
Abstract
Background and Aims:
Reoperations after operative treatment of hip fracture patients may be associated with higher costs and inferior survival. We examined the acute hospital costs, long-term reoperation rates, and survival of patients with a new hip fracture.
Materials and Methods:
A total of 490 consecutive new hip fracture patients treated at a single center between 31 December 2004 and 6 December 2006 were analyzed retrospectively. Fractures were classified according to Garden and AO. All medical records were checked manually. The costs of reoperations were calculated using the diagnosis-related groups (DRG)-based prices. Survival analysis was performed using the life-table method. The follow-up time was 10 years.
Results:
In all, 70/490 patients (14.3%) needed reoperations. Of all reoperations, 34.2% were performed during the first month and 72.9% within 1 year after the primary operation. The hemiarthroplasty dislocation rate was 8.5%, and mechanical failures of osteosynthesis occurred in 6.2%. Alcohol abuse was associated with a heightened risk of reoperation. The mean direct costs of primary fracture care were lower than the mean costs of reoperations (€7500 vs €9800). The mortality rate at 10 years was 79.8% among non-reoperated patients and 62.9% among reoperated patients.
Conclusions:
According to our hypothesis, the cost per patient of reoperation in acute care was 31% higher than the corresponding cost of a primary operation. Reoperations increased the overall immediate costs of index fractures by nearly 20%. One-third of all reoperations were performed during the first month and almost 75% within 1 year after the primary operation.
Introduction
Hip fractures are the most common fractures requiring surgical treatment among adults. The long-term results following hip fracture surgery are generally poor, including the loss of independence in approximately half of the cases (1) and mortality rates of up to 37% over the first year following surgery (2).
Complications in the surgical treatment of elderly patients’ hip fractures are frequent, with rates ranging from 8% to 11% according to the literature (3, 4). Hip fractures are also complicated by a 0%–49% need for revision surgery, which is influenced heavily by fracture characteristics and surgical interventions (5). Dislocation is a serious complication of hip hemiarthroplasty and leads to a reoperation in many cases. The reported rates of dislocation after hip hemiarthroplasty vary from 1% to 22% (6).
In relation to other low-energy fall injuries, the treatment of a hip fracture is the most expensive (7). The Finnish National Hip Fracture Database of PERFormance, Effectiveness and Costs of Treatment episodes (PERFECT) includes hospital-specific follow-up data for at least 1 year for each patient and currently covers the period 1999–2013 (8). According to the last PERFECT database, the annual average total costs per hip fracture patient in Finland were €30,906 in 2013 (range: €26,332–€37,822). Acute hip fracture costs in Europe ranged from approximately €2,000 in Bulgaria to roughly €25,000 in Denmark (9).
The aim of this study was to examine the reoperations and survival after the initial operative treatment of patients with hip fractures with a follow-up period of 10 years and to calculate the immediate direct costs of the operations.
Material and Methods
We retrospectively analyzed 490 consecutive patients with a new hip fracture requiring operative treatment at the Päijät-Häme Central Hospital in Lahti, Finland, from 31 December 2004 to 6 December 2006. The Päijät-Häme Central Hospital is responsible for an area of 210,000 inhabitants. Femoral neck fractures were classified according to the Garden classification (S72.0) and trochanteric (S72.1) and subtrochanteric (S72.2) fractures according to the AO classification. The Finnish version of the NOMESCO Classification Procedural Codes was used (10): NFB10 (uncemented hemiarthroplasty); NFB20 (cemented hemiarthroplasty); NFB30 (uncemented primary total hip arthroplasty); NFB40 (hybrid total hip arthroplasty); NFB50 (cemented primary total hip arthroplasty); NFJ50 (osteosynthesis of the neck with cannulated screws); NFJ52 (osteosynthesis of the proximal femur with dynamic hip screws (DHS) or Medoff-plate); NFJ54 (osteosynthesis with an intramedullary-nail); and NFK10 (Girdlestone excision arthroplasty). Basicervical fractures were classified as pertrochanteric fractures. All hemiarthroplasty operations were performed using a posterior approach and one total arthroplasty using an anterolateral approach. The baseline characteristics of the patients are shown in Table 1. The study was approved by the ethics committee of Päijät-Häme Central Hospital.
Type of fracture, operation, and implant.
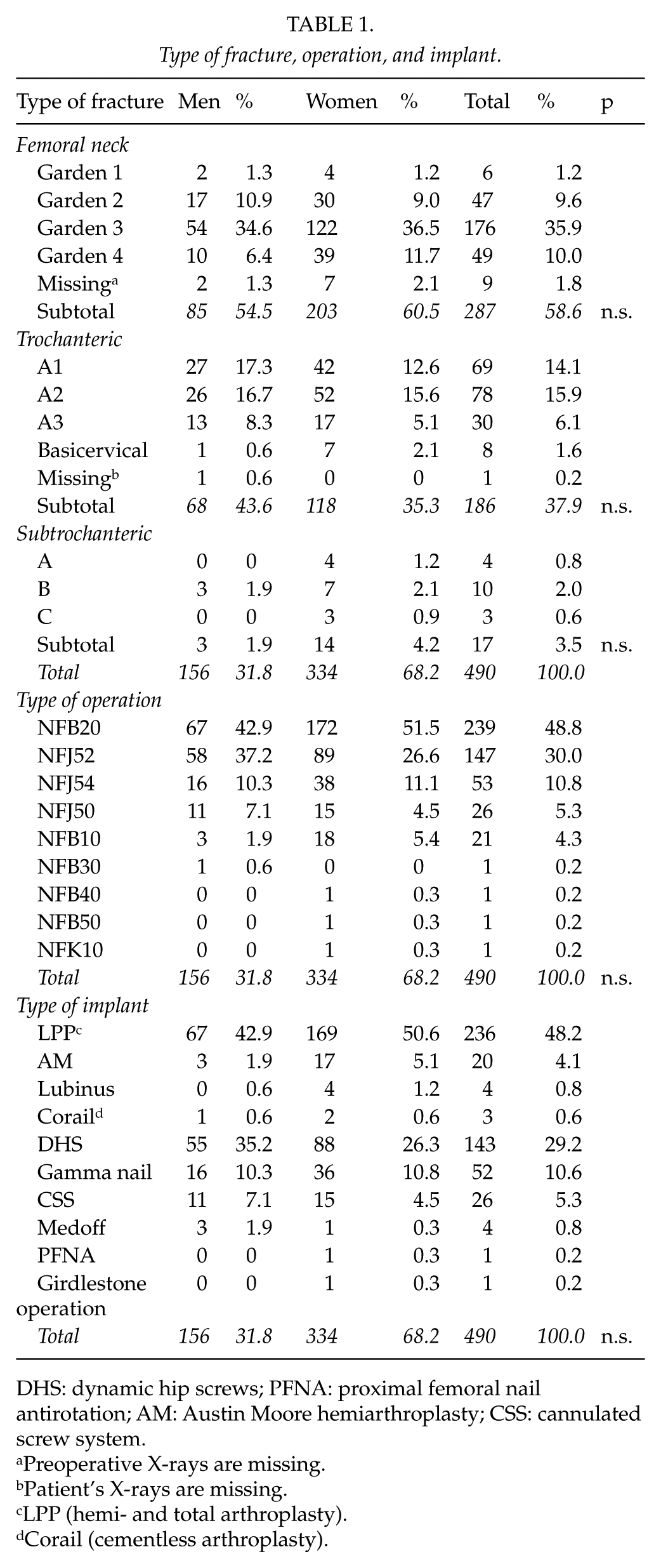
DHS: dynamic hip screws; PFNA: proximal femoral nail antirotation; AM: Austin Moore hemiarthroplasty; CSS: cannulated screw system.
Preoperative X-rays are missing.
Patient’s X-rays are missing.
LPP (hemi- and total arthroplasty).
Corail (cementless arthroplasty).
Medical records of all patients were checked manually (R.T.). The following parameters were collected from the patient records: the patient’s personal identity code, age, sex, and date of admission, as well as the date of operation, experience of the surgeons (orthopedic surgeon vs resident), and dates of discharge and death. The deaths were obtained from the Finnish Causes of Death statistics. Pre-existing comorbid conditions increasing the risk of falling were identified (alcoholism, Alzheimer’s disease, dementia, stroke, Parkinson’s disease, previous intracranial hemorrhages, schizophrenia). The length of the hospital stay (LOS) during the primary fracture care and complications that could potentially lead to reoperations were recorded and analyzed.
The immediate direct costs of reoperations for each patient were calculated using the diagnosis-related groups (DRG)-based prices of our hospital in 2016. Survival analysis was performed using the life-table method. In this method, the observed survival rates of the groups are compared with survival rates based on sex- and age-specific life tables for the whole population of the same age (reference population) in Finland. The calculations of the survival rates are based on the individual life expectancies of the target population for the target years. The relative survival curve of the reference population would be 1.00 (7).
If the survival curve of the group remains below the survival of the reference population, there is excess mortality in the group (Fig. 1). The deaths were obtained from the Finnish Causes of Death statistics. The follow-up time of survival was from 31 December 2004 to 5 May 2017 (minimum of 126 months = 10.5 years).
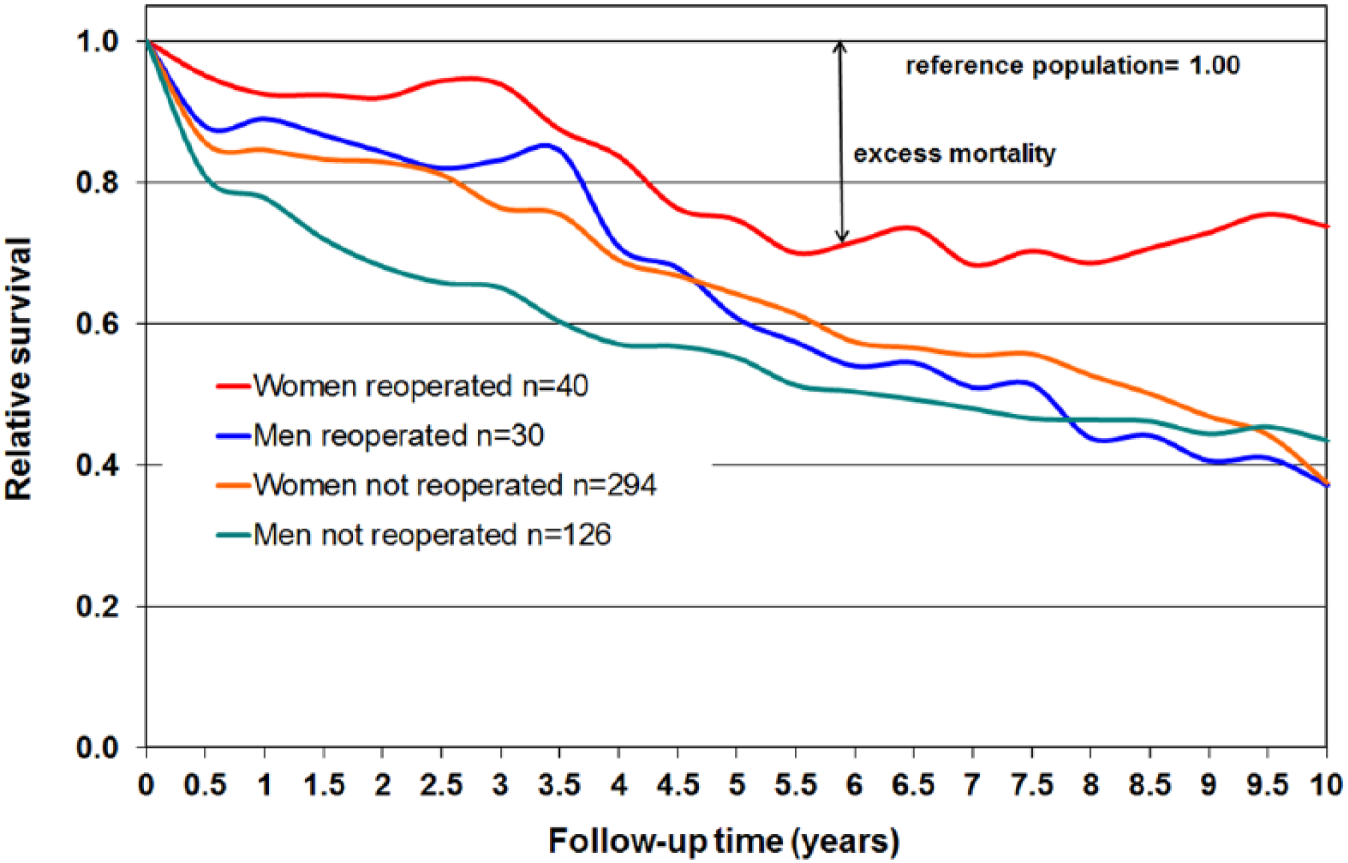
Survival of reoperated and not reoperated hip fracture patients.
Statistical Analysis
Standard methods of descriptive statistics were used, such as tabulations, means, and standard deviations (SDs). Because there were no stated hypotheses, the chi-square test was used and two-way analysis of variance applied. Fisher’s exact test was used when appropriate.
Results
Complications and Reoperations
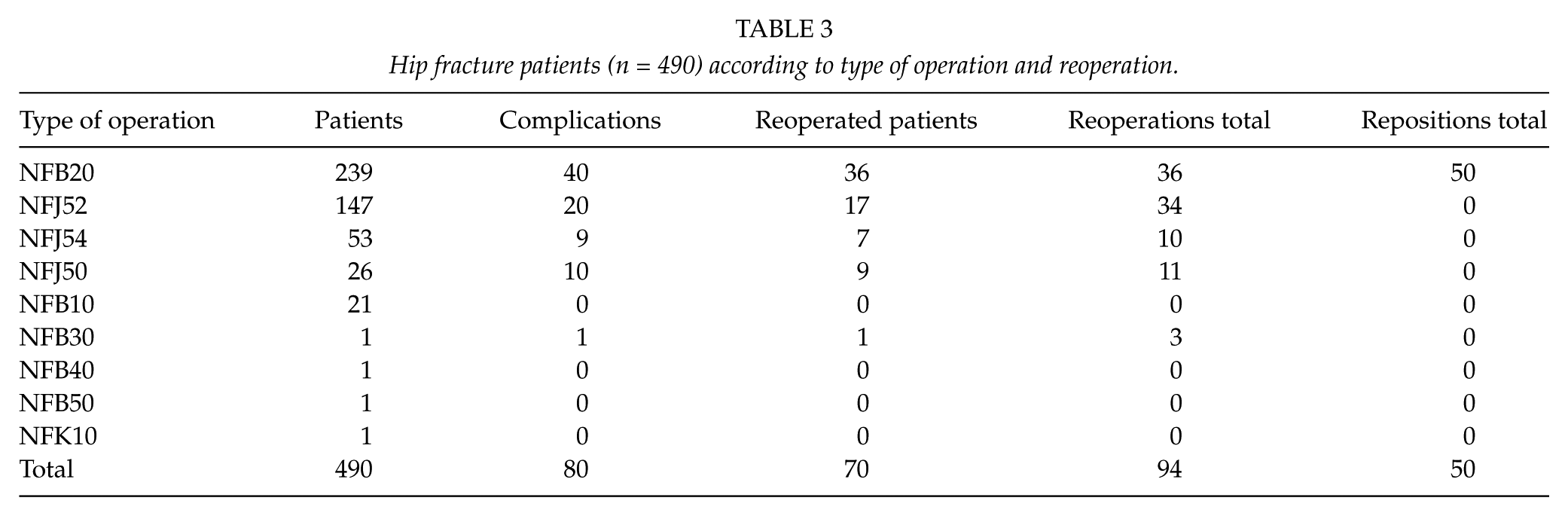
In this study, 16.3% (80/490) of the patients sustained complications, for example, postoperative hemorrhagia, superficial wound infections, deep surgical site infections (DSSI), dislocations, and periprosthetic fractures after the primary operations (Table 2). During the follow-up, 87.5% (70/80) of the patients with complications needed reoperations. Overall, 94 reoperations and 50 closed repositions (range: 1–4) were performed on 70 patients during the 10-year follow-up (Table 3). Of all the patients with a femoral neck fracture (n = 287), 16% (n = 46) needed a reoperation. The corresponding proportion among patients with a trochanteric fracture (n = 186) was 11.3% (n = 21), and among patients with a subtrochanteric fracture (n = 17) was 17.6% (n = 3). The overall rates of reoperations were 52.9% after arthroplasties (1 total and 36 hemiarthroplasties) and 47.1% after osteosyntheses (33/70).
Complications causing reoperations.
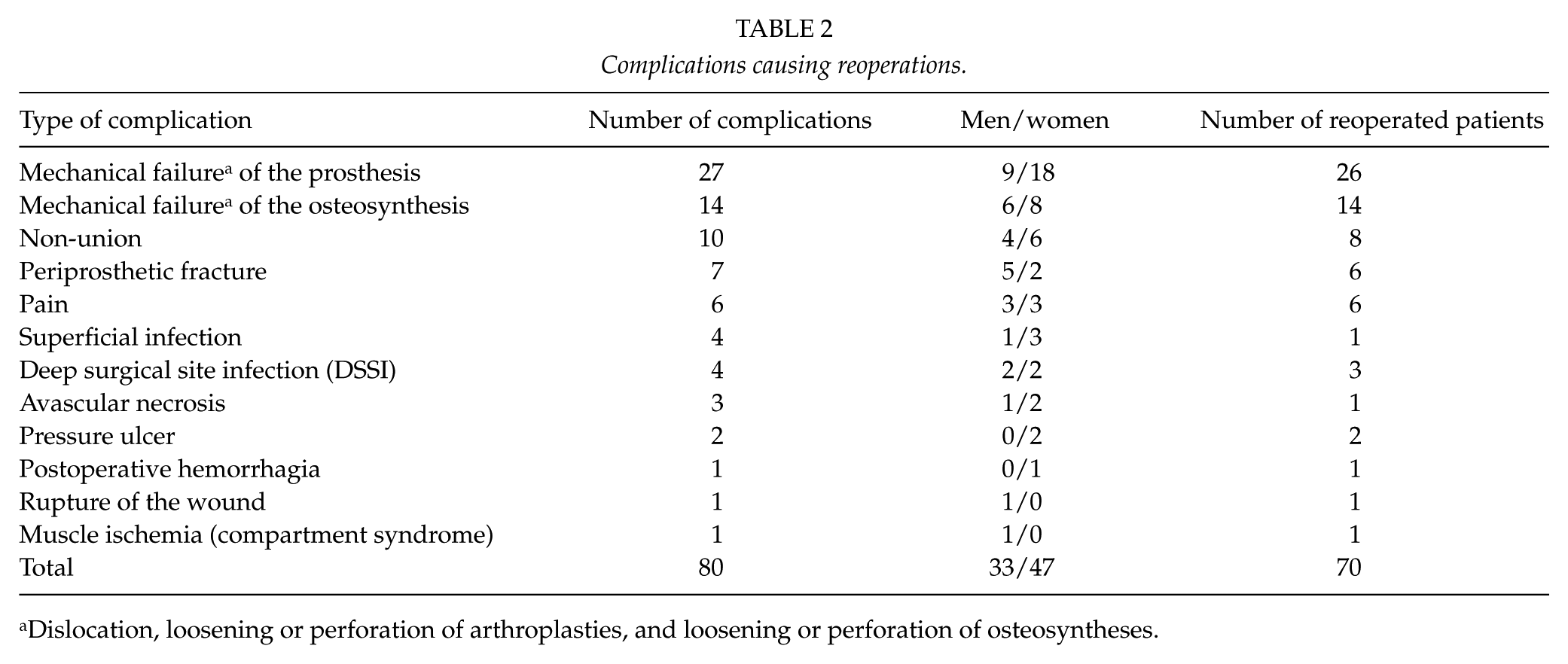
Dislocation, loosening or perforation of arthroplasties, and loosening or perforation of osteosyntheses.
Hip fracture patients (n = 490) according to type of operation and reoperation.
Of all first reoperations, 34.2% (24/70) were performed during the first month and 72.9% (51/70) within 1 year after the primary operation. There is a slight difference in complications leading to reoperations between men (30/156) and women (40/334) (χ2 = 4.57, d.f. = 1, p < 0.05).
The most common complication leading to a reoperation was a dislocation. The overall dislocation rate was 8.7% (23/263). Among hemiarthroplasty patients, the dislocation rate was 8.5% (22/260) and among total arthroplasty patients, correspondingly, 33.3% (1/3). Of all patients treated with osteosynthesis, 14.6% (33/226) were reoperated on. The most common cause of reoperation was the use of cannulated screws in patients with femoral neck fractures (9/26, 34.6%; Table 3). A mechanical failure of osteosynthesis was the cause of reoperation in 6.2% (14/226). All these patients needed a reoperation. Non-union occurred in 4.4% (10/226) of the osteosynthesis patients and led to reoperations in 80% of these patients (8/10). There were slightly more reoperations among those patients who were primarily operated on by residents guided by an orthopedic surgeon (χ2 = 8.24, d.f. = 2, p < 0.05).
The total infection rate was low, 1.6% (8/490). The infection rate after arthroplasty was 1.5% (4/263). Infection usually led to reoperations, the rate being 50% (4/8). Pain was a reason for six late reoperations (1.2%): two gamma nails, one DHS, and one cannulated screw system (CSS) were removed, and two LPP-EcoFit (Implantcast, GmbH) hemiarthroplasties were converted to total arthroplasty because of painful acetabular erosion. There were seven periprosthetic fractures; of which, six were reoperated on.
Patients with certain pre-existing comorbid conditions (alcohol abuse, Alzheimer’s disease, and dementia) were at a greater risk of reoperations (Fisher’s exact = 0.013). In further analysis, especially patients with recorded alcohol abuse (39/490, 8%) had a heightened risk of reoperation (χ2 = 13.48, d.f. = 3, p < 0.01). One-third (14/39, 35.9%) of the patients with recorded alcohol abuse needed reoperations after primary operations. Five of these cases were prosthesis dislocations and three failures of the osteosynthesis. Other reasons resulting in a reoperation were non-union in two cases, pain in two cases, one DSSI, and one avascular necrosis.
Mortality
For the whole patient cohort (mean age: 79 years, SD 12), the overall mortality was 79.8% (391/490) at the end of the 10-year follow-up: 82% (274/334) of the women and 75% (117/156) of the men died. The mortality risk was the highest in the first year after hip fracture. The 30-day, 6-month, 1-year, 2-year, 3-year, 4-year, 5-year, 6-year, 7-year, 8-year, 9-year, and 10-year cumulative mortality rates were 7.3%, 18.0%, 22.2%, 31.2%, 40.0%, 50.4%, 56.9%, 67.1%, 68.4%, 72.0%, 75.7%, and 79.8%, respectively.
Patients who survived were approximately 10 years younger than those who died during the 10-year follow-up: 66 years (SD = 13 years) and 76 years (SD = 13 years), respectively. The annual cumulative mortality rates among the reoperated patients (n = 70) at 1, 2, 3, 4, 5, 6, 7, 8, 9, and 10 years were 12.8%, 18.6%, 21.4%, 34.3%, 44.2%, 50.0%, 54.3%, 58.6%, 60.0%, and 62.9%, respectively. There were no reported deaths within 30 days following the index fracture operation of the reoperated patients.
The 10-year survival of the reoperated and non-reoperated patients according to sex is presented in Fig. 1. The observed survival of the reoperated women was higher than expected (χ2 = 7.27, d.f. = 1, p < 0.001) and higher than that of the non-reoperated women.
At the end of the 10-year follow-up, 37.1% (26/70) of the reoperated patients were still alive (9 men and 17 women with mean ages of 64.9 years (SD = 11.45 years) and 80.8 years (SD = 9.9 years), respectively). Correspondingly, 17.4% (73/420) of the non-reoperated patients were alive (30 men and 43 women with mean ages of 68.5 (SD = 14.1) and 81.6 (SD = 9.6) years, respectively).
Costs
The total direct costs (sum of costs of operative care and hospital stay) of all hip fracture patients were €4,351,236, out of which the total costs of reoperations were €685,402 (18.7%). The average length of hospital stay (LOS) after the primary operation was 9.0 days. The additional LOS caused by complications was 7.2 days on average. The mean direct cost of primary fracture care differed significantly from the mean cost of reoperations (€7481 vs €9791).
Discussion
The complications and reoperations after hip fractures place a significant burden on health care by increasing the overall costs and use of resources. According to the Danish Fracture Database (n = 10,000) that was launched in 2011 to establish nationwide prospective quality assessment of all adult (85%) and pediatric (15%) fracture-related surgery, proximal femur (33%), distal radius (15%), and ankle fractures (12%) were the three most common primary fractures needing surgery in adults. The most common anatomical location for a reoperation was the proximal femur (30%), followed by the ankle (19%), the distal radius (6%), and the tibial shaft (6%) (11). The reoperations after a hip fracture are therefore an important issue to investigate. In this study, we have reported the complication types, complication rates, reoperation rates, and direct costs of index fractures and reoperations, as well as the mortality among 490 consecutive hip fracture patients during the follow-up of 10 years.
During the follow-up, a total of 14.3% of the patients needed reoperations due to complications. The most common reasons for reoperations were dislocations, mechanical failures, non-unions, and periprosthetic fractures. Of all reoperations, 34.2% were performed during the first month and 72.9% within 1 year after the primary operation.
Our 30-day and 1-year mortality rates among all 490 hip fracture patients (7.1% and 22.2%, respectively) were slightly higher than the corresponding means of 5.7% and 18.4% reported in the Finnish National Hip Fracture Database (8). However, the 1-year mortality in our study was lower than the rate of approximately 30% reported in many studies (2, 12, 13). In our study, the mortality risk was highest within the first year after a hip fracture, and similar results are also reported in epidemiological studies (14, 15). For the whole patient cohort, the overall mortality at the end of the 10-year follow-up was 80%.
In a Finnish earlier study with a 8-year follow-up, 9% of the patients required 1 or more reoperations as a result of a complication of the primary operation. Of the reoperations detected, 65% were performed during the first year after treating the acute hip fracture and 85% within 2 years (7). A Swedish study reported a reoperation rate of 18% for basicervical hip fractures after a median follow-up of 4.8 years (range: 2.2–8.8 years). Of the first reoperations, 80% were performed within 1 year and 92% within 2 years (16). In the last Swedish national hip register from 2015 with a follow-up of 0.75–1.75 years, the reoperation rate for femoral neck fractures was 4.5% and for trochanteric fractures 3.6% (17). The rate was highest among femoral neck fractures treated with osteosynthesis (5.2%), while it was 4.4% in patients treated with hemiprosthesis and 3.6% in patients treated with total prosthesis (17). According to a meta-analysis, it is still controversial in treating displaced femoral neck fractures (6). In comparison to internal fixation, arthroplasty (hemi-, bipolar, or total arthroplasty) significantly reduce the risk of reoperation, but the risk of infections and early postoperative deaths are higher (6). A more recent meta-analysis shows that in fit elderly, total arthroplasty may lead to better outcomes but has higher dislocation rates compared to hemiarthroplasty (18). The Norwegian Hip Fracture Register reported a low reoperation rate among 11,116 patients aged >70 years with cemented (2.5%) or uncemented (5.1%) primary hemiarthroplasties for displaced fractures. In this report, the mean follow-up was 1.65 years (1–5 years) (19). A recent study on reoperations between the Norwegian Hip Fracture Register and the Swedish Hip Arthroplasty Register on hemiarthroplasties after hip fractures during 2005 and 2010 reported a 3.5% reoperation rate in Norway and a 3.6% rate in Sweden (20). The higher re-operation rate reported here was mostly due to a few specific issues. First, there was a substantial number of patients with a history of alcohol abuse in this cohort (8% of all patients), which partly explains the higher reoperation rate. More than one-third of patients with a history of alcohol abuse needed reoperations after primary operations. Second, the follow-up time was longer than in most studies. Third, the reoperation rate after cannulated screw fixation was almost 7 times higher in our study than in the one reported by the Swedish National Hip Register (17).
In this study, the most common complication types were dislocations and mechanical failures. The detected dislocation rate after hemiarthroplasty was 8.8%, which is in coherence with the dislocation rate published previously among hip fracture patients (8%–13%) when a posterior approach was used (14, 21). At our hospital, we usually use the posterior approach. In an earlier Finnish study on hip hemiarthroplasty (n = 575), 5.6% of the patients experienced at least 1 dislocation (22). An operation delay of over 48 h was also associated with a trend for increased dislocation (22).
Our total infection rate was 1.6%, and for arthroplasties, the DSSI rate was 1.5%. This is in line with the previous studies. In Norway, the infection rate after hemiarthroplasty was 1.8% and in Sweden 1.0%. The mean follow-up was 1.67 (0–6) years in Norway and 1.82 (0–6) years in Sweden (19). Hip fractures typically produce the highest cost per fracture event, and the economic burden is highly sensitive to the health care environment (23). In this study, the overall direct costs of hip fracture care in a single institution among 490 hip fracture patients were over 4 million euros, nearly 20% of which were caused by reoperations. The average costs of index fracture care and reoperations including hospital stay were €7481 and €9791, respectively. The Finnish National Hip Fracture Database includes no information on reoperations (8) but entails the estimated costs of the first year after the index fracture. In our study, the mean direct costs of primary fracture care were €7481 per patient, which is only 25% of the average first-year costs of hip fracture reported in the Finnish database. However, according to an earlier Finnish prospective study on the total 1 year costs in 106 consecutive hip fracture patients, only 25% of all costs were caused by acute hospital care (24). A similar result was reported from the Netherlands: acute hospital care accounted for 22% of the total 1 year medical costs (25).
Reoperations are known to increase the total costs significantly. In this study, the costs of reoperations were 18.7% of the total direct costs. In an English hip fracture study, all procedures requiring reoperations led to a significant increase in the total costs, increasing the overall immediate costs of index fractures by 14% (26). Several studies have suggested that the reoperations after failed internal fixation double the costs (27, 28). When reoperations were included in the cost analyses, there was no difference in costs between hemiarthroplasty and internal fixation (28) or total arthroplasty and internal fixation (27), although the index arthroplasty operations are more expensive.
While interpreting our results of this study, one has to note the high frequency of alcohol abuse history within the cohort. Heavy alcohol use has been associated with a heightened hip fracture risk (29). It has been suggested to increase fixation failure, non-union, and avascular necrosis in younger patients (30). In our study, alcohol use was also associated with a significantly higher risk of reoperation. Therefore, in our clinical setting, patients with known alcohol abuse should be treated not only for their fractured hip but also for their alcoholism more efficiently. This might significantly reduce the need for reoperations and the costs of hip fracture care in the future.
Strengths and Limitations
Due to the retrospective nature, this study has some limitations: the accuracy of the medical records and potential information bias. In addition, we only considered the costs of reoperations in acute hospital care. The costs after primary care, for example, costs of nursing home stays, municipal home care, visits to the outpatient department, patients’ own share of the hospital costs, transportation costs, and extra medication costs, remained unaccounted for.
There is also a potential for immortal time bias, because patients have to live a certain time before complications are noticed after the primary hip fracture operation. However, 75% of all reoperations were performed during the first postoperative year after the index hip fracture. According to Fig. 1, the difference of the relative survival between reoperated women and men versus non-reoperated is noticed already at 6 months and 1 year after the operation of the index hip fracture. Therefore, the possible bias is questionable. One reason might be that the medical follow-up of the reoperated patients is better than that of the non-reoperated, because, for example, cardiovascular problems of these patients needing a reoperation can be treated before the reoperation.
The strengths of our study were the long follow-up time, detailed patient-specific data, and the large number of consecutive patients at a single institution. All medical records and radiographs were also reviewed by R.T.
Conclusion
Hip fractures and complications after the operative treatment of hip fractures cause a substantial socioeconomic burden. In our study, the average costs of reoperation per patient were 31% higher than those of the primary operation, and reoperations caused nearly 20% of the overall direct costs of hip fractures. One-third of all reoperations occurred during the first postoperative month and 75% during the first year. Every seventh patient who underwent osteosynthesis was reoperated on, mainly after the use of cannulated screws. Dislocations occurred in 9% after hemi- and total arthroplasty. Alcohol abuse was associated with an increased reoperation rate. Paying attention to the rehabilitation of individuals with alcohol abuse could lead to fewer complications.
Footnotes
Acknowledgements
The authors would like to thank D.Sc. Tech., adjunct professor (biometrics) Matti Kataja for statistical analyses.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the Competitive State Research Financing of the Expert Responsibility area of Tampere University Hospital and the Päijät-Häme Medical Society.