
Abstract
Osteoarthritis (OA) is an extremely common form of chronic joint disease which can affect the knees and other joints of older adults, leading to debilitating disability in the knee and consequent reduction in quality of life. Intra-articular platelet-rich plasma (PRP) or hyaluronic acid (HA) injections are effective for maintaining long-term beneficial effects without increasing the risk of intra-articular infection. However, few studies have compared the relative value of HA and PRP for OA treatment. PRP is more effective than HA for OA treatment in recent studies of this topic. We systematically searched Medline, SpringerLink, Embase, Pubmed, Clinical Trials.gov, the Cochrane Library, and OVID for all articles published through May 2018. Any study was included that compared the effect of HA and PRP (consistent treatment cycle and frequency of injection) on patient’s pain levels and functionality improvements. Review Manager 5.3 was used to analyze data regarding these two primary outcomes. We included 10 total studies in the present meta-analysis. International Knee Documentation Committee (IKDC; MD: 10.37, 95% confidence interval (CI): 9.13 to 11.62, p < 0.00001), Western Ontario and MacMaster Universities Osteoarthritis Index (WOMAC; MD: −20.69, 95% CI: −24.50 to −16.89, p < 0.00001, I2 = 94%), and Visual Analogue Scale (VAS; MD: −1.50, 95% CI: −1.61 to −1.38, p < 0.00001, I2 = 90%) differed significantly between the PRP and HA groups. Knee Osteoarthritis Outcome Scores (KOOSs) did not differ significantly (χ2 = 23.53, I2 = 41%, p = 0.11). Our hypothesis appears not to be confirmed because PRP and HA did not differ significantly with respect to KOOS score. However, the IKDC, WOMAC, and VAS scores differed significantly. Thus, based on the current evidence, PRP appears to be better than HA at achieving pain relief and self-reported functional improvement. Ia, meta-analyses of randomized clinical trials.
Introduction
Knee joint osteoarthritis (OA) is the leading cause of joint degeneration in older individuals. 1 The disease process is characterized by articular cartilage degeneration and whole joint disease. 2,3 These lesions lead to joint dysfunction and pain, which can seriously negatively impact the patient’s quality of life.
Although numerous treatment methods exist to treat knee OA, weight loss and other conservative management approaches, including non-weight bearing exercise and pain control medication, are only effective for those with early stage knee OA. Patients with advanced OA tend to require total knee replacement surgery. 4,5 Recently, intra-articular platelet-rich plasma (PRP) and hyaluronic acid (HA) injections have proven effective for maintaining long-term beneficial effects without increasing the risk of intra-articular infection. 6 As shown by previous studies, HA exerts its effect either through restoring synovial fluid viscoelasticity and mechanical properties or via stimulating endogenous HA production from chondrocytes as well as synoviocytes. 7 –9 It should be noted that a best-evidence systematic review has been published that opposes HA application. 10 PRP is a novel growth factor produced via centrifuging autologous whole-blood and isolation of high platelet count plasma. 11 –13 PRP has been in use in bone, cartilage, and soft tissue for over four decades 10 and is now increasingly been applied in orthopedics and sport medicine. 14 However, there exist considerable controversy with regard to the application of PRP injections. Therefore, we hypothesized that PRP may function better than HA as a means of treating OA, and as such, we performed a meta-analysis to verify this hypothesis.
Materials and methods
Search strategy
We systematically searched Medline, SpringerLink, Embase, Pubmed, Clinical Trials.gov, the Cochrane Library, and OVID for all articles published through May 2018. Search terms: osteoarthritis or OA; hyaluronic acid or HA; platelet-rich plasma or PRP intra-articular injection; total knee arthroplasty or TKA; and total knee replacement or TKR.
Data selection
Two investigators independently screened all study titles and abstracts to determine whether they were eligible for inclusion. Discussion resolved disagreements, and a third investigator helped resolve any discrepancies as needed. Inclusion criteria were as follows: (1) studies must be randomized clinical trials (RCTs); (2) must include 20 or more randomized participants; (3) studies have a 1+ month follow-up duration; (4) both pain and functionality were assessed as study outcomes in a quantitative manner using scoring systems, including the International Knee Documentation Committee (IKDC), Western Ontario and MacMaster Universities Osteoarthritis Index (WOMAC), Numeric Rating Scale (NRS), Knee Osteoarthritis Outcome Score (KOOS), and Visual Analogue Scale (VAS); (5) number of injection, PRP:HA = 1:1 (details are given in Table 2); (6) at least 80% of participants were retained throughout follow-up; and (7) articles were in English, full-text manuscripts.
The characteristics of included studies.

HA: hyaluronic acid; PRP: platelet-rich plasma; RCT: randomized clinical trials; OA: osteoarthritis.
Characteristics of the five trials selected showing general information.
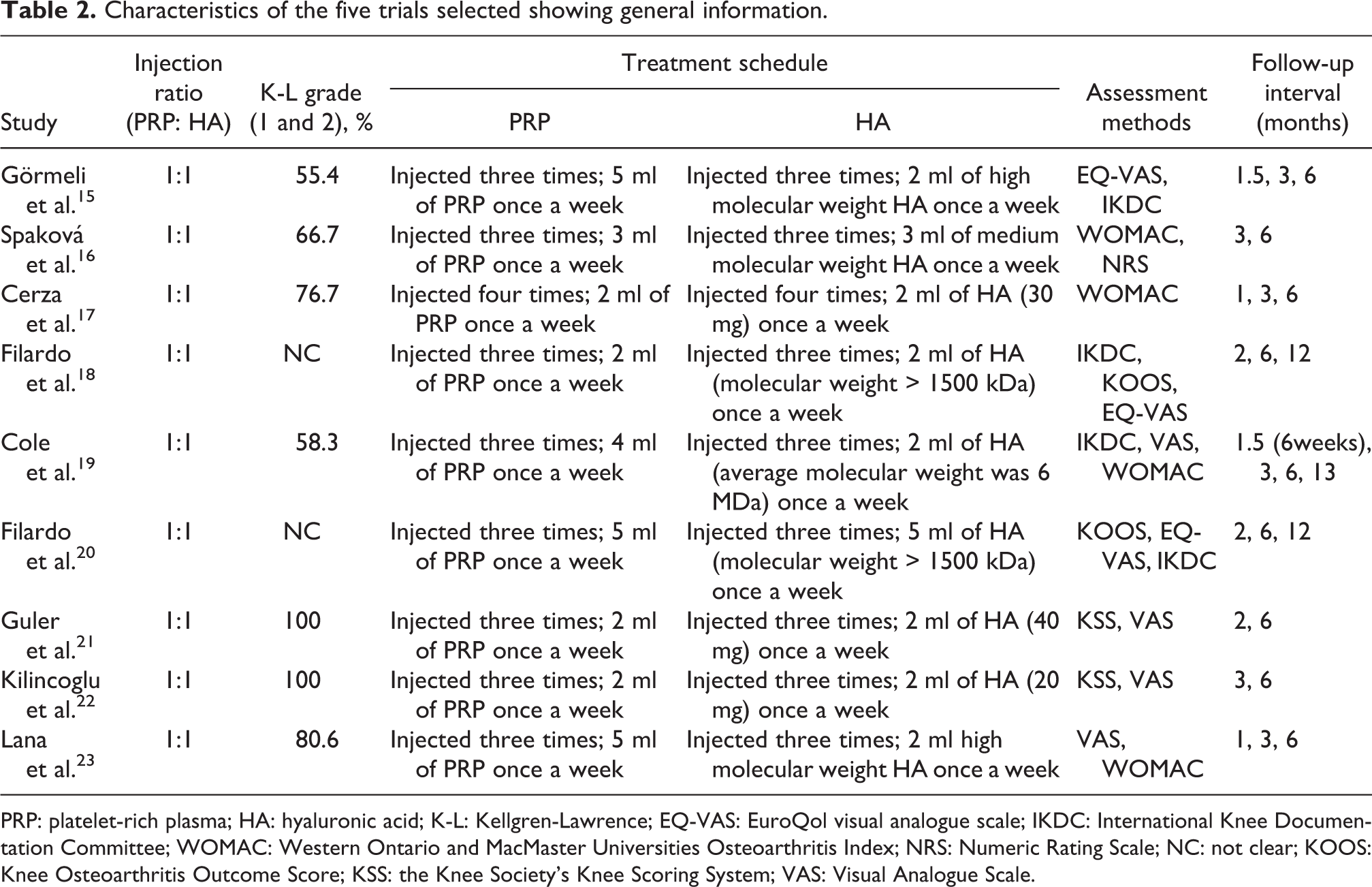
PRP: platelet-rich plasma; HA: hyaluronic acid; K-L: Kellgren-Lawrence; EQ-VAS: EuroQol visual analogue scale; IKDC: International Knee Documentation Committee; WOMAC: Western Ontario and MacMaster Universities Osteoarthritis Index; NRS: Numeric Rating Scale; NC: not clear; KOOS: Knee Osteoarthritis Outcome Score; KSS: the Knee Society’s Knee Scoring System; VAS: Visual Analogue Scale.
Data extraction
The two investigators each independently extracted the following pieces of information from each study: age, number of participants, study design, study population, study interventions, and pain/functionality scores (KOOS, IKDC, WOMAC, or VAS) upon follow-up. All discrepancies were resolved by a third investigator. Standard deviations (SDs) that were not included in the studies were estimated on the basis of the following formula: SD = √n × (P97.5 − P2.5)/[2 × (=tin v(1 − 0.95, n − 1))], with P97.5 and P2.5 representing percentiles, n representing sample size, and (=tin v(1 − 0.95, n − 1)) being determined with Microsoft Excel.
Assessment of study quality and bias risk
Study methodological quality was estimated through use of the Jadad scale, with stores of 4 or higher representing a study of high quality. Bias risk was estimated based on the Cochrane Handbook for Reviews of Interventions (RevMan Version 5.3). The two investigators independently reviewed each study and determined whether there was a high, low, or uncertain risk of bias with respect to the study selection, performance, detection, attrition, or reporting protocols, in addition to other potential sources of bias. A third investigator resolved any discrepancies when discussion alone was insufficient to do so.
Statistical analysis
Study data were analyzed using the RevMan software, with risk ratios and 95% confidence intervals (CIs) being determined for binary variables. A weighted mean difference with corresponding CI was determined for continuous variables based on provided mean and SD values. The I2 value was used to assess heterogeneity, with 25–50%, 50–75%, and >75% indicating a respective low, moderate, or high degree of heterogeneity. For studies with an I2 value > 50%, possible sources of heterogeneity were determined via sensitivity analyses with p < 0.05 as the significance threshold.
Results
We believe this to be the first meta-analysis assessing RCTs that had PRP and HA efficacy with a consistent frequency of injection (total number of injections, PRP:HA = 1:1). We ultimately based this meta-analysis on a total of 10 RCTs, incorporating 526 patients injected treated via PRP and 537 treated via HA.
Study characteristics
We initially identified 916 possible articles which may have been relevant to the present analysis (Figure 1). A total of 20 full publications was isolated after title and abstract review (n = 596) and duplicate removal (n = 300). We then assessed the full text of these 20 manuscripts, leading us to exclude an additional 10 of the studies, resulting in 10 RCTs being included in the present meta-analysis. Study characteristics are compiled in Tables 1 and 2. These RCTs compared effects in the HA and PRP groups when the same frequency of intra-articular injections and the same treatment cycle were employed.

Flowchart showing study identification, inclusion, and exclusion.
Risk of bias
We next assessed risk of bias in these studies (Figure 2). All present studies were randomized in design; 15 –24 however, one of these studies 18 failed to properly describe the randomization sequences used, while another study 19 failed to properly detail the allocation concealment strategy. In two of the trials, there was insufficient information provided with respect to participant or personnel blinding, resulting in a high risk of performance bias, in addition to a high risk of attrition bias because of a lack of information with respect to how incomplete outcome data were handled. 18,19 In total, three trails 18 –20 lost some patients during follow-up.

Risk of bias summary.
Analysis of study heterogeneity and sensitivity
We detected substantial heterogeneity with respect to different methods on VAS score. Using an analytical approach, individual studies were omitted from the analysis to identify sources of high heterogeneity, which allowed us to determine that the primary source was the RCT by Cole et al. 19 Following omission of this study, I2 was lowered to 74% for VAS score. However, pooled change significance values were unchanged after this omission, suggesting robust results.
IKDC score upon 6-month follow-up
Four studies 15,18 –20 compared IKDC scores from PRP and HA groups, revealing a significant difference between the two (MD: 10.37, 95% CI: 9.13 to 11.62, p < 0.00001). However, we detected significant heterogeneity, warranting caution when interpreting this finding (χ2 = 17.12, I2 = 82%; Figure 3).

Forest plot of IKDC score in the PRP group compared with the HA group. IKDC: International Knee Documentation Committee; PRP: platelet-rich plasma; HA: hyaluronic acid.
WOMAC score at the 6-month follow-up
Two studies 16,17 included WOMAC scores, with a significant difference in these scores between PRP and HA groups (MD: −20.69, 95% CI: −24.50 to −16.89, p < 0.00001, I2 = 94%; Figure 4). We were not able to determine which study contributed to the underlying heterogeneity via a sensitivity analysis, but a leave-one-out approach revealed that PRP was consistently associated with better WOMAC score improvements than was HA even though heterogeneity did not decrease significantly.

Forest plot of WOMAC score in the PRP group compared with the HA group. WOMAC: Western Ontario and MacMaster Universities Osteoarthritis Index; PRP: platelet-rich plasma; HA: hyaluronic acid.
VAS score at the 6-month follow-up
Data on VAS score were provided by four studies, 15,19,22,24 with scores in the PRP and HA groups differing significantly (MD: −1.50, 95% CI: −1.61 to −1.38, p < 0.00001, I2 = 90%; Figure 5), and we can find that PRP was still demonstrated to be better than HA in VAS scores, though one study 24 suggested that HA was superior to PRP in VAS score (MD: 2.28, 95% CI: 0.68 to 3.88).

Forest plot of VAS score in the PRP group compared with the HA group. VAS: Visual Analogue Scale; PRP: platelet-rich plasma; HA: hyaluronic acid.
KOOS at the 6-month follow-up
Three studies 18 –20 provided data on the KOOS score, which did not differ significantly between groups (χ2 = 23.53, I2 = 41%, p = 0.11; Figure 6).

Forest plot of KOOS score in the PRP group compared with the HA group. KOOS: Knee Osteoarthritis Outcome Score; PRP: platelet-rich plasma; HA: hyaluronic acid.
Discussion
PRP, as a growth factor treatment, has been applied in bone, cartilage, and soft tissue repair for over four decades 25,26 and is increasingly been applied in orthopedics and sports medicine. 27 Several studies have reported that upon application of PRP, the activated platelets are able to produce molecules including growth factors that can in turn drive cell migration to this region, thereby enhancing tissue healing and altering the inflammatory processes that underlie OA progression. Cerza et al. 17 reported that PRP achieved superior clinical outcomes to HA. Other studies 28 –30 comparing PRP treatment with HA also reported that PRP worked better than HA for patients with OA. In this meta-analysis, we found that KOOS did not differ significantly between PRP and HA groups, whereas PRP was better than HA with respect to IKDC, WOMAC, and VAS. These results highlight that treatment with PRP works better than HA in patients with OA in terms of relieving pain and improving joint functionality.
Prior studies 31 –33 and several meta-analysis 13,34,35 assessing PRP efficacy revealed PRP to not be better than HA in the context of effectively designed double-blind trials, suggesting the possibility that poor blinding protocols could explain any benefits ascribed to PRP. This is not consistent with our conclusions. We observed no differences in KOOS. However, a slight better outcome with respect to symptoms and pain in the KOOS scoring system was noted in the PRP group when compared with HA group (−2.66; −1.73, 0.12, respectively). This difference was not, however, statistically significant (p > 0.05). The inconsistent results may be a result of inconsistencies in the number of injections in PRP group and HA group among the studies. Furthermore, relatively small numbers of RCTs and patients may have influenced these outcomes.
The main outcomes investigated were the IKDC, WOMAC, VAS, and KOOS scoring systems. PRP and HA have the potential to decrease hyperplasia of the synovial membrane and alter cytokine levels, thereby changing the homeostasis of the joint. This can result in transient improvements in clinical readouts without prolonged benefits to the structure of the underlying cartilage. 36,37 Görmeli et al. 15 conducted an RCT investigating the effect of multiple PRP injections and suggested that multiple injections improve clinical outcomes more effectively than single PRP or HA injections. This suggests that the frequency of injections may be a key determinant of intervention outcomes. In this meta-analysis, we focused on the literature that kept a consistent number of injections (injection ratio, PRP:HA = 1:1, details are given in Table 2) in order to assess the results as accurately as possible. Given that this meta-analysis highlights the beneficial effects of PRP, this suggests that PRP may more effectively relieve pain and enhance self-reported functionality.
It seemed that the statistical analysis could be more persuadable using the studies with the same injection number and same interval time and analyzing the data of longer follow-up results, but ultimately, it was impossible to gather enough literature with the same injection number and same interval time, but we can set strict literature inclusion criteria to ensure us to have literature with injection number of consistent proportion (details are given in in Table 2) and same interval time. Among the 10 studies we included, the longest follow-up time of 1 article was 3 months, 6 articles were 6 months, 2 articles were 12 months, and 1 article was 13 months (details are given in Table 2). In order to make a resourceful comparable analysis, we selected 6 months after surgery as a time point for evaluation. We observed substantial methodological and clinical heterogeneity among these studies, with a variety of dosing strategies and PRP/HA preparations used across studies. Furthermore, different trials exhibited significant variability with respect to OA grades and outcome scores for study populations, adding additional high-level heterogeneity to this analysis. These areas of uncertainty made it increasingly difficult to accurately synthesize and interpret pooled study results. This meta-analysis has certain limitations. For one, only English articles were included, and as such incorporating further studies has the potential to increase the underlying heterogeneity and thereby alter our conclusions. Second, the frequency of injections varied between studies, with eight studies using a treatment frequency of three injections, one study using a frequency of four injections, and one study having a single injection. This variation may increase the heterogeneity and hence affect our results. Lastly, follow-up times varied among included studies. As such, in the future, larger RCTs with more patients are needed as a means of confirming the value of PRP for OA treatment.
Conclusions
Our hypothesis appears not to be confirmed because the PRP and HA groups did not differ significantly with respect to the KOOS score. However, significant difference can be seen in the IKDC, WOMAC, and VAS score. Thus, based on the current evidence, PRP appears to be better for pain relief and self-reported functional improvement. Further studies are needed to investigate the appropriate injection dose, frequency as well as interval time of injection in patients with knee OA.
Footnotes
Authors’ contributions
Qipeng Wu and Xuefen Luo contributed equally to this study. QW and XL participated in the design of the study; BM and QW carried out data curation; XC and BM performed the statistical analysis; JW and XC carried out investigation; YX and QW carried out project administration; QW and XL operated software; GL carried out supervision; BM and YX carried out validation; QW and XL conceived of the study, participated in its design and coordination and helped to draft the manuscript; GL and JW participated in the sequence alignment and drafted the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.