
Abstract
Background and Aims:
Smoking increases the risk of postoperative complications after bariatric surgery. Therefore, preoperative smoking cessation is mandatory according to Danish guidelines before elective bariatric surgery. The aim of this study was to investigate if patients scheduled for bariatric surgery continue to smoke on the day of their operation despite recommendations.
Materials and Methods:
A prospective single-center study including all patients scheduled for bariatric surgery from June to December 2017 at Zealand University Hospital in Denmark. Urine samples were collected on the day of surgery to test for cotinine. During the minimum preoperative period of 3 months, patients were repeatedly informed of the increased risk of complications, that smoking cessation was mandatory, that rescheduling of the surgery was possible if more time to achieve smoking cessation was necessary, and if tested positive on the day of surgery, the operation would be canceled.
Results:
Of the 71 patients included, 9 patients (13%) were tested positive. After confrontation with the test result, all but 1 patient confessed to smoking. Overall, 6 out of 12 patients (50%) who were actively smoking at the time of referral tested positive, and 2 out of 25 patients (8%) who claimed to have smoked previously tested positive. No patients claiming no smoking history tested positive.
Conclusion:
Despite information that smoking cessation was mandatory, and the scheduled bariatric operation would be canceled in case of smoking, up to 50% of patients with a history of smoking still smoked on the day of surgery.
Introduction
Smoking increases the risk of postoperative complications after bariatric surgery. Two studies including National Surgical Quality Improvement Program (NSQIP) data from 41,445 and 33,714 patients, respectively, showed that smoking increased the risk for pneumonia and sepsis almost by a factor of 2 after gastric bypass and increased the overall risk of 30-day complications with 20% after gastric sleeve (1, 2). In the long-term, smoking increases the risk for marginal and perforated ulcers (3).
Therefore, preoperative smoking cessation is advised by the American Associations of Metabolic and Bariatric Surgery and is required by the Danish Health Authorities. At Zealand University Hospital in Denmark, we therefore have a strict policy of mandatory smoking cessation prior to bariatric surgery. Our aim with this study was to investigate how many patients continued to smoke despite this policy.
Material and Methods
The study was a prospective single-center study including all patients scheduled for laparoscopic gastric bypass or gastric sleeve from June to December 2017.
Patients were referred by a general practitioner and eligibility was assessed by an endocrinologist, a surgeon, a dietitian, a nurse, and a psychologist on request. According to Danish guidelines, indication for surgery was a body mass index > 35 kg/m2 plus an obesity-related comorbidity including type 2 diabetes, hypertension, polycystic ovarian syndrome, obstructive sleep apnea, or arthrosis. Patients underwent minimum 3-month preoperative preparation, during which they had individual and group consultations in order to reach a required 8%–12% weight loss and complete smoking cessation minimum 6 weeks prior to surgery.
All patients were extensively informed of the increased risk of complications associated with smoking. Support for smoking cessation was available for all patients. Postponement of the scheduled operation was possible if more time for smoking cessation was needed. Patients were informed that a urine test for smoking on the day of surgery was mandatory and that the operation would be canceled in case of a positive test. Information on smoking cessation was repetitively provided by the bariatric team throughout the preoperative period at minimum three subsequent consultations. Nicotine replacement therapy was not allowed.
The preoperative smoking status was divided into active, previous, and never smoking and was defined at the first consultation. All patients reported complete smoking cessation at subsequent consultations. The target population for the smoking cessation intervention was all actively smoking patients regardless of self-reported smoking status.
The study was conducted as a Clinical Assurance Project, which allowed for data collection and data storage.
Nicotine Testing
Urine samples were collected from all patients on the day of surgery and were tested for cotinine. The cotinine urine test provided high sensitivity (>99%) and specificity (>99%) for smoking for at least 72 h. Cotinine has a long half-life compared to other metabolites used for distinguishing smokers from non-smokers and has shown to be the most effective indicator (4). Cut-off levels are 568 nmol/L, which means that all products containing nicotine will give a positive result. However, patients passively exposed to smoking will generally not test positive. Results are available within 5 min.
Statistical Analysis
Data were analyzed using non-parametric statistics. Categorical data were assessed by the chi-square test and continuous data by the Mann–Whitney U test; p < 0.05 was considered significant.
Results
During the inclusion period, 71 patients were scheduled for bariatric surgery. Nine (13%) patients tested positive for cotinine on the day of their scheduled surgery. Overall, median age was 37 (range = 22–58) years. Median age among patients testing positive was 32 (range = 22–48) years, and they were thus younger than patients testing negative (p = 0.051). For further characteristics see Table 1.
Characterization of patients undergoing bariatric surgery and tested for urine cotinine at the day of bariatric surgery.
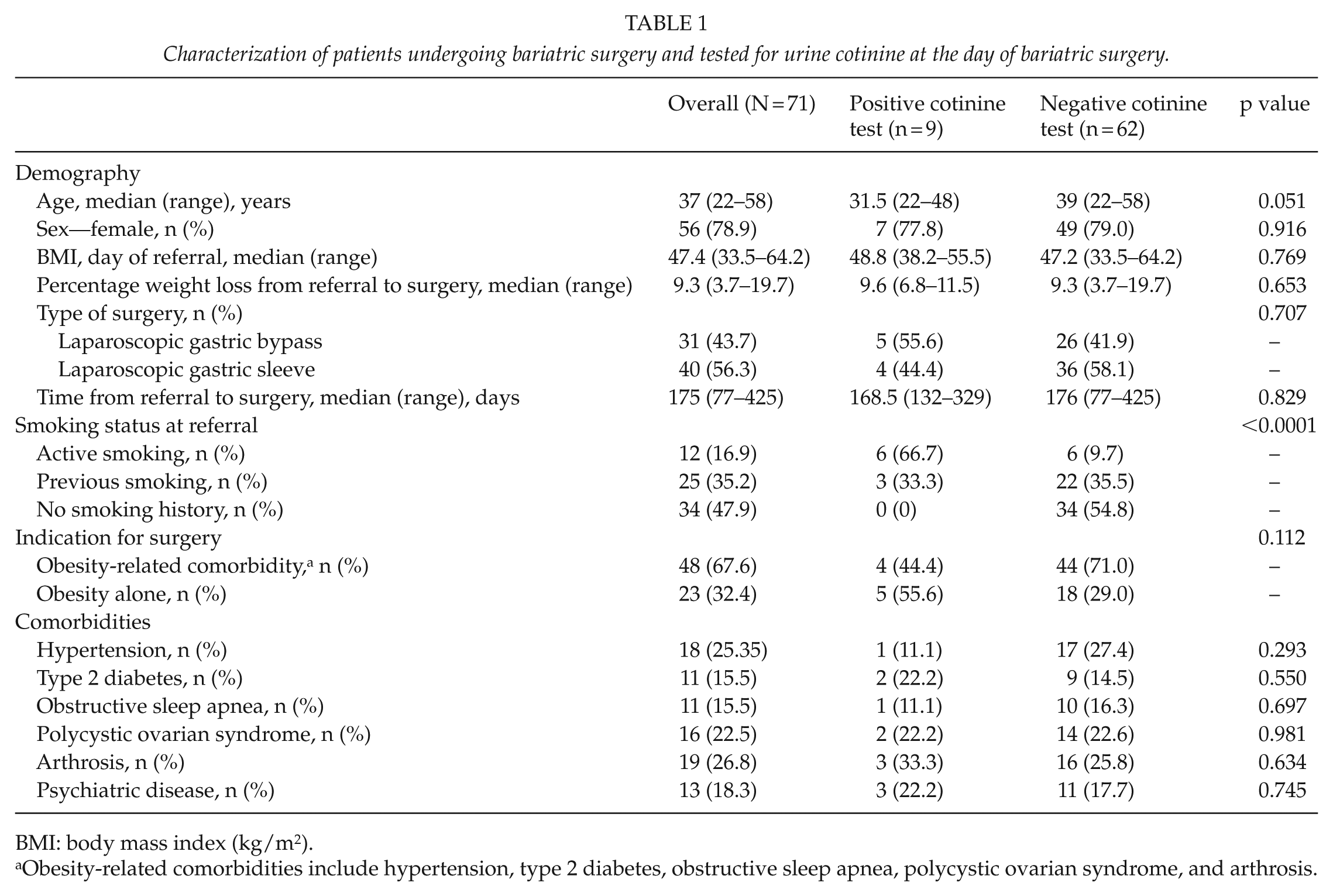
BMI: body mass index (kg/m2).
Obesity-related comorbidities include hypertension, type 2 diabetes, obstructive sleep apnea, polycystic ovarian syndrome, and arthrosis.
A total of 12 (17%) patients were actively smoking when referred to surgery of which 6 (50%) patients failed to quit smoking. In total, 25 (35%) patients claimed to have been smoking previously of which 3 (8%) patients failed to quit smoking. The remaining 34 (48%) patients had never smoked and none tested positive for cotinine.
Eight of the nine (89%) patients who tested positive confessed to smoking. One patient claimed to have been heavily exposed to passive smoking due to her job at the psychiatric ward. The surgery was rescheduled 3 months later, where the test was negative.
Two patients confessed to smoking immediately, whereas the rest confessed after the test result. Reasons for continuation of smoking were similar among patients and each had several excuses including nervousness about the upcoming surgery, the need for one last cigarette before smoking cessation, that the test would not detect the smoking, and the belief that smoking would not be harmful for the surgical outcome. One patient was admitted to the surgical ward 3 weeks after cancelation of the surgery due to anastomosis leakage after having undergone self-paid bariatric surgery abroad.
Discussion
Up to 50% of the patients scheduled for either laparoscopic gastric bypass or gastric sleeve were still smoking on the day of surgery. This in spite of thorough information regarding the increased risk of complications when smoking, the possibility of rescheduling if more time for smoking cessation was needed, and cancelation of the surgery if the patient continued to smoke. Except younger age and smoking at the time of referral, no other predictive factors were found.
Patients referred for bariatric surgery have been through multiple diets and are highly motivated. Thus, this study also emphasizes the difficulty of smoking cessation. The primary argument for the strict smoking policy is the significantly higher risk of postoperative complications (1–3). One patient canceled due to lack of smoking cessation was admitted with anastomotic leakage after surgery abroad, and it can only be speculated if it was caused by insufficient surgery or impaired healing because of smoking. The risk of complications must be set opposed to the necessity of the surgery; as bariatric surgery is a treatment of a benign condition among high-risk patients, preoperative optimization is essential for the postoperative result. An investigation of the association between smoking status and temperament characteristics showed that obese smokers had higher anxiety and lower control, whereas obese ex-smokers presented higher coping and control characteristics (5). This indicates that patients able to quit smoking could have better long-term outcomes due to increased compliance. In addition is the more general discussion whether a tax-financed healthcare system with limited resources should offer benign surgery under suboptimal conditions.
Patients whose surgeries were canceled due to smoking were terminated in the bariatric outpatient clinic. They had the possibility of undergoing self-paid surgery at a private hospital or being re-referred to our clinic after 1 year, if they still met the national criteria for bariatric surgery and stopped smoking. Postponing could lead to increased morbidity; a study investigating the impact on the healthcare system if bariatric surgery is delayed found delayed surgery more expensive and less effective, especially among patients with type 2 diabetes (6). There is also the possibility of patients undergoing surgery elsewhere under less strict conditions with a subsequent higher risk for severe complications. Thus, strict no-smoking policies have negative effects worth considering.
This study consists of a relatively small population, but with a clear outcome. Therefore, as smoking cessation was based on cotinine levels in urine, the results are considered to be convertible with larger populations.
The test we used declared high sensitivity and specificity. We believe the sensitivity to be sufficiently high, as eight out of nine patients afterward confessed to have smoked, and one patient claimed to have been heavily exposed to passive smoking. It is a potential limitation that nicotine replacement therapy or heavy exposure to passive smoking also test positive. Since smoking cessation is mandatory according to Danish guidelines, we wished to use the most reliable indicator for smoking cessation, and as shown in this study the cotinine testing was more reliable than self-reporting. Despite the possible limitations, measurement of cotinine in urine has obvious advantages, as the assessment is non-invasive, non-expensive, and results are available within few minutes.
However, it is challenging to find an appropriate time for testing. If performed too soon, there is a risk that patients start to smoke again. But if performed late—as on the day of surgery in this study—a cancelation could make it difficult to prepare another patient instead. Therefore, testing 1–2 days before surgery is considered optimal.
In Denmark, help for smoking cessation is primarily offered through the local municipality. Thus, we have now changed policy and require smoking cessation before referral for surgery. To develop the best possible policy, increased focus on help for smoking cessation, more knowledge regarding the risk for postoperative complications among bariatric patients, and data comparing smoking-related postoperative complications with the risk of worsening of obesity-related comorbidities are warranted.
In conclusion, despite extensive information regarding increased risk of postoperative complications following bariatric surgery when smoking, that smoking cessation was mandatory prior to surgery, and that the scheduled bariatric operation would be canceled in case of smoking, up to 50% of patients with a history of smoking still smoked on the day of surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.