
Abstract
Background and Aims:
Traditionally, patients requiring an orthopedic emergency operation were admitted to an inpatient ward to await surgery. This often led to congestion of wards and operation rooms while, for less urgent traumas, the time spent waiting for the operation often became unacceptably long. The purpose of this study was to evaluate the flow of patients coded green in a traffic light–based coding process aimed at decreasing the burden on wards and enabling a scheduled emergency operation in Central Finland Hospital.
Materials and Methods:
Operation urgency was divided into three categories: green (>48 h), yellow (8–48 h), and red (<8 h). Patients, who had sustained an orthopedic trauma requiring surgery, but not inpatient care (green), were assigned an operation via green line process. They were discharged until the operation, which was scheduled to take place during office hours.
Results:
Between January 2010 and April 2015, 1830 green line process operations and 5838 inpatient emergency operations were performed. The most common green line process diagnoses were distal radial fracture (15.4% of green line process), (postoperative) complications (7.7%), and finger fractures (4.9%). The most common inpatient emergency operation diagnosis was hip fracture (24.3%). Green line process and inpatient emergency operation patients differed in age, physical status, diagnoses, and surgical procedures.
Conclusion:
The system was found to be a safe and effective method of implementing orthopedic trauma care. It has the potential to release operation room time for more urgent surgery, shorten the time spent in hospital, and reduce the need to operate outside normal office hours.
Keywords
Introduction
The number of patients in hospitals awaiting emergency orthopedic surgery varies widely from day to day. Fractures of the hip, ankle, wrist, spine, and proximal humerus have been reported to be the five commonest fractures, comprising two-thirds of all fractures requiring hospitalization (1). Traditionally, all trauma patients requiring operative care were admitted to hospital to await surgery. This meant that, at busy times, time to operation could extend up to several days, resulting in a high inpatient ward burden, decreased patient satisfaction, and excessive pressure on operating rooms. The backlog that built up for operations was often eased using additional operating teams and, even in the absence of medical indications, by operating during nighttime. In recent years, increasing attention has been focused on the increased risk for complications, the extra costs of nighttime operations, and the health risks night working poses for employees (2,3).
Categorizing systems have been introduced to prioritize patients awaiting a surgical operation. One of these is the so-called traffic light coding system (4). In this system, emergency operations are uniformly classified with an urgency color code. Patients with the highest priority are coded red. These, critically ill, patients must be operated on within 8 h. For patients coded orange and yellow, the respective levels of urgency are 8–24 and 24–48 h. It has been previously shown that this categorizing system is able to increase the quality of care and satisfaction of the operating room staff (5).
An extension to the original traffic light coding system is the “green line” process (6). After careful preparation, patients considered suitable for green line process (GLP) are discharged to home or a secondary care facility from the emergency department await their planned operation, scheduled to take place at a given time within the following week.
The literature on patient flow in the traffic light system has focused on the treatment of patients coded as red, orange, or yellow (4). To our knowledge, no studies exist on emergency orthopedic trauma prioritization. Very little research exists on delayed care processes among orthopedic trauma patients, even though this may be a common practice in many hospitals nowadays. Due to limited operation room (OR) resources, the waiting time for patients with a less urgent trauma often extends beyond the time originally planned, as more urgent traumas, such as hip fractures, need to be treated first. This generates dissatisfaction in both patients and personnel, overcrowding of inpatient wards and pressure to operate outside normal office hours. The aim of this study was to evaluate patient flow and the feasibility of the GLP of care compared to the traditional organization of emergency orthopedic surgery in patients over 16 years of age.
Materials and Methods
Central Finland Hospital (CFH) is a trauma level II/III hospital offering orthopedic trauma care to a regional population of approximately 250,000, or approximately 5% of the Finnish population. The material for this retrospective cohort study was collected between 1 January 2010 and 23 April 2015. The surgical specialties analyzed were orthopedics, orthopedic traumatology, and hand surgery.
Green Line and Inpatient Emergency Operations
In this study, GLP refers to a process of care for patients requiring emergency—but not immediate—operative treatment. In GLP, the patients who require surgery, but not inpatient care are discharged from the hospital and subsequently given a date for their operation, which will be performed as soon as possible during normal office hours. Before introduction of GLP, all patients requiring an orthopedic emergency operation were admitted to hospital until their operation could be fitted into the OR schedule. In this study, we refer to these patients as inpatient emergency operation (IEO). In CFH, one OR is dedicated for orthopedic IEO every day during office hours and one OR for all emergency operations outside office hours. One OR is reserved for GLOs 4 days a week (Tuesday to Friday) during normal Finnish office hours (7.30–15 o’clock).
Patients eligible for GLP are identified in the emergency department according to the pre-determined criteria that are presented in Discussion. In addition, some patients are assigned to GLP in an outpatient orthopedic traumatology clinic or in the trauma ward. Patients are carefully informed about the planned operation and any necessary imaging and laboratory tests are then performed or scheduled to be performed later. A coordinating nurse schedules the operation for the next available GLP day. A specialist in orthopedic surgery or hand surgery, or an experienced surgical resident, is assigned to perform GLP operations on each day.
Preoperative care is individually planned for each GLP patient. Most patients are admitted to hospital in the morning and discharged after the operation on the same day. Patients requiring postoperative inpatient care or monitoring are admitted to the trauma ward until discharge or transfer to a tertiary care unit. GLP has been used in CFH since 2008.
Data Retrieval
The research data were retrieved from an electronic medical record (Effica, Tieto Corporation, Helsinki, Finland) and included time from the decision to operate to the operation, length of postoperative hospital stay, age, number of re-operations and mortality. The American Society of Anesthesiologists (ASA) physical status classification is routinely applied in all cases and these data were also collected. Mortality was determined as total deaths with no analysis of causality. The mortality data were gathered for patients who had died during their period of admission to hospital or in the tertiary care unit where they had been transferred from the hospital for further rehabilitation. Diagnoses were classified using the ICD-10 (International Statistical Classification of Diseases and Related Health Problems 10th Revision) classification and the procedures using the NOMESCO (Nordic Medico-Statistical Committee) classification of surgical procedures (Finnish version).
Data were also collected from a database where emergency department data (decision to operate) are combined with perioperative data. The data set was completed with data on the length of the postoperative ward period (Effica osastonhallinta). SQL queries were made using Microsoft SQL Server Management Studio 2008 (Redmond, USA) to filter the data. The data set was imported to QPR ProcessAnalyzer (automated business process discovery tool, QPR Software Plc, Helsinki, Finland) for visualization and analysis.
Central Finland Health Care District granted permission for this study. Permission from the ethical committee was not required, as the data set comprised anonymized registry data and the patients were not contacted.
Statistics
Categorical variables were compared across the operation groups using chi-square test. The level of significance was set to 0.05. Analyses were done using R statistical package v3.3.3 (R foundation, Vienna, Austria).
Results
Between 1 January 2010 and 23 April 2015, a total of 1830 GLP operations and 5838 IEOs were performed (annual numbers presented in Supplementary Figure 1). The patients between the groups presented different age distributions and prior health statuses. According to the ASA classification, GLP patients were significantly healthier than the IEO patients (p < 0.0001). GLP patients were also significantly younger; mean age of GLP and IEO patients was 48 and 61 years, respectively (<0.0001) (Supplementary Table 1).
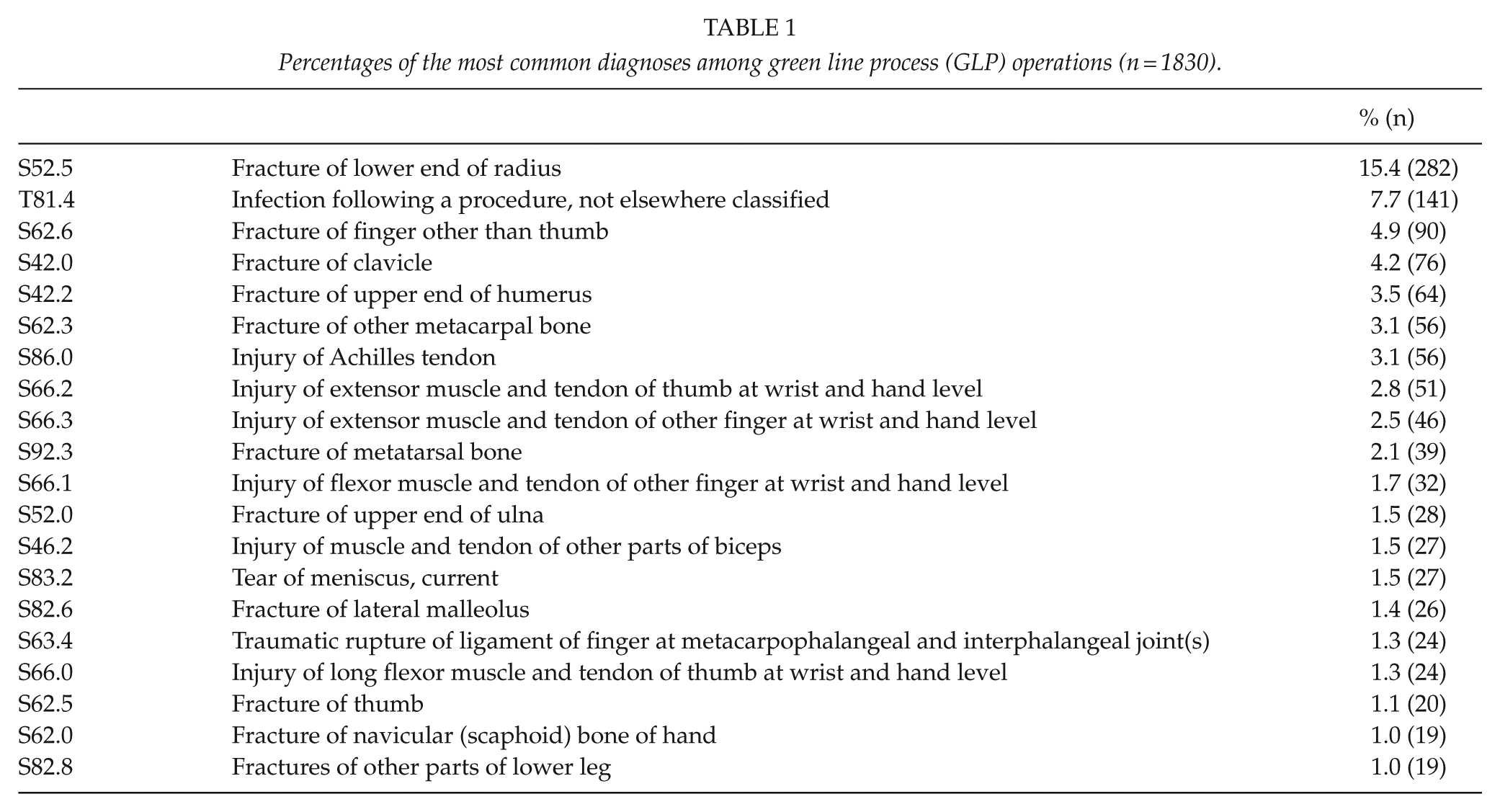
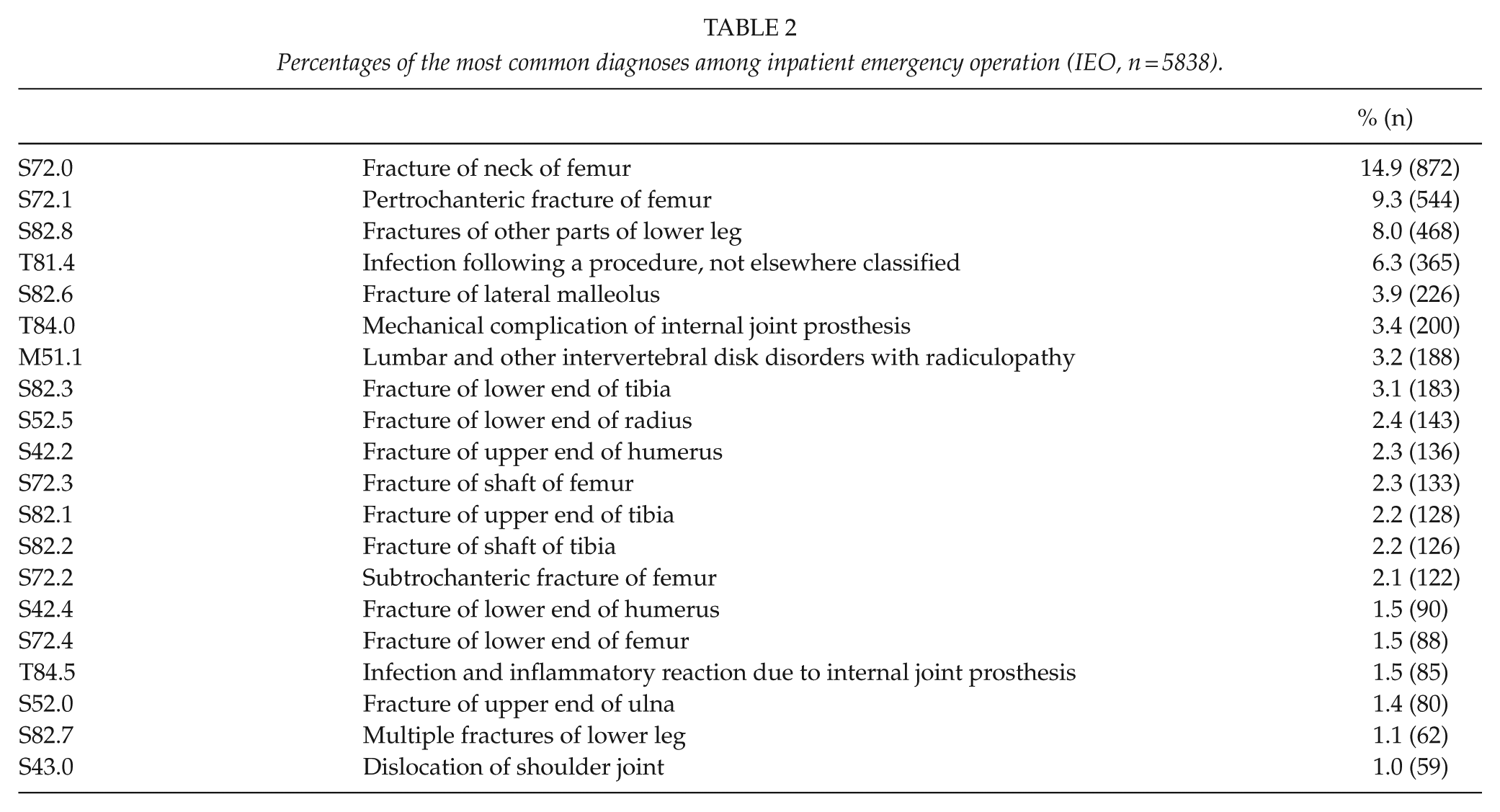
The most common GLP diagnosis was distal radial fracture, which was recorded as the primary diagnosis 282 times and accounted for 15% of all GLP operations (Table 1, annual numbers presented in Supplementary Figure 2). The same diagnosis was also recorded as the primary IEO diagnosis 143 times, accounting for 2.4% of all IEOs (Table 2). Diagnosis S52 (all fractures of the forearm) was the primary diagnosis in 19.8% of all GLP operations (n = 364). The second most common diagnosis among GLP patients was T81.4 (infection following a procedure), which was recorded as the primary diagnosis in 8% (n = 141). The most common procedures among the IEOs were fractures of the head or neck of femur (S72.0) and pertrochanteric fractures (S72.1), which accounted for 15% (n = 872) and 9% (n = 544), respectively, and thus, 24% (n = 1416) of all IEOs.
Percentages of the most common diagnoses among green line process (GLP) operations (n = 1830).
Percentages of the most common diagnoses among inpatient emergency operation (IEO, n = 5838).
Time from the decision to operate to the operation itself differed between the GLP operations and IEOs; 65% of the patients assigned to GLP were operated within a week of the decision on operative treatment; 68% of IEOs were performed within 24 h and 92% within 3 days (p < 0.001) ( Figure 1).
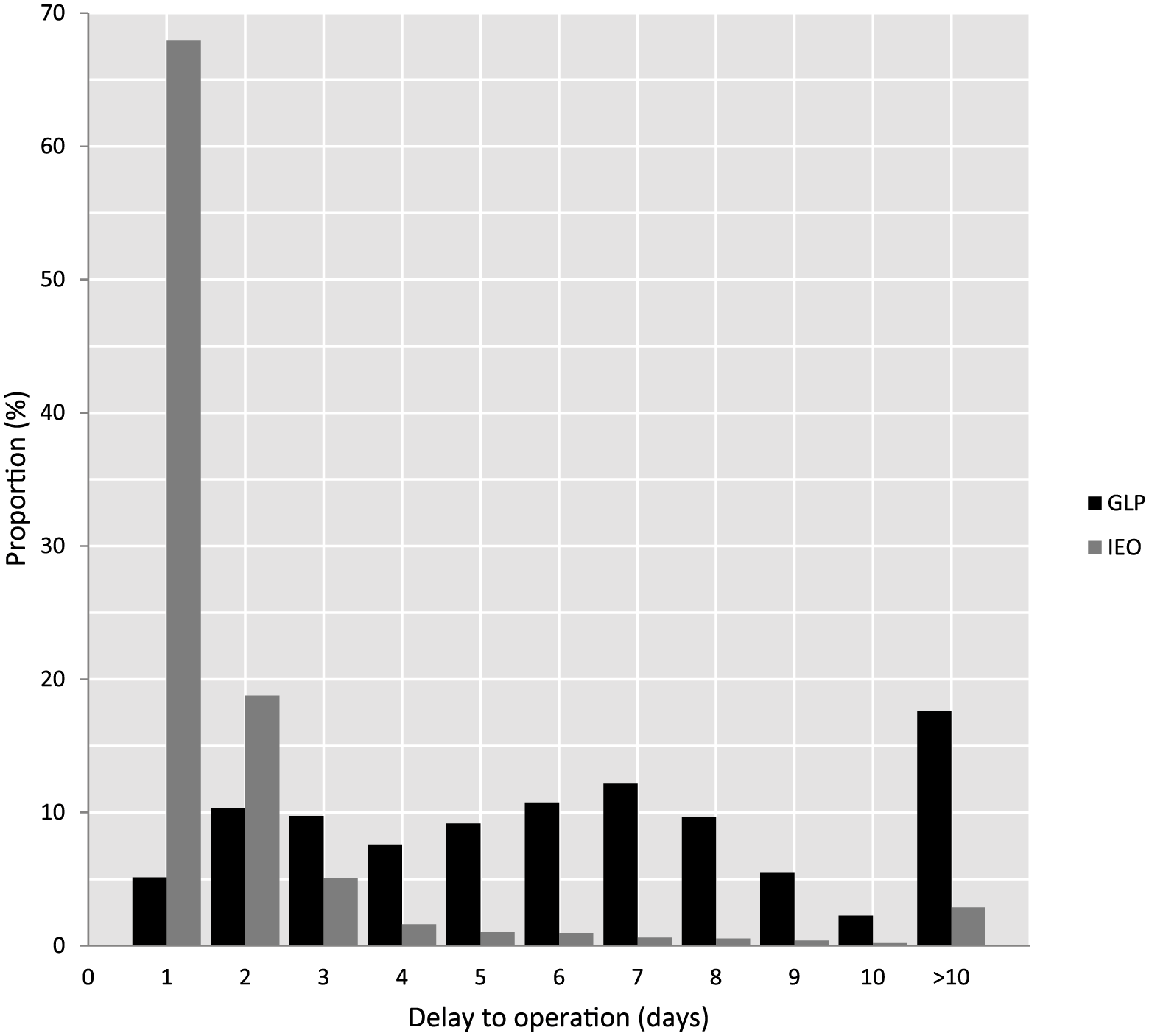
Proportions of patients receiving green line operations (GLP, black) and inpatient emergency operation (IEO, gray) by time to surgery in days.
Length of inpatient stay (LOS) differed between the GLP operations and IEOs. Admittance time was less than a day in 58% of GLP patients. Median admittance duration was 9 h. Among the IEO patients, only 10% were discharged within the operation day and the median admittance duration was 2 d 19 h (p < 0.001) (Figure 2).
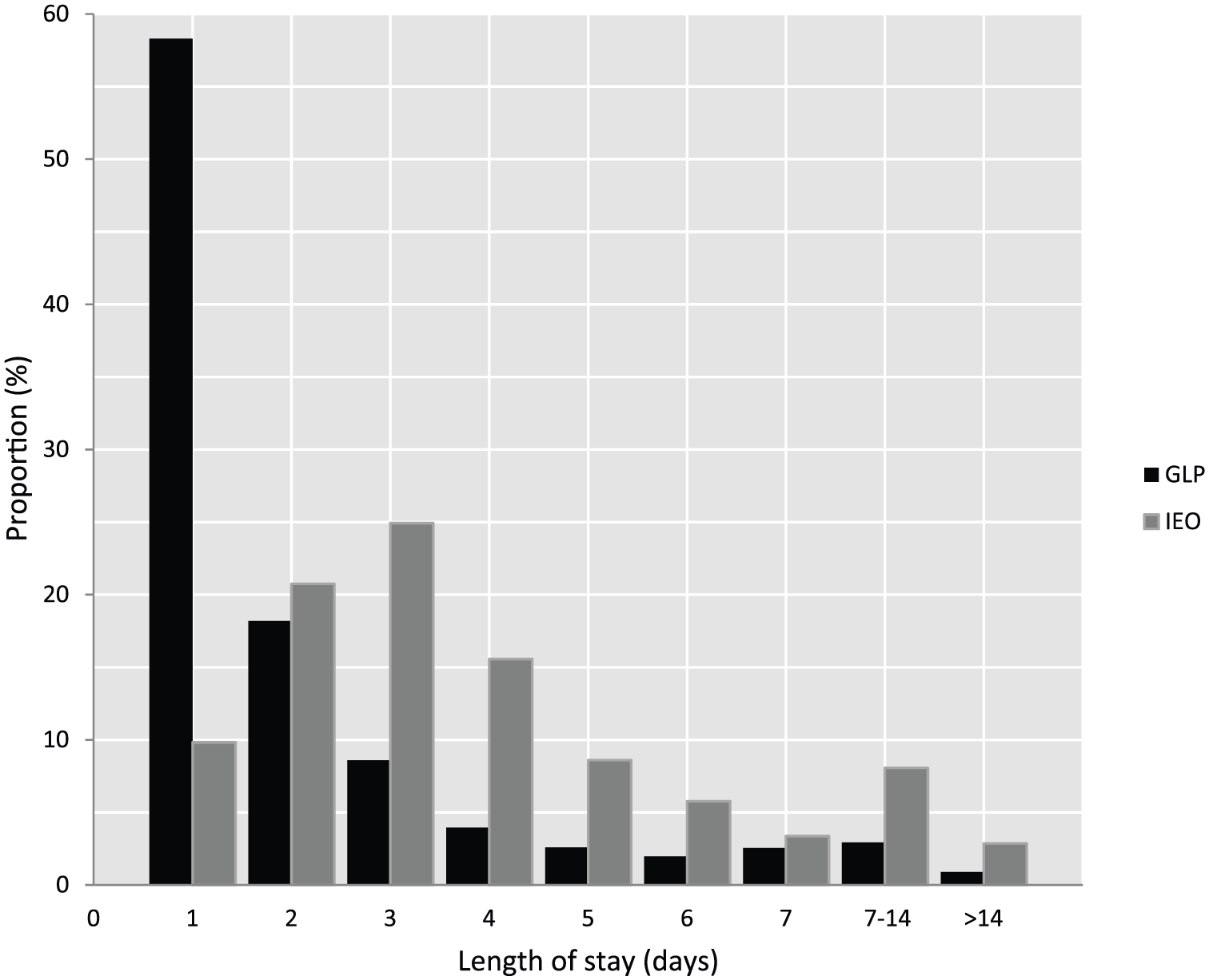
Length of inpatient stay of green line operations (GLP, black) and inpatient emergency operation (IEO, gray).
Among GLP operations, 64 patients (3.5%) were re-operated within 2 months due to postoperative infection (diagnosis code T8*, complications following surgery), compared to 335 of IEOs (5.8% of all IEOs). Postoperative infections were thus significantly more common among IEOs (p < 0.001). Mortality within 30 days of the operation was 0.1% (1) among GLP patients and 3.1% (182) among the IEOs. The percentages for 90 d mortality were 0.4% (n = 7) for GLP and 5% (n = 292) for IEOs (p < 0.001).
68% of the GLP operations were performed by a senior consultant, and the remaining 32% by a resident surgeon-in-training. For the IEOs, the corresponding proportions were 56% and 44%.
The number of procedures performed via GLP increased throughout the period analyzed. The annual number of GLP operations increased by 44%, from 284 to 408 between 2010 and 2014, whereas the number of IEOs showed no significant change. Currently, some operations, such as plating of distal radius fractures, are performed almost solely as GLP operations.
Discussion
In this study, we report our experience with GLP. The results indicate that not all acute trauma patients require inpatient care while waiting for an operation. The green line emergency trauma operation process has proved to be a well-functioning way of managing acute traumas in the domains of orthopedics and hand surgery. GLP has potential advantages compared to the traditional management of acute orthopedic trauma. The traditional system requires the hospitalization of patients until their operation. Usually, they cannot be given a specific time for their operation, meaning that if their trauma does not require immediate operative care they could, during busy seasons and due to limited OR resources, find themselves awaiting surgery for several days. For some patients, this may also entail extended periods of preoperative fasting. This may have a detrimental effect on satisfaction, of both the patient and medical personnel, and hence on the outcome of the operation. The green line system described in this study, originally developed in Töölö hospital, Helsinki, was implemented in our hospital to even out patient flow and increase the efficiency in the daytime use of operating rooms.
Safety
GLP may increase time to surgery for some patients. It is therefore important to assess the safety of the process. We found that complications are not unequivocally associated with the time spent on the surgical waiting list and re-operations were actually more frequent in IEO group. However, this is likely due to differences in diagnoses, procedures, and patients, not GLP versus IEO per se.
Increased mortality following hip fractures has been well documented (7). Furthermore, delay in surgery for more than 48 h increases hip fracture mortality (8). In contrast, the reported survival of wrist fracture patients may resemble or even be better than that of the general population (9, 10). To the best of our knowledge, no evidence has been presented to show that the outcome of common orthopedic injuries requiring surgery, such as closed upper extremity fractures and tendon injuries, is poorer if the delay between the decision to operate and the operation is over 48 h. For distal radius fractures, the outcome appears not to be affected if primary surgery is not performed for more than 3 weeks post injury (11). Mortality data on upper extremity fracture patients treated as outpatients are not available (9).
The outcomes of nighttime operations and surgery performed during off-hours have debated for many years. Overnight physicians in surgical wards have shown a higher rate of medication errors compared to off-call physicians (12). For surgical operations, the risk of complications is higher for those performed at weekends (13). The outcomes of trauma patients may also be poorer during off-hours (14). The safety and quality of operations performed by post-call personnel is inferior to that of operations performed during the daytime by residents who have not been on call the previous night (15, 16). We have, therefore, a strong incentive to focus our emergency operations during office hours.
Hip fractures form a large-volume inpatient group. Their postoperative outcome can be improved by not unnecessarily delaying the operation (17). In our experience, the green line system facilitates a timely operation for urgent (such as hip fractures) and a scheduled operation for less urgent (wrist fractures) traumas. Each green line operation is scheduled to take place at a specific time and in a specific OR with a consultant or an experienced surgical resident as the main operating surgeon.
Implications in Training
Performing definitive surgery for upper extremity injuries during normal office hours also has beneficial effects in surgeon training. During off-hours, only limited staff is likely to be present and experienced consultants may be absent. This can lead to situations where a surgeon in training is obliged to operate without adequate expert back-up. Insufficient surgical experience has been shown to have an adverse effect especially in the treatment of distal radius fractures (18–20). The green line system enables surgeons in training to perform operations with dedicated consultants during office hours. This may have a favorable influence on surgeon training in general. However, some studies suggest that the outcomes of some emergency orthopedic operations are not related to surgeon experience or time of day of surgery or night working prior to surgery by the attending surgeon (21, 22). In the case of hip surgery, this may be explained by the relatively short learning curve, which has been shown to vary between 20 and 35 patients, depending on the specific operation (23). These numbers are smaller than have been reported for volar plating of distal radius fractures (20). Hence, it may be more feasible for residents to perform surgery for hip fractures than for distal radius fractures during off-hours.
GLP has several potential advantages. Here we have listed some of the most important in our perspective:
Patients are given a specific time during the next few days for the operation;
Decrease in hospital admissions;
Patients are not required to fast for an operation that could be re-scheduled multiple times due to prioritizing of more urgent operations;
The patients requiring immediate operative treatment can be operated without delays (severe traumas such as hip fracture);
Preoperative planning is improved;
Increased efficiency of operating rooms due to better scheduling of operations;
Decreased need to operate during nighttime without medical indications;
Decreased need for extra operating teams outside office hours;
Surgical residents are better able to participate in operations and operate under the supervision of senior surgeons during daytime.
Injuries Suitable for Green Line Operations
Several traumas appear to be suitable for delayed operative care. These include most upper limb fractures, many ankle and foot fractures, and several tendon, muscle, and peripheral nerve injuries. These injuries mainly derive from low-energy events and do not have definitive requirements regarding hospital surveillance and care. To the best of our knowledge, no evidence has been adduced against delayed treatment of these injuries. Hence, we continue to assign patients with these types of injuries for GLP. However, whatever patient management system—such as GLP described in this study—is used, it must be subjected to immediate review and modification if evidence emerges that delaying treatment for certain injuries has deleterious effects.
To be suitable for GLP, the patient must meet certain criteria. These include the following:
Independent OR an adult support person available OR secondary/tertiary care available if not independent;
No need for immediate medical care or surveillance prior to operation;
Inpatient care does not improve prognosis;
Sufficient pain medication available.
Fractures and tendon injuries of the upper limb, wound debridements, and skin graft operations are especially well suited for GLP and are among the most frequent diagnoses in this system. Definitive guidelines for recruitment to GLP cannot easily be established. The types of injuries that are most often assigned to GLP display wide variation in their clinical manifestations, and hence not all finger fractures or skin graft operations are suitable for delayed treatment. Therefore, individual patient assessment, including cognitive, social, and clinical aspects, remains as an important part of the GLP.
Fractures of the hip, ankle, wrist, spine, and proximal humerus were the five most common fractures, accounting for 64% of all fractures requiring hospitalization, in our hospital before the introduction of the green line system (1). In contrast to this earlier situation, we found that nowadays wrist fractures rarely require hospitalization. Hip and ankle fractures remain the most common traumas requiring hospitalization.
The waiting times for IEOs and GLP operations showed a completely different distribution. One explanation for this is that IEOs are usually implemented as soon as possible. The day of the week a GLP is assigned is likely to have an influence on the waiting time for a GLP operation, since these operations are only performed 4 days a week and only during office hours. This explains the finding that the waiting time for a GLP operation peaked at 2 and 6 to 7 days.
Mortality was significantly lower among the GLP operations than IEOs. This is likely due to the less severe nature of GLP diagnoses and differences between the patients. In the same population, before application of GLP, the mortality after upper extremity fracture was known to be significantly higher compared to general population: at 1 year follow-up, the mortality was 3.0% (9).
Limitations
Our study has some weaknesses. It would be useful to compare the utilization rate of the operating rooms, delays between diagnosis and operation, hospital admissions and possible complications with the same data prior to implementation of the green line system. A prospective study is needed to further assess the safety and efficacy of the green line system. The present data are reliant on the accuracy of the diagnostic and procedural records. It is plausible that due to possible inaccuracies in the records that the data do not include all the relevant operations.
Conclusion
The green line emergency operative care system offers several potential advantages compared to the conventional inpatient operating system. GLP is likely to reduce the inpatient ward burden and reduce the time to surgery for IEO patients admitted to hospital with an urgent need for surgery. Another important advantage is shorter LOS. It is also likely that the direct costs of care are lower due to the shorter mean LOS. Further studies are needed to investigate which patient—and trauma—related factors predict the best outcome for a GLP operation.
Supplemental Material
Supplementary_files_for_GLP – Supplemental material for Scheduled Emergency Trauma Operation: The Green Line Orthopedic Trauma Surgery Process Of Care
Supplemental material, Supplementary_files_for_GLP for Scheduled Emergency Trauma Operation: The Green Line Orthopedic Trauma Surgery Process Of Care by M. Ax, A. Reito, M. Koskimaa, A. Uutela and J. Paloneva in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
M.A. wrote the manuscript. M.A., A.R., M.K., and J.P. performed the data analysis. All authors contributed to the conception and design of the study, to critical analyses of the data, to interpretation of the findings, and to critical revision of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.