
Abstract
Background:
Studies comparing recovery of men and women after hip fracture have reported conflicting results, some reporting worse recovery in male patients, while others found no differences between genders.
Methods:
Recovery was compared in 105 male and 433 female patients with hip fractures and in age-matched groups of patients 50 years or older, who were home-dwelling and received similar rehabilitation. Residential status, walking ability, hip pain and activities of daily living function were recorded at admission and 4 and 12 months postoperatively, along with mortality and re-operations.
Results:
No differences were observed between men and women 4 and 12 months postoperatively regarding residential status (p = 0.181 vs p = 0.883), mortality rates (p = 0.232 vs p = 0.880) or total activities of daily living scores (p = 0.546 vs p = 0.435). Walking ability was better among male patients prefracture (p < 0.001) and 4 and 12 months after fracture (p < 0.001, p = 0.031, respectively). In age-matched pair analysis, no differences were found regarding mortality, residential status, walking ability, or ADL score. Cox regression analysis identified mortality risk factors as being age, prefracture ADL score, American Society of Anesthesiologists score 4–5 and place of rehabilitation. Sex was not mortality risk factor.
Interpretation:
Home-dwelling male and female patients had similar courses of recovery from hip fracture, although there were singular differences in specific activities of daily living functions and postoperative pain. There were no differences in mortality, even when prefracture characteristics were considered. Mortality was higher among older patients and who had high American Society of Anesthesiologists scores and low prefracture activities of daily living scores.
Introduction
Hip fractures are a considerable burden on the elderly population, causing significant morbidity and mortality (1). Home-dwelling patients with hip fractures form an important socioeconomic subgroup, which is the target of rehabilitation and other supportive measures aimed at maintaining their prefracture abilities and residential status (2). It is also important to study the characteristics and recovery courses of female and male patients in this subgroup, and how the two genders respond to supportive measures (3–5). Thus, determining factors that predict outcomes in these subgroups is of major importance.
Many hip fracture studies have focused on female patients since the majority of hip fractures occur in women (6–9). However, the number of hip fractures in men increased rapidly at the end of the 20th century (10), one reason being increased life expectancy of men (11), although overall hip fracture incidence in Finland has since leveled-off (12). Previous studies comparing men and women after hip fracture have reported conflicting results. Numerous studies report that men have higher postoperative mortality and more postoperative complications than women (3–5,9), but others have found increased mortality in women instead (13) or no gender differences at all when pre-operative health is considered (14,15). One study reported that men are more likely to require institutionalization and assistive devices for mobilization after hip fracture (16), while another found no differences in functional recovery (17). The methods used in the studies are quite variable, as are the follow-up times and inclusion criteria. This makes it difficult to compare different studies.
The aim of this study, which was based on data from a prospective, randomized, controlled trial, was to compare the recovery of home-dwelling male and female patients who had similar rehabilitations after hip fracture by assessing their functional and residential status and their mortality.
Materials and Methods
The study population consisted of 105 male and 433 female patients with non-pathological low-energy hip fracture who were treated surgically in Oulu university hospital between 1997 and 2000. The inclusion criteria for this study were age 50 years or older and the ability to live in one’s own home or in sheltered housing, which is comparable to a home of one’s own but is overseen by a supervisor and where some assistance is available. After the surgery, the patients were transferred to orthopedic ward where they were randomized (using opaque envelopes) to receive one of three types of rehabilitation: physically oriented (private rehabilitation unit; 41 male and 146 female patients), geriatrially oriented (public geriatric department; 30 male and 141 female) or healthcare center hospital rehabilitation (34 male and 146 female). We have reported in our previous article the outcome differences regarding different rehabilitation types (18). This analysis focuses on effects of gender on recovery using the same data.
The patients were assessed by a surgeon upon admission and by a study nurse who was involved in the research. A standardized form (Standardized Audit for Hip Fractures in Europe (SAHFE)) (19,20) was completed for each patient at admission. The forms recorded the following information: patient age, sex, place of residence, locomotor ability, use of walking aids, use of home help services, type of fracture, any pathological fractures, primary operation, activities of daily living (ADL) functioning, social status (19–21), associated diseases (cardiovascular diseases, paralysis, respiratory diseases, urological diseases, diabetes, rheumatism, Parkinson’s disease, malignancies, Paget’s disease, dizziness, use of corticosteroids) and American Society of Anesthesiologists (ASA) grade (22).
The 4- and 12-month follow-ups were performed using an inquiry form (19,20) that was completed by the patient and, if there were missing data, by the nurse via a telephone interview. The following information was recorded at 4 and 12 months postoperatively: the place of residence, locomotor ability, the use of walking aids, the patient’s own evaluation of his or her walking ability and hip pain, the use of home help services, and ADL functions. ADL functions (dressing, bathing or showering, eating, using the toilet, shopping, household chores, laundry, preparation of meals, banking/finances, use of transportation) were recorded and analyzed using a five-point scale classification according to Zuckerman et al. (20). The ADL score was calculated based on this classification so that each separate function was scored from 1 (best function) to 5 (worst function), and the total score was calculated by summing the scores for all ten ADL functions. The maximum score was 50 points. Mortality and re-operations (type and reason) up to 12 months postoperatively were recorded on a special form.
The study protocol was approved by the University’s Ethics Committee, and written informed consent was obtained from each patient prior to participation. This study is registered as a current controlled trial (registration number ISRCTN94467061).
Statistics
The statistical analysis was performed using SPSS for Windows version 20 (SPSS Inc., Chicago, IL, USA). The chi-square test was used to analyze the categorical variables, and the Kruskal–Wallis test and the Mann–Whitney U-test were used for continuous variables. In matched-pair analysis, McNemar test was used for dichotomic and Wilcoxon test for categorical or continuous variables. We considered p < 0.05 to be statistically significant. Because of significant age differences between genders, a separate matched-pair analysis was conducted. Pairs were formed manually (the outcome variables being hidden to the researcher) by pairing all 105 male patients with a female patient having the smallest age difference. Cox regression analysis was used to compare mortality between men and women after adjustment for explanatory variables in non-pair matched groups.
Results
Prefracture Characteristics
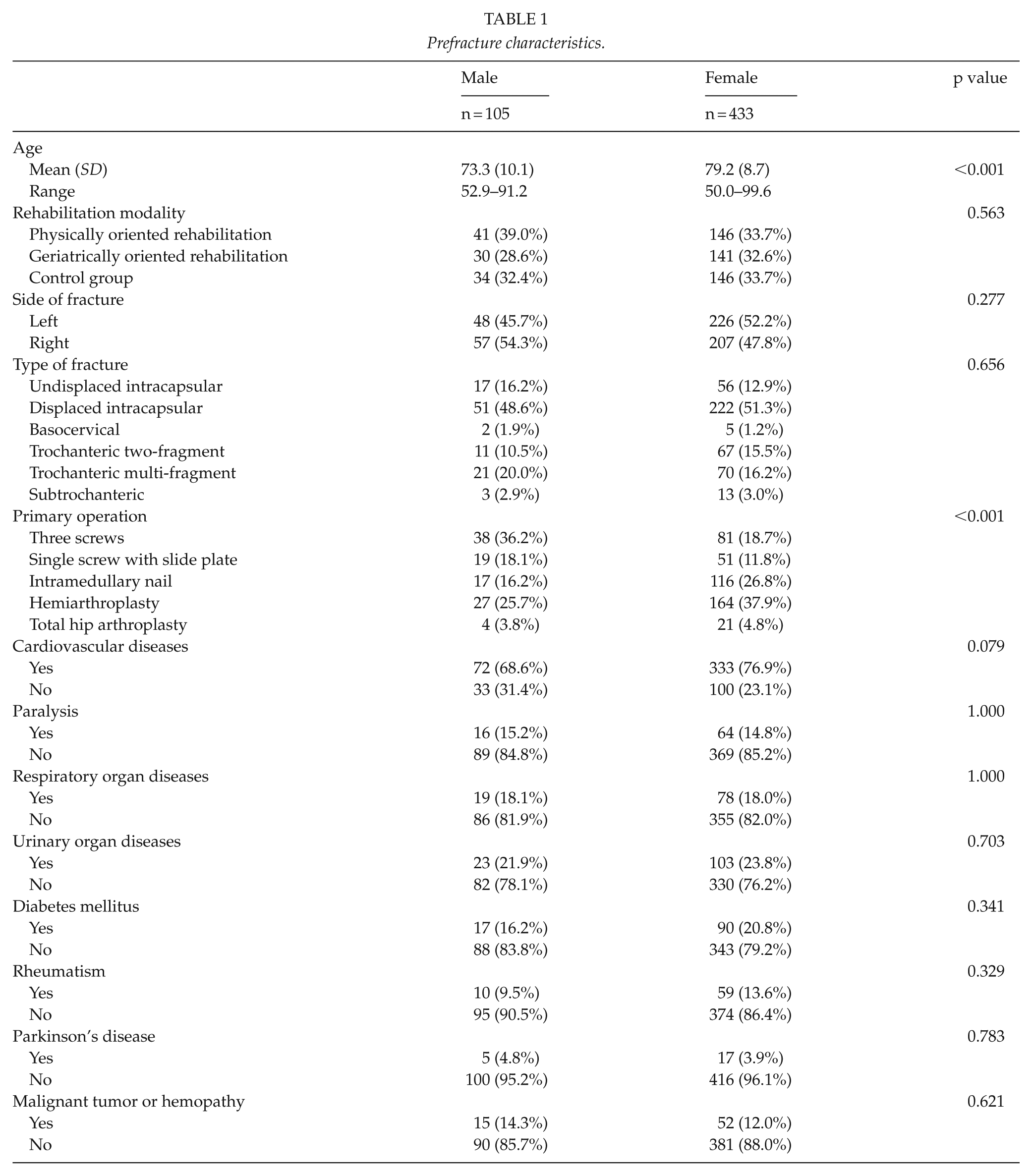
At the time of the hip fracture, the male patients (mean age, 73.3 years) were significantly younger than the female patients (mean 79.2 years, p < 0.001; Table 1). There were no differences between men and women regarding the distribution of different rehabilitation modalities (p = 0.563), fracture side (p = 0.277), type of fracture (p = 0.656), or associated diseases (Table 1). Men were more often treated with three screws or a single screw with a slide plate, while female patients had more operations with intramedullary nails and hemiarthroplasty (p < 0.001; Table 1). Male patients were more likely to have better prefracture walking ability than female patients (p < 0.001), and were more able to shop independently (p = 0.001), manage finances (p < 0.001), and travel independently before the fracture (p < 0.001; Tables 1 to 3). Female patients had better prefracture ADL scores for housework (p < 0.001) and for preparing meals (p = 0.035) than male patients (Table 3). No differences were observed regarding other ADL functions (Table 3). In matched-pair analysis, there were no significant differences in any prefracture parameters (Table 4). Three patients were lost in total after 4 months and before 12 months follow-up.
Prefracture characteristics.
Mortality, residential status, functional capacity and complication rate.
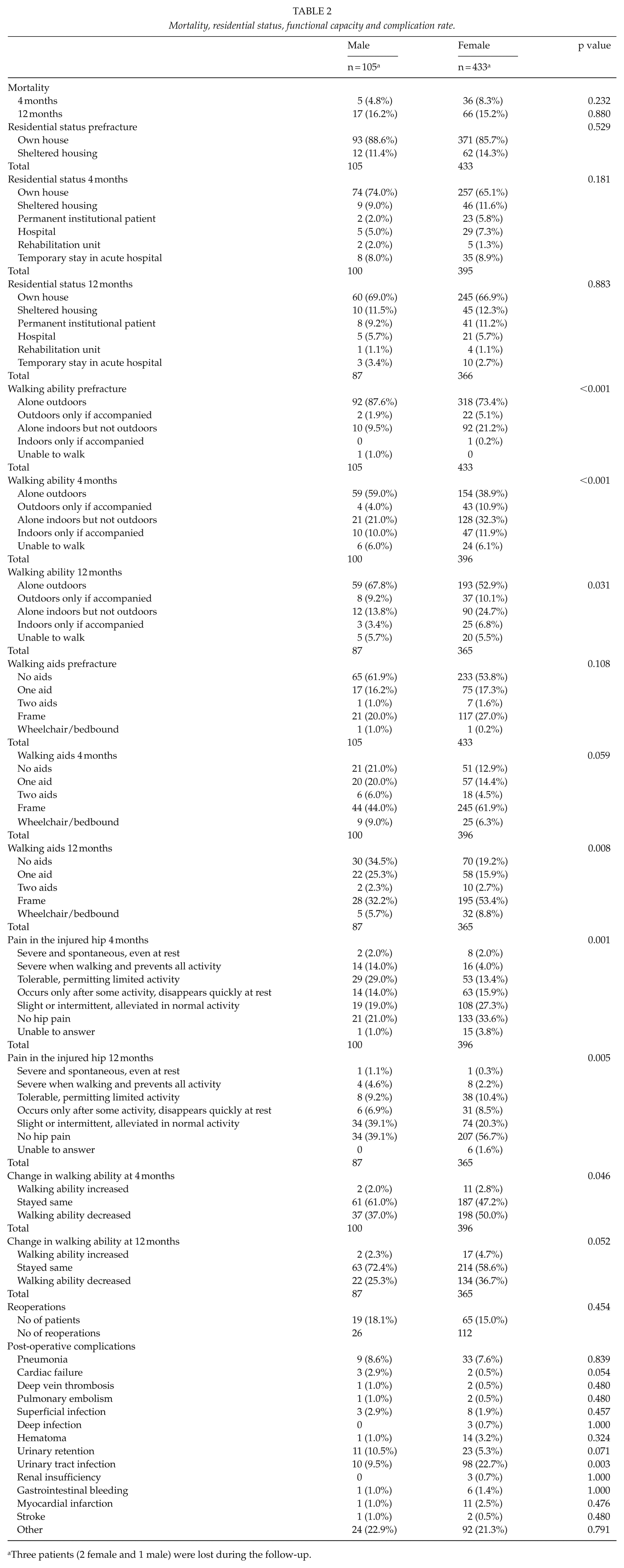
Three patients (2 female and 1 male) were lost during the follow-up.
Functions in activities of daily living.

ADL: activities of daily living.
Three patients (2 female and 1 male) were lost during the follow-up.
Age-matched pair analysis of 105 male and 105 female patients.
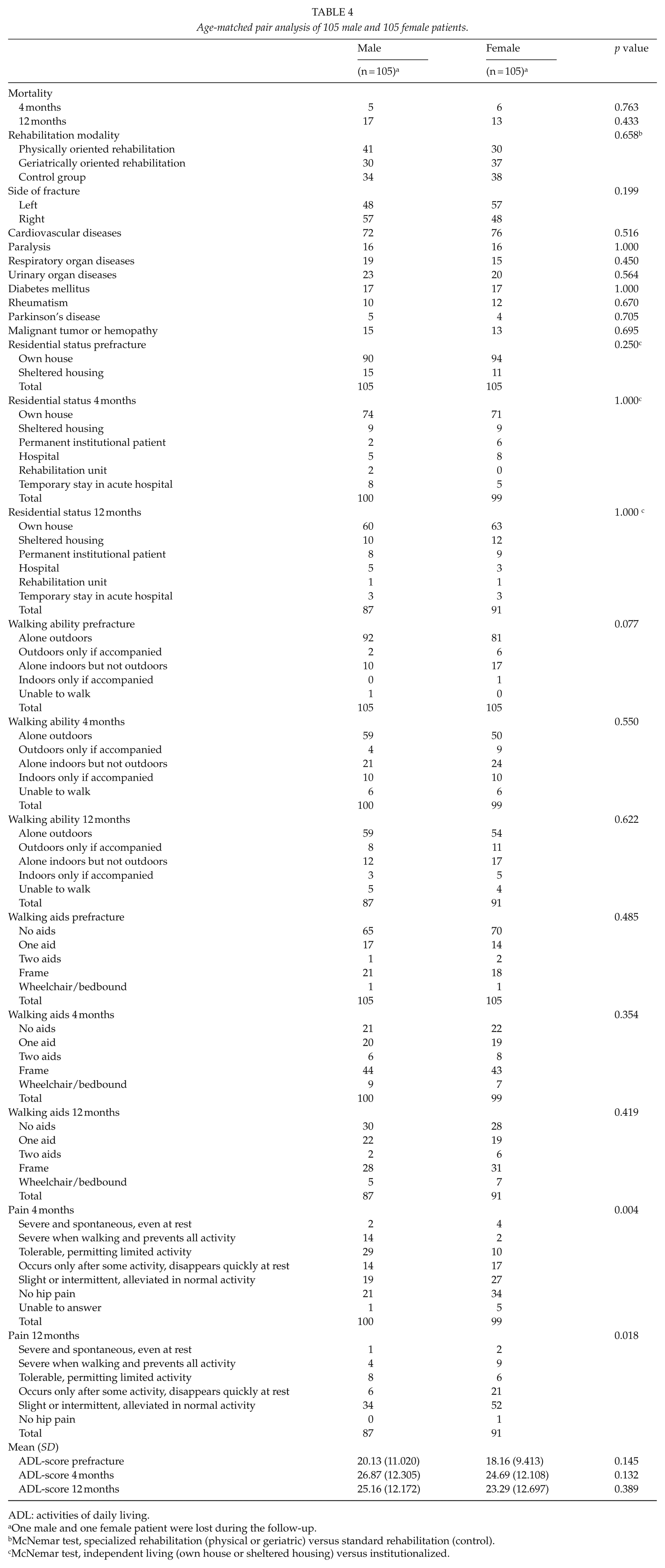
ADL: activities of daily living.
One male and one female patient were lost during the follow-up.
McNemar test, specialized rehabilitation (physical or geriatric) versus standard rehabilitation (control).
McNemar test, independent living (own house or sheltered housing) versus institutionalized.
mortality, Residential Status, Complication Rate, And Hip Pain 4 And 12 Months After The Fracture
No differences were found between the groups in terms of mortality (p = 0.232 and p = 0.880 at 4 and 12 months, respectively) or residential status (p = 0.181 vs p = 0.883; Table 2). There were no differences in post-operative complications between males and females except for urinary tract infections, which were more common in female patients (p = 0.003; Table 2). Pain in the injured hip was less common among female than male patients at the 4- and 12-month follow-ups (p = 0.001 and p = 0.005, respectively; Table 2). An analysis of matched pairs showed significant differences in postoperative pain at 4 and at 12 months in favor of female patients (p = 0.004 vs p = 0.018), but no gender differences were found regarding mortality (p = 0.763 vs p = 0.433) or residential status (p = 1.000 vs p = 1.000; Table 4).
Walking Ability
Male patients had better walking ability both 4 (p < 0.001) and 12 (p = 0.031) months after the fracture, and they needed fewer walking aids at 12 months (p = 0.008) than their female counterparts (Table 2). Women showed worse walking ability at 4 months (p = 0.046; Table 2) and at 12 months (p = 0.052; Table 2) compared to their prefracture status. In a separate analysis of matched-pairs, no differences in walking ability were observed prefracture (p = 0.077) or at 4 (p = 0.550) and 12 (p = 0.622) months after the fracture. The matched-pair analysis showed no differences regarding the use of walking aids (Table 4).
Cox Regression Analysis
A Cox regression analysis (Table 5) of survival 12 months after the fracture showed that the following significantly increased the risk of death: age (hazard ratio (HR): 1.028, 95% confidence interval (CI): 1.001–1.059), prefracture ADL score (HR: 1.047, 95% CI: 1.020–1.074), ASA score 4–5 compared to ASA score 1–3 (HR: 1.880, 95% CI: 1.135–3.113), and physical rehabilitation compared to geriatric (HR: 2.019, 95% CI: 1.092–3.733) and standard rehabilitation (HR 2.151, 95% CI 1.167–3.965). Sex (p = 0.236), type of fracture (p = 0.559), prefracture walking ability (p = 0.068), living alone (p = 0.321), and cardiovascular disease (p = 0.629) were factors that did not affect the mortality rate.
Cox regression analysis on survival for 12 months after the fracture.
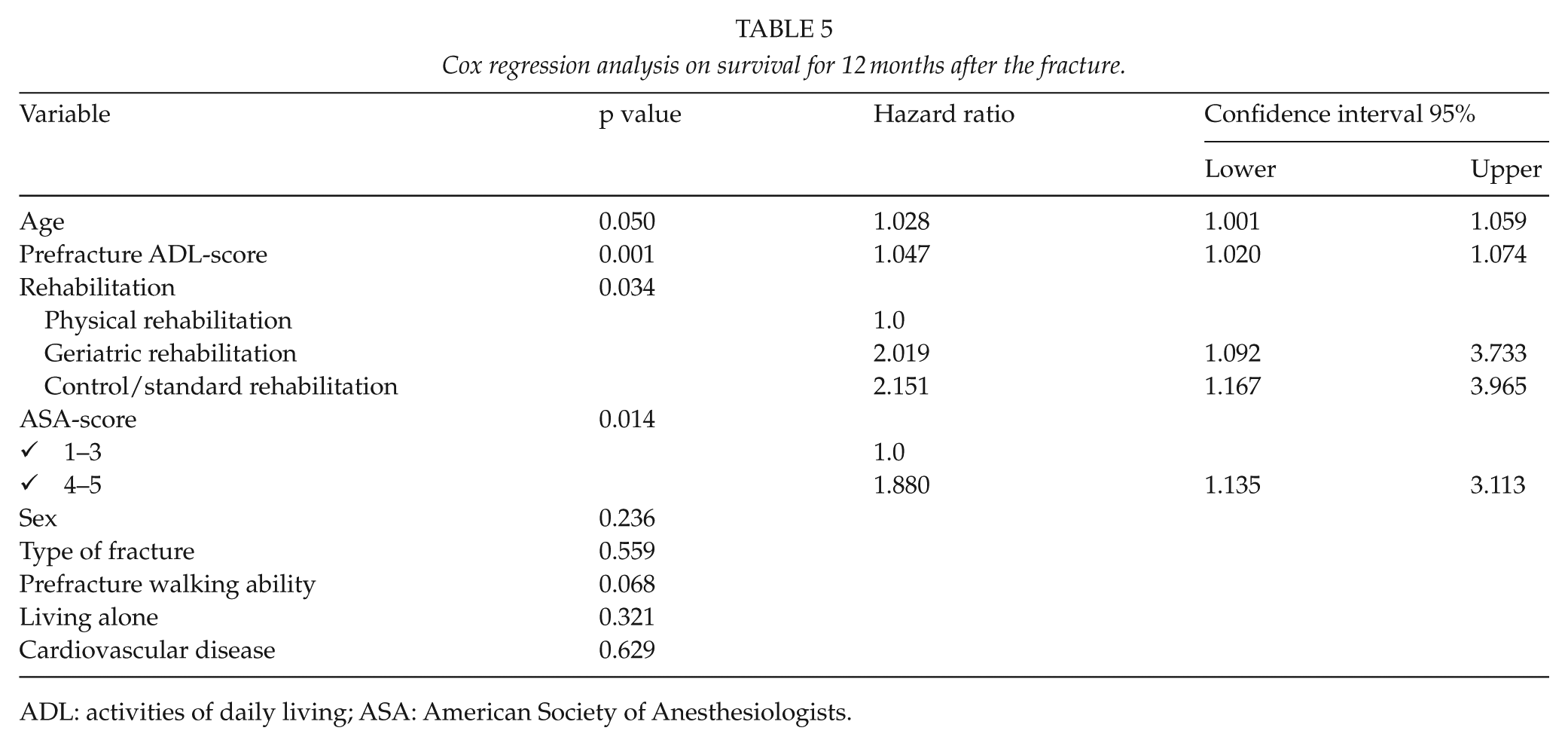
ADL: activities of daily living; ASA: American Society of Anesthesiologists.
Adl Functions
Male patients were more able to shop independently at 4 (p < 0.001) and 12 (p = 0.013) months, use transportation at 4 (p < 0.001) and 12 (p = 0.038) months, and manage banking/finances 4 months (p = 0.010) after the fracture (Table 3). Female patients were more able to prepare meals independently at 4 (p = 0.021) and 12 (p = 0.002) months, do household chores at 4 (p = 0.030) and 12 (p = 0.016) months, and to do laundry at 12 months (p = 0.029). No other significant differences were observed in ADL functions. There were no significant differences in the total ADL scores between men and women at 4 (p = 0.546) and 12 (p = 0.435) months. The detailed results are shown in Table 3. The matched-pair analysis did not show significant differences in total ADL-scores (Table 4).
Recovery In Specific Rehabilitation Settings
We compared male and female patients in each rehabilitation setting (detailed data are available upon request). There were no differences in mortality between men and women in the physical rehabilitation (p = 0.34 and p = 0.755 at 4 and 12 months, respectively), geriatric rehabilitation (p = 0.741 vs p = 0.456), or healthcare center hospital settings (p = 1.000 vs p = 0.355). Similarly, we found no differences in the ADL scores at the 4- and 12-month follow-ups in physical rehabilitation (p = 0.757 vs p = 0.639), geriatric rehabilitation (p = 0.436 vs p = 0.920), and healthcare center hospital settings (p = 0.213 vs p = 0.523).
Discussion
In our prospective study, we found that preoperative health factors including ADL function, ASA-score, age and place of rehabilitation predicted mortality during the year-long follow-up after the fracture, rather than sex which seemed to have no effect on risk of death. Also, our results had no major differences regarding functional recovery between men and women, although minor differences in specific daily functions were observed.
We found no difference in mortality between home-dwelling male and female patients with hip fracture during the 12-month post-fracture follow-up period. This finding differs from many earlier studies that found that male patients have a higher mortality risk after hip fracture than female patients (3–5,9,17). However, one previous study (23) found no difference in mortality and an earlier Finnish study reported higher mortality among female patients (13). Notably, only a few of these studies focused on home-dwelling patients (3–5) as in our study. In these three studies, the statistical methods differed from our direct comparison between male and female sex as they take into account other factors that affect mortality using either regression analysis or generalized estimating equations. This makes it difficult to compare them to our study. The patients were also generally older in these earlier studies, i.e., 60 years old (3) or 65 years old (4,5) or older.
Because of the difference in age between the men and women in this study, we also conducted a Cox regression analysis on survival and found that age, ASA score, and prefracture ADL score were independent risk factors for mortality. Sex alone did not predict mortality. Previous studies reported that the prefracture risk factors for post-fracture mortality include comorbidities (4), ASA score (4,24), and age (4); our findings are consistent with most of these studies. Men have often been reported to have a higher ASA rating or preoperative risk, suggesting that they have more severe medical comorbidities at the time of surgery than women (25,26). Men have also been reported to have a higher risk of postoperative complications (4). Myers et al. (27) found that men were 10 times more likely to develop pneumonia than women. Some studies have reported that male sex is an independent risk factor for mortality after surgery for hip fracture in home-dwelling patients (3–5). Endo et al. (4) conducted a study of 983 independently living patients with hip fracture after one year of follow-up and reported an increased risk of death among men after considering age, ASA rating, comorbidities, and postoperative complications. Similarly, Fransen et al. (3) studied patients aged 65 years or older and concluded that male sex was a risk factor for mortality after considering baseline characteristics. These authors noted that the mostly two-level measurement of prefracture health status (diseases and function often reported as yes–no answers instead of larger rating scale) may have overestimated the effect of male gender on mortality. Hawkes et al. (5) also found higher mortality in previously community-dwelling, male patients one year post-fracture. Our Cox regression analysis results suggested the opposite, indicating that other pre-existing factors explain the gender differences rather than gender itself, a view that has been proposed by some earlier studies (14,15). The reasons underlying the conflicting results remain unclear, but they may be related to the use of different covariates in the analyses as well as differences in inclusion criteria or differences in postoperative rehabilitation that were not controlled for in the analysis.
Men and women showed some differences in functional recovery for specific functions, although generally no major differences were observed. Male patients had better outcomes for mobility-requiring tasks, while female patients had better results for housework-related tasks. Quite often, the differences were present before the fracture. It seems likely that these differences in specific ADL functions may be due to conformity to traditional gender roles that are imposed by society rather than to better physical function per se. Men seemed to have significantly better walking ability than women, even before the fracture, but the differences disappeared when female and male patients were age-matched. Female patients consistently reported less postoperative pain, in both age-matched and non age-matched analyses. Our findings are in line with numerous earlier studies that found no significant differences in functional recovery between men and women (4,5,17,23,28). At least one study found that female gender was a risk factor for lower functional recovery after hip fracture (29). It has been suggested that patients who survive the initial post-fracture period are similar in terms of the factors that influence functional status in the later post-fracture period (17).
We observed no differences in residential status between men and women after the fracture. After 12 months, approximately 80% of both male and female patients were able to live independently or in sheltered housing that was comparable to living at home. Age-matching the patients did not change the results. The ability to live independently requires a certain level of mobility and function, which explains the similar results in both residential status as well as mobility and ADL function. It was reported previously that hip fracture significantly increases the risk of being institutionalized regardless of gender (3), with age, low level of mobility, and dementia identified as known risk factors for institutionalization (2). While some studies have reported a higher risk of institutionalization in men (3,16), others found no difference between men and women (2,28). A study by Holt et al. conducted in Scotland found that men and women were similar in their ability to return home at a 120-day follow-up, but they also found that men had a greater risk of institutionalization when the prefracture characteristics were considered. We did not consider prefracture characteristics in our direct chi-square tests, making it hard to compare their study with ours. In addition, in the Scottish study only two-thirds of the patients were living at home prior to their hip fracture. Vochteloo et al. (2) studied the risk factors for failure to return to the prefracture place of residence and found that female sex was associated with a higher risk at discharge, but that there were no differences between men and women 3 and 12 months later. However, the authors noted that the data involving residential status were greatly limited (66 patients at the 12-month follow-up). Fransen et al. (3) compared previously community-dwelling patients with hip fracture to randomly selected controls and found that hip fracture increased the risk of institutionalization and mortality in both men and women, but the effect was markedly greater in men. However, the study used institutionalization and mortality rate as a single variable, so it may not be comparable to other studies. In general, it is difficult to compare studies in this field in terms of determining the risk of institutionalization because there is great variation regarding the methods that are used and in the study populations.
The major strength of our study was its clear, structured design, which allowed us to identify even small changes in health and functional status during the 12-month follow-up period. The study population was sufficiently large, and only 3 patients were lost during follow-up. The rehabilitation settings in our study were well-defined and were similar for men and women, allowing us to consider the effect of the rehabilitation setting when evaluating the results. This study was based on a secondary analysis of data that were used in earlier report (18) where we found that specialized physically oriented rehabilitation resulted in lower mortality and better short-term ability to live independently. To ensure that different rehabilitation modalities would not affect the results, we verified that the distribution of male and female patients was the same in different rehabilitation groups and also considered the rehabilitation modality as an explanatory variable in our Cox regression analysis. We also compared men and women in three specific rehabilitation settings and found no major differences. One limitation of our study is that there were more women than men—a common result in hip fracture studies because the majority of hip fractures are in women. Our study population had significantly larger female population (4.1 to 1 female-male ratio) compared to some newer studies (1,12), which may be caused by an epidemiological trend of decrease of hip fracture incidence among women (12). The men were also significantly younger than the female patients, which may have served as a confounding factor. However, this was considered in our matched-pair analysis. It should also be noted that our results for these home-dwelling patients may not be generalizable to patients in institutions.
Our results show that home-dwelling men and women (50 years or older) with a low-energy hip fracture have a similar risk of mortality, institutionalization, and functional decline after hip fracture. Differences in walking ability between the genders were seen, although this was age-dependent since the differences disappeared after age-matching. Female patients reported significantly less post-operative pain than male patients. High ASA score, age, and low prefracture functional status predicted mortality. More attention should be directed toward patients with these attributes in order to minimize poor treatment outcomes.
Footnotes
Acknowledgements
We thank Eila Haapakoski and Tuula Rauma for technical assistance.
Author’s Note
This study is registered as a current controlled trial (ISRCTN94467061)
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the Finnish Office for Health Technology Assessment (Finohta), a public assessment agency working as a part of National Institute for Health and Welfare. The authors declared no conflict of interest.