
Abstract
Background and Aims:
Intra-articular injections of viscosupplements have been an option in the treatment of knee osteoarthritis. Platelet-rich plasma is an experimental treatment in osteoarthritis. Previous studies have shown that platelet-rich plasma reduces osteoarthritis symptoms in similar proportions as viscosupplements. The aim of this study was to compare platelet-rich plasma versus viscosupplements in terms of symptoms’ relief and time to arthroplasty.
Material and Methods:
A total of 190 patients included in this retrospective study received either intra-articular injections of platelet-rich plasma (94 patients) or hyaluronic acid (86 patients) between January 2014 and October 2017. Western Ontario and McMaster Universities Osteoarthritis Index, Visual Analogue Scale, and range of motion were measured before injection, at 15 days, 6 months, 12 months, and at last follow-up. We compared outcomes between these two groups using propensity score analysis for risk adjustment in multivariate analysis and for one-to-one matching.
Results:
Hyaluronic acid–treated patients experienced a higher arthroplasty rate (36.0% vs 5.3%, p < 0.001), lower range of motion, worse Visual Analogue Scale and Western Ontario and McMaster Universities Osteoarthritis Index scores, and increased risk of any arthroplasty occurrence (log-rank < 0.001) than platelet-rich plasma patients. Cox proportional hazards analysis revealed a tendency to decrease the risk of knee arthroplasty for the patients treated by platelet-rich plasma (hazard ratio = 0.23, 95% confidence interval, 0.05–1.05, p = 0.058). When the treatment method was adjusted for propensity score in the propensity score–matched pairs (n = 78), we found that platelet-rich plasma group still showed significant improvement over the hyaluronic acid group in arthroplasty rate (12.8% vs 41.0%, p = 0.010), Visual Analogue Scale and Western Ontario and McMaster Universities Osteoarthritis Index scores, but not in the range of motion, during the mean follow-up of 16.7 months.
Conclusion:
Intra-articular injections of platelet-rich plasma associated with better outcomes than hyaluronic acid in knee osteoarthritis. Platelet-rich plasma might prolong the time to arthroplasty and provide a valid therapeutic option in selected patients with knee osteoarthritis not responding to conventional treatments. Further larger studies are needed to validate this promising treatment modality.
Keywords
Background and Aims
Knee osteoarthritis (OA) is the most common degenerative joint disease and a significant burden to the society (1). It is a debilitating and progressive disease that often leads to arthroplasty when non-operative treatments fail (1). The incidence of OA is increasing and studies predict that joint replacement surgery demand will grow rapidly (2–4).
Non-operative treatments include non-steroidal anti-inflammatory drugs (NSAIDs), weight loss, dietary supplements such as glucosamine and chondroitin sulfate, topical agents, intra-articular injections of corticosteroids, and/or hyaluronic acid (HA) (5–8). The role of glucosamine and chondroitin sulfate is still debated (7, 8). None of these treatment options can modify the natural course of the disease, but can instead alleviate the symptoms (8). Intra-articular injections of corticosteroids and/or HA viscosupplementations are often the last treatment options before arthroplasty.
Single intra-articular injection of HA is expensive and did not diminish the inflammatory process in the joint, causing sometimes adverse reactions (9–11). Viscosupplementation seems to delay the need for joint replacement surgery up to 3.6 years compared to placebo, when multiple injections are given to patients, and the arthroplasty survivorship is higher in up to 5-year follow-up (12, 13).
Intra-articular platelet-rich plasma (PRP) treatments aim to balance the pro-inflammatory and catabolic state in OA-affected joint toward anti-inflammatory and anabolic state, which is thought to reduce patients’ symptoms (14–18). Effects of the intra-articular treatments usually decline after 6–12 months, but a trend of decline in pro-inflammatory cytokines has also been observed, further reinforcing the anti-inflammatory properties of PRP in OA symptoms’ alleviation (19, 20).
Both HA and PRP have demonstrated to provide pain relief; however, there is no consensus whether one of them provides better outcomes (19–22). In addition, in the available studies, although some of them randomized, the comorbidities, types of OA, and treatment factors vary, which can affect the outcomes. Furthermore, the length of follow-up is very heterogeneous among the published studies, further complicating interpretation of these data (14, 15, 20, 21). Thus, the comparison of these two treatment modalities is difficult due to problems with forming comparable groups and to avoid confounding factors (20).
To overcome these issues, we analyzed our long-term results of knee injections using PRP and HA by adjusting the baseline differences between the two groups using propensity score analysis. We hypothesized that patients treated with PRP would have less arthroplasty operations and better outcome measurement scores than patients treated with HA.
Thus, the aim of this study was to investigate and compare the effects of PRP versus HA in the treatment of mild to moderate knee OA, in terms of arthroplasty avoidance and symptoms relief.
Material and Methods
We retrospectively evaluated all consecutive patients who received knee injections of PRP or HA due to knee OA between January 2014 and October 2017 at the Welfare District of Forssa, Finland. The clinical investigation for this study was conducted in accordance with the ethical principles of the World Medical Association Declaration of Helsinki. This study was approved by the Institutional Review Board, and individual informed consent was waived because the source data were de-identified.
The outcomes of patients who received knee injections of PRP (experimental group) were compared with those of patients who received HA due to knee OA (control group). Patients with major systemic disorders (hematological diseases, infections, immunodeficiency, active or fulminant rheumatoid disease), major symptomatic hip arthrosis at the same side of the knee, and pregnancy or possible pregnancy were excluded from the study. Inclusion criteria were age between 18 and 90 years, knee OA diagnosed by radiographic imaging, pre-intervention pain Visual Analogue Scale (VAS) of 30–100, and Kellgren–Lawrence (KL) grade 1–3 OA. Patients who have received any other kind of intra-articular injections or oral medication other than paracetamol/NSAIDs were excluded from this study.
Patients were followed up with physical examination, comprehensive of Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire, VAS, and range of motion (ROM) of the knee.
Data were meticulously collected both from a prospectively maintained departmental database and from the patients’ electronic medical records. Patients’ demographics, treatment modality, frequency, and knee OA grades were analyzed, and clinical outcomes were directly compared between the experimental and control groups. Patients were assessed for their symptoms before injections, at 15 days after treatment, at 6 months, at 12 months, and/or at the last follow-up. The primary outcome measure was the occurrence of any knee arthroplasty at follow-up after intra-articular injections. Secondary outcome measures included adverse events, VAS, WOMAC, and ROM of the knee.
The PRP group received three intra-articular injections at 10–14 days interval (defined as one treatment term). Commercial Glo PRP kit (GloFinn Corporation, Salo, Finland) was utilized in manufacturing of autologous PRP from patients’ whole blood. A specifically trained nurse drew up to 10 mL of patients’ whole blood in a syringe and the whole blood was centrifuged 5 min at 1200 r/min. Excess red blood cells (RBCs) were removed between centrifugations. The final product contained four to eight times higher concentration of platelets compared to the whole blood. One typical injection consisted of approximately 5 mL of PRP. Five patients received more than one treatment term and, thus, more than three injections, while three patients received less than three injections all together.
The HA group had received either single intra-articular injection or three injections at 1-week interval (defined as one treatment term). A total of 33 patients in the HA group received more than one treatment. HA products utilized were high-viscosity and high-molecular-weight products: Hylan G-F 20 (Synvisc One®, Naarden, Netherlands, 6,000,000 Da, 48 mg/6 mL injection) or sodium hyaluronate (Arthrum75®, Chartres, France, ⩾2,800,000 Da, 75 mg/3 mL injection). Five patients received low-molecular-weight HA (Hyalgan®, Abano Terme, Italy, 500,000–730,000 Da, 20 mg/2 mL injection). The follow-up was calculated from the time of the first injection until the last control.
Statistical Analysis
Continuous variables were reported as the mean ± standard deviation. Pearson’s chi-square test, Fisher’s exact test, and the Mann–Whitney test or t-test were used for univariate analysis, as appropriate.
Logistic regression with enter selection was performed to calculate the likelihood of patients to be included in either the PRP group or HA group. Hosmer–Lemeshow’s test was used to assess the regression model fit. Variables included in the regression model are shown in Table 1. The calculated propensity score was employed for one-to-one matching as well as to adjust for other variables in estimating their impact on the postoperative outcomes (23). One-to-one propensity score matching between study groups was done using the nearest neighbor method and a caliper of 0.2 of the standard deviation of the logit of the propensity score (24). Continuous outcomes were compared in the propensity score–matched (PSM) groups using paired t-test or Wilcoxon signed-rank test as appropriate; differences in proportions were compared using the McNemar’s or binominal test as appropriate.
Baseline characteristics of patients who underwent intra-articular injections of PRP or HA for knee OA.
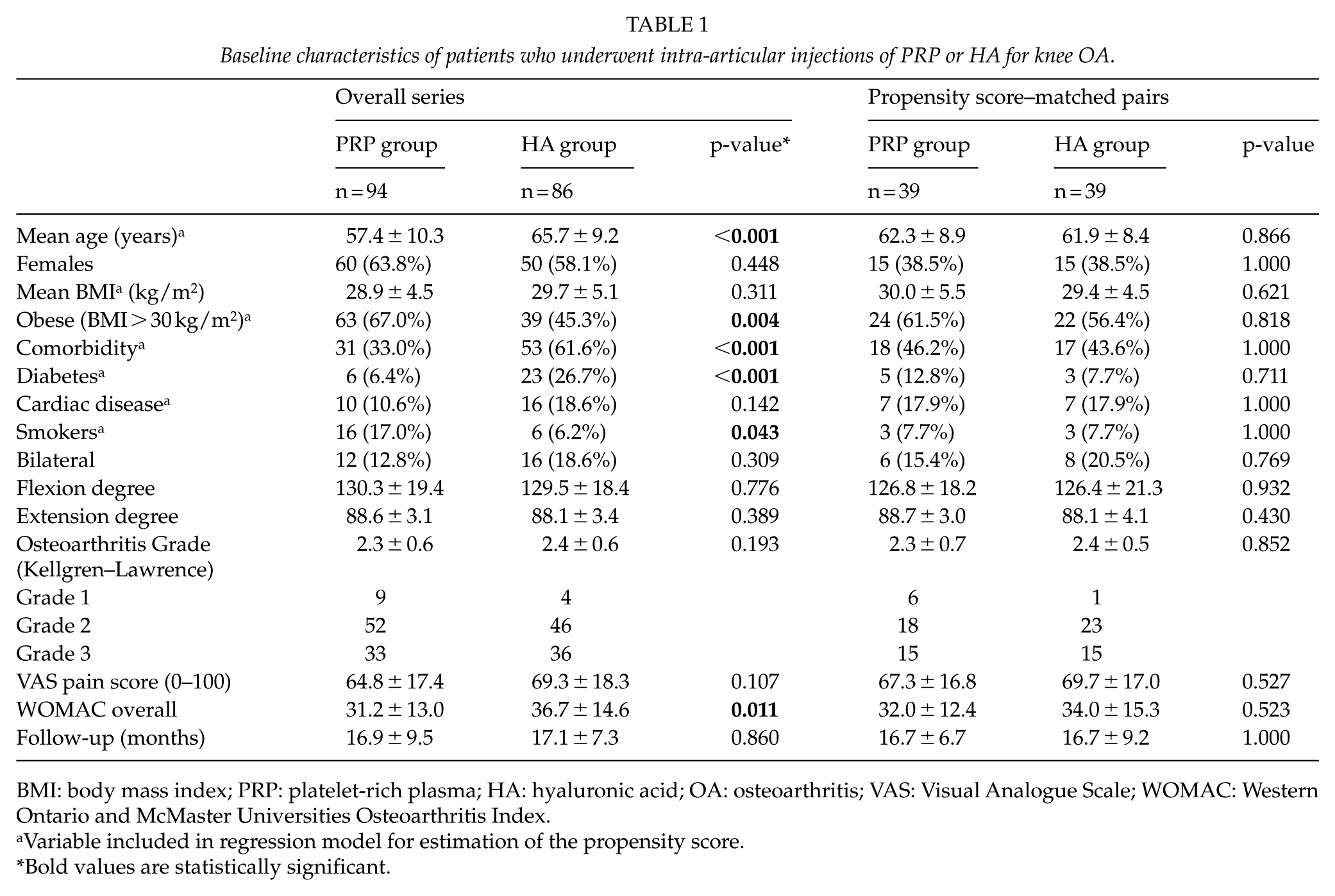
BMI: body mass index; PRP: platelet-rich plasma; HA: hyaluronic acid; OA: osteoarthritis; VAS: Visual Analogue Scale; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index.
Variable included in regression model for estimation of the propensity score.
Bold values are statistically significant.
Long-term outcome was assessed by Kaplan–Meier’s methods in the overall series and in the propensity-matched pairs with the log-rank test and the Cox proportional hazards method with log minus log test. All p-values <0.05 were considered statistically significant. All analyses were carried out using SPSS statistical software (IBM SPSS Statistics, version 23, Armonk, NY).
Results
A total of 180 consecutive patients, treated for knee OA between 2014 and 2017, were included into this study. Of them, 94 patients (52%) received PRP injections while 86 (48%) received HA injections. Baseline characteristics are outlined in Table 1, showing significant difference in age, obesity prevalence, comorbidity, diabetes, and overall WOMAC score, which were significantly higher among HA group. Mean follow-up was similar in both groups and over 17 months. Similar adverse events occurred in both groups, while the number of injections was significantly higher among PRP group (PRP 3.2 ± 1.2 vs HA 1.7 ± 0.9, p < 0.001).
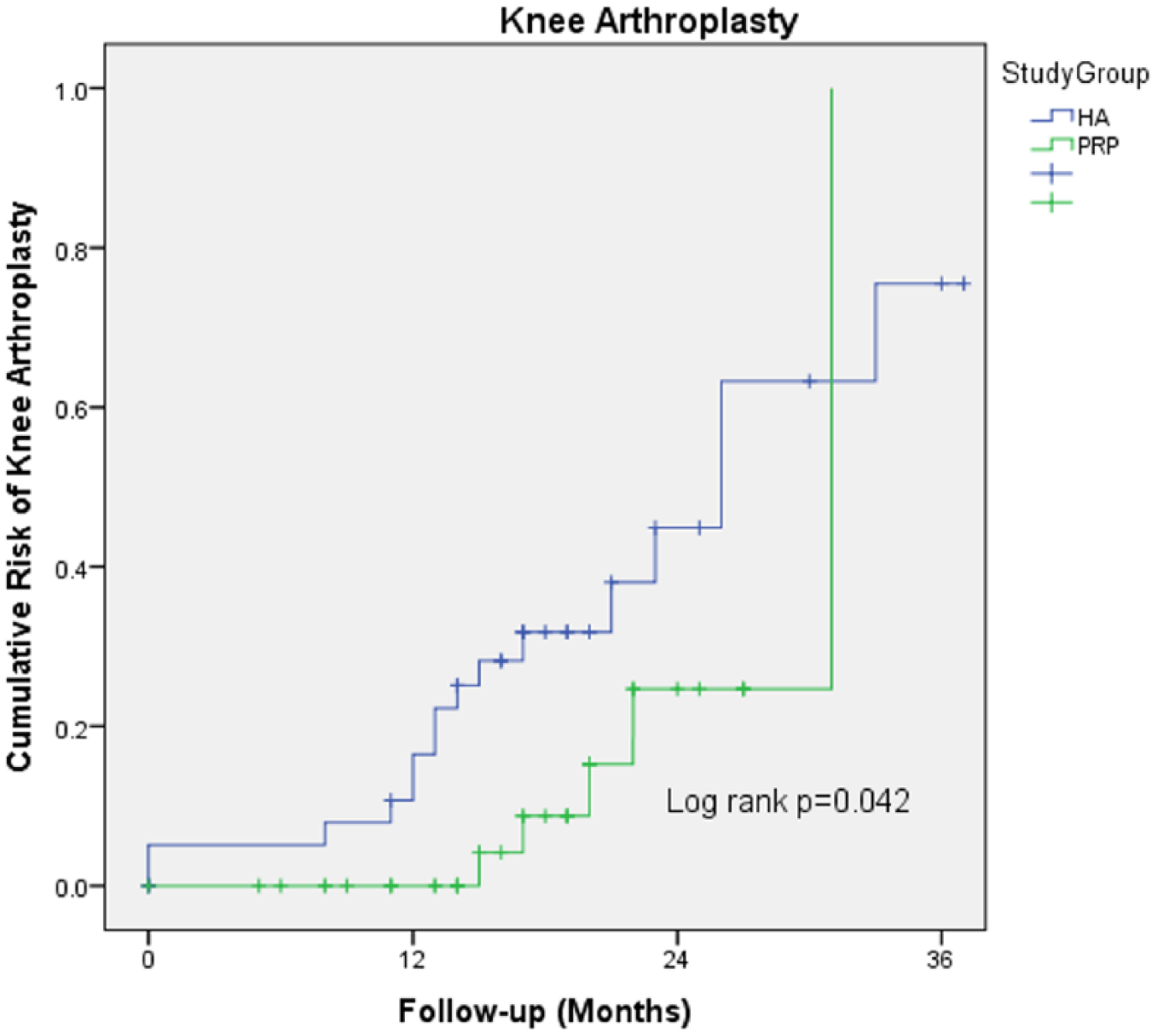
The HA patients experienced a more than fourfold higher odds for arthroplasty rate (36.0% vs 5.3%) than the PRP patients (odds ratio (OR), 4.4; 95% confidence interval (CI), 1.9–10.1; p < 0.001, Fig. 1 and Table 2). Cox proportional hazard model including confounding factor identified by univariate analysis revealed a tendency to decrease the risk of knee arthroplasty for the patients treated by PRP (hazard ratio (HR) = 0.23; 95% CI, 0.05–1.05; p = 0.058; Fig. 2).
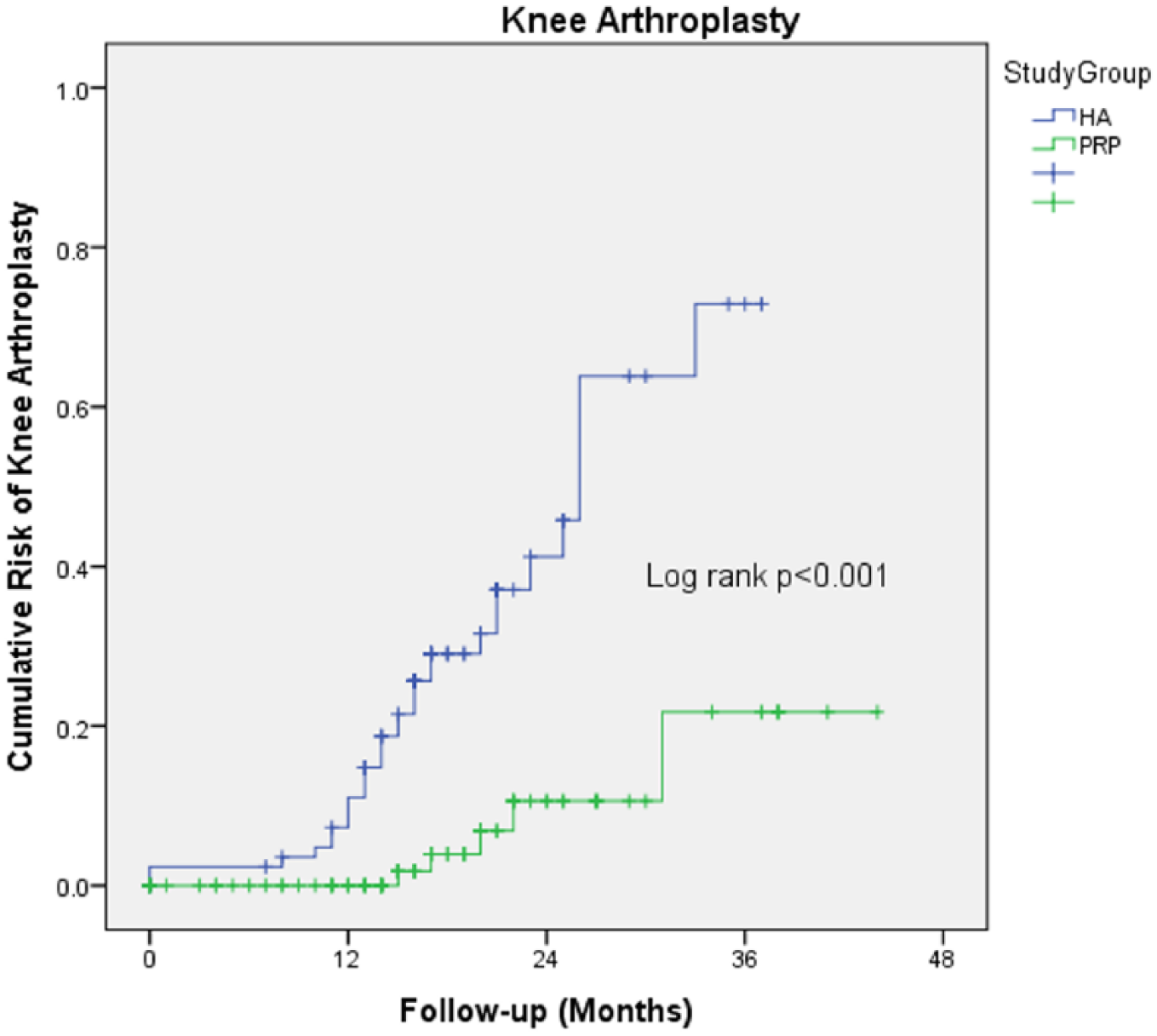
Kaplan–Meier curves of any arthroplasty occurrence for patients who underwent intra-articular injections of PRP or HA for knee OA.
Outcomes of patients who underwent intra-articular injections of PRP or HA for knee OA.
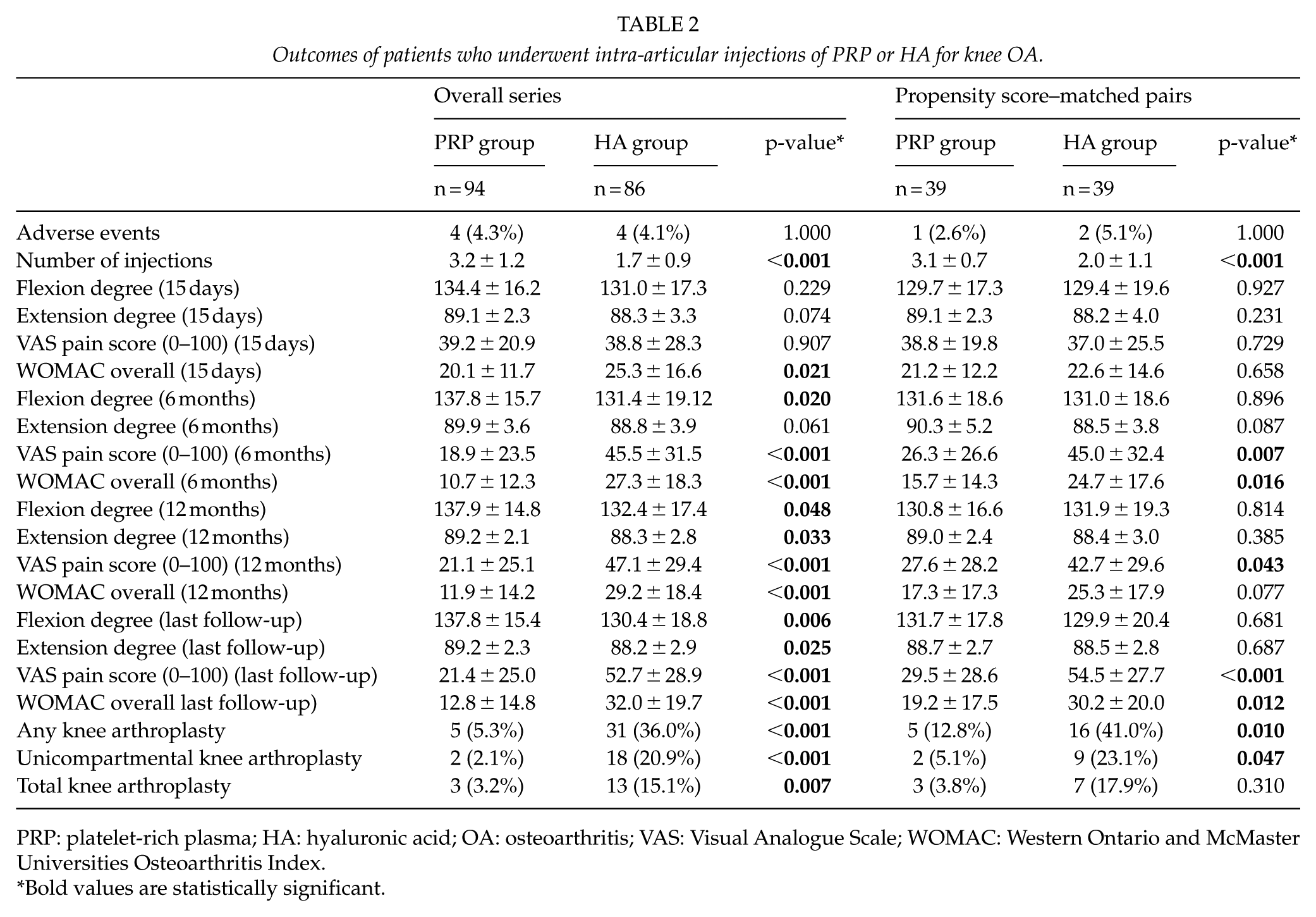
PRP: platelet-rich plasma; HA: hyaluronic acid; OA: osteoarthritis; VAS: Visual Analogue Scale; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index.
Bold values are statistically significant.
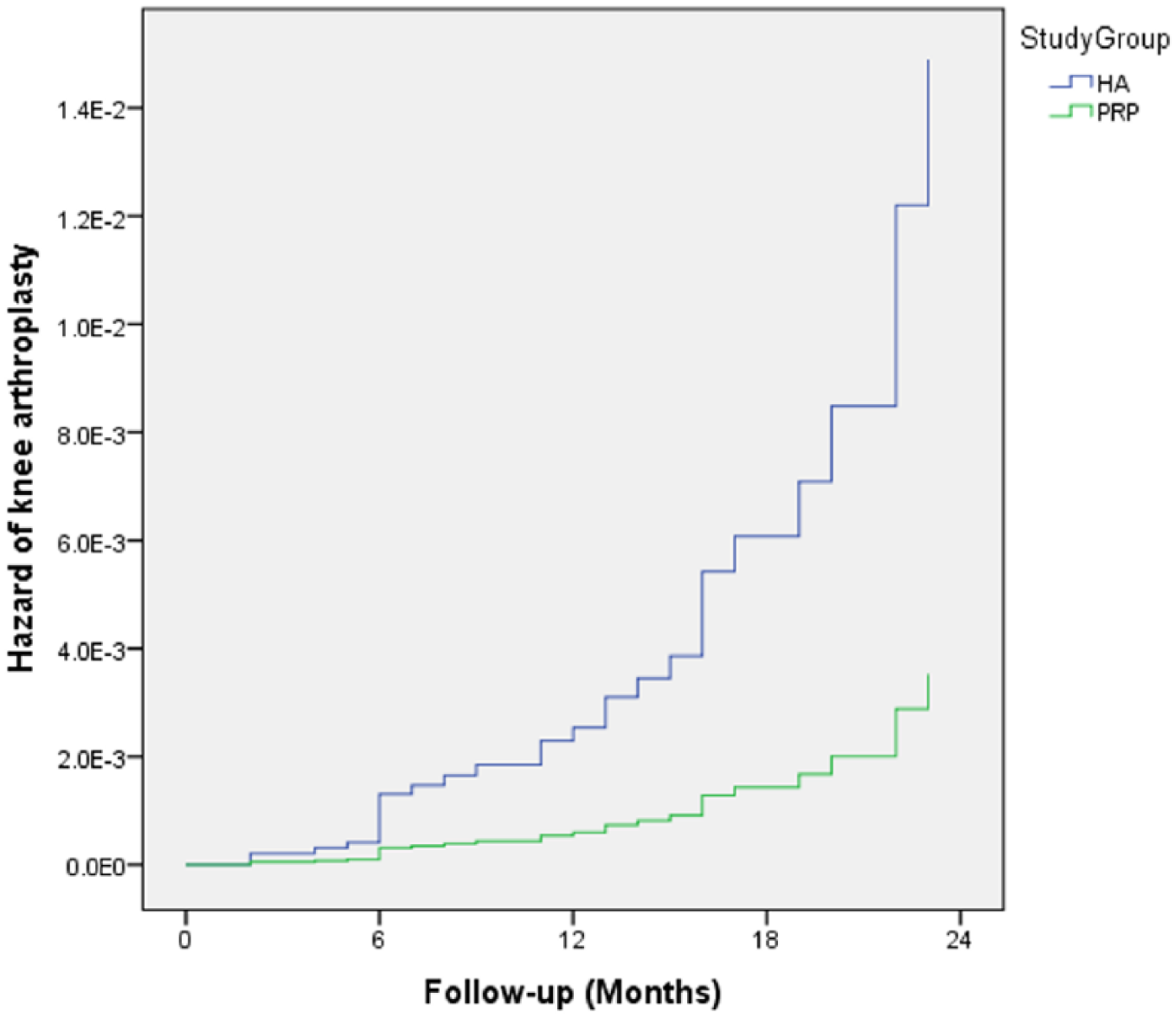
Cox proportional hazards estimates of knee arthroplasty according to intra-articular injections of HA or PRP for knee OA (HR = 0.23, 95% CI, 0.05–1.05, p = 0.058).
Among secondary outcomes, VAS pain score showed a statistically significant difference favoring PRP group at 6 months, at 1 year, and at last follow-up. Similarly, WOMAC overall scores and ROM were significantly better at all the treatment intervals among PRP patients (Table 2, Figs 3). Kaplan–Meier curves showed a statistically significant difference in risk of any arthroplasty between the two groups (Fig. 1).
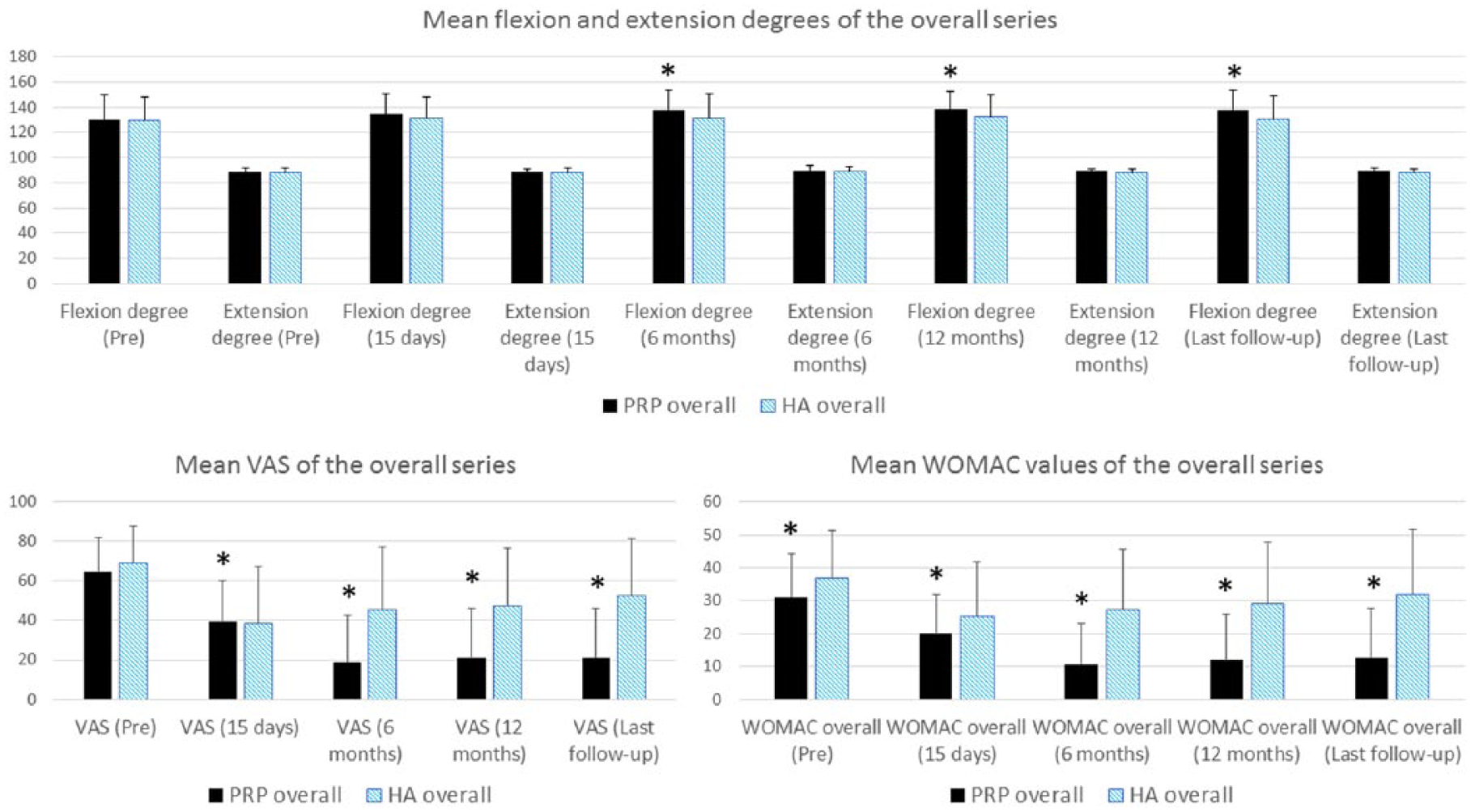
Mean values of range of motion, VAS, and WOMAC in the overall series of PRP and HA groups. ROM values expressed in extension 0 to 90 degrees and flexion 0 to 155 degrees. Columns with a statistically significant difference are marked with asterisk (*).
The propensity score yielded 39 matched pairs without any differences in baseline characteristics (Table 1). The number of injections was still significantly higher among PRP group (3.1 ± 0.7 vs 2.0 ± 1.1, p < 0.001), while the arthroplasty rate was significantly higher among HA patients even when matched through the propensity score (PRP 5 vs HA 16, p = 0.010).
Furthermore, a statistically significant lower VAS pain score was observed in PRP group at 6 months, at 12 months, and at last follow-up. Similarly, WOMAC overall score showed a statistically significant difference at 6 months and at the last follow-up favoring PRP over HA patients (Table 2, Fig. 4). In contrast, we did not detect any statistically significant differences in ROM (extension and flexion degree) at any follow-up point in the PSM group (Table 2, Fig. 4). Kaplan–Meier curves showed a statistically significant difference in risk of any arthroplasty between the two matched paired groups (Fig. 5).
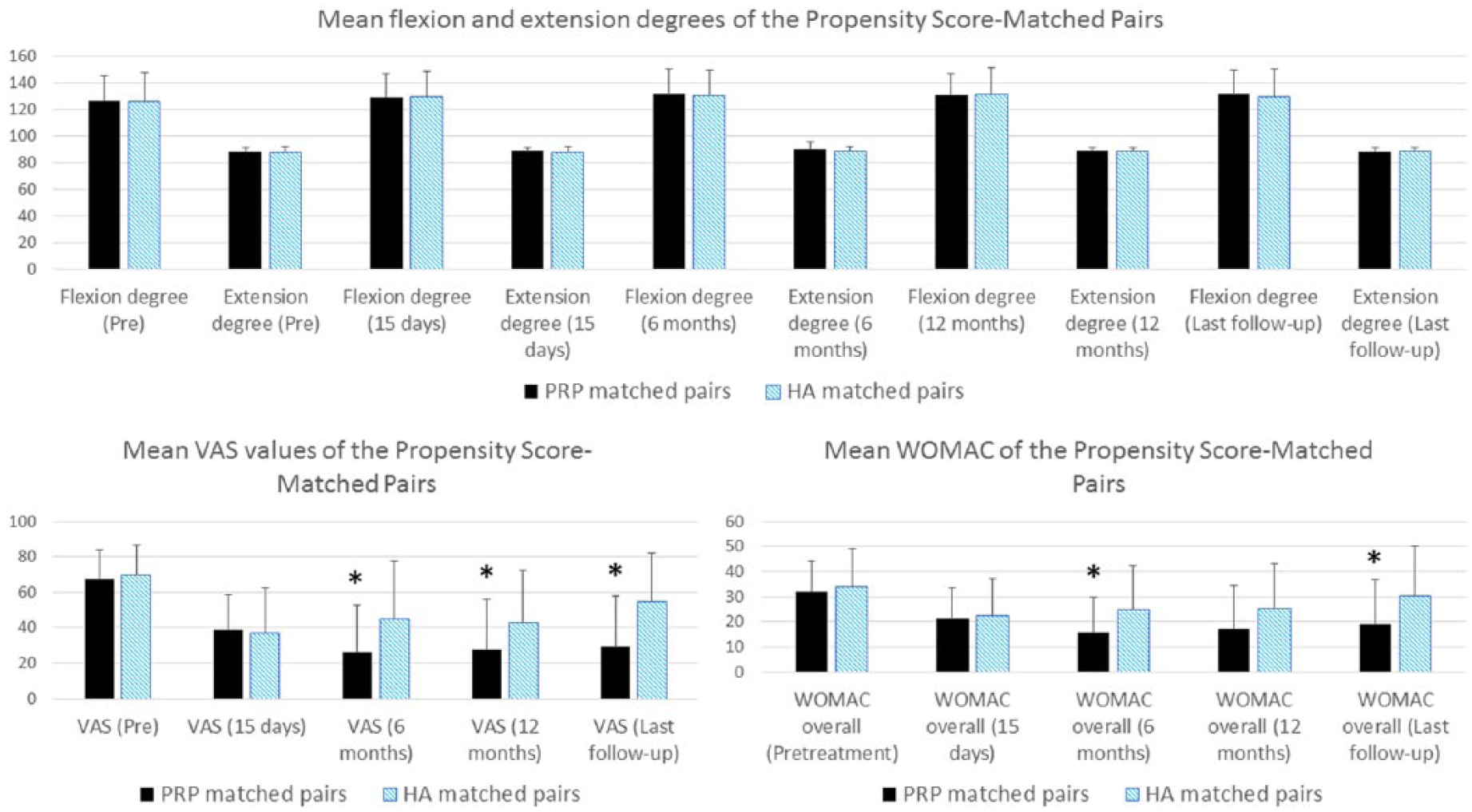
Mean values of range of motion, VAS, and WOMAC in the propensity score–matched pairs of PRP and HA groups. ROM values expressed in extension 0 to 90 degrees and flexion 0 to 155 degrees. Columns with a statistically significant difference are marked with asterisk (*).
Kaplan–Meier curves of any arthroplasty occurrence for patients who underwent intra-articular injections of PRP or HA for knee OA after propensity score matching.
Discussion
In our study, PRP outperformed HA in both the overall patient series and in the PSM series in symptom alleviation and in terms of avoiding the knee arthroplasty. Our results are consistent with the current literature, providing that PRP results in a statistically significant improvement in major pain and functional outcome measurements when compared to HA (15–22, 25–27). To the best of our knowledge, this is the first study to report differences on the risk of arthroplasty between autologous PRP versus HA in knee OA, and the first PSM study to compare PRP to HA.
There has been only one previous study about arthroplasty delay involving PRP by Turajane et al. (22) including 60 patients. They compared intra-articular injections of autologous activated peripheral blood stem cells (AAPBSC) with PRP added growth factors, and HA along with arthroscopic mesenchymal stem cells versus the same combination without the added growth factors versus only intra-articular HA. They found that AAPBSC groups performed better than HA alone; however, they concluded that further research on the matter is required (22). Our study demonstrated a statistically significant difference in delaying knee arthroplasty favoring patients treated with autologous knee intra-articular injections of PRP versus high-molecular-weight HA.
There have been some reports indicating that PRP may not be superior to HA (19, 28). Filardo et al. (28) did not find any statistically significant differences between PRP and HA groups in the International Knee Documentation Committee (IKDC) subjective score and VAS score (28). Cole et al. (19) found a statistically significant difference favoring PRP in IKDC and VAS score at 24 and 52 weeks. However, no statistically significant differences between PRP and HA in WOMAC pain score were found at any follow-up point (19). Possible confounding factors in the studies were use of frozen PRP surplus and statistically significant age difference between the groups, different PRP protocols utilized, and statistically significant difference of body mass index (BMI) between the groups (19, 28).
Randomized controlled trials (RCTs) showed that multiple intra-articular PRP injections are statistically significantly more effective in early knee OA than placebo, HA or single injections of PRP (14, 25–27). A meta-analysis of RCTs by Shen et al. (20) concluded that PRP injections reduce knee pain and improve WOMAC scores better than other intra-articular injections (including HA, saline, corticosteroids, and ozone) up to 12 months (20). In our study, the VAS score showed similar results favoring the PRP group at 6 months, 12 months, and last follow-up, even after propensity score analysis. In addition, our WOMAC outcomes corroborate Cerza et al.’s study (14), which demonstrated superior clinical outcomes for PRP against HA with WOMAC scores. Our results verified the ones of Shen et al.’s (20) meta-analysis, but with a longer follow-up (20).
We did not find significant differences in ROM between the groups and this is probably due to the mild to moderate grade of OA in the study populations, as joint becomes truly rigid in the later stages of OA. Adverse effects were meticulously documented in our study, but we did not find serious adverse effects in either of the groups. The adverse effects recorded were mostly prolonged pain of the injection site (up to 5 days) or mild effusion post injection. Previous studies found no serious adverse effects in treating patients with intra-articular PRP injections (20, 25–28).
Strengths of this study are the reasonable number of patients and relatively long follow-up. The propensity-score matching also improves the reliability of the study by reducing the demographic differences between the groups. The multivariable regression using propensity score analysis allowed the opportunity to control for selection bias and confounding by treatment indication. Particularly, this is important when there is a relatively large number of confounders compared with the number of outcomes (29). This unique approach of using propensity scores permitted us to consider not only the factors that affected outcome but also the factors that contributed to selection for the type of injection.
A limitation of this study is the retrospective view point. A true randomization of the patients would further reduce the possible bias concerning the patient selection. The PRP group in the overall series were younger, more obese, and smoked more often than HA groups. However, the HA group were older, had more comorbidity, and had greater initial WOMAC overall score. The PRP group received significantly more injections than the HA group, due to the treatment protocol inherent to these two different methods, and we consider it irrelevant. In addition, due to the lack of data, we have no information about the amount of oral medications used for arthrosis, although paracetamol and NSAIDs were mostly prescribed. Nonetheless, patients who have received any other kind of intra-articular injections or oral medication other than paracetamol/NSAIDs were excluded from this study.
We lost over 50% of the total patients enrolled to this study during the propensity score analysis. This is probably due to the physician leaning toward HA, rather than PRP, when treating heavily symptomatic OA patients. HA has a longer history and it has been successfully utilized before, which may lead to a bias of continued use in uncertain situations such as heavily symptomatic OA. Nevertheless, propensity score analysis has its pitfalls and weaknesses due to its methodology, as there might be some variables not included in the propensity score which might have affected the treatment selection and outcomes (29).
Reduction of symptoms and slowing the disease progression are the goals of treatment (30). A recent consensus statement included HA as one method in achieving the goals (30). In this view, PRP may prove to be a viable alternative to HA when patients are not yet ready for arthroplasty. A larger RCT study with longer follow-up is required to determine the length of arthroplasty delay. Moreover, defining the optimal PRP injection interval in order to provide the maximum efficacy would be of great interest. It is still unknown whether PRP is a disease-modifying treatment option in OA, as it is still a progressive disease that will eventually ruin the affected joint.
Conclusion
This study demonstrated that PRP intra-articular knee injections compared to HA reduce the odds of knee arthroplasty in mild to moderate knee OA patients. A significant improvement in pain at 6 months and thereafter in the PRP group versus HA group was found. Similarly, a statistically significant improvement was also detected in WOMAC overall score at 6 months and at the last follow-up. A trend toward improvement in WOMAC overall was observed at 12 months. Our results suggest that autologous PRP may be an effective treatment for patients with mild to moderate knee OA.
The authors suggest that PRP may be used as an alternative to high-molecular-weight HA in mild to moderate graded symptomatic knee OA as it seems to reduce the odds of early arthroplasty and alleviate symptoms better than other injection therapies. In our experience, three injections given at 2-week interval as one treatment term may be optimal. Treatment terms might be repeated when symptoms arise again or until symptoms are not alleviated. Arthroplasty should be considered when neither HA nor PRP reduce the symptoms. Longer follow-up studies to further clarify the role of PRP in arthroplasty delay are warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.