients had received an open repair of a primary or a recurrent inguinal or femoral hernia, with or without mesh, in LA, RA, or GA. If data on the hernia type, groin (right or left), or type of operation were missing in the Danish Hernia Database, data were retrieved from the Danish National Patient Register, if possible, and linked through civil personal registration numbers. A single case was defined by a unique identification code consisting of a Danish civil personal registration number and the date of operation. In this way, a case was defined as a single patient undergoing a single operation. Patients could thereby appear several times if they had received more than one open groin hernia repair, that is, cases were defined as operations and not as patients. Patients without permanent residence in Denmark were excluded to minimize loss to follow-up.
Outcomes were urinary retention in the first week following open groin hernia repair, and urethral stricture, prostate surgery, and mortality all within in the first postoperative year. Prostate surgery included resection, incision, or ablation of the prostate. Events of urinary retention, urethral stricture, and surgery on the prostate were identified in the Danish National Patient Register through ICD-10 diagnoses or Nomesco procedure codes. All included ICD-10 diagnose codes and Nomesco procedure codes are presented in Supplementary Table 1. Dates of death were retrieved from the Danish Register of Causes of Death. Data from the 1st January 1998 to the 31st December 2014 were available from the Danish National Patient Register and the Danish Register of Causes of Death, while available data from the Danish Hernia Database covered the 1st January 1998 to the 31st December 2015.
Cases could have urinary retention, urethral stricture, or have undergone prostate surgery before the open groin hernia repair. These factors may have led surgeons to allocate these patients to certain types of anesthesia. To reduce this risk of selection bias, we followed cases for these urological complications in a look-back period of 1 year before their groin hernia repair. Cases with urological events within the look-back period were excluded. The remaining cases were followed for urological complications and mortality for 1 year after the groin hernia repair. We had data from all included registers covering 1998–2014. Consequently, the look-back period covered the 1st January 1998 to the 30th December 2013, the inclusion period of operated cases covered the 1st January 1999 to the 31st December 2013, and the follow-up for outcomes covered 1st January 1999 to the 31st December 2014. To examine the relevance of the problem in more recent time, we also investigated the incidence of each outcome for patients operated within the last 6 years of the inclusion period, that is, 2008–2013. Up to 95% of all groin hernia repairs performed in public and private hospitals in Denmark from 1999 to 2013 were reported in the Danish Inguinal Hernia Database (12).
Data management and analyses were performed in IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA). Outcome incidences are presented both unadjusted and adjusted for each anesthetic type with 95% confidence intervals (CIs). The association between the type of anesthesia and each urological complication was investigated with logistic regression and the results are presented as odds ratios (OR) with 95% CIs. Mortality was analyzed with a Cox regression, and the results are presented as hazard ratios with CIs. A backward elimination approach was used with a cut-off at a p-value of 0.2. The logistic and the Cox regression were adjusted for the following covariates: age, year of surgery, type of admission (elective or emergency), type of hernia (inguinal, femoral, etc.), type of surgery, side of the affected groin (unilateral or bilateral), operation number (i.e. if it was the first groin hernia repair, the second, the third, and so on), and type of anesthesia. In addition, the Cox regression was adjusted for Charlson comorbidity index (16), thereby taking both the number and severity of comorbidities into account. ICD-10 codes in the Danish national patient register were recoded into disease categories as described by Quan et al. (17), and each category was assigned the appropriate weight, according to the Charlson comorbidity index (16). Weighted values for each case were summed and used as the final variable for comorbidity.
Results
We included 113,069 groin hernia repairs in 103,081 male patients. A flow diagram of the inclusion and exclusion of patients is illustrated in Fig. 1, and demography is summarized in Table 1. The incidences of the three types of anesthesia are illustrated in Fig. 2.
Demography according to the type of anesthesia.
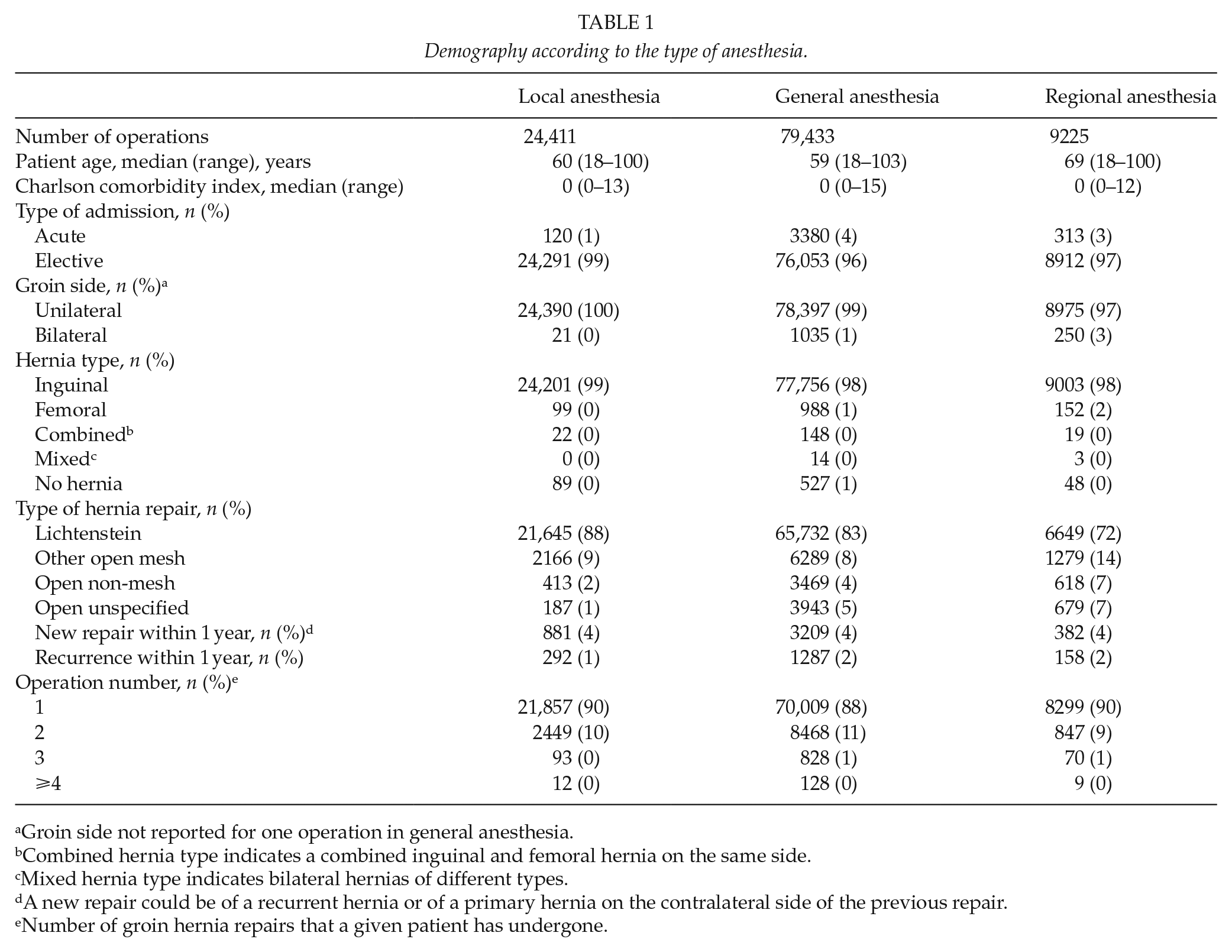
Groin side not reported for one operation in general anesthesia.
Combined hernia type indicates a combined inguinal and femoral hernia on the same side.
Mixed hernia type indicates bilateral hernias of different types.
A new repair could be of a recurrent hernia or of a primary hernia on the contralateral side of the previous repair.
Number of groin hernia repairs that a given patient has undergone.
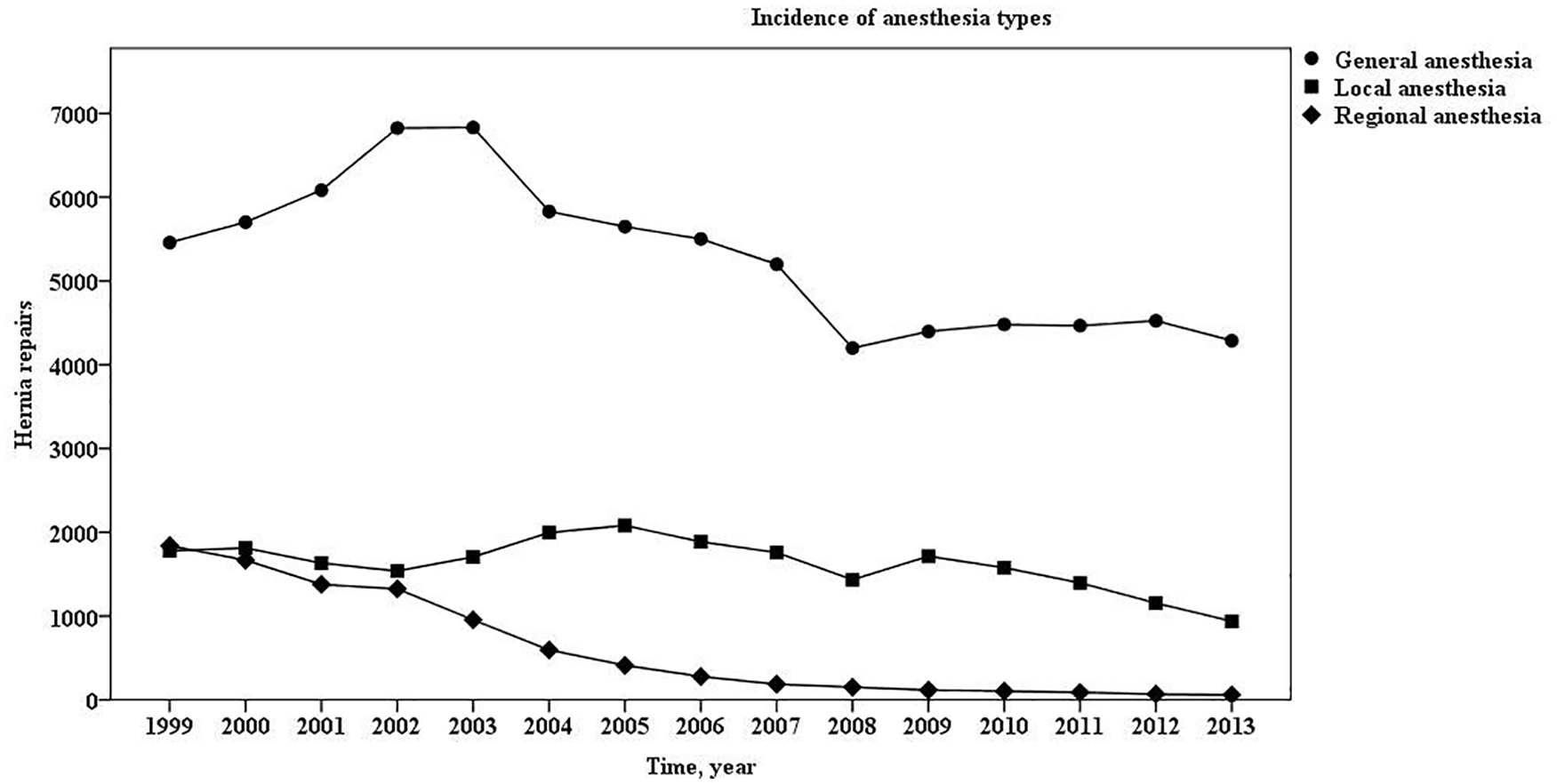
Incidence of anesthesia types.
Unadjusted mortality within the first postoperative year was higher after RA compared with LA and GA (Tables 2 and 3). However, there was no difference between anesthesia groups when adjusting for covariates (Table 4). Factors influencing mortality were increasing age, year of surgery, Charlson comorbidity index, increasing operation number, type of admission, and type of hernia repair. Out of 526 patients undergoing prostate surgery within the first year after open groin hernia repair, 12 patients (2%) died during the follow-up time. Of these patients, three had LA, four had GA, and five had RA for their groin hernia repair.
Unadjusted postoperative complication rates—data from the entire follow-up period.
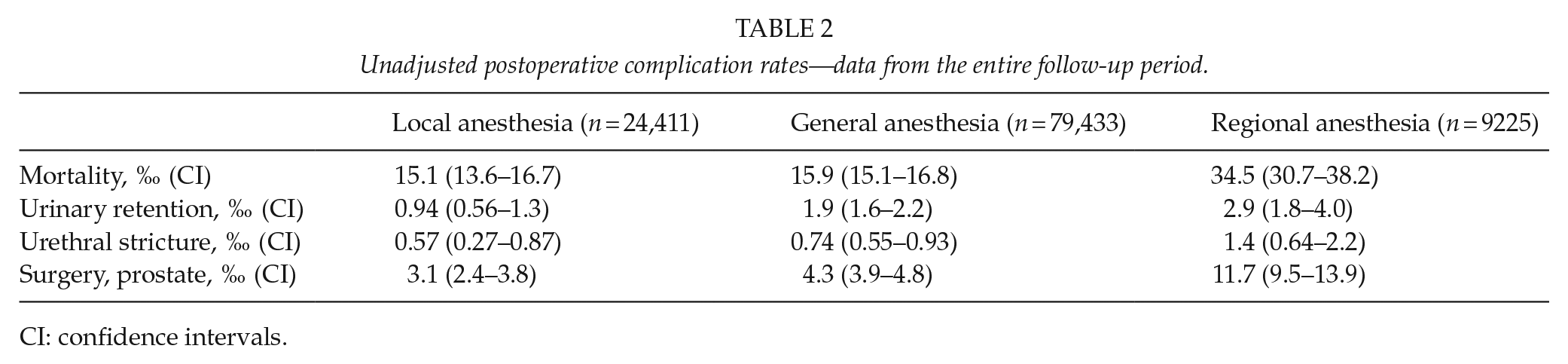
CI: confidence intervals.
Unadjusted postoperative complication rates—data from 2008 to 2013 and followed for complications between 2008 and 2014.
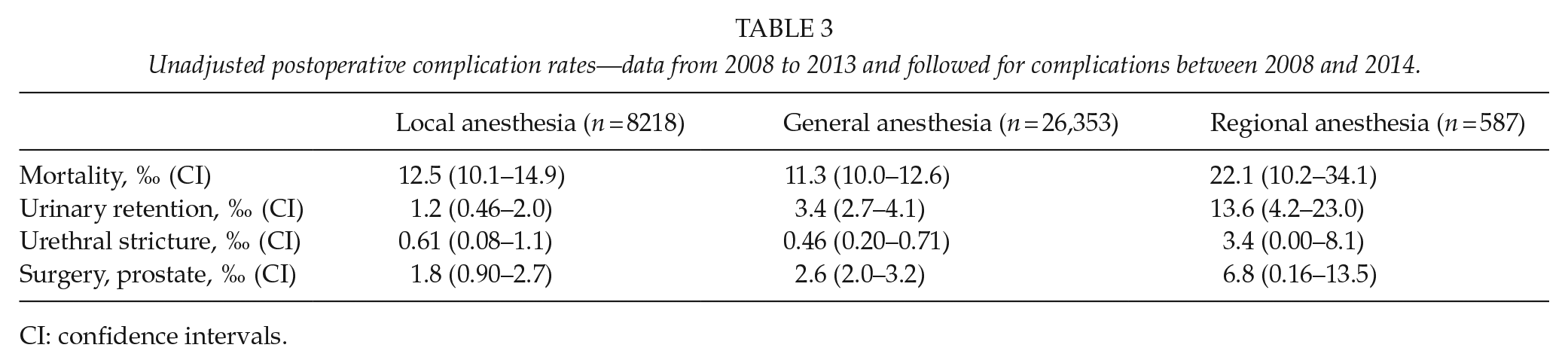
CI: confidence intervals.
Mortality—the first year after open groin hernia repair.
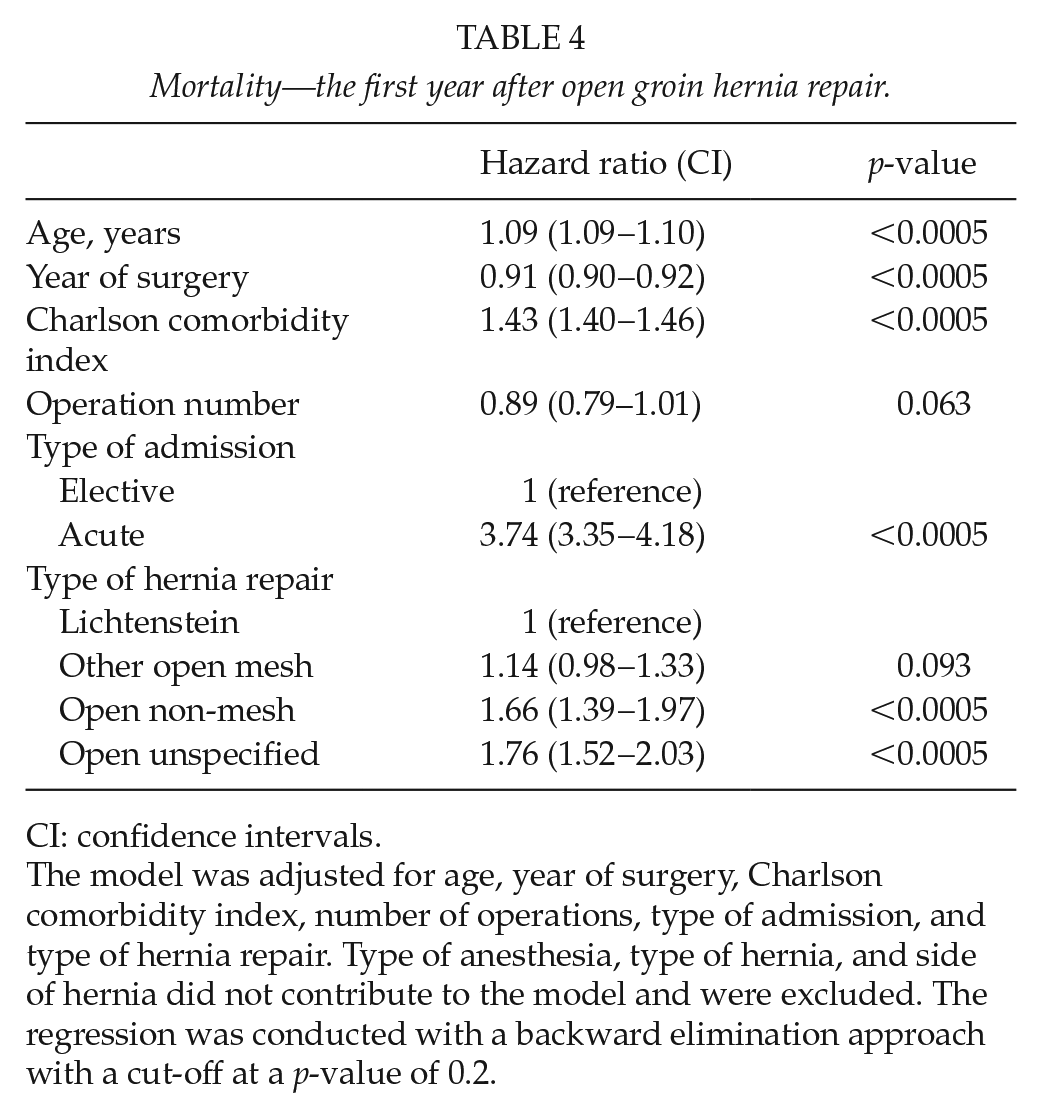
CI: confidence intervals.
The model was adjusted for age, year of surgery, Charlson comorbidity index, number of operations, type of admission, and type of hernia repair. Type of anesthesia, type of hernia, and side of hernia did not contribute to the model and were excluded. The regression was conducted with a backward elimination approach with a cut-off at a p-value of 0.2.
Compared with LA, both unadjusted rates of urinary retention and the risk of urinary retention adjusted for covariates were higher after GA with an OR of 1.64 (95% CI = 1.05–2.57, p = 0.031) and RA with an OR of 2.99 (95% CI = 1.67–5.34, p < 0.0005) (Tables 2 and 5). Rates of urethral stricture did not differ between anesthesia groups, and logistic regression showed no difference in the risks of having urethral stricture between the types of anesthesia. Regarding the remaining covariates, increasing age was a risk factor for urethral stricture with an OR of 1.07 (95% CI = 1.05–1.08, p < 0.0005) while more recent repair was a protective factor with an OR of 0.945 (95% CI = 0.897–0.995, p = 0.032).
The risk of urinary retention—the first week after open groin hernia repair.
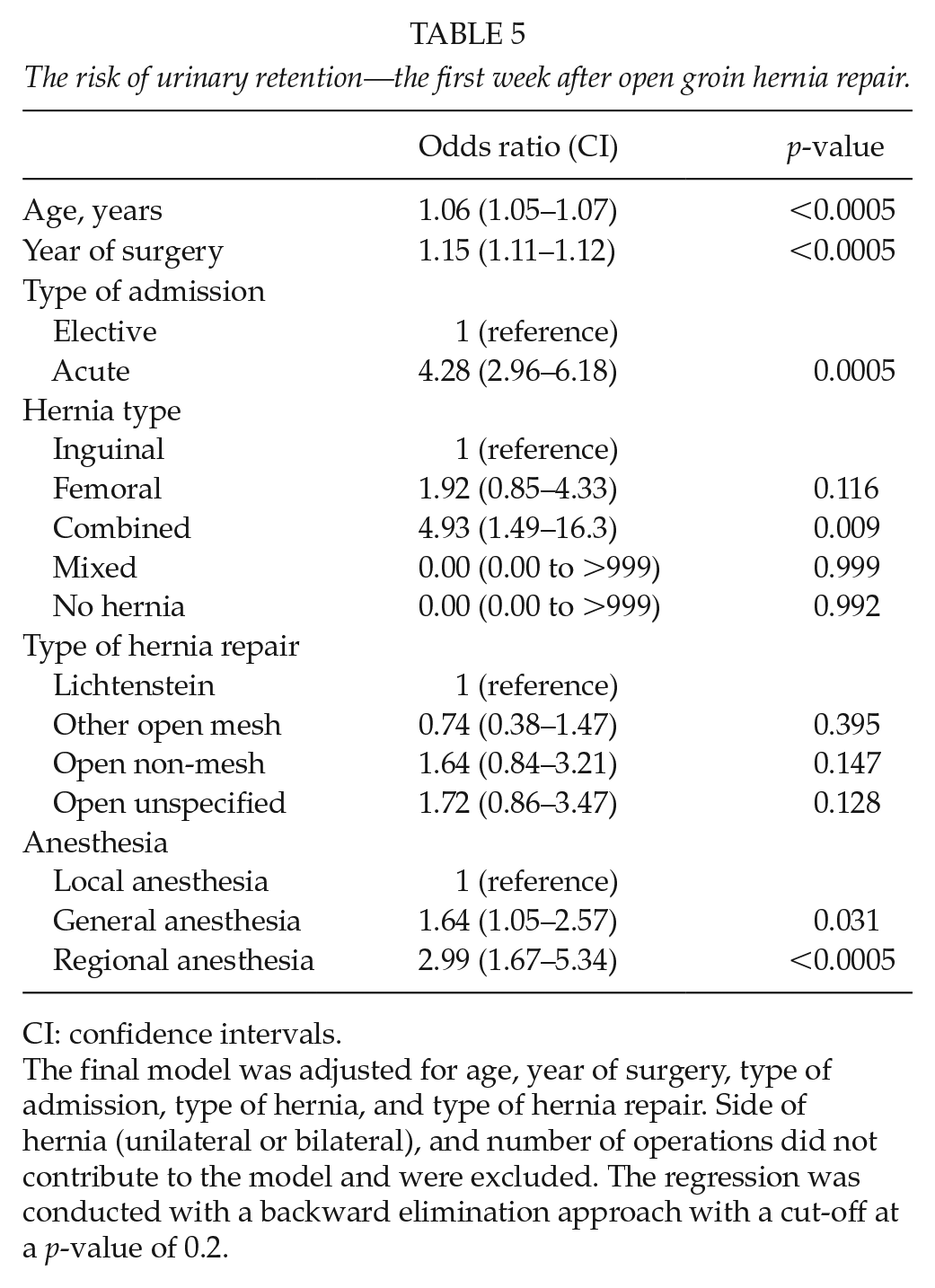
CI: confidence intervals.
The final model was adjusted for age, year of surgery, type of admission, type of hernia, and type of hernia repair. Side of hernia (unilateral or bilateral), and number of operations did not contribute to the model and were excluded. The regression was conducted with a backward elimination approach with a cut-off at a p-value of 0.2.
Unadjusted rates of prostate surgery were highest after RA, intermediate after GA, and lowest after LA. The logistic regression showed an increased risk after GA and RA compared with LA, with an OR of 1.58 (95% CI = 1.23–2.03, p < 0.0005) and 1.90 (95% CI = 1.40–2.58, p < 0.0005), respectively (Table 6).
The risk of surgery on the prostate—the first year after open groin hernia repair.
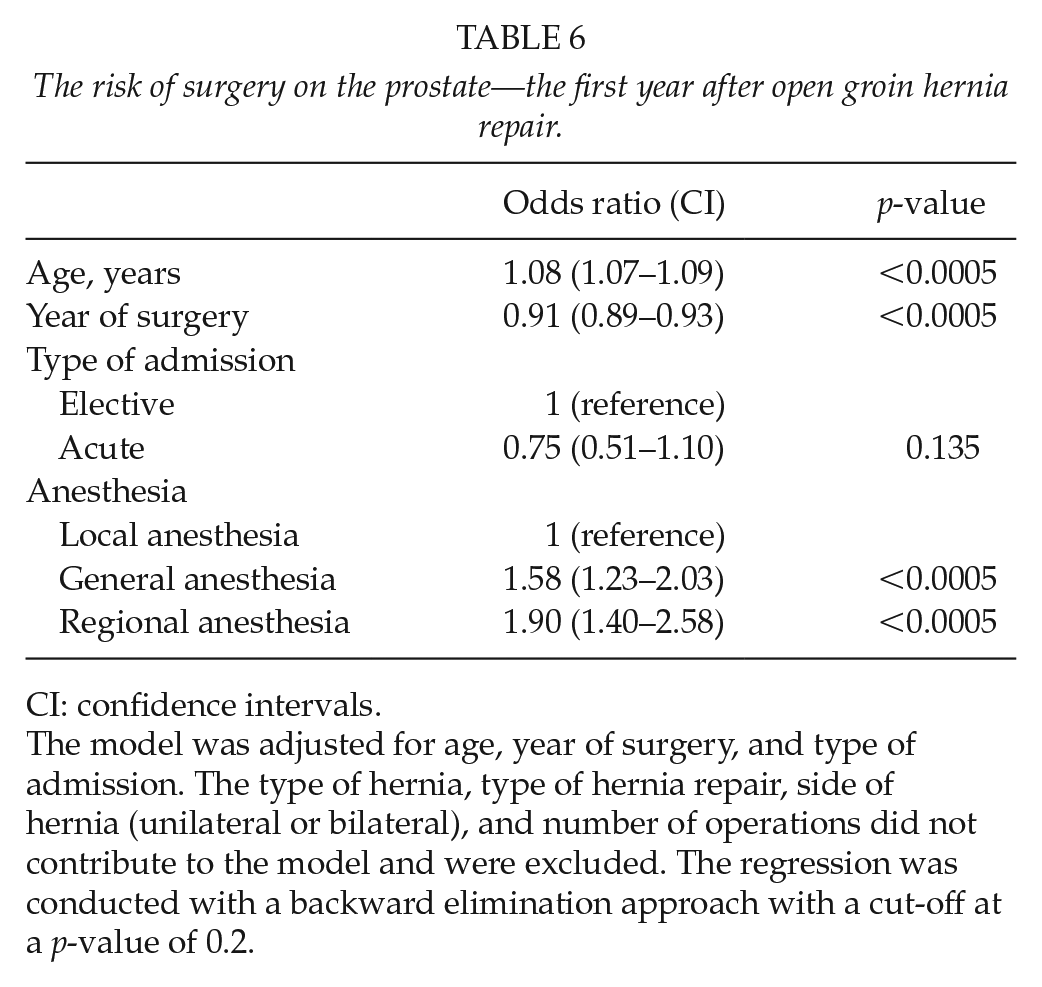
CI: confidence intervals.
The model was adjusted for age, year of surgery, and type of admission. The type of hernia, type of hernia repair, side of hernia (unilateral or bilateral), and number of operations did not contribute to the model and were excluded. The regression was conducted with a backward elimination approach with a cut-off at a p-value of 0.2.
Unadjusted rates of mortality and prostate surgery after GA were lower in patients operated within the last 6 years compared with the total follow-up period. However, urinary retention after GA and RA had increased while still being low. Patients operated within the last 6 years had the same absolute risk of complications between the three anesthesia groups except urinary retention, which was highest after RA and lowest after LA (Table 3).
Discussion
This cohort study with linked data from three nationwide databases showed a lower risk of urinary retention within the first week and prostate surgery within the first year after open groin hernia repair in LA compared with both GA and RA. There was no difference in risk of ureteral stricture or 1-year mortality between anesthesia groups. Patients in GA had a lower mortality and risk of prostate surgery when operated within the last 6 years of the inclusion period compared with the total inclusion period. Urinary retention after GA and RA had increased in patients operated during the last 6 years compared with the total inclusion period, while the absolute risks remained low.
Our finding of a lower risk of urinary retention after LA compared with GA and RA is in line with previous studies (2,3). The absolute risk of urinary retention was very low in all cases in this study and may be clinically irrelevant. The incidence rate of urinary retention in the general male population is estimated to 2.2‰–8.5‰ per year (18), and urinary retention has been estimated to occur in 10.6% of all patients after open inguinal hernia repair (19). While the reporting of surgical procedures and mortality to the databases is high (13,14), it is plausible that urinary retention might be less frequently registered since it will not trigger a fee to the clinical department. The finding of a low risk of urinary retention in this study may therefore reflect incomplete reporting of diagnose codes. Our finding that LA is associated with the lowest risk of prostate surgery is in accordance with a previous register study, which found a lower risk of urological complications after LA compared with RA (1). However, our finding that the type of anesthesia did not influence postoperative mortality differs from results of the same study which reported a higher mortality after RA (1). This previous study did not adjust for covariates. We found a slightly higher crude mortality rate after RA compared with LA and GA which was not confirmed by the Cox regression. Cases had a median age which was 10 years older in the group undergoing RA compared with the patients in the two other groups of this study. Higher unadjusted mortality rates as well as previous unadjusted findings of a higher mortality after RA could therefore reflect differences in age as well as comorbidity.
Strengths of this study include a large study population and several years of prospective data reported with a consistent use of ICD-10 and Nomesco codes throughout the study period. The nationwide coverage of both acute and elective surgery of both primary and recurrent repairs of inguinal and femoral hernias increases the external validity of the results. Furthermore, this is one of the few studies with urinary retention after groin hernia repair as a primary outcome. The positive predictive value of ICD-10 diagnostic coding in the Danish National Patient Register has been validated as consistently high for the Charlson comorbidity index, as the positive predictive value for all diagnose codes pooled is 98%, ranging from 82% to 100% within the individual disease categories (20). Limitations of this study include the possibility that cases could undergo new surgical interventions within the time of follow-up. The rates of all outcomes could increase if cases underwent new groin hernia repairs or other surgical interventions requiring anesthesia during the follow-up time. As for all register studies, our study was dependent on the variables reported in the included registers and on complete reporting of outcomes and exposures. Factors such as smoking habits, alcohol consumption, body mass index, and blood pressure may all influence postoperative mortality. However, none of these covariates were reported in the included registers and could consequently not be adjusted for in the Cox regression. Obesity of the patient, inexperience of the surgeon, and large or complicated hernias may prolong the operation time. Longer operations demand greater amounts of anesthetics, which may increase the risk of urological complications. Furthermore, less experienced surgeons may prefer GA as it is easier to operate fully sedated patients. Surgeons may also be reluctant to operate patients with obesity or large or complicated hernias in LA, thereby introducing selection bias in favor of LA. Operation time and experience of the surgeon are not reported in the Danish Hernia Database. Even though hernia size is now registered in the database, it has not been from the commencement of the database and is only reported in 10% of patients operated between 1998 and 2015. LA, GA, and RA can be performed with different techniques, and with different types of anesthesia that may all have differing effects on postoperative complications. Different doses of intravenous fluids could also influence the risk of urological complications since excessive use of perioperative fluids is a risk factor for urinary retention (8). While these factors may influence the results, they are not reported in the included registers and could consequently not be assessed.
International guidelines advocate for LA for open inguinal hernia repair based on the assessment of a lower risk of complications. RA is discouraged, as it has no advantages compared with LA and GA (21). In this study, LA had the lowest morbidity compared with GA and RA. RA was neither associated with the lowest morbidity nor mortality. Accordingly, our results support current guidelines. The incidence of stricture, prostate surgery, and mortality after open groin hernia is too low to be assessed in randomized controlled trials. Rates of urinary retention were also low in this study, possibly due to underreporting in the Danish National Patient Register. However, previous studies have reported varying but higher rates of urinary retention than the rates found in this study (2,3,19), and urinary retention after open groin hernia repair in LA, RA, or GA may be further investigated in future randomized controlled trials and subsequent meta-analyses.
In conclusion, LA for open groin hernia repair was associated with the lowest risk of urological complications when compared with GA and RA. Mortality did not differ between anesthesia types and was low after prostate surgery within the first year after open groin hernia repair. Consequently, our results advocate for the use of LA for open groin hernia repair even though results may be influenced by confounders not reported in the included registers and possibly by incomplete reporting of events of urinary retention.
Supplemental Material
Supplementary_Table_1 – Supplemental material for Mortality and Urological Complications After Open Groin Hernia Repair in Local, General, and Regional Anesthesia: A Nationwide Linked Register Study
Supplemental material, Supplementary_Table_1 for Mortality and Urological Complications After Open Groin Hernia Repair in Local, General, and Regional Anesthesia: A Nationwide Linked Register Study by J. H. H. Olsen, K. Andresen, S. Öberg, L. Q. Mortensen and J. Rosenberg in Scandinavian Journal of Surgery
Footnotes
Declaration Of Conflicting Interests
J.H.H.O., K.A., S.Ö., and L.Q.M. reported no potential conflicts of interest. J.R. reported personal fees from Merck, outside the submitted work.
Ethical Approval
The study was approved by the Danish Data Protection Agency (journal number: 2012-58-0004). According to Danish law, local ethics committee approval was not required.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.