
Abstract
Background & Aims:
The prevalence of gallstone disease increases with age, being early cholecystectomy the most accepted treatment in the vast majority of patients in order to prevent complications and recurrence. The aim of this study is to determine the recurrence rate and its possible predictors after initial non-operative management.
Materials and Methods:
We reviewed a consecutive series of patients, older than 65 years, admitted for a gallstone-related disease and treated with a non-operative management between January 2010 and December 2013. We analyzed comorbidities, clinical data, diagnosis, management, recurrence, and its treatment. Median follow-up after the discharge was 2 years. Recurrence was analyzed by a Kaplan–Meier survival curve. Possible recurrence’s predictors were analyzed.
Results:
The study included 226 patients. Mean age was 80.4 ± 7.2 years, 127 (56%) were female. The main causes of index hospitalization were acute cholecystitis (58%) and biliary pancreatitis (18.1%). After 2 years of follow-up, the recurrence rate was 39.8%; mean time to recurrence was 255.2 ± 42.1 days, 81% of patients recurred within 1 year. Bile duct disease implied a higher recurrence rate than the gallbladder disease group (52% vs 33%, p < 0.001). Subjects with two or more diagnoses during index admission presented higher recurrence rate (32% vs 49%, p < 0.001).
Conclusion:
More than a third of elderly patients could present a recurrence within 2 years after initial non-operative management. Early cholecystectomy should be considered at index admission in order to prevent recurrence.
Introduction
Gallstone disease is a very common condition in the general population. Prevalence of gallstones increases with age, from 8% in people younger than 40 years old to more than 50% in people older than 70 (1). In this last group, the incidence of symptomatic gallstone disease is around 30%, representing the most common cause of acute abdominal pain in elderly population (1, 2). Elderly patients have been found to have higher risk of developing gallstone-related complications (3–6). Furthermore, early recurrence of symptomatic disease in elderly population has been estimated around a third of patients on follow-up (5, 7–9), being these episodes related with increasing morbidity rates for each new episode (5, 7, 10).
Current guidelines recommend early cholecystectomy (EC) in order to prevent gallstone-related complications and recurrence in the absence of contraindication for the surgical procedure (11–13). Although cholecystectomy has been described to be effective and safe for elderly patients (14–18), the treatment of symptomatic cholelithiasis with EC still remains a debatable issue. Elderly patients are less likely to undergo a surgical treatment, due to patient’s preference, surgeon reticence, and related comorbidities (9). Finally, they present a higher risk of surgery-related complications with an increase in morbidity, mortality, costs, and recurrence rate (RR) (7, 9, 10).
The aim of this study is to analyze the results of non-operative management (NOM) of symptomatic gallstone disease in the elderly patients determining gallstone-related diseases RR. Furthermore, we evaluated predictors of recurrence in our series.
Material and Methods
Patients and Characteristics
Single-institution retrospective study of a consecutive series of patients, older than 65 years old, with gallstone-related disease (including biliary colic, acute calculous cholecystitis (ACC), cholangitis, choledocholithiasis, and biliary pancreatitis), requiring hospitalization, treated with NOM between January 2010 and December 2013. An abdominal ultrasound (US) was routinely performed in order to confirm the gallstone-related symptoms. If there were doubts regarding possible presence of choledocholithiasis, based on biochemical data, a magnetic resonance cholangiopancreatography (MRCP) was additionally performed during the admission. Exclusion criteria were (1) biliary disease without a gallstone etiology, biliary malignancy, or pancreatitis not related to a gallstone disease, (2) patients with surgical management at initial hospitalization (H1), (3) patients who died during H1 and (4) patients without an adequate follow-up.
Protocols in our center included surgical indications according to the guidelines regarding the years of the study (11, 19). Patients with biliary colic alone were admitted if the episode was refractory to analgesia, and EC was performed within the first 24 h during admission. In the case of acute cholangitis, EC was performed in selected cases once the patient’s general condition improved. For ACC, EC was performed based on severity grade, performance status, and time from onset of symptoms, preferably within the first 72 h, according to Tokyo Guidelines (11, 19).
This study was approved by our local Research Ethics Board.
Our database included the following variables: age (being patients classified in two groups: from 65 to 80 years or older than 80), gender, Elixhauser comorbidity index (20), symptoms at H1 (including nausea or vomit, abdominal pain, body temperature measured over 38°C as fever, or neurological symptoms), biochemical data, US findings at initial emergency department (ED) admission (including the presence of pericholecystic fluid, gallbladder wall thickening, perforation of gallbladder wall, gallbladder distension, Murphy’s sign, common bile duct (CBD) dilatation), diagnosis, and management (including therapeutic interventions as endoscopic retrograde cholangiopancreatography (ERCP), or percutaneous cholecystostomy). A same-admission cholecystectomy was defined as EC, and elective cholecystectomy performed after discharge defined as delayed cholecystectomy (DC).
In addition, we grouped initial diagnosis as gallbladder disease (biliary colic, ACC) and bile duct (BD) disease (cholangitis, choledocholithiasis, and biliary pancreatitis).
The median follow-up was 2 years after discharge, and data concerning recurrence and subsequent treatment were recorded.
Study Outcomes
Primary outcome was to analyze RR and mean time to recurrence. Recurrence was considered as any visit to the ED (including patients with and without hospitalization) due to relapse of symptomatic gallstone-related disease after discharge.
Secondary outcomes were number of recurrent episodes, management for new episodes (including rates of cholecystectomy after H1), and possible predictors of recurrence after initial NOM.
Statistical Analysis
Baseline characteristics at H1 were described and stratified into two groups: recurrence and no recurrence. Study outcomes at follow-up were summarized depending on recurrence.
All statistical analyses were performed using SPSS® 23.0 for Windows (SPSS Inc, Chicago, Illinois, USA). Descriptive values are expressed as percentage or mean ± standard deviation (SD) and median with interquartile range. The chi-square test or Fisher’s exact test was used for comparison of categorical variables, and Student’s t-test was used for continuous variables. A survival analysis was performed, and Kaplan-Meier survival curve for time to recurrence was created. Patients were followed during a 2-year period and were censored at the time of surgery, or if no recurrence occurred by this period.
The statistical significance of the differences for Kaplan–Meier survival curve was assessed by log-rank test. The differences were considered significant at p value of <0.05.
Results
At H1, 131 patients had ACC (58%), 41 had acute pancreatitis (18%), 22 had cholangitis (9.7%), 21 had biliary colic (9.3%), and 11 had choledocholithiasis (4.9%). Management of the first episode was with antibiotics alone for 127 patients (56.3%), and an invasive procedure (as cholecystostomy or ERCP) was performed in 99 patients (43.8%). Table 1 summarizes the patient characteristics at H1 in each group by recurrence. The mean age for the overall cohort was 80.4 ± 7.2 years, with a predominance of female ratio (56%). A total of 108 patients (47.8%) had a high comorbidity index. Analyzing cohort characteristics, these were comparable in both groups.
Cohort characteristics.
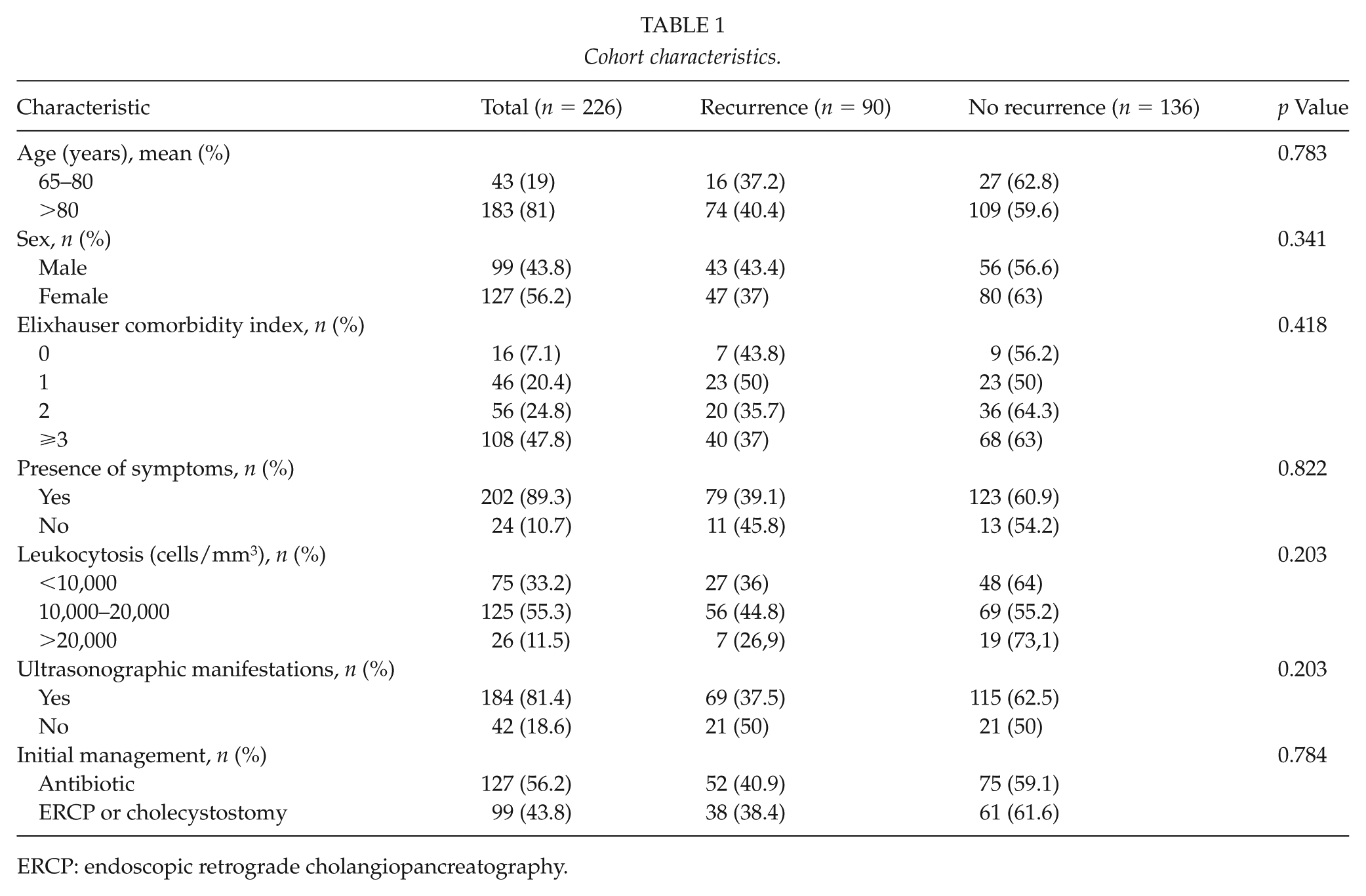
ERCP: endoscopic retrograde cholangiopancreatography.
Results of recurrence and management at follow-up are listed in Table 2. The 2-year cumulative RR was 39% (90 patients). The mean time to recurrence during the follow-up was 255.2 ± 42.1 days (8.5 months). Recurrence was 81% after 1 year and 88% within 2 years. Only 10 of 90 patients (11.1%) developed a recurrence later than 2 years following H1. Among the 90 patients that recurred, 57 (63%) presented a single new episode, 17 (18%) two recurrent episodes, and 16 (17%) three or more. After H1 discharge, 40 patients (44%) underwent surgery, 25 (62.5%) with a DC, and 15 (37.5%) during admission for a recurrent episode. ERCP was performed in 37% of patients with recurrence and cholecystostomy in 16%.
Outcomes over 2 years of follow-up.
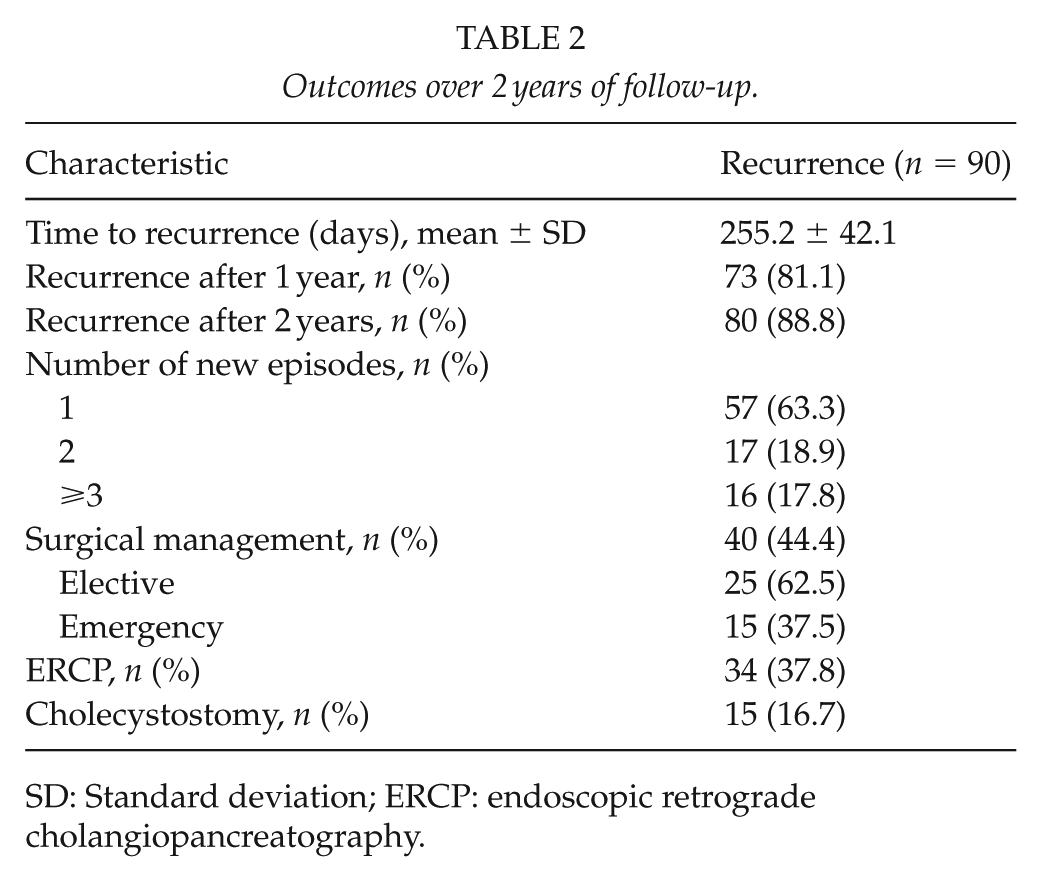
SD: Standard deviation; ERCP: endoscopic retrograde cholangiopancreatography.
Diagnoses at H1 were grouped as gallbladder disease and BD disease (Table 3), showing a higher RR in the BD group (33% vs 52%, p < 0.001). Subjects with two or more diagnoses presented a higher RR (32% vs 49%, p < 0.001) as well.
Diagnosis and recurrence.
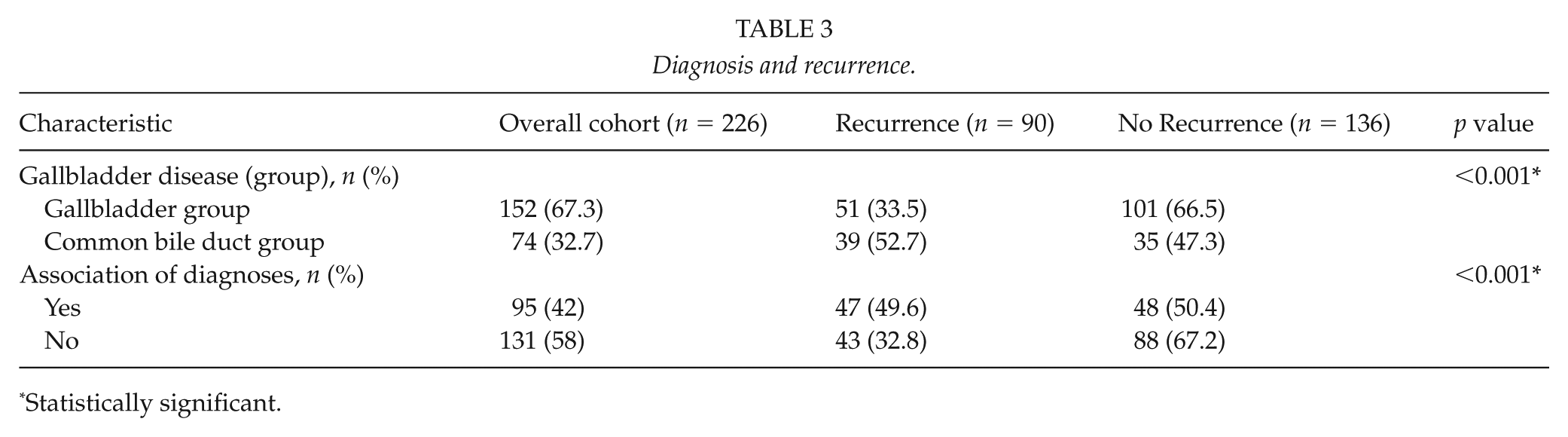
Statistically significant.
Curves for time to recurrence are illustrated in Figs 1 and 2. Kaplan–Meier analysis of time to recurrence was performed comparing both groups of diagnoses for biliary disease. The diagnosis group was not found to be a significant predictor of time to recurrence (p = 0.112) (Fig. 2).
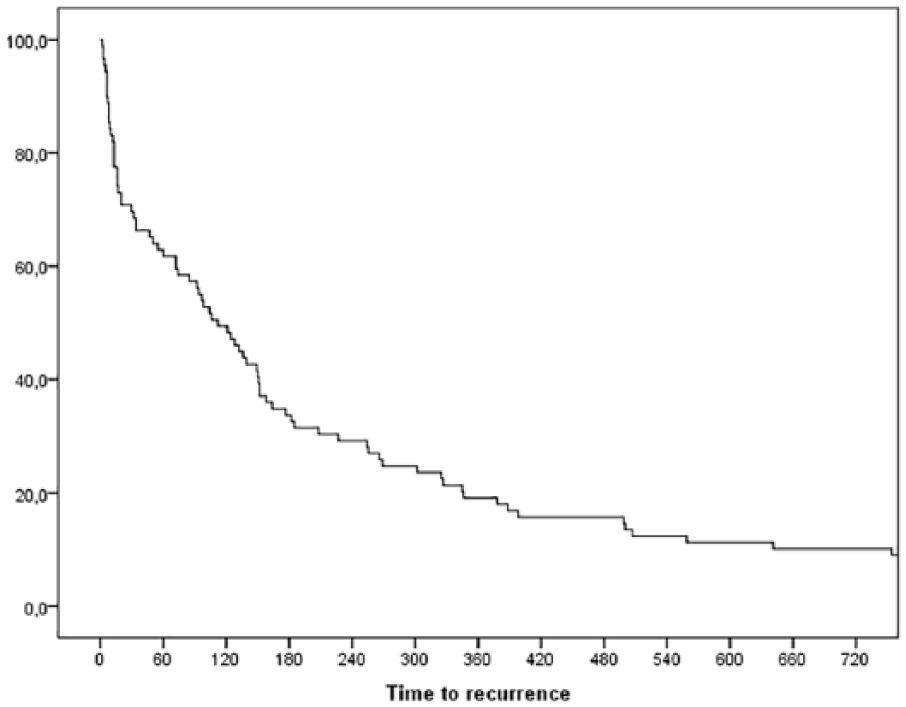
Kaplan–Meier curve for time to recurrence after 2 years.
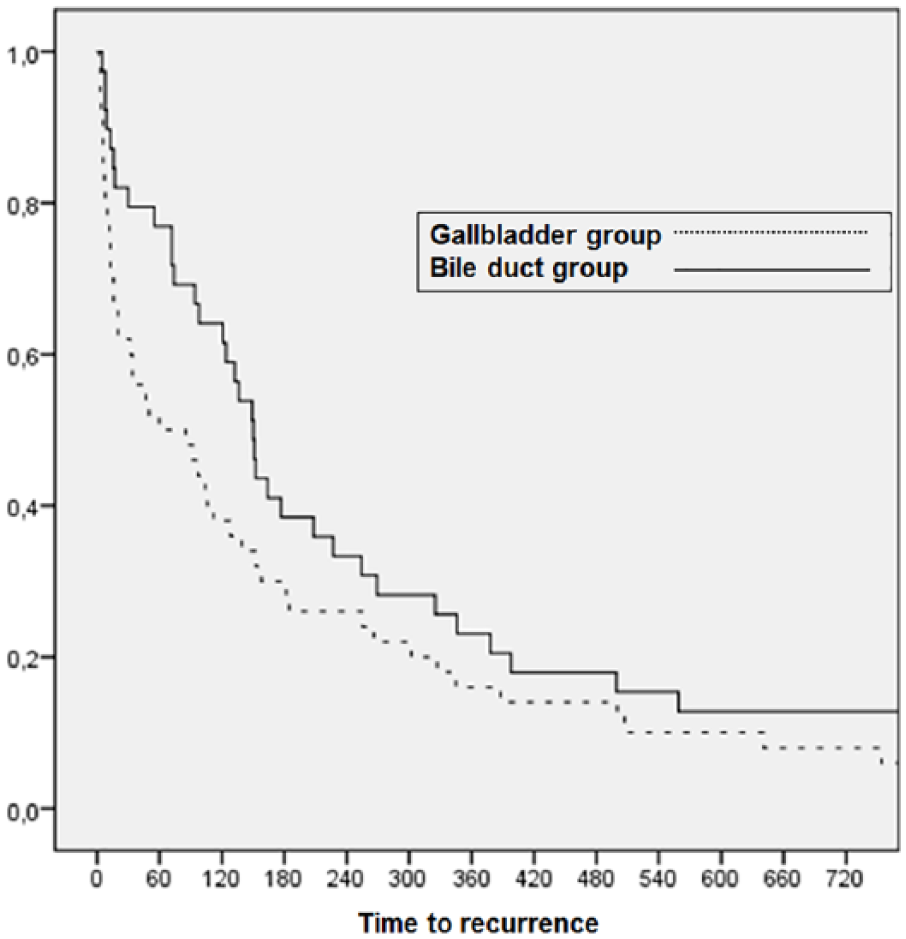
Kaplan–Meier curve for time to recurrence depending on diagnosis group.
Discussion
Gallstone disease presents a high incidence and morbidity in elderly population. Although cholecystectomy is the most accepted treatment, a high proportion of elderly patients still undergo an NOM (8, 9). Only a few studies have analyzed the RR after NOM of symptomatic gallstone disease in the elderly patients (5, 7–9, 21). Previous retrospective analyses notified RR around one-third of patients after a 1-year follow-up (6, 9), increasing up to 40% in the long term (7, 8, 10). In our series, we found an RR of 32% after 1 year and 39% within 2 years from H1.
In addition to this, we found higher RR in patients initially diagnosed with a BD disease when compared to the gallbladder disease group (52% and 33%, respectively). These findings have been previously supported by other authors (6–8). Trust et al. (8) reported an RR of 43% for biliary pancreatitis, and a recent review of conservative treatment for ACC notified a rate of 22% after a 2-year follow-up (22). This is the reason why current guidelines recommend an EC in these cases (8, 12). Furthermore, in our series, RR was also related with the presence of two or more diagnoses for the same patient, which represents a higher probability of relapse episodes according to the severity of the first event.
Moreover, while EC has shown similar outcomes to DC (15, 17, 18), NOM would imply a higher risk of conversion and complications in the case of a surgery for a recurrent episode (5, 7, 8, 16). In addition, significant additional costs per re-admission could be associated (7). In our study, only 44% of patients with recurrent episodes underwent a cholecystectomy, and 37% of them during re-admission for a relapse.
Some authors have established protective role related to female gender and for additional invasive procedures (7, 9). Bergman et al. (9) reported a 1-year recurrence-free survival rate of 70% after additional invasive procedures during H1 as ERCP or cholecystostomy. Short-term RR described after ERCP for acute pancreatitis is around 5%–20% (9, 23, 24) and 27%–35% (25, 26) after cholecystostomy for ACC. Despite reporting decrease in RR with additional procedures, the gallstone-related readmissions remains higher than in patients managed definitively with cholecystectomy (8). In our patients, the cholecystostomy was not related with a decrease in RR. According to current guidelines (11, 12), it could be a safe and effective procedure in critically ill patients or subjects presenting serious medical comorbidities.
Our study presents some limitations: it is a retrospective review, and there were no pre-specified criteria for NOM. In addition to this, our study only included index admission for new episodes of biliary disease, but it does not take into account outpatient attending the ED, so that the true RR could have been underestimated. Finally, we were not able to capture all recurrent episodes of disease of patients who further attended in other centers (however, inter-hospital movement is uncommon in the elderly population on our area).
Conclusion
NOM of the first episode for symptomatic gallstone disease showed an RR of 39% after a 2-year follow-up. RR was related to the specific diagnosis and severity of the first episode at H1. If there are no contraindications for surgery, cholecystectomy should be considered during the initial admission in order to prevent relapses.
Footnotes
Acknowledgements
All listed co-authors were integrally involved in the formation of this manuscript via study conception/design and/or data acquisition and analysis/interpretation. Furthermore, all authors made significant contributions to the drafting or critical revisions of the manuscript, and all authors gave final approval prior to submission for publication. This study was presented at the 31st National Congress of Surgery, Spanish Surgical Association. November 7–10, 2016, Madrid, Spain. A minor group of patients included in this study was previously analyzed inside a prior brief report published in a local journal by the same authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.