
Abstract
Objectives:
Chronic pancreatitis produces disabling pain and loss of pancreatic endocrine/exocrine function. Almost half of the patients will need surgery during the course of the disease. Certain conditions, such as extrahepatic portal hypertension or cavernous transformation of the portal vein, can increase the risk of morbidity and mortality. These complications must be borne in mind in the design of the surgical treatment of chronic pancreatitis. This study is a systematic review on the coexistence of chronic pancreatitis and extrahepatic portal hypertension/cavernous transformation in patients undergoing pancreatic surgery.
Methods:
We conducted an unlimited search updated on 10 December 2017, which yielded 535 results. We selected 11 articles.
Results:
Main indication for surgery was intractable pain. Presence of extrahepatic portal hypertension and/or cavernous transformation increased intraoperative bleeding and general postoperative morbidity, though the increase in general morbidity was less when the different postoperative complications were analyzed individually. Case series showed a higher mortality in patients with extrahepatic portal hypertension.
Conclusion:
Little is known about the presence of extrahepatic portal hypertension in patients undergoing pancreatic surgery for chronic pancreatitis. More studies are needed in order to standardize criteria for vascular involvement in patients with chronic pancreatitis, in order to select the surgical technique and, if necessary, to establish contraindications, in this subgroup of patients.
Keywords
Introduction
Chronic pancreatitis (CP) is a pathological fibro-inflammatory syndrome that produces a progressive and permanent destruction of the pancreas in individuals with genetic, environmental, and/or other risk factors. Potential causes include toxic factors such as alcohol or smoking, metabolic abnormalities, idiopathic mechanisms, genetics, autoimmune responses, and obstructive mechanisms (1).
The destruction of pancreatic parenchyma results in disabling pain, loss of the endocrine and exocrine function of the pancreas, and other complications, such as bleeding, biliary obstruction, or venous thrombosis at the level of the splenomesenteric axis (2). The management of CP must address these three aspects. Therapeutic options include the use of analgesics, including opioids, endoscopic techniques, and/or surgery (2).
Almost half of the patients with CP require surgery during the course of the disease (2). Indications for surgery are intractable abdominal pain; suspicion of malignancy; or presence of local complications such as pseudocysts, bleeding, obstruction or stenosis of the pancreatic duct, duodenum, compression/obstruction of the portal vein, extrahepatic portal hypertension (EPH), pancreatic fistula, and pseudoaneurysms (2, 3, 4).
EPH is defined as extrahepatic hypertension of the portal venous system in the absence of liver cirrhosis (5). It is caused by thrombosis or compression of the splenomesentericoportal venous axis, which may affect the portal vein, splenic vein, or superior mesenteric vein, or all of them. When there is a complete obstruction of the mesentericoportal axis, a cavernous transformation (CvT) of the portal vein may develop (6). Between 5% and 10% of patients with CP present complication with EPH (7). The incidence of CvT is less well known: until 1990, only 26 cases had been reported (8).
Portal thrombosis and EPH are considered to be risk factors for pancreatic surgery in CP (7), but the evidence is limited.
We performed a systematic review of the literature on patients with CP and splenic-portal-thrombosis/EPH undergoing surgery for the treatment of CP, in order to determine the surgical risk based on morbidity and mortality after surgery.
Methods
Adhering to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (PRISMA12NL) (9), an unlimited systematic search was performed in PubMed and Cochrane Library for articles published up to 10 December 2017, including case reports.
The search was made using the following medical subject headings (MeSH) terms: ((pancreatitis, chronic) OR (pancreatitis surgery)) AND ((hypertension, portal) OR (portal vein) OR (venous thrombosis)), and the eligibility criterion was any type of article that included patients diagnosed with CP with EPH and/or vascular abnormalities who had undergone any type of pancreatic surgery for the treatment of their disease, including case reports.
Selected studies were evaluated. Patients were defined as those diagnosed of CP with EPH and/or associated vascular abnormalities, who underwent pancreatic surgery. The following data were included, if available: number of patients, age, sex, diagnostic criteria for EPH, vascular involvement, cause of surgery, type of surgery performed, surgical time, intraoperative blood transfusion, reoperations, morbidity, readmissions, and mortality.
The articles were included or rejected based on predefined criteria according to the information obtained from the title and summary, and in case of doubt, after reading the complete article. The references of the selected articles were also checked, and one article not included in the initial search was found.
The quality of the studies included was evaluated according to the evidence levels of the Oxford Center for Based Medicine (PRISMA13NL) (10) and using Manterola et al.’s (11) scale.
Results
Description of the Articles Included in the Study
The initial search yielded 535 articles, but only 11 (2.05%) met the inclusion criteria (Fig. 1).
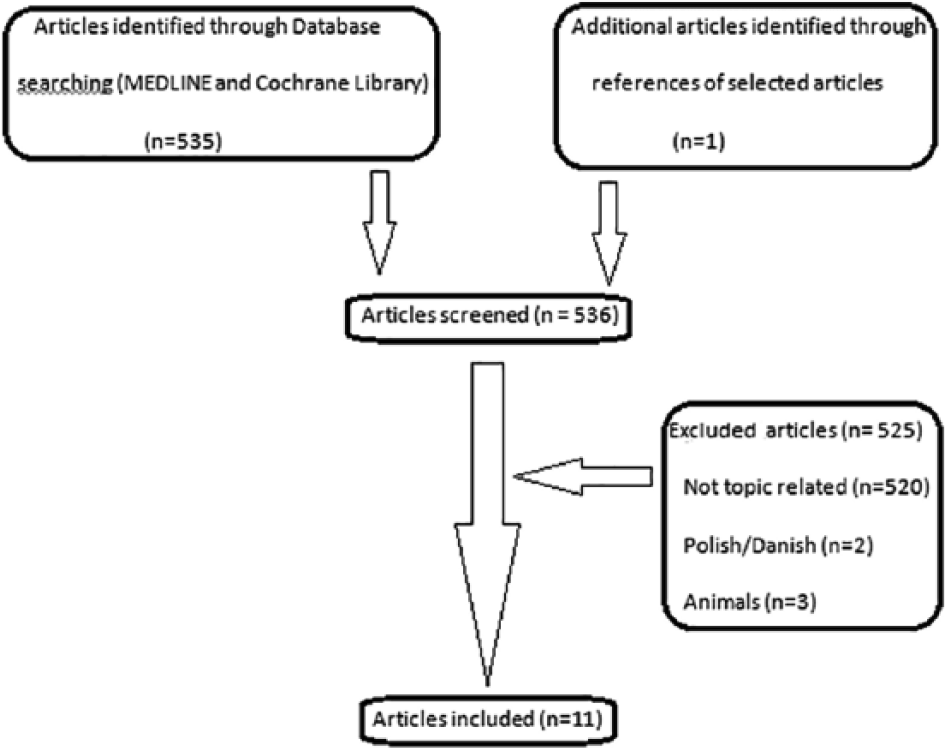
Flowchart.
In total, 10 of the articles included focused on patients with EPH and/or vascular abnormalities and CP who underwent pancreatic surgery. One of them specified the presence of CvT; another defined whether the venous involvement covered one or more branches and specifically separated these patients when describing the data. Another included 5 patients with cirrhosis among the 57 patients with EPH. The 11th article dealt exclusively with patients with CvT.
Regarding the type of study, two were case reports. Kayaalp et al. (2) described a patient with portal thrombosis without CvT, and Bail et al. (8) presented a case of CvT. The other nine articles were case series. Bockhorn et al. (6) (702 patients), Alexakis et al. (4) (112 patients), Adam et al. (7) (185 patients), and Izbicki et al. (12) (154 patients) compared groups of patients with or without vascular alterations in their series; another four articles included only patients with vascular alterations or EPH: Sakofaras et al. (13) (34 patients), Mariethoz et al. (14) (12 patients), Ramesh et al. (15) (57 patients, 5 with associated liver cirrhosis), and Bernades et al. (16) (266 patients, only 25 of whom underwent surgery); and the last one, Bloechle et al. (17) (30 patients), compared the performance of pancreatic resection or drainage in patients with and without EPH, evaluating the recovery of mesenteric venous flow in patients with and without EPH (Table 1).
Characteristic of the studies and clinical characteristic of patients and indications for surgery.
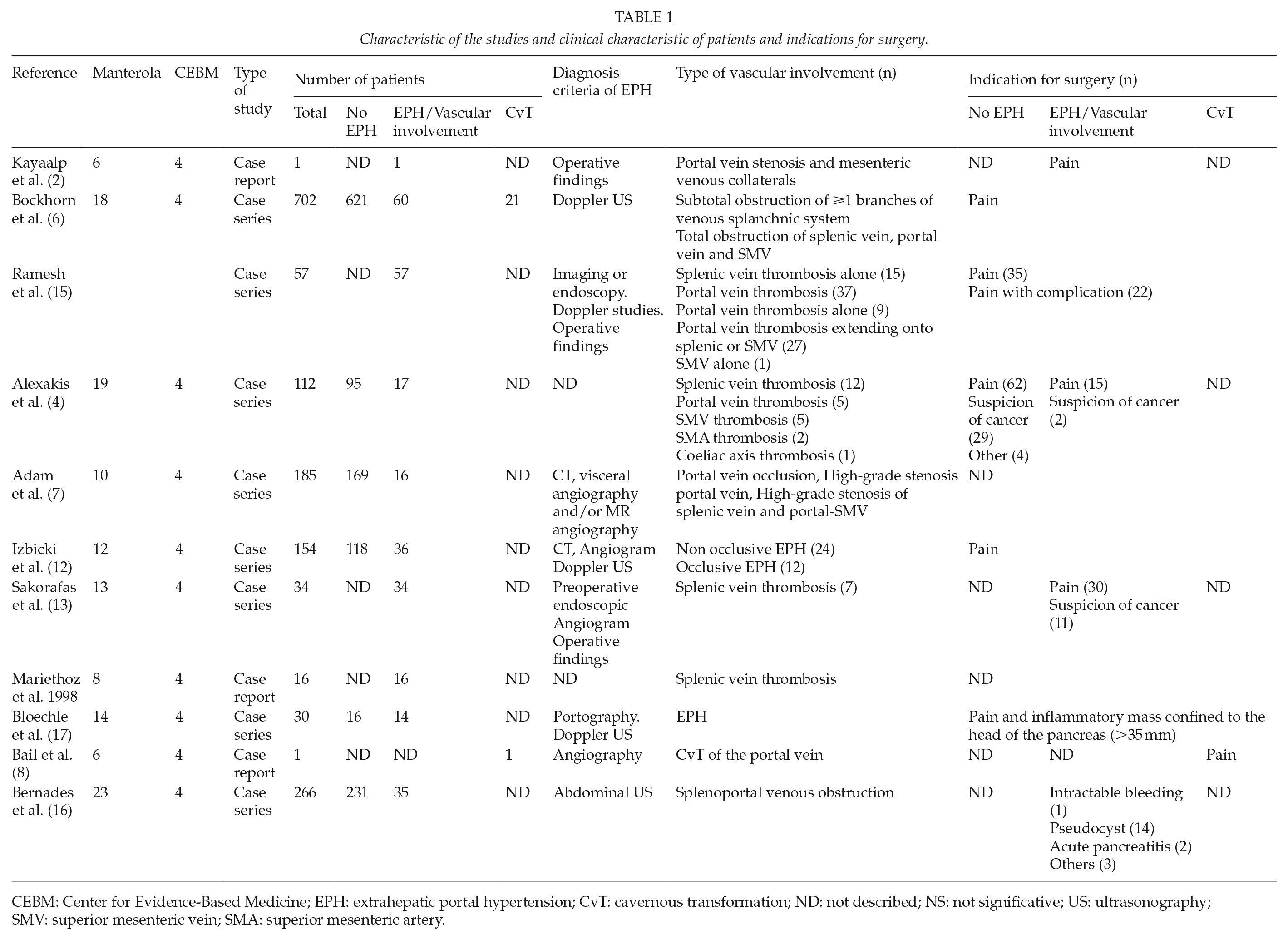
CEBM: Center for Evidence-Based Medicine; EPH: extrahepatic portal hypertension; CvT: cavernous transformation; ND: not described; NS: not significative; US: ultrasonography; SMV: superior mesenteric vein; SMA: superior mesenteric artery.
Evaluation of Study Quality
Study quality was assessed using the Manterola scale and the levels of evidence of the Oxford Center for Evidence-Based Medicine (CEMB). The range obtained on the Manterola scale was 6–23, with a median of 12.5 (Table 1) (11). Using levels of evidence, a score of four was obtained for all articles (Table 1) (10).
Analysis of Results
Patients were mostly male, in the fourth or fifth decade of life. The main cause of indication for surgery was intractable pain (Table 1) (2, 6, 15, 17).
Intraoperative bleeding, defined by the number of blood units transfused intraoperatively, was higher in patients with EPH (7, 12, 17) and was highest in those with CvT (6) (Table 2). Bernades et al. (16) reported a substantial intraoperative blood loss due to portal-systemic venous circulation in 8 of 26 operations in patients with splenic or mesenteric obstruction, and in four of six operations in patients with portal obstruction.
Type of surgery, intraoperative red blood cells, and hospital stays.
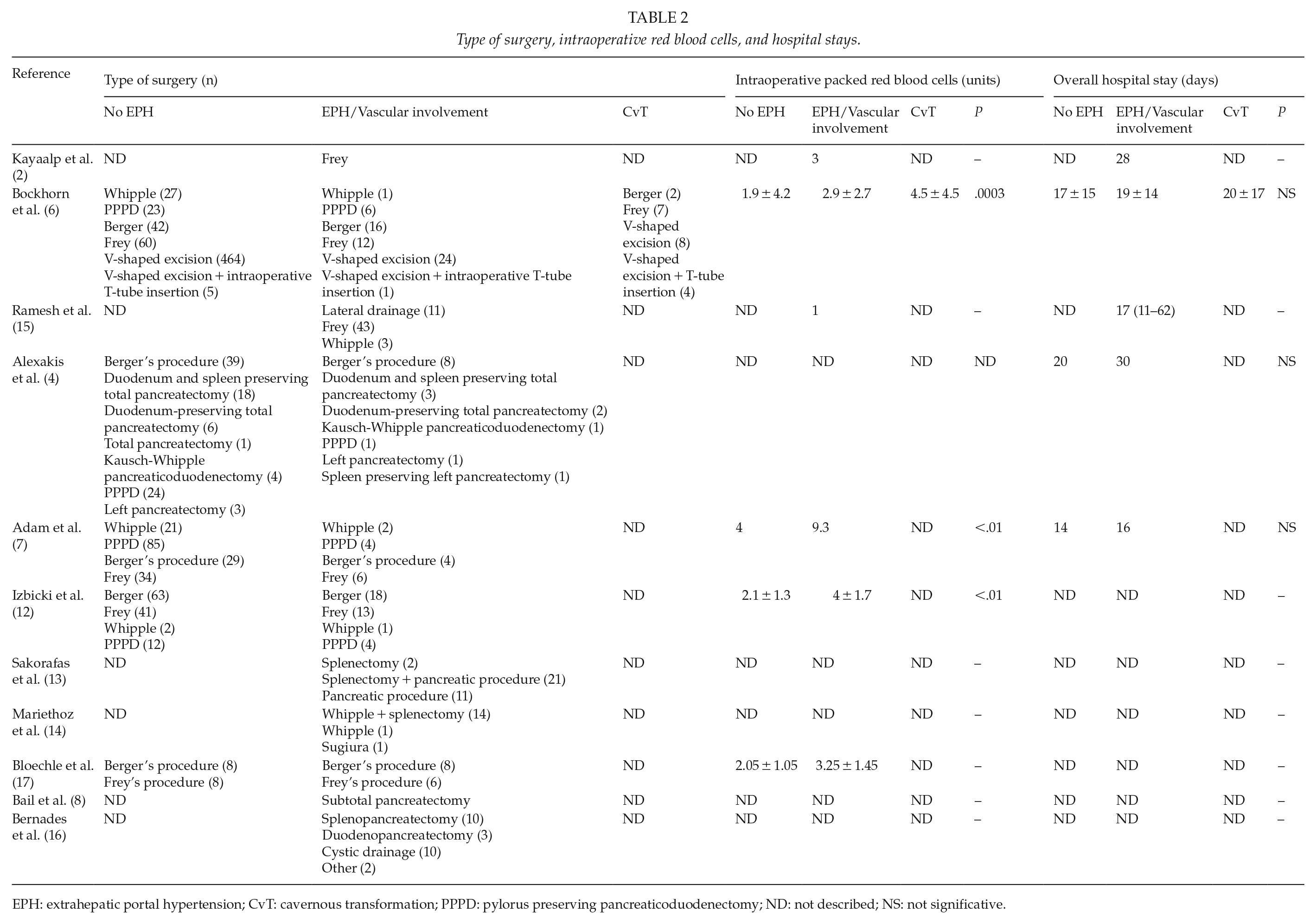
EPH: extrahepatic portal hypertension; CvT: cavernous transformation; PPPD: pylorus preserving pancreaticoduodenectomy; ND: not described; NS: not significative.
None of the series showed significant increases in overall hospital stay between patients with or without EPH. The mean stay was less than 20 days (6, 7, 12, 15) (Table 2). Case series studies described the type of surgery (Table 2), but none of them described the complications associated to them.
The presence of EPH and/or CvT caused an increase in general postoperative morbidity, which was statistically significant in the series presented by Alexakis et al. (4), Bockhorn et al. (6), and Izbicki et al. (12) (Table 3).
Morbidity and reoperation.
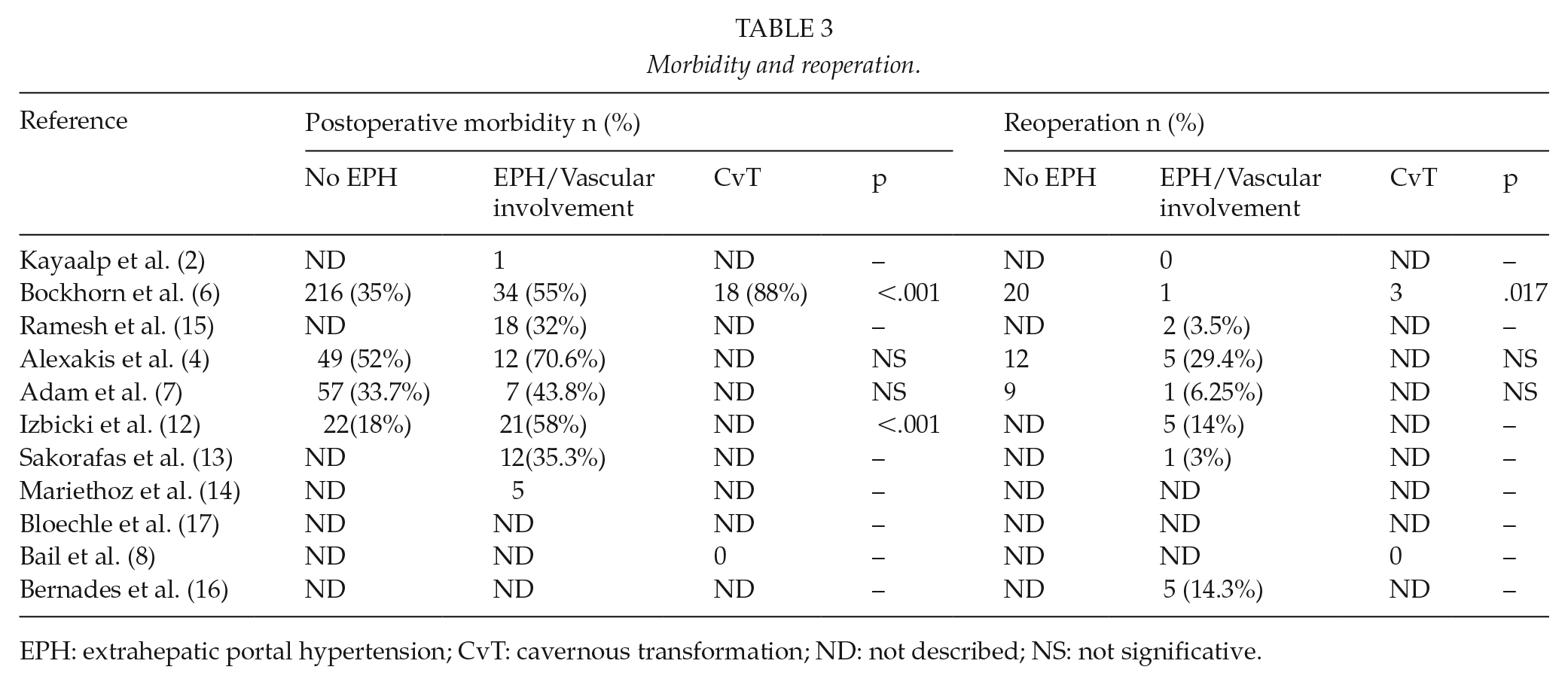
EPH: extrahepatic portal hypertension; CvT: cavernous transformation; ND: not described; NS: not significative.
Table 4 displays the postoperative complications of the articles and shows the statistically significant differences between each group of patients and each recorded complication.
Postoperative complications.
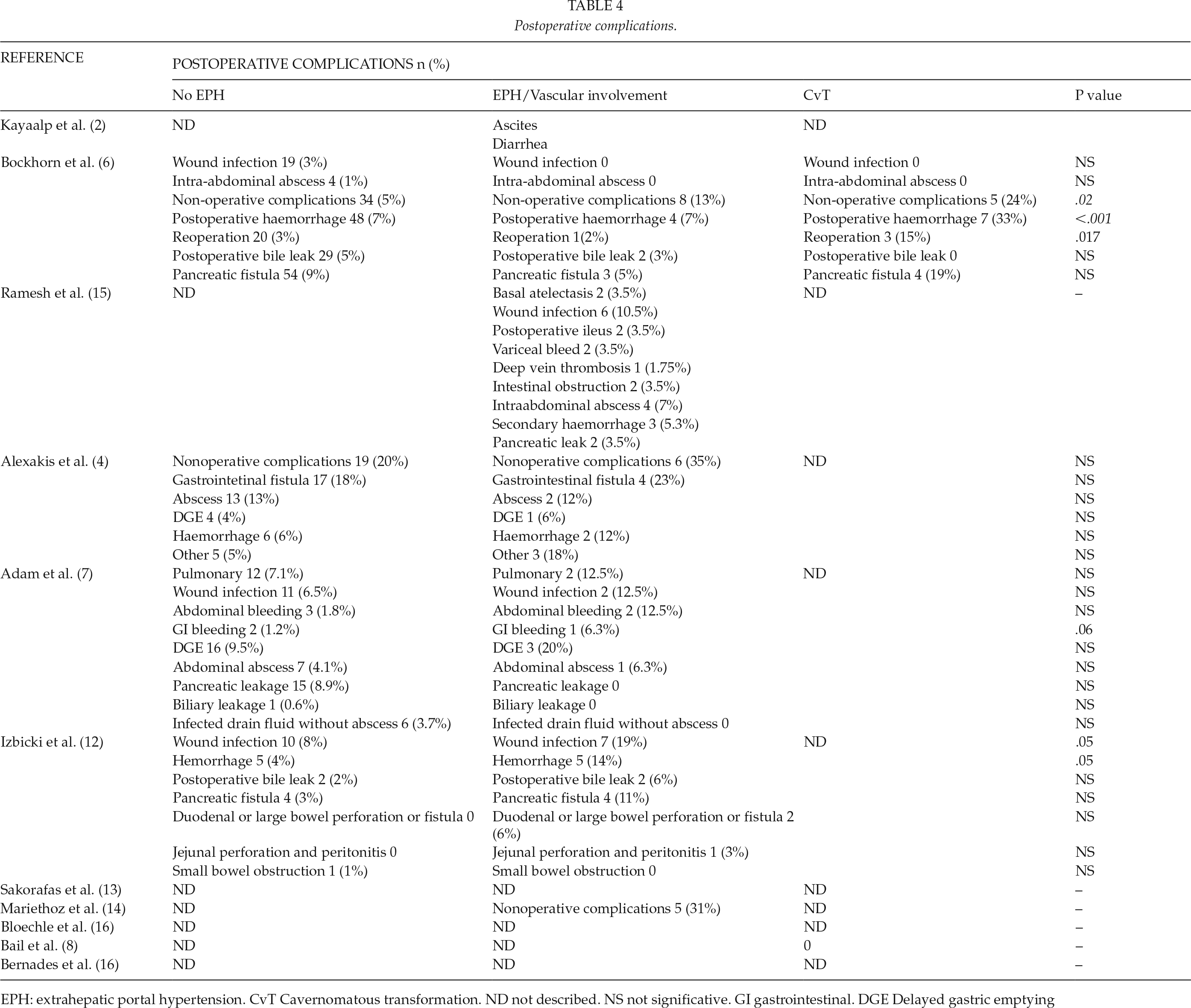
EPH: extrahepatic portal hypertension. CvT Cavernomatous transformation. ND not described. NS not significative. GI gastrointestinal. DGE Delayed gastric emptying
Mortality was zero in the two case reports included in our study (2, 8). However, the case series showed a higher mortality in patients with EPH, with the exception of Bloechle et al. (17). Alexakis et al. (4) concluded that the presence of vascular abnormalities should be considered a risk factor for mortality (OR: 9.96, p = 0.016). According to Bockhorn et al. (6), the increase in mortality was significant only in patients with CvT. Adam et al. (7) and Izbicki et al. (12) observed increased mortality in patients with EPH (6.3% versus 1.1% and 6% versus 0%, respectively), although this increase was not statistically significant. Ramesh et al. reported one death, in a patient with a Child B liver cirrhosis (Table 5).
Postoperative mortality.
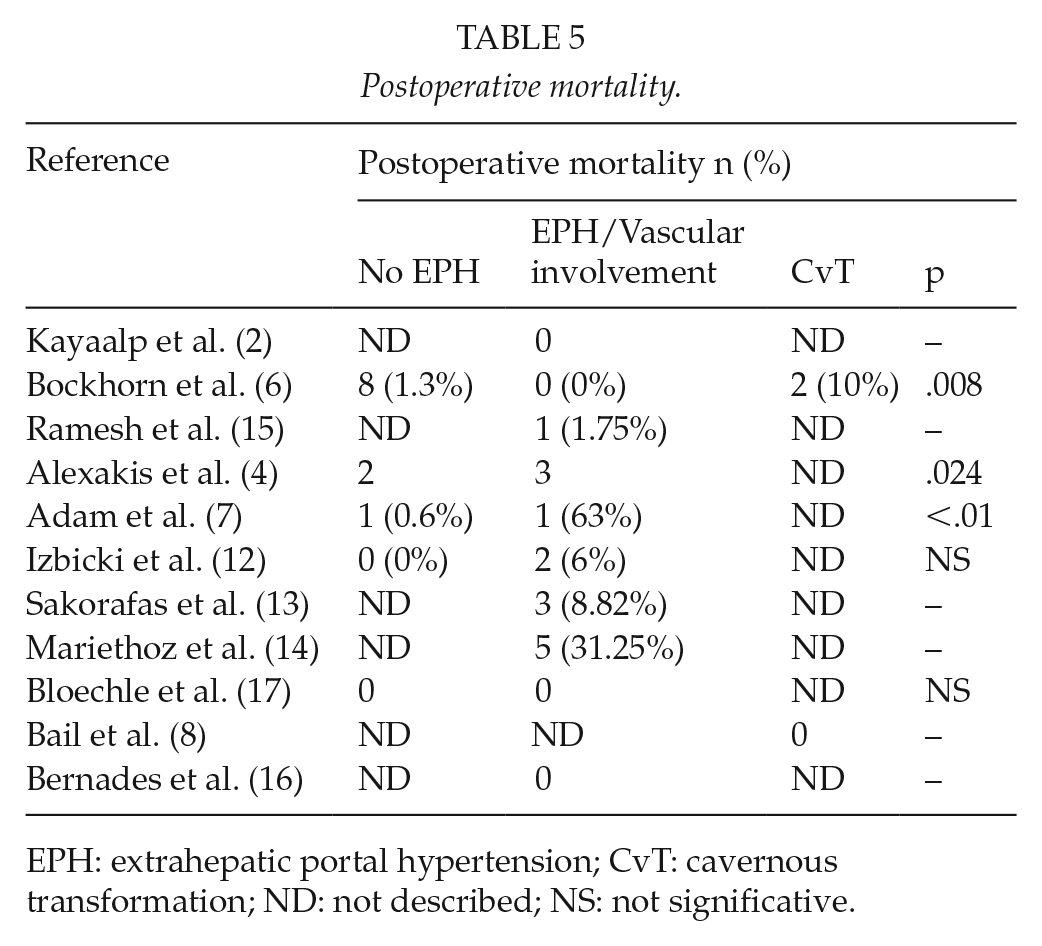
EPH: extrahepatic portal hypertension; CvT: cavernous transformation; ND: not described; NS: not significative.
Presence of EPH or CvT increased surgical time in all published series, with reports of increases of around 110 min. The increase was significant in the series published by Izbicki et al. (12) (p < 0.05), Adam et al. (7) (p < 0.01), and Bloechle et al. (17) (p < 0.05).
With regard to surgical results, all groups presented a significant improvement in terms of pain and time to return to work. During a mean follow-up of 32 months (range: 2–60), Bockhorn et al. (6) reported that 2 of the 21 patients in the CvT group died from causes unrelated to CP and 1 patient from the same group was reoperated after 12 months due to biliary stenosis. Two more patients in the EPH group died of non-surgical complications. Following up patients for a mean of 51 months (range: 36–66), Izbicki et al. (12) reported nine late deaths (death >1 year after surgery); the rate was around 6% in both groups, 7/109 in patients without EPH and 2/31 in patients with EPH. Pancreatitis relapsed in 21% (23/109) of patients without EPH and in 23% (7/31) of patients with EPH. In total, 70% of the no EPH group and 65% of the EPH group were able to return to work as usual. After a mean follow-up of 18 months (range: 3–61) in patients with EPH, Adam et al. (7) reported only one reoperation, for an incisional hernia. Alexakis et al. (4) performed a mean follow-up of 18 months (range: 3–60) in patients without vascular alterations, of whom 15 were readmitted and 3 died: one from variceal bleeding at 26 months, one due to general weakness despite all efforts to maintain calorie intake at 5 months, and the last one from hepatorenal failure due to chronic liver disease at 24 months. For patients with vascular complications of the disease, the median follow-up was 24 months (range: 3–48). One patient died 25 months after surgery with Berger’s technique due to hepatorenal failure after resuming alcohol consumption, and three patients were readmitted to hospital. In Ramesh et al. (15) study, follow-up ranged from 19 to 209 months (median: 106). Three patients died of intercurrent disease and three had esophageal variceal bleeding that was successfully managed by endoscopic therapy.
Discussion
Surgery in patients with CP is considered a valid treatment option and is especially effective for pain relief (6). EPH represents a major surgical risk, because it increases surgical time, blood loss, and postoperative complications. When surgery is indicated in a symptomatic patient, there is no absolute recommendation about which procedure should be performed (9).
The main indication of pancreatic surgery is the suspicion or presence of a neoplasia. Surgery for CP is less frequent, even though up to 50% of patients with CP may require surgery at some point during their illness due to the symptoms (essentially pain) or the onset of complications (2). Most patients who may require pancreatic surgery are middle-aged. In this situation, it would be very useful to identify risk factors that could allow us to make a preoperative selection, such as the presence of EPH (Fig. 2).
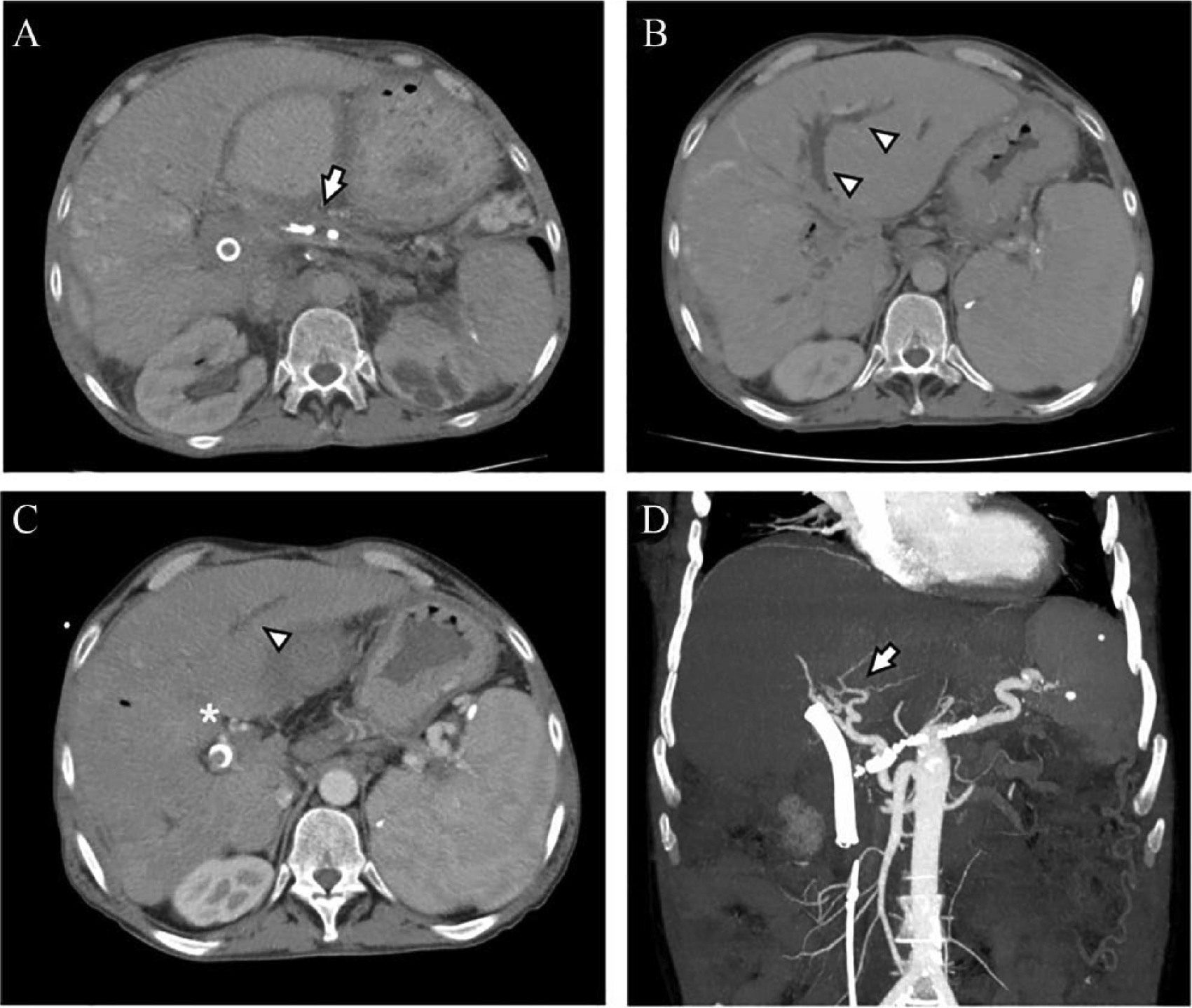
Contrast-enhanced MDCT (A) shows pancreatic atrophy with main pancreatic duct dilatation and intraductal calcifications due to chronic pancreatitis (arrow). Non-opacification of the portal vein and its branches was found (arrowheads in B and C) with multiple periportal vessels due to cavernous transformation (asterisk in C) and splenomegaly. Coronal MIP reconstruction (D) shows collateral circulation in the liver hilus (arrow).
A substantial body of literature on pancreatic surgery in patients with CP is available, with reports of good results in terms of pain reduction and improvement of disability. However, if we add the presence of EPH or CvT to the search, the data obtained are much more limited and level of evidence is low (6, 7, 9). In the series published by Bockhorn et al. (6), for instance, which included 702 patients with CP, only 13% (81/621) had EPH or CvT, and in the report by Bernades et al. (15), 266 patients with CP and EPH were followed up, but only 25 underwent surgery.
Few studies on pancreatic surgery in CP in patients with EPH or CvT are available, and the ones published to date vary widely in terms of methodology. For example, there is no widely applied definition of vascular involvement. Portal hypertension in CP may represent a spectrum of hemodynamic changes ranging from those with only Doppler ultrasound evidence of compromise to the portal circulation, to those with clear-cut varices, splenomegaly, and other collaterals (15). The lack of standardization of diagnosing vein involvement is a limitation to these revisions, and clear diagnosis criteria are needed in the future.
The case series published report an increase in surgical time, a greater need for intraoperative transfusion, and a higher rate of postoperative morbidity, with a trend toward higher mortality in this subgroup of patients. When morbidity is analyzed specifically, only Bockhorn et al. (6) and Izbicki et al. (12) reported statistically significant difference between postoperative hemorrhage in patients with and without EPH. Morbidity is recorded in many different ways, and none of the articles use any of the international classification systems to classify a complication in an objective and reproducible manner.
The same happens with type of surgery. Case series described the number of procedures that have been done for each group but do not specify the complications of the patients based on the surgery performed, so it is difficult to establish if there is a surgical technique that should be considered as the first choice in a patient with CP and EPH. The data on the surgical procedure are missing when referring to morbidity, and it should be addressed to be able to use the vein involvement as a potential contraindication to surgery. The studies included do not focus on the different surgical techniques being used in relation to morbidity, surgical time, or transfusions. They describe how many of the procedures are done, but do not present complications. All case series present pancreatic resections and pure decompression procedures, and none of them specify morbidity of each. Therefore, it would be necessary that more studies should specify what type of procedure has been carried out and the evolution.
The evidence available on the presence of EPH in patients undergoing pancreatic surgery for CP is limited. More studies are needed to standardize criteria on vascular involvement in patients with CP, in order to select an appropriate surgical technique or, if necessary, to establish contraindications in this subgroup of patients. The evaluation of morbidity should use international classification systems so that the results can be compared and reproduced, and a long-term follow-up is necessary in order to improve prognosis and assessment of post-surgical quality of life.
Conclusion
Little is known about the presence of EPH in patients undergoing pancreatic surgery for CP. More studies are needed in order to standardize criteria for vascular involvement in patients with CP, in order to select the surgical technique and, if necessary, to establish contraindications, in this subgroup of patients.
Footnotes
Author Contributions
R.A.L.F. and J.M.R.Á. contributed to study conception and design. R.A.L.F., A.M.V., and L.G.D.L.S. contributed to acquisition of data. R.A.L.F., A.M.V., and A.J.L.M. contributed to analysis and interpretation of data. R.A.L.F., A.M.V. and L.G.D.L.S. contributed to drafting of manuscript. R.d.L.P.L., and J.M.R.A. contributed to critical revision of manuscript and final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.