
Abstract
Background and Aims:
There are no population-based studies about hospital admissions and need for surgical treatment of congenital lower-limb deficiencies. The aim is to assess the impact children with lower-limb deficiencies pose to national hospital level health-care system.
Materials and Methods:
A population-based study was conducted using the national Register of Congenital Malformations and Care Register for Health Care. All 185 live births with lower-limb deficiency (1993–2008) were included. Data on hospital care were collected until 31 December 2009 and compared to data on the whole pediatric population (0.9 million) live born in 1993−2008.
Results:
The whole pediatric population had annually on average 0.10 hospital admissions and the mean length of in-patient care of 0.3 days per child. The respective figures were 1.5 and 5.6 in terminal lower-limb amputations (n = 7), 1.1 and 3.9 in long-bone deficiencies (n = 53), 0.6 and 1.9 in foot deficiencies (n = 26) and 0.4 and 2.6 in toe deficiencies (n = 101). Orthopedic surgery was performed in 72% (5/7) of patients with terminal amputations, in 62% (33/53) of patients with long bone, in 58% (14/24) of patients with foot and in 25% (25/101) of patients in toe deficiencies. Half (54%) of all procedures were orthopedic operations.
Conclusion:
In congenital lower-limb deficiencies the need of hospital care and the number of orthopedic procedures is multiple-fold compared to whole pediatric population. The burden to the patient and to the families is markedly increased, especially in children with terminal amputations and long-bone deficiencies of lower limbs.
Keywords
Introduction
Major congenital anomalies have an impact on the quality and length of life of the affected individuals. Prenatal screening and treatment of congenital anomalies increase the overall costs of national health systems (1). Previously, few population-based studies have described the burden to hospital care in congenital anomalies and Down’s syndrome (2–5). Patients with spina bifida have been reported to consume more health care resources than other surgically treated congenital anomalies in Kenya (6). Data on need for hospital admissions and surgical treatment are not only important for health resource allocation but also to the individual patients and families who are preparing to live with a child who has a congenital anomaly.
Congenital lower-limb deficiencies are rare with a live birth prevalence of 2.1 per 10,000 live births (7). There are no population-based studies about hospital admissions and need for surgical treatment of congenital lower-limb deficiencies. Earlier reports on lower-limb anomalies are hospital-based studies or case presentations describing surgical treatment of different subtypes of lower-limb deficiencies (8–12).
Our purpose in this national population-based study was to evaluate the number of hospital admissions, total time spent in hospital and frequency of surgical interventions in children with congenital lower-limb deficiencies. In addition, we wanted to explore possible differences between the subgroups of these congenital anomalies.
Materials and Methods
The data on congenital lower-limb deficiencies were collected from the national Register of Congenital Malformations (FRM) and the Care Register for Health Care (FHDR), both maintained by the National Institute for Health and Welfare (THL). FRM contains data on all live births, stillbirths, and fetuses from spontaneous abortions and terminations of pregnancy for severe fetal anomalies, all with at least one major congenital (fetal) anomaly. The data contain only cases born in Finland during the study years. Nationwide linkable data on all in-patient hospital discharges and outpatient visits are registered in FHDR.
FRM receives and actively gathers data on congenital (fetal) anomalies from hospitals, health-care professionals and cytogenetic laboratories. FRM also draws data with the help of the unique personal identification code (PIC) from other national health registers: Medical Birth Register, Register on Induced Abortions, FHDR (hospital discharge data on congenital anomalies from the first two calendar years after birth), all maintained by THL, as well as from Cause-of-Death Statistics, maintained by Statistics Finland. Included major structural anomalies and chromosomal defects were coded according to the 9th Revision of the International Classification of Diseases (ICD-9) of the World Health Organization during the study period in the FRM (13).
Basic variables collected in FHDR include PIC (including date of birth and sex), area of residence, hospital ID, admission and discharge days, operation days, as well as diagnoses of patient’s medical problems. Diagnoses were recorded according to the ICD-9 during 1987−1995, and with ICD-10 since 1996. Operations were registered according to the classification of the National League of Hospitals during 1986−1996, and from 1996 onward with the Finnish version of Nordic Medico-Statistical Committee (NOMESCO) procedure classification.
During the years 1993−2008 there were 942,692 live births in Finland according to the national Medical Birth Register (2013) (14). We collected all live births (194) for fetal anomalies with lower-limb deficiency born in 1993–2008 from FRM. Diagnoses and medical records of all the cases were re-evaluated by a pediatric and orthopedic surgeon and a medical geneticist (J.S. and A.R.). If diagnosis was unclear additional information (e.g. patient records, photographs, X-ray images, specialist opinions) was requested from the hospitals concerned. Problematic cases were also discussed with two pediatric orthopedic surgeons (I.H. and Y.N.). Nine children who died during their birth admission were excluded. The final study population (185 cases, mean follow-up 9.8 years (range 1.0−17.0 years)) was subdivided to terminal amputations (7), long-bone (53), foot (24), and toe (101) deficiencies. Long-bone deficiencies were further divided to femoral, tibial, and fibular deficiencies using the classification systems of Aitken (15), Jones (16), and Achterman–Kalamchi (AK) (17). At the end the study data were cross-linked with the Care Register for Health Care data.
Cases with lower-limb deficiency were cross-linked with the national FHDR data by the PIC. Number of all hospital admissions (excluding the birth episode), surgical and non-surgical admissions, days spent in hospital, as well as number and type of surgical operations were analyzed from 1 January 1993 until 31 December 2009 in the 185 patients with lower-limb deficiencies and in the whole pediatric population live born in 1993−2008 (N = 942,692).
Statistical Methods
Continuous variables were described as means and ranges. Categorical variables were described as frequencies and relative proportions (percentages). Counts of events were modeled with Poisson regression using logarithm of patient count per group as offset parameter. The probability of cases remaining free of all operations, all orthopedic operations, and all operations concerning lower-limb deficiency was estimated using the method of Kaplan–Meier and the differences between subgroups were tested using log-rank test. Cox’s regression model was used to calculate the hazard ratios (HR) with 95% confidence intervals (CI). p values less than 0.05 were considered statistically significant. All analyses were conducted using R version 3.0.2 (R Foundation for Statistical Computing, Vienna, Austria) and SAS System for Windows, version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
The whole pediatric population live born in 1993−2008 had 1,524,481 hospital admissions and 4,194,675 hospital days during the 17–year-long study period. Mean number of hospital admissions was thus 0.10 and mean length of in-patient care 0.3 days per child per year.
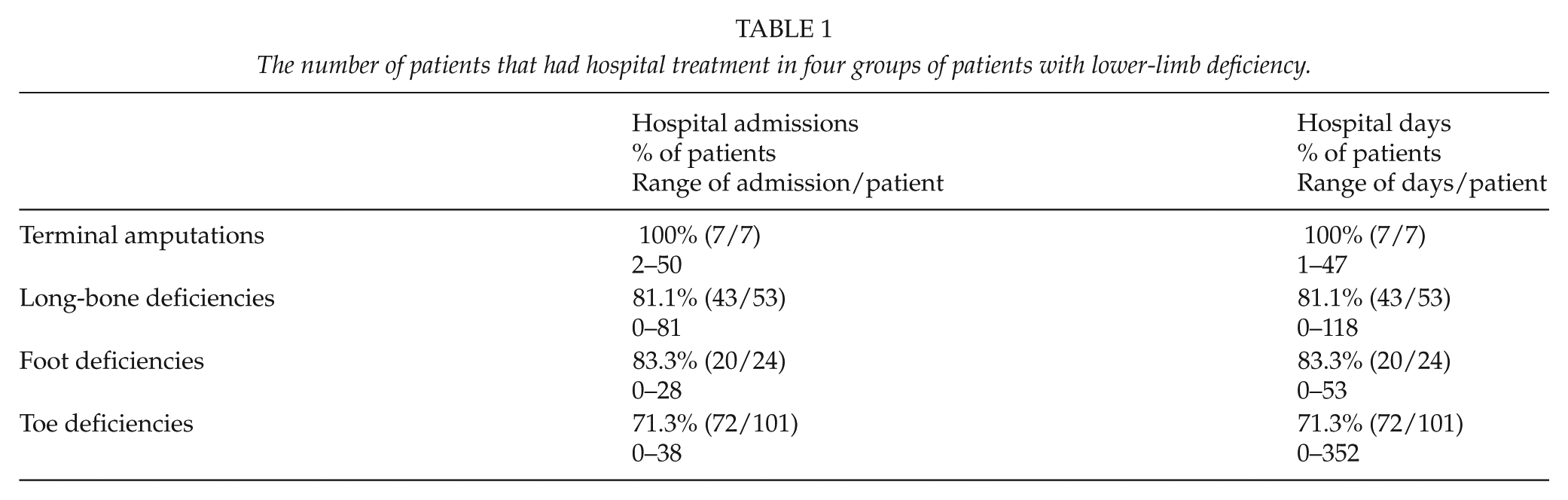
The 185 children with lower-limb deficiencies had altogether 1140 hospital admissions and 5170 days spent in hospital (Tables 1 and 2). Annually the mean number of hospital admissions was 0.6 (range 0−5), and days spent in hospital 2.9 (range 0−124) per child, which was 6- and 10-fold compared to the whole live born pediatric population in Finland. Half (49%) of the admissions were surgical and 119 (64%) of the patients had altogether 561 operations during the follow-up time. More than half (54%) of these procedures were orthopedic operations directed to lower limbs (226), upper limbs (70), and spine (8). The Kaplan–Meier estimate of cases having at least one operation, one orthopedic operation, and one operation concerning deficiency was 64%, 44%, and 32% after 10-year follow-up (Fig. 1.)
The number of patients that had hospital treatment in four groups of patients with lower-limb deficiency.
The percentage of patients and the range of treatment per patient that had surgical treatment in four groups of patients with lower-limb deficiency.
ENT: ear, nose, and throat procedures, GI-surgery: gastrointestinal surgery.
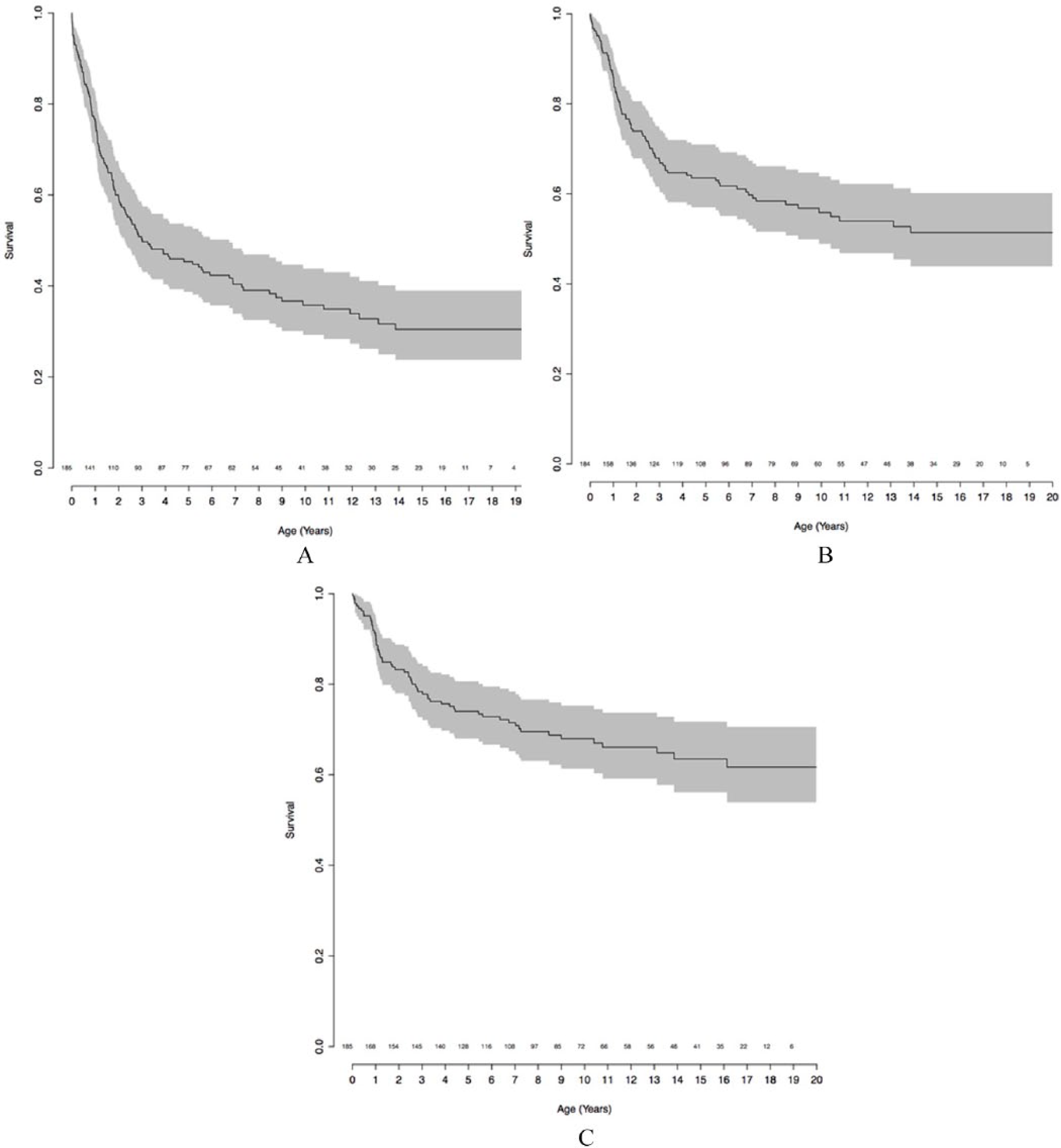
Five and ten-year operation free survival in A) all operations, B) orthopedic operations, and C) operations concerning lower-limb deficiency. Number of patients at risk for operation in x scale.
Seven patients with terminal amputations (lower leg 4 (bilateral 1), foot 3 (bilateral 2)), had annually mean 1.5 (range 1−4) hospital admissions and mean 5.6 (range 1−25) days of in-patient care, which was 15- and 19-fold compared to the whole live born pediatric population. All seven patients had surgical treatment during the study period. Orthopedic procedures were done between 0.4 and 2.4 years of age (Tables 1 and 2).
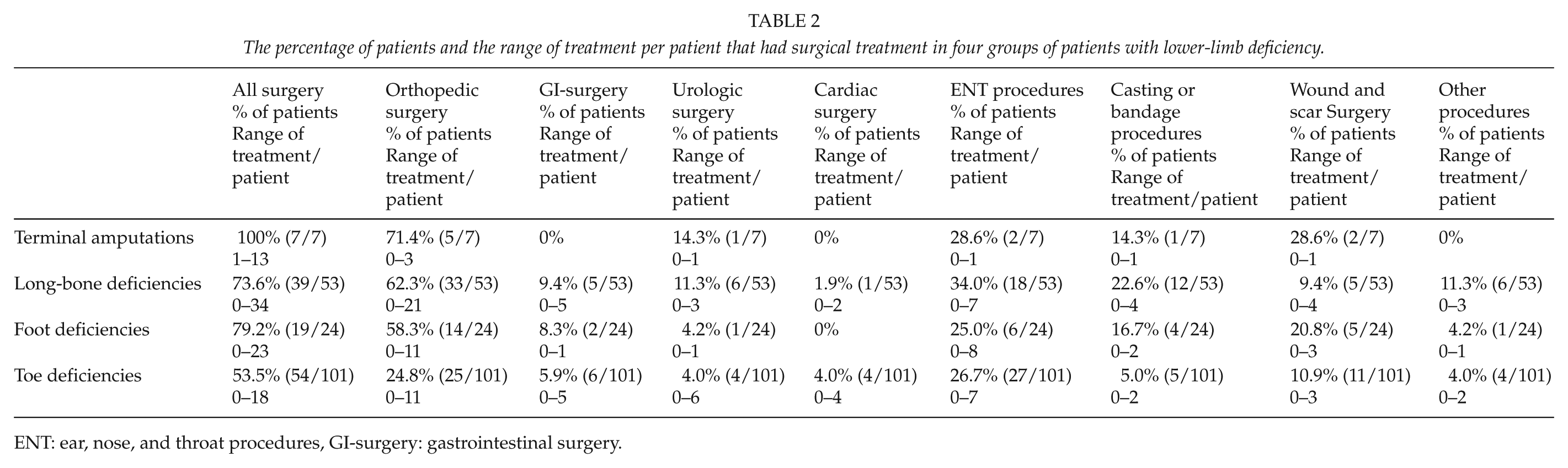
The 53 patients with long-bone deficiency (PFFD 11, tibia 5, fibula 37) had annually mean 1.1 (range 0−5) hospital admissions and 3.9 (range 0−10) days of hospital care. These figures were 11- and 13-fold compared to the whole live born pediatric population in Finland (Tables 1 and 2). The proportion (Kaplan–Meier estimate) of patients (53) with a long-bone deficiency having at least one operation, one orthopedic operation, or one operation concerning lower-limb deficiency by 10 years of age was 77%, 67%, and 70% (Fig. 2).
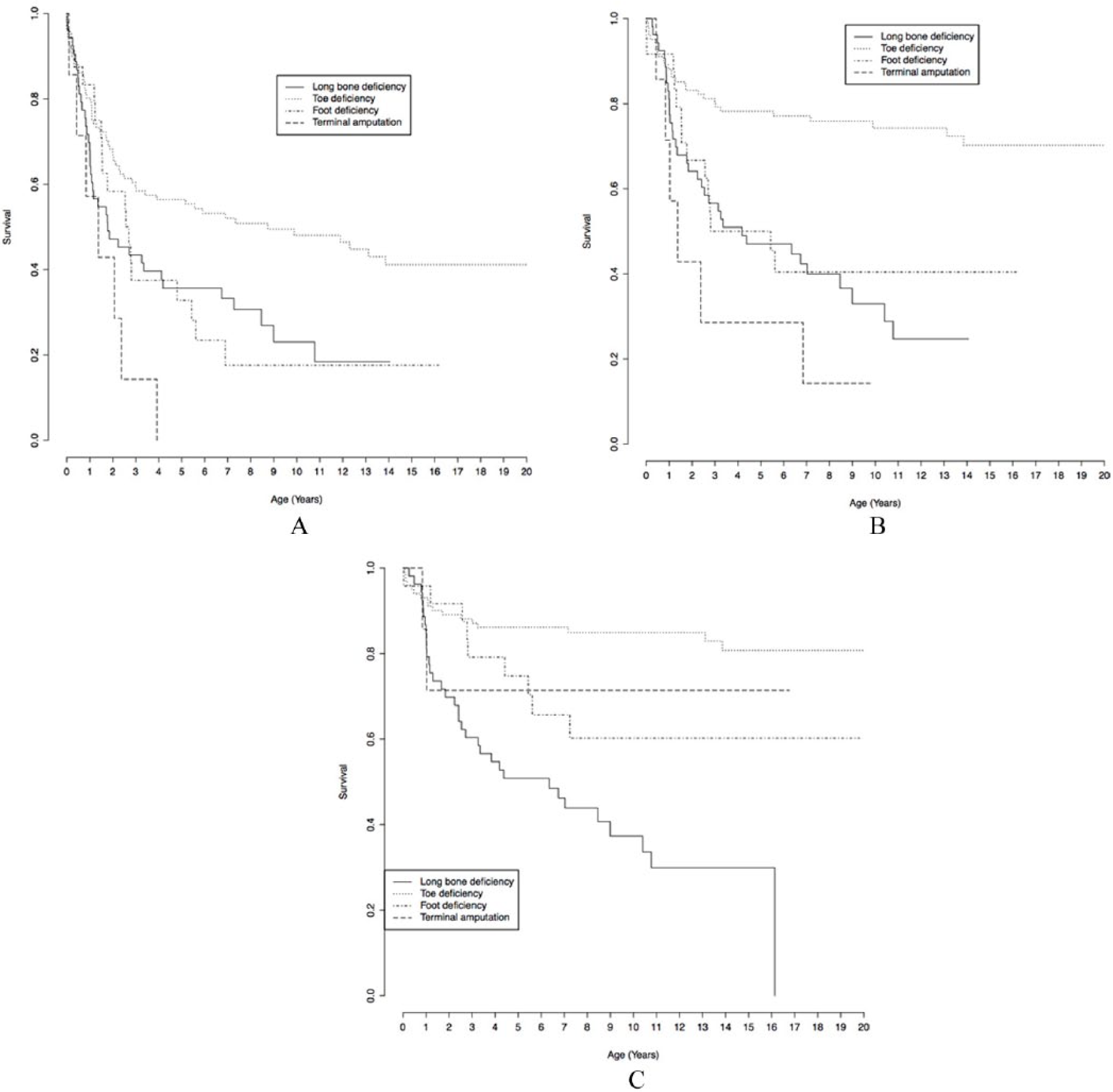
Five- and ten-year operation-free survival in A) all operations, B) orthopedic operations, and C) operations concerning lower-limb deficiency in different patient groups.
The live birth prevalence of PFFD was 0.12 per 10,000 live births in Finland. In total, 8 of the 11 children with PFFD had a median 5.5 operations (range 1−25) per child. Two-thirds (41/62, 66%) of these procedures were orthopedic surgery involving lower limbs. Limb lengthening surgery was done to three children with Aitken class A hips between 2.3 and 6.6 years of age. One child went through two limb lengthening procedures (Table 3).
Long-bone deficiencies; the number of different subtypes, and the number of their orthopedic procedures (lower-limb procedures subcategorized to osteotomies, lengthenings, amputations, epiphyseodesis procedures, soft tissue surgeries, hardware removals, and other procedures).
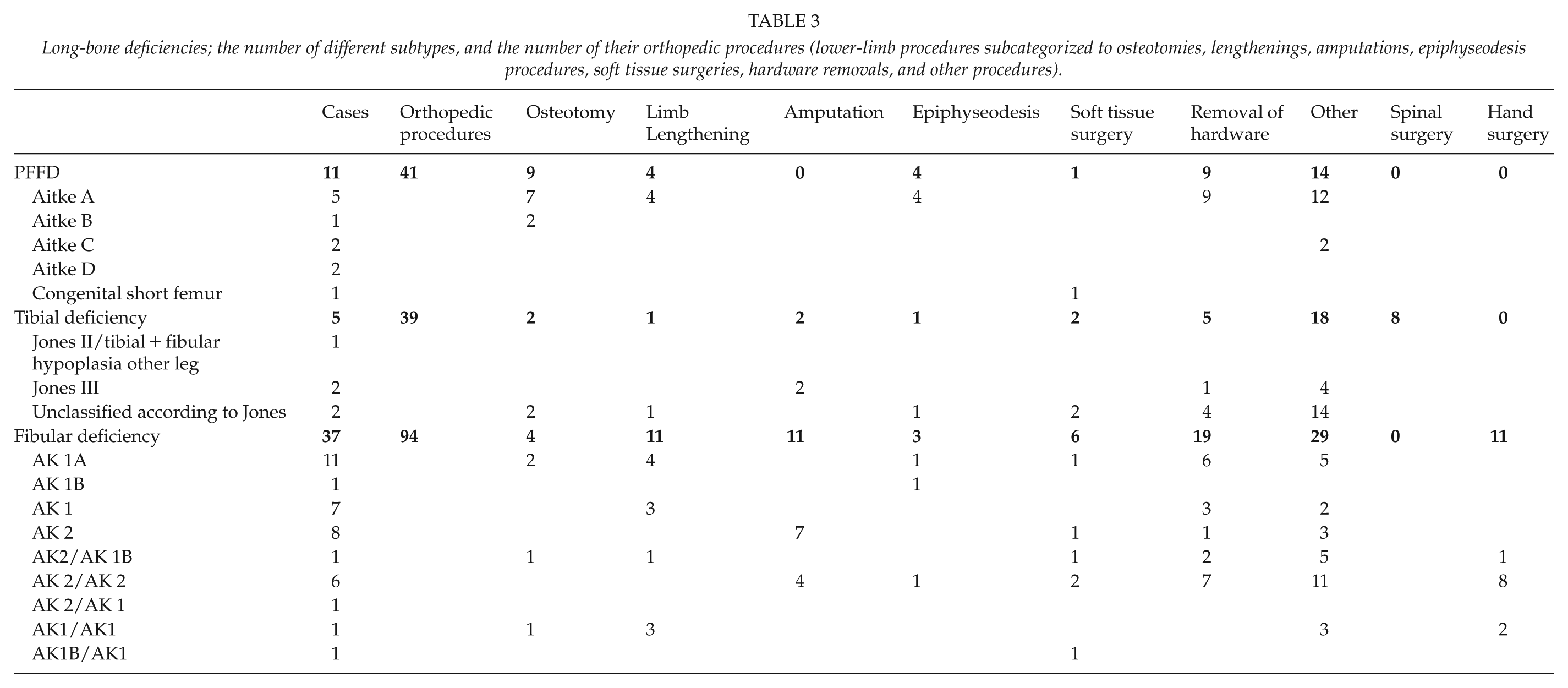
The live birth prevalence of tibial deficiency was 0.05 per 10,000 live births in Finland. All five children with tibial deficiency (1 Jones II, 2 Jones III, and 2 unclear types) had hospital admissions and surgical procedures, of which the majority (39/55, 71%) were orthopedic operations directed to lower limb (31) and spine (8). Two patients with Jones III type tibial deficiency had an amputation (at 1.8 and 3.6 years of age). One limb lengthening was performed in a less than 4-year-old patient with an unclassified type of tibia deficiency (Table 3).
The live birth prevalence of fibular deficiency was 0.39 per 10,000 live births in Finland. In total, 26 of the 37 patients with fibular deficiency (10 bilateral) had a median of three operations (range 1−34) per child. Nearly two-thirds (94/155, 61%) of these operations were orthopedic procedures directed to lower (83) and upper (11) limbs. In total, 10 children with AK2 type deficiency had an amputation at median 1.1 years of age (0.5−2.4). Lengthening was performed in six children (five AK1, one bilateral AK 2/AK 1B) between 1 and 16 years of age (Table 3).
The 24 patients with foot deficiencies (nine split-feet) had annually mean 0.6 (range 0−2) hospital admissions and 1.9 (range 0−6) days in hospital care. This was sixfold compared to the whole live born pediatric population during the study period. In total, 19 of these 24 patients had a median of two operations (range 1−23) per child. More than half (46/84, 55%) of these operations were orthopedic procedures, which were equally divided to lower- (24) and upper-limb (22) surgery performed between 0 and 16 years of age. (Tables 1 and 2) The proportion (Kaplan–Meier estimate) of patients (24) with foot deficiency having at least one operation, one orthopedic operation, or one operation concerning foot deficiency by 10 years of age were 82%, 60%, and 25% (Fig. 2).
The 101 patients with toe deficiencies had yearly mean 0.4 (0−3) hospital admissions and 2.6 (range 0−47) hospital days, which was four- and ninefold compared to the whole live born pediatric population in Finland. Half (54/101, 53%) of these children had a median of two operations (range 1−18) per child. Orthopedic procedures comprised 42% of all operations, of which nearly two-thirds (47/76, 62%) were addressed to lower limbs at mean age of 3.3 (range 0.1−13.9) years (Tables 1 and 2). The proportion (Kaplan–Meier estimate) of patients (101) with toe deficiencies having at least one operation, one orthopedic operation, or one operation concerning toe deficiency by 10 years of age was 52%, 26%, and 19% (Fig. 2).
In 43 (43/185, 23%) cases no hospital admissions were registered. In total, 29 of these patients had a toe deficiency, 7 AK type IA fibular deficiency (follow-up 1.4−8.1 years), 3 PFFD (Aitken A, C, and D one each, follow-up 4.3−11.1 years), three had one missing metatarsal and one had bilateral cleft feet (follow-up 1.3–11.5 years).
Compared to patients with toe deficiency the other groups of patients run bigger risks to be operated (Table 4).
Risk to operations* compared to patients with toe deficiency.
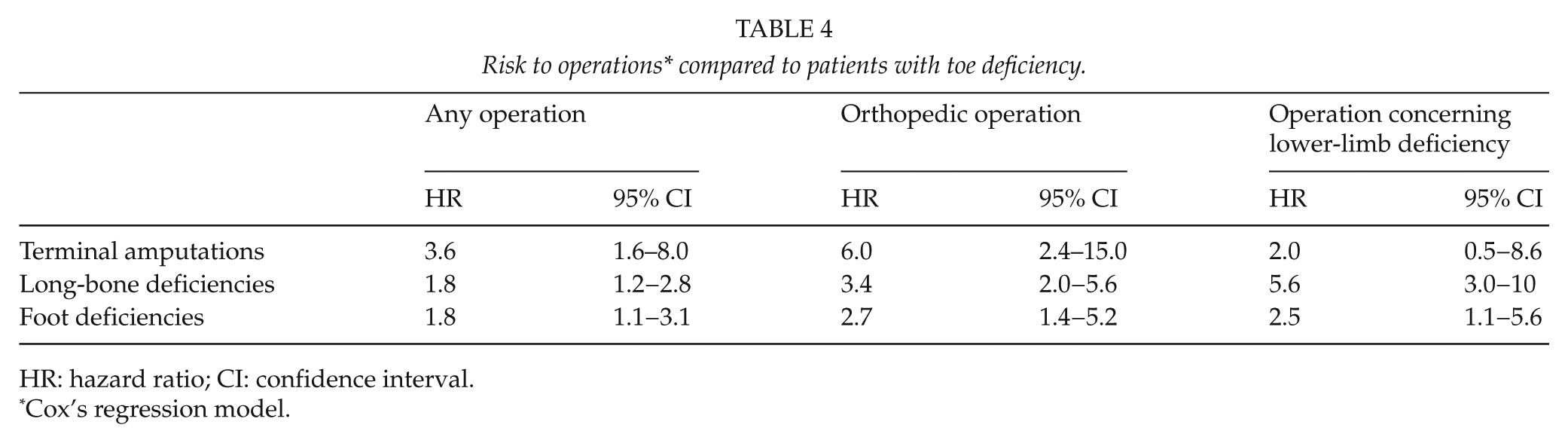
HR: hazard ratio; CI: confidence interval.
Cox’s regression model.
Discussion
According to our study the need of hospital care and the number of orthopedic procedures are multiple-fold compared to the whole pediatric population. There are, to our knowledge, no previous population-based studies concerning treatment of congenital lower-limb deficiencies. It has previously been reported that children with major birth defects are 2.5 times more likely to have hospital care than children without congenital defects (2). Children with orofacial clefts have been calculated to have on average a fivefold number of hospital admissions and an 11-fold length of hospital treatment compared to normal population (5). In addition to children with congenital malformations hospitalization rates are also increased in patients with different syndromes, for example, children with Down’s syndrome, which is associated with a fivefold hospitalization rate compared to the general population (4). Our results show even higher figures for hospital admissions and length of in-patient care in patients with congenital lower-limb deficiency.
The strength of this population-based retrospective study is that the data were drawn from the national Register of Congenital Malformations and the Care Register for Health Care, both with high accuracy and validity and a 100% country-coverage (13, 18, 19). Case data were further validated by examining all available medical records and radiographs. The weakness of this study is the short follow-up time in cases born recently and the fact that some children with a minor lower-limb deficiency might not be reported to the registers.
According to a questionnaire in the United States sent via Amputee Coalition of America (ACA) children with congenital limb deficiency patients treated for an amputation had mean 0.3 stays per child and mean 7.0 total nights at the hospital compared to mean 0.1 stays and mean 2.5 nights in children with congenital limb deficiency without amputation (20). In this study by Weir et al. (20), over 90% of the children had other medical visits to the hospital. In our study the mean number of annual hospital admissions was higher varying between 1.5 in terminal amputations and 0.4 in toe deficiencies. On the other hand, in our study the mean duration of hospital treatment in the four different groups of lower-limb deficiencies (1.9–3.9 days) was lower compared to Weir et al. (20) data. Differences in these studies may be explained due to the accuracy of data collection (questionnaire vs register study). Besides this, the study population is a little bit different in Weir’s and in our study. Weir’s study includes only amputated congenital limb deficiency patients. Also study populations in both studies include very heterogeneous anomalies concerning the difficulty of the anomaly. Patients with limb deficiency also have associated other anomalies and diseases which may affect to admissions and duration of hospital treatment. In addition, differences of health-care systems between countries may have an effect to the results.
Proximal focal femoral deficiency is a rare congenital deformity with a prevalence of 1 in 50,000 (21). In Finland, the live birth prevalence was about the same range, 0.11 per 10,000 live births. PFFD has been traditionally treated with limb lengthening, rotationplasty or amputation (22). In Gillespie’s and Torode’s system group 1 patients (congenital short femur) limb lengthening can be considered. Group 2 (Aitken types A, B, and C) patients are generally treated with prosthesis after surgical limb modification, whereas Group 3 (Aitken type D) patients are managed prosthetically (12, 23). Treatment of the 11 patients in this series was done according to these guidelines: 4/5 of patients with Aitken A had a limb lengthening, whereas none of the four patients with Aitken C or D deficiency had surgical intervention.
Congenital deficiency of the tibia is rarest of the lower extremity deficiencies, with a prevalence of approximately 1 per 1 million live births (9). Our data showed higher live birth prevalence of 0.05 per 10,000 live births in Finland. Tibial deficiency cannot always be classified by the Jones method. The number of non-classifiable cases has varied between 11% and 15% in previous reports (11, 24), which is clearly less than in our study (2/5, 40%). In the series of Fernandez-Palazzi et al. (9), all 22 patients were treated surgically. Clinton and Birch (11) reported two patients whose infant films suggested type 3 deficiency. They were treated with knee disarticulation and the other also with Syme amputation and tibiofibular synostosis. In the data of Spiegel et al. (10), type 2 and 3 cases were treated with Chopart or Syme amputation. We noted two type 3 Jones cases and one type 2 case. All our five patients had surgery; two type 3 cases were treated with amputation. Type 2 deficiency had no orthopedic surgery.
Fibular deficiency is the most frequent long-bone deficiency in lower limbs with an approximate incidence of 7.4–20 per 1 million live births (25, 26). The live birth prevalence was a little bit minor (0.39 per 10,000 live births) in Finland. Patients with fibular deficiency with less than three toe rays and a poor ankle joint have traditionally been treated with amputation and prosthetic rehabilitation. Limb lengthening procedures have been performed in patients with a less severe foot defect and a predicted limb length inequality not exceeding 30% (27). Non-operative treatment has been recommended in mild forms of fibular deficiency in patients with a functional plantigrade foot, and limb length inequality not exceeding 5% (8). Treatment of fibular deficiency in Finland appears to be performed according to these recommendations; all patients with AK type 2 deficiency were treated with an amputation.
Children with congenital partial foot deficiencies rarely need surgical intervention, do not develop contractures, and have minimal functional limitations (28). The goals of the cleft foot treatment are comfort and good function in standard shoes (29). Symptomatic cleft feet are usually treated with accommodative shoe wear or orthoses. Different surgical procedures have been described in few patients (29, 30). In our study, children with foot and toe deficiencies had a clearly lower risk to orthopedic surgery and surgical corrections of the limb deficiency. Eight of the nine children with a cleft foot had hospital admissions, five of them had foot surgery (two bony procedures, two soft tissue procedures, and one amputation (ankle or foot)).
Conclusion
Compared to the whole live born pediatric population there is a higher risk to hospital care in patients with lower-limb deficiency, especially in long-bone deficiencies and terminal amputations. Two-thirds of children with lower-limb deficiency have surgery during the first 10 years of their life.
Footnotes
Acknowledgements
Investigation performed at the Department of Paediatric Orthopaedic Surgery, University of Turku and Turku University Hospital, Turku, Finland.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author I.H. has received research grants from Medtronic International and Innosurge AS. Author J.S. has received grants from the Turku University Hospital and Turku University Foundation. Other authors declare that they have no conflicts of interest.
Ethical Approval
This article does not contain any studies with human participants performed by any of the authors. No ethical board approval needed (registry data). The National Institute for Health and Welfare authorized the use of the health register data in scientific research, as required by the national data protection legislation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was received from the Turku University Hospital and Turku University Foundation. The funding source did not play any role in the investigation. The funds were used only for salary of the corresponding author.