
Abstract
Background and Aims:
Emergency surgery represents an essential aspect of surgical care, but little is known about realization of the planned emergency class. Different systems such as NCEPOD classification and Timing of Acute Care Surgery classification have been developed for the timing of the emergency surgery. The aim of the study was to find out how well planned urgency class is being implemented.
Materials and Methods:
The planned and realized waiting times for all emergency surgeries were studied during the 6-month period in the Oulu University Hospital. The catchment area of the hospital includes a population of 742,000. The urgency in the hospital is planned in a four-step scale: an extremely urgent (E) patient should be taken immediately to the operating theater. Class I urgency surgery should start within 3 h (180 min), class II within 8 h (480 min), and class III within 24 h (1440 min). Surgeon plans urgency at his discretion, and no specific urgency has been imposed on certain diagnoses thus the surgeon’s perceptions of the illness or trauma affects the assessment.
Results:
Extreme urgent patients had an average waiting time of 26 min. For class I patient, the average waiting time was 59 min, while 93% of surgeries were started within the target time. For class II and class III patients, these figures were 337 min and 86% and 830 min and 78%, respectively.
Conclusion:
With regard to urgency, the higher the degree of urgency, the greater the chance of the surgery being realized within the planned time.
Introduction
In developed countries such as Finland, emergency surgeries account for approximately 25% of all surgeries performed (1, 2). Key issue in organizing emergency surgery is assessment of the emergency class. Considering the varying and individual nature of illnesses and injuries, the classification must be flexible. Various systems such as NCEPOD (National Confidential Enquiry into Patient Outcome and Death) classification and Timing of Acute Care Surgery classification (TACS) have been implemented for timing of emergency surgery (3, 4). Although being in the center of the emergency surgery, surprisingly little is known about the realization of planned emergency class.
In a recently published study, Finland was reported to have high healthcare access as well as a high quality index for all surgical domains (injuries, adverse effect of medical treatment, appendicitis, and gallbladder diseases), so one could assume that the Finnish surgical on-call system is a well-functioning one (5).
Material and Methods
Oulu University Hospital is the largest hospital in Northern Finland, with 148 surgical and 26 intensive care unit beds. It is a level I trauma center. The hospital’s catchment area includes a population of 742,000.
The on-call is arranged as follows: one resident has responsibility for both operating theaters and surgical wards; the resident has authority over the order of operations; and on-call consultants are arranged for gastrointestinal surgery, cardiothoracic surgery, vascular surgery, urology, hand surgery, plastic surgery, spinal surgery, and neurosurgery. Residents have at least 2 years of experience in the surgery (they have passed general surgical training period). Most often residents have on-call experience between 4 and 6 years.
With regard to surgical urgency, four possible categories exist. An extremely urgent (E) patient should be taken to the operating theater immediately. Class I urgency surgery should start within 3 h (180 min), class II within 8 h (480 min), and class III within 24 h (1440 min). The surgeon has discretion to determine urgency, and no specific urgency has been assigned to certain diagnoses. Thus, the surgeon’s perception of the illness or trauma affects the assessment of urgency. It might also be affected by, for example, a desire to secure a convenient operating time, the individual patient’s requirements, or other non-medical reasons. A resident places patients in the right order of urgency and negotiates with the anesthesiologist and with the specialist surgeons if needed. The treatment of the critically ill patients is planned together with resident, consultant surgeon, intensivist, and anesthesiologist.
The distance from the emergency department to the operating theaters is circa 150 m. One computed tomography (CT) device is placed in the emergency department, so patients do not usually need to be moved to the radiologic department for diagnostic imaging. Distance from the surgical wards to the operating theaters is circa 100 m.
The realization of the urgency class (planned urgency class and realized waiting time) was investigated over a 6-month period (June 2016 to December 2016). The results show the average waiting time (from placing the patient on the operating list to the initiation of the operation) as well as the proportion of operations that were started within the target time. All data were collected from the hospital’s surgical database.
Results
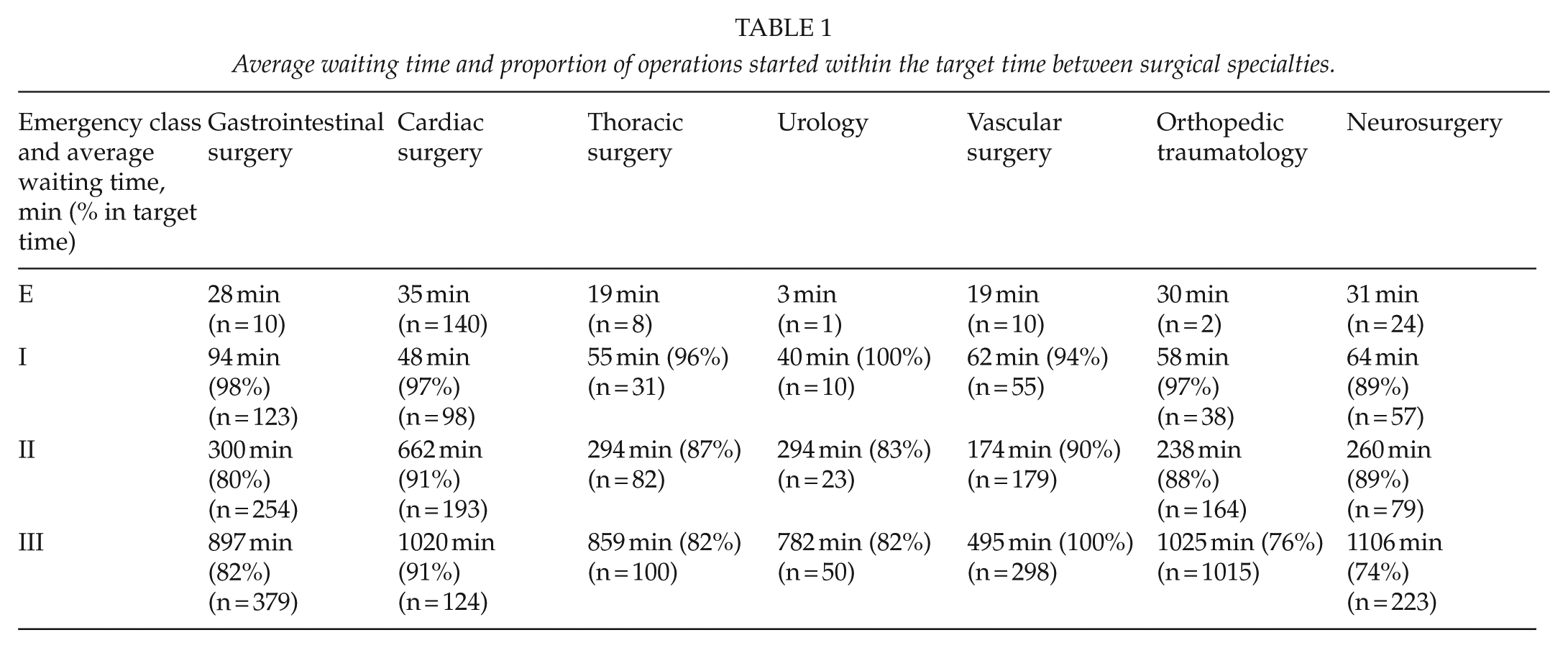
The average realized waiting time and the proportion of operations started within the target time are described in relation to both the different surgical specialties (Table 1) and to the particular surgery (Table 2).
Average waiting time and proportion of operations started within the target time between surgical specialties.
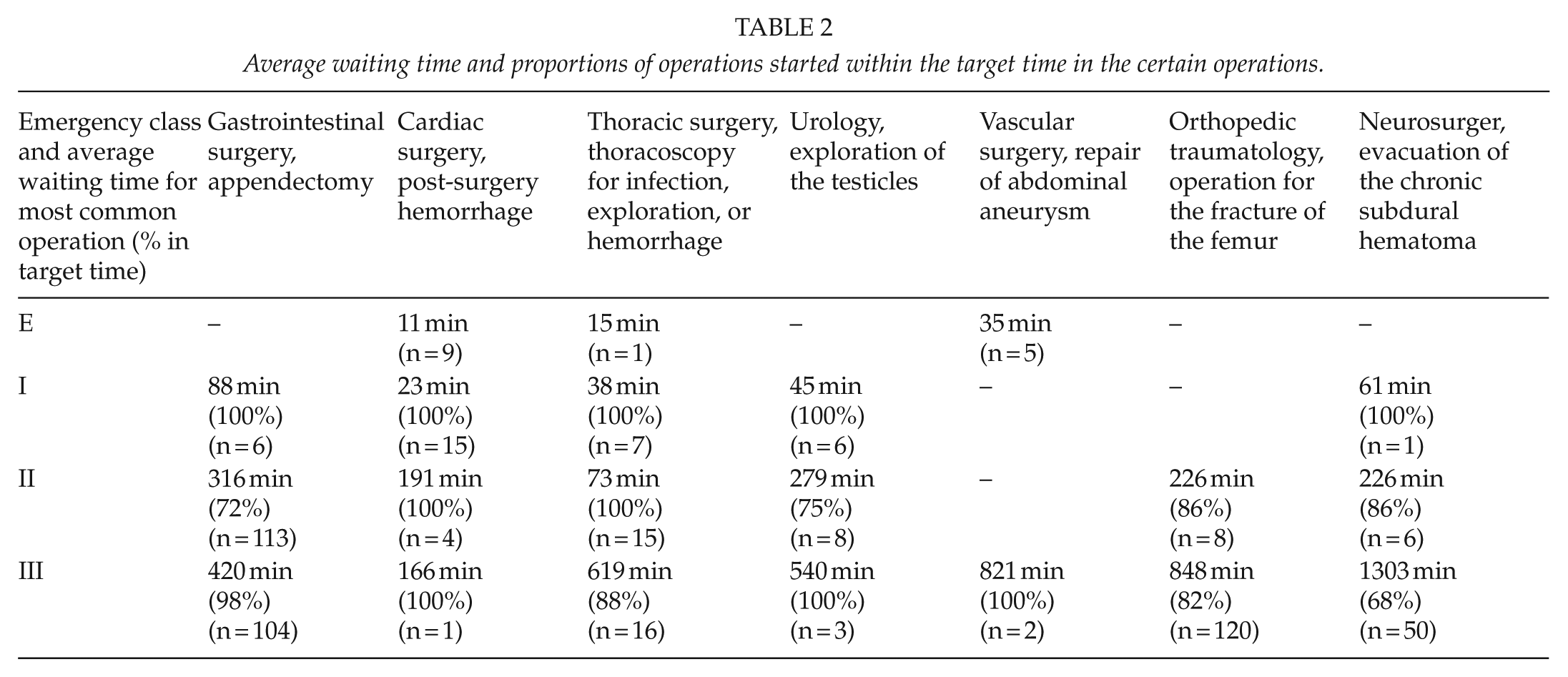
Average waiting time and proportions of operations started within the target time in the certain operations.
Of all the operations, 4.5% (197/4350) were classified as being extremely urgent, and they had an average waiting time of 26 min. Class I was assigned to 9.7% (421/4350) of operations, which had an average waiting time of 59 min (93% within the target); class II was assigned to 23.3% (1013/4350) of operations, which had an average waiting time of 337 min (86% within the target); and class III was assigned to 62.5% (2719/4350) of operations, which had an average waiting time of 830 min (78% within the target) (Fig. 1).
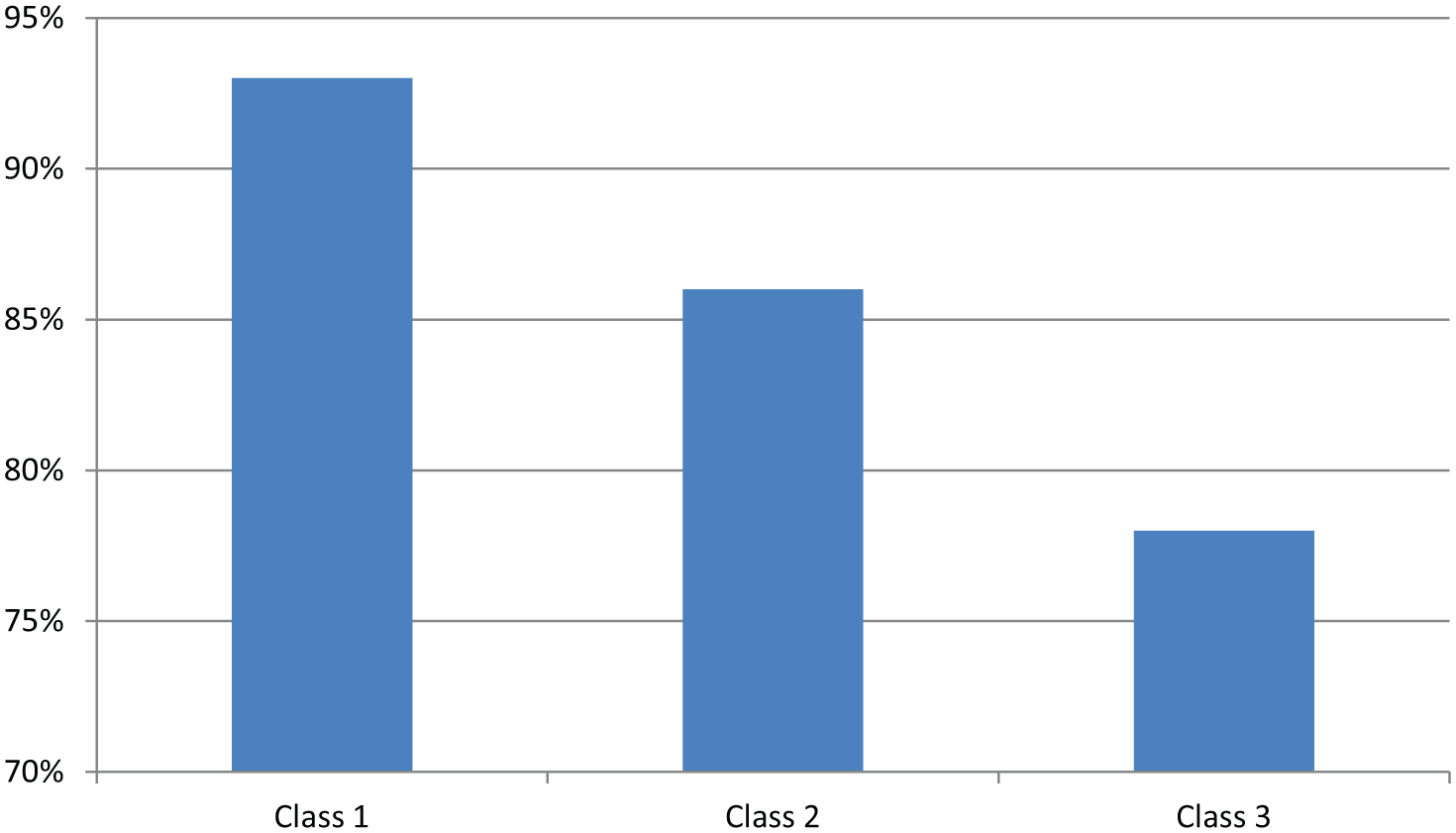
Proportions of the operations started at the target time within urgency classes.
Discussion
Taking into account the importance of the subject, the triage of surgical patients to operating theater has triggered surprisingly rare discussions and publications. Various types of urgency classification systems exist in the world, such as the NCEPOD classification used in the United Kingdom and the TACS (3, 4). The NCEPOD classification has four categories: immediate, urgent, expedited, and elective. It is rather inaccurate with the most urgent patients (immediate patient should be taken to the theater immediately; urgent within a few hours; while for expedited, days of waiting is allowed). The TACS is an initiative of the World Society of Emergency Surgery Group. The TACS divides patients into four categories: immediate or extreme urgent surgery, surgery within an hour from diagnosis, surgery within 6 h from diagnosis, and surgery within 48 h from booking the operation. Most hospitals have a system designed for their own conditions. The Helsinki University Hospital has published a traffic light coding system, where the red code indicates surgery no later than 8 h from booking the surgery, the orange code no later than 24 h, and the yellow code no later than 48 h (6). The Helsinki University Hospital was able to decrease night-time surgery using this classification. Our hospital’s system is close to TACS.
The realization of the planned urgency has been studied astonishingly rarely—we were not able to find any articles about topic in the literature. Thus, we investigated this in the Oulu University Hospital whose catchment area includes a population of 742,000 and which is a class I trauma center in Northern Finland, Scandinavia.
The patients’ planned urgency class realized well in the most urgent classes (I and II). The operations were, on average, realized faster than the required urgency class (in class I, 93% and in class II, 86% within the target). Operations in extreme urgent class (E) realized very fast—average waiting time of 26 min is most likely spent carrying the patient to the operating room and preparing the procedure. It is obvious that the condition of the individual patient is taken into account and that when the urgency is clear, the treatment is accomplished very quickly. The proportion of patients operated on within the target time decreased as the urgency decreased. The majority of patients (57%) were allocated to class III and as high a proportion as 22% in this group had a waiting time over the target of 24 h. O’Leary et al. (7) found that in Galway University Hospital (which has equal population base as Oulu University Hospital), one-third of all emergency surgical patients had to wait longer than 24 h for surgery. In Galway University Hospital, the priority target for appendectomy was <8 h and realized mean time-to-theater was 13 h (780 min) for appendectomy. In our hospital, for the appendectomy, the time-to-theater was 88 min in the class I (100% in target), 316 min in the class II (72% in target), and 420 min in the class III (98% in target). These results shed light to the fact that time-to-theater may be usually longer than what is anticipated.
Our simultaneous study about perceptions of surgeons of the on-call duty gives some clues about the reasons for the delay (unpublished data). The possible causes are rush, the surgical team’s desire to select the most suitable patients for themselves, the tiredness of professionals, and pursuit to save operating theater resources for more seriously ill patients. It is impossible, however, to say the exact reasons for the delays because our computer system does not require the registration of the cause of the delay. Also, the real reason does not necessarily want to be recognized (e.g. if surgeon has chosen for himself the most interesting operation and not the most urgent patient). Delays were the most common in the least urgent class. The so-called “green line” for non-urgent emergency surgery (schedule is approximated early and the patient may go home to wait) is instituted in some hospitals (6). This study encourages such a policy.
As a conclusion, the higher the degree of urgency, the greater the chance of the surgery being realized within the planned time. Less urgent patients have often unreasonably long waiting time to operating theater.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Northern Ostrobothnia Hospital District.