
Abstract
Background:
Intra-articular hyaluronic acid (HA) injection is used in management of knee, hand and hip osteoarthritis. While HA injection is included in the list of evaluated therapies, its efficacy and optimum dosing still have no consensus. This study was conducted to explore the possibility of using single injection HA to increase patient convenience while maintaining the therapeutic efficacy.
Methods:
We present a prospective, open label, non-blinded, randomized controlled trial performed in accordance with guidelines in principles of good clinical practice. Block randomization was done for patients to receive either single 5 ml GO-ON injection or the conventional three injections of 2.5 ml GO-ON at weekly interval. Baseline Western Ontario McMaster University Osteoarthritis (WOMAC) scores were evaluated and recorded. All subjects were re-evaluated at 3 months and the WOMAC score recorded again as primary end points. Data analyses were performed with IBM SPSS Statistics for Windows software (version 21.0, IBM Corp, Armonk, New York, USA).
Results:
In the cohort of 127 patients, 33 were males and 94 females. The mean age was 59.1 years (standard deviation (SD) = 7.25) in single injection arm and 60.1 years (SD = 7.72) in triple injection arm. The two groups were recorded to have no significant difference in age (p = 0.46
Conclusion:
The study shows single 5 ml dose regime comparing well with conventional three doses of 2.5 ml of intra-articular GO-ON HA injected at weekly intervals and confirms good efficacy, tolerability and safety of single larger dose of GO-ON knee intra-articular injection.
Introduction
Hyaluronic acid (HA) is a glycosaminoglycan constituent of synovial fluid and cartilage in matrix in normal knee. In 1997, the US Food and Drug Administration approved the use of intra-articular HA products for the treatment of pain in osteoarthritis (OA) of the knee in patients who have failed to respond adequately to conservative non-pharmacological therapy. While HA injection is included in the list of evaluated therapies, the efficacy of HA is not conclusively established in meta-analyses. 1 –4
In OA, the molecular weight (MW) and concentration of natural/endogenous HA are decreased. 5 The available exogenous HA formulation for the treatment of knee OA may vary in MW, origin and technique of administration.
Previous studies have shown that repeat courses of the exogenous HA are safe and effective in the treatment of pain associated with OA of the knee. 6
Trigkilidas and Anand (2013) reported a systematic review on the effectiveness of HA intra-articular injections in managing OA knee pain and found that HA injections have a modest effect on early to moderate knee OA. The most effective outcome was seen at 6–8 weeks post injection period. 7
The therapeutic effect of multiple knee intra-articular GO-ON injections has been tested in a number of clinical trials. 8,9 The objective of this study was to compare the equivalence in the efficacy of two different doses/strength of an intermediate MW preparation GO-ON (i.e. single 5 ml vs. three 2.5 ml injections at weekly interval) at midterm follow-up, that is, at 3 months. GO-ON 2.5 ml prefilled syringe at a concentration of 10 mg/ml was supplied by the company for the trial purpose.
Materials and methods
This prospective, open label, non-blinded, randomized controlled trial was performed in a single centre
GO-ON (Meda Groups, Sollna, Sweden) is a preparation of sodium hyaluronate obtained by fermentation from Streptococcus equi., with an intermediate MW (range 800 k–1500 kDa), presented in 2.5 ml prefilled syringe at a concentration of 10 mg/ml. It is approved by the Malaysian National Pharmaceutical Board for the management of OA in cycles of 3–5 weekly injections.
Before inclusion, patients were evaluated for fulfilment of the entry criteria. Inclusion criteria required patients of either gender, aged from 40 to 80 years, 10 to be otherwise healthy and ambulatory and diagnosed with either unilateral or bilateral knee OA. Diagnosis of OA was made on radiological criteria. We included patients with Kellgren–Lawrence grade I to III radiographic scores on standard knee radiographs done within 6 months of our enrolment date (Kellgren–Lawrence grade III is included as it is quite often the presenting stage, due to lack of awareness and belief in alternative/traditional medicine). Patients also should not have had knee intra-articular viscosupplement injections in 6 months prior to enrolment.
Exclusion criteria included females attempting to conceive, patients who have participated in another clinical trial within 90 days prior to randomization, severe hip OA, known allergy or hypersensitivity to HA, significant systemic illnesses and patients planned for total knee replacement surgery at target joint.
Informed consent was sought from all eligible subjects prior to randomization. A computer generated list of random numbers was used. All subjects were randomized with a 1:1 allocation using block randomization.
At every initial visit, the allocation sequence was hidden from the physicians who screen the patient. When the patient’s eligibility was confirmed, the physician will be informed by the study coordinator as to which arm the patient belongs, that is, single or triple injection, based on the randomization list generated. Only the study coordinator, independent from patient assessment and recruitment, had access to the randomization list.
After randomization, baseline Western Ontario McMaster University Osteoarthritis (WOMAC) questionnaires were recorded and then were generated in computer by independent research assistant as pre-WOMAC scores. Subsequently, patients were given appointment for knee viscosupplement injection according to the assigned arm of randomization.
The GO-ON knee intra-articular injections were injected as an outpatient procedure in the orthopaedic clinic treatment room under aseptic precautions. After injecting local anaesthesia and performing an arthrocentesis, GO-ON HA was injected using 18 gauge needles. Standard technique of arthrocentesis and intra-articular injection was followed. During the procedure, optimal knee joint positioning and needle insertion site were determined according to clinician’s judgement after taking into consideration the knee anatomy and pathologic condition.
Patients were allowed to continue taking their usual doses of analgesic medications and concomitant rescue medications, and physiotherapy was allowed. During follow-up at 3 months, all subjects were re-evaluated clinically and the WOMAC score recorded again as primary end points. Efficacy of the treatment in both arms was measured as the mean change in WOMAC score from baseline.
Clinical evaluation for any adverse reactions was conducted after each knee intra-articular injection in both groups. Any systemic adverse events or septic complication requiring hospital admission were also recorded and managed accordingly.
Sample size calculation
The sample size estimation was based on mean difference in WOMAC score at baseline and 3 months. The sample size was computed based on the assumption of an anticipated overall difference of 12, standard deviation (SD) of 21 and dropout rate of 20%. Type 1 error was set at 0.05. A resulting sample size of 120 patients (60 patients per group) provided greater than 80% power to detect a difference between the single injection group and triple injection group.
Statistical analysis
The analyses were performed with IBM SPSS (version 21.0, IBM Corp, Armonk, New York, USA). Descriptive statistics was analysed for age, gender and Kellgren–Lawrence radiological grades between single injection and triple injection group.
Categorical data collected for gender and Kellgren–Lawrence radiological grades were presented as frequencies and percentage. Numerical data of age which are normally distributed were presented as mean and SD. Independent t-test was used to compare age between single and triple injection group. Pearson’s χ 2 test for independence was used to compare differences of gender and Kellgren–Lawrence grade between single and triple injection group.
The changes in WOMAC scores at baseline and post-treatment after 3 months were tested using repeated measures analysis of variance (ANOVA). The changes in WOMAC scores were compared between single and triple GO-ON injection adjusted by other confounding factors such as age, gender and Kellgren–Lawrence radiological grades of patients to minimize bias.
Results
Three hundred five patients were screened for this trial (Figure 1). One hundred thirty satisfied the inclusion criteria. The total numbers of failures at screening were 175, the commonest reason being advanced OA (Kellgren–Lawrence grade IV) and history of recent (within 3 months of screening) knee viscosupplement intra-articular injection.

Trial profile.
One hundred twenty-seven patients were available to be randomized to the two arms of the trial. Sixty-three patients received single injection (GO-ON 5 ml) and 64 patients received triple injections (2.5 ml at weekly interval).
One patient had to be excluded from this trial after he developed symptoms of acute gouty arthritis in the contralateral knee after the first knee intra-articular injection. Two patients defaulted for the 3 months follow-up, after being randomized and receiving the knee intra-articular GO-ON injections as per protocol.
In the entire cohort of 127 patients, 33 were males and 94 females. The mean age was 59.1 years (SD = 7.25) in the single injection arm and 60.1 years (SD = 7.72) in the triple injection arm. Most of the female (56.4%) patients were in the single GO-ON injection arm, while most of the male (69.7%) patients had triple GO-ON injections. The two groups were recorded to have no significant difference in age (p = 0.461) and Kellgren–Lawrence radiological grade (p = 0.694; Table 1).
Descriptive statistics among single injection and triple injection group.
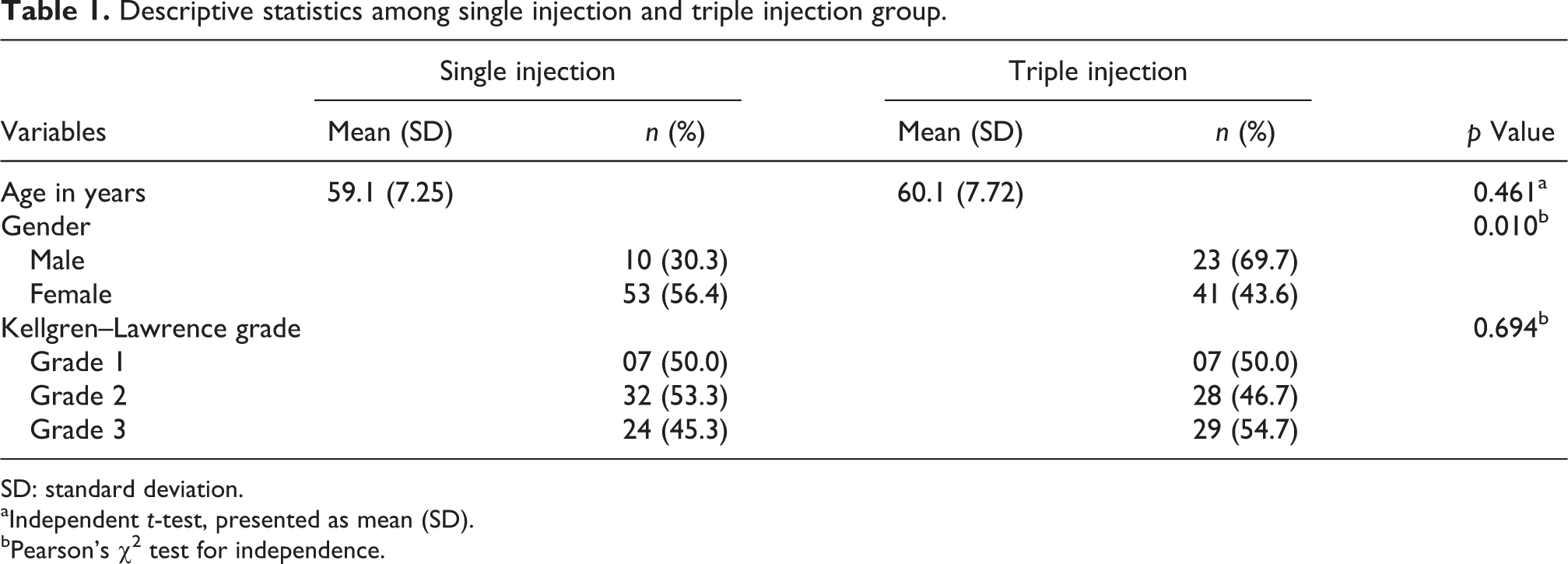
SD: standard deviation.
aIndependent t-test, presented as mean (SD).
bPearson’s χ 2 test for independence.
There was a significant increase in the WOMAC scores in patients of both groups from the baseline (pre-injection) to that recorded at 3 months (post-injection; p < 0.001; Table 2). Further analysis done by comparing changes in WOMAC scores from baseline (pre-injection) to 3 months post-injection between the two arms (single and triple GO-ON injection) adjusted by other factors such as age, gender and Kellgren–Lawrence radiological grade of the patients (Table 3, Figure 2) showed marked improvement in WOMAC scores at 3 months (post-injection; p = 0.011), although there was no statistical significant difference noticed in this clinical improvement between the two arms (p = 0.889).

Pre and post 3 months GO-ON HA injection WOMAC score, adjusted by age, gender and knee X-ray Kellgren–Lawrence grade.
Changes of WOMAC scores post-GO-ON injection among 127 subjects.
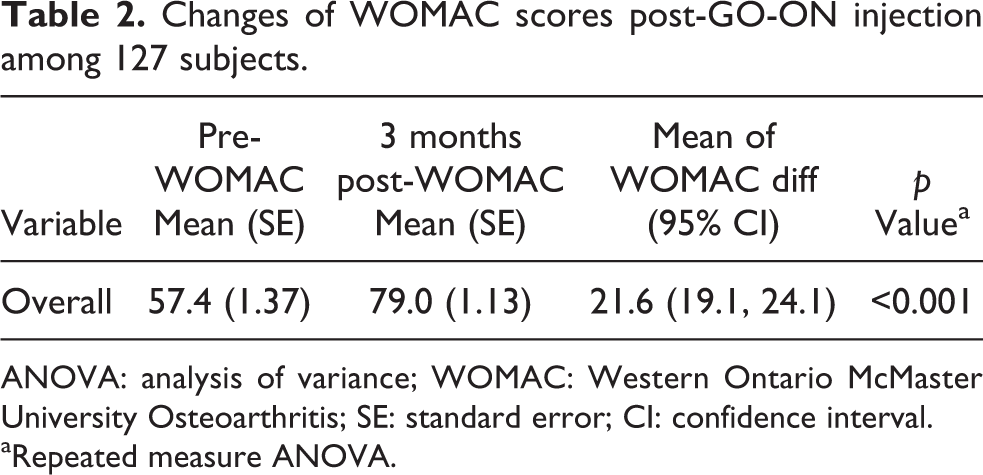
ANOVA: analysis of variance; WOMAC: Western Ontario McMaster University Osteoarthritis; SE: standard error; CI: confidence interval.
aRepeated measure ANOVA.
Factors associated with pre- and post-WOMAC scores using general linear model.

WOMAC: Western Ontario McMaster University Osteoarthritis; SE = standard error; ANCOVA: analysis of covariance.
aMultifactorial repeated measure ANCOVA test, adjusted by age (p value = 0.519).
Mild, localized and self-limiting symptoms of pain, swelling and post-injection flare were documented in both arms. There were no immediate or intermediate septic complications requiring hospital admissions in the entire cohort.
Discussion
This study was conducted to explore the possibility of using single injection HA to increase patient convenience while maintaining the therapeutic efficacy. The study was conducted in two groups, with one receiving the conventional three dose regime of viscosupplementation while the other was tested with the new larger single-dose injection regime. The results in both groups at the end of 3 months did not show any statistical difference.
While there are several published results regarding use of conventional (repeated) doses of viscosupplement knee intra-articular injections in the treatment of knee OA, 2,6,8 to our knowledge, this is the first prospective study comparing the efficacy of two different strength or dose of GO-ON formulations.
The results at 3 months revealed single intra-articular GO-ON (5 ml) injections to be as effective as the standard three GO-ON injections (2.5 ml given as weekly doses for three weeks). Both groups of patients recorded 33% improvement in WOMAC score at 3 months (i.e. from baseline score of 59.7 to 79.7) which was statistically significant (p value = 0.011). Generally, any WOMAC score improvement of 12–18% from baseline is regarded as significant. 11
Analysis of the groups using multifactorial ANOVA, adjusted by age, gender and Kellgren–Lawrence radiological grade, revealed similar improvements at 3 months; however, the results were not statistically significant. According to the Malaysian Osteoporosis Clinical Practice Guideline, women are twice as likely to suffer from knee OA as men. 12 While our study also showed a female predominance, the difference in gender does not affect the primary outcome of the study.
Among several factors influencing the outcome of knee intra-articular HA injection, Lussier et al. noted that patients with early and intermediate disease (Kellgren–Lawrence I–III) did better than patient with more advanced disease (grade IV). 13
Although this study was not powered to demonstrate the safety analysis of both arms, trends in types and frequencies of adverse reactions were assessed using post-injection clinical examination. Most literature report a low incidence of local adverse reactions after knee intra-articular viscosupplement injections 6,14 using conventional small dose repeated intra-articular knee injections. Results of this study showed similar adverse events such as pain, swelling, post-injection flare and stiffness which were generally self-limiting and transient. There were no new or systemic adverse events in both groups despite the study group using larger volume of the viscosupplement, suggesting similar safety profiles for both groups. The 5-ml GO-ON single intra-articular administration was seen to be well tolerated.
This new regime of single larger dose (5 ml GO-ON injection) is convenient due to fewer injections and related events of localized adverse effects and hence likely to be generally more acceptable compared to triple injections. Additionally, apart from the single injection therapy itself being cheaper, it also reduces inconveniences related to frequent clinic visits and doctor consultations, adding to cost saving to the patient and the system.
Most literature looking at similar treatment modalities reported 6 months to 1 year follow-up results. Our study had a relatively short follow-up period of 3 months. Currently, these patients are being planned to be followed up to 1 year to determine sustainability of results derived at 3 months.
Potential bias in the results can be expected as both investigators and patients were not blinded. Patients in the study were free to use rescue analgesics (i.e. celecoxib, etoricoxib, diclofenac sodium, paracetamol) following the injection, and the non-standardized use of analgesic might affect the accuracy of the clinical improvement.
The study has used WOMAC assessment as the only outcome variable. The study involved more than one assessor which could add to potential bias in the clinical assessment.
The study did not use an inactive placebo arm; however, majority of past HA trials showed that HA is more superior to placebo. 15 As our goal was to compare the equivalence in the efficacy of two different doses/strengths of GO-ON injections and since the 2.5 ml triple injection has been approved and has long recorded efficacy and safety, a placebo arm would not provide greater clarity in this study.
Conclusion
This comparative prospective and randomized controlled trial assessing the efficacy of single larger dose of 5 ml GO-ON intra-articular injection to the knee showed similar improvement in results at 3 months as the conventional multi-dose regime. There was no statistically significant difference noticed in the clinical improvement between the two regimes. The efficacy of the single dose regime compared well with the conventional dose of 2.5 ml injected weekly with significant improvement of WOMAC scores from baseline in both groups (33%).
This study primarily confirmed the efficacy of single 5 ml GO-ON intra-articular viscosupplement injection to be equivalent to the multiple injections of GO-ON 2.5 ml triple injections.
We applied the approach FLAE (first last authorship emphasis) for the sequence of authors. All authors have read and approved the content of the manuscript.
Footnotes
Acknowledgements
The authors would like to thank the Director General of Health for permission to publish this article. The authors would also like to thank Staff Nurse Famala Rose A/P Lurthusamy at Clinical Research Centre, Hospital Sultan Abdul Halim, Sungai Petani, Kedah, Malaysia, for her assistance in data collection; Mr Shahrul Aiman Soelar, Statistician from Clinical Research Centre, Hospital Sultanah Bahiyah, Alor Setar, Kedah, Malaysia; and Dr Ang Boon Suen from Department of Physiology, Universiti Sains Malaysia who has assisted in the statistical analysis of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was partly funded by Meda Healthcare Sdn Bhd, Malaysia.