
Abstract
Background and Aims:
To compare outcomes between posterior spinal fusion of juvenile idiopathic scoliosis and adolescent idiopathic scoliosis patients with a minimum of 2-year follow-up. The juvenile idiopathic scoliosis patients were fused to the stable vertebra and adolescent idiopathic scoliosis to the touched vertebra. We hypothesized that extending the spinal fusion to the stable vertebra in juvenile patients would provide similar outcomes compared with fusion to the touched vertebra in adolescents.
Materials and Methods:
A prospective comparative study of 21 consecutive children with juvenile (Risser 0) and 84 adolescent (Risser ⩾2) idiopathic scoliosis (1:4 ratio) undergoing bilateral segmental pedicle screw instrumentation and direct vertebral derotation with a minimum of 2-year follow-up.
Results:
Juvenile patients had a significantly larger main curve (58° vs 53°, p = 0.003), more fused levels (p = 0.012) and posterior column osteotomies (p = 0.014) than adolescent patients. Distal adding-on (>10°) was observed in one (4.7%) juvenile and three (3.6%) adolescent patients (p = 0.80), without the need for revisions. Scoliosis Research Society 24 total score averaged 101 in juvenile and 97 in adolescent group at 2-year follow-up (p = 0.047).
Conclusion:
Posterior spinal fusion with bilateral segmental pedicle screw instrumentation to the stable vertebra provides similar clinical and radiographic outcomes in juvenile patients as compared with adolescents with fusion to the touched vertebra in idiopathic scoliosis. Health-related quality of life as measured using the Scoliosis Research Society 24 questionnaire at the end of follow-up was better in the juvenile as compared with the adolescent group.
Keywords
Introduction
Juvenile idiopathic scoliosis (JIS) is defined as a form of idiopathic scoliosis diagnosed between the ages of 3 and 9 years 11 months (1, 2). Untreated JIS is associated with increased mortality due to cardiopulmonary compromise while untreated adolescent idiopathic scoliosis (AIS) is not (3). Early spinal fusion may result in short trunk and restrictive lung disease, and therefore, growth-friendly instrumentation has been recommended in the skeletally immature patients with JIS (2, 4). However, it has been reported treating progressive JIS between the age of 9 and 11 years using a definitive spinal fusion with better curve correction, less surgeries, and minimal loss of spinal height as compared with traditional growing rods (5).
Progression of the spinal deformity due to continued growth of the unfused anterior part of the spine—known as distal adding-on—may complicate definitive spinal fusion at an early age (6–8). To prevent distal adding-on a combined anteroposterior approach has been recommended in patients with significant growth left (6–9). Despite the differences between JIS and AIS, studies reporting the outcomes of definitive spinal fusion using bilateral, segmental pedicle screw instrumentation (PSI) on radiographic parameters (9, 10) and health-related quality life (HRQoL) (10) are few in the juvenile subgroup. The effect of direct vertebral column derotation (DVR) on rib hump and distal adding-on in this patient cohort is neither known (9, 10).
Bilateral PSI, which traverses all three spinal columns, may lower the risk of distal adding-on as compared with hybrid instrumentation (9, 11). Recently, Sponseller et al. (9) reported distal adding-on more than 10° in seven out of 20 children with open triradiate cartilage even when using pedicle screws. However, majority of their patients with distal adding-on were fused one level short of stable vertebra and bilateral, segmental PSI was not used in all patients. Thus, it remains unclear whether bilateral segmental PSI up to stable vertebra can provide long-term stable fusion also in patients with JIS compared with fusion to touched vertebra in AIS.
The purpose of this study was to compare outcomes between posterior spinal fusion of JIS to stable vertebra and of AIS to touched vertebra with a minimum of 2-year follow-up (FU). We hypothesized that extending the spinal fusion to the stable vertebra in juvenile patients would provide similar outcomes compared with fusion to the touched vertebra in adolescents.
Materials and Methods
Study Design
The study was a prospective comparative cohort study on the clinical, radiographic, and HRQoL using the Scoliosis Research Society 24 outcome questionnaire (SRS-24) (12, 13) in patients with JIS (Risser 0) and AIS (Risser ⩾ 2) in a single center. Patients with major thoracolumbar or lumbar curve (Lenke 5) were excluded. The patients were enrolled between 2009 and 2015. Twenty-one children fulfilled the inclusion criteria (diagnosis of JIS, Risser 0, 15 patients with open triradiate cartilage, without associated spinal cord anomalies or syndromes). Eighty-four AIS patients (diagnosis of AIS, Risser ⩾2, aged 13–18 years) were enrolled consecutively under the same time period to create a comparison group with a 1:4 ratio.
The study subjects were followed using standardized protocol including preoperative and immediate postoperative assessment, and two visits at the outpatient clinic at 6 months and at 2 years after surgery (Table 1). We have chosen to perform definitive spinal fusion for the juvenile patients when the estimated length of thoracic spine will reach at least 22 cm after spinal deformity correction. A major curve Cobb angle of ⩾45° was the indication for operative treatment in both groups (14, 15), and DVR was used in all patients to provide spinal derotation (14). All the operations were performed at our University Hospital by the same two experienced orthopedic spine surgeons.
Clinical characteristics of the study groups.
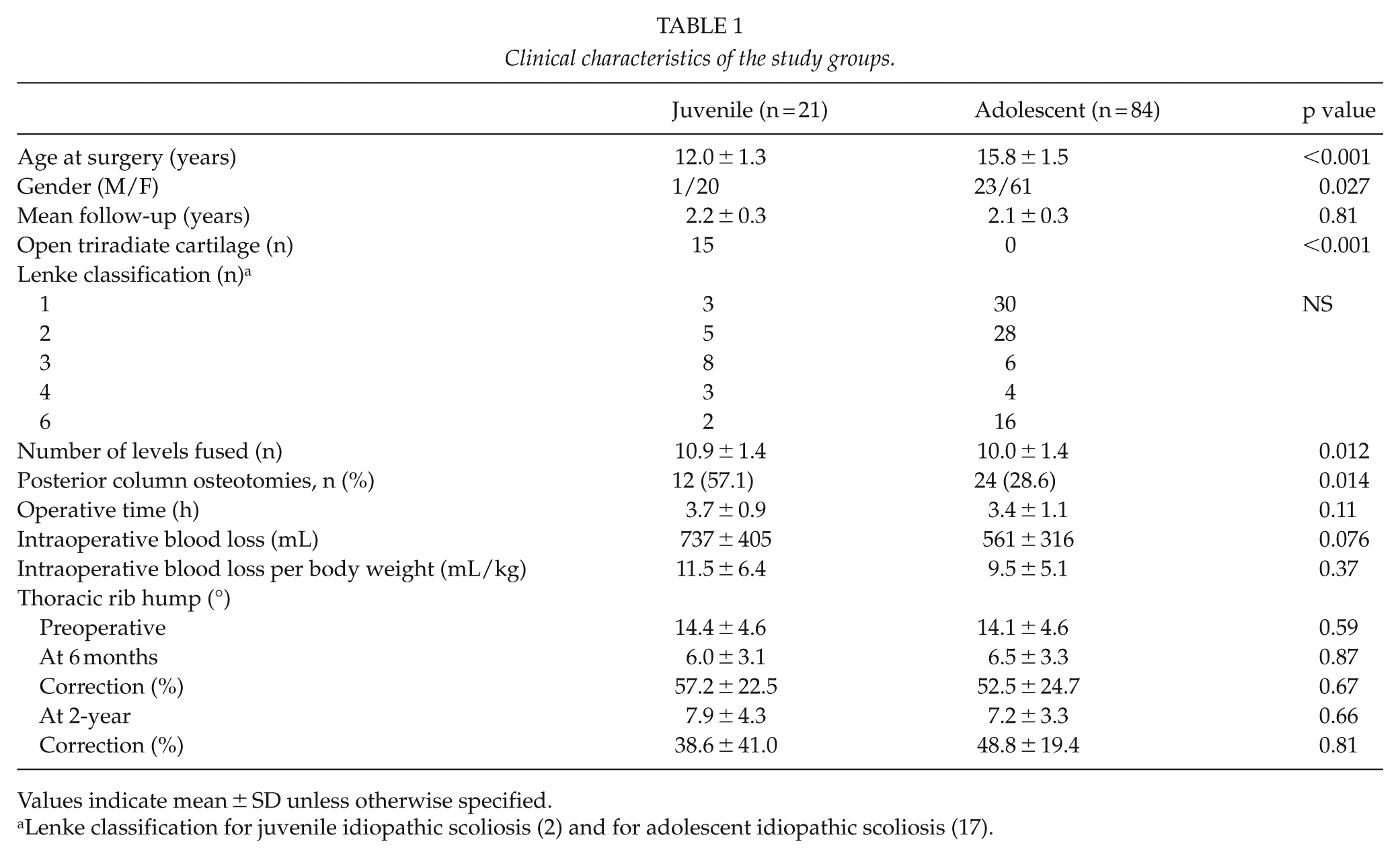
Values indicate mean ± SD unless otherwise specified.
SRS-24 Outcome Questionnaire
All patients filled out the SRS-24 questionnaire (12, 13) preoperatively, at 6 months, and at 2-year FU. The SRS-24 is a disease-specific HRQoL questionnaire used to assess the current state of the patient with scoliosis, and the effects of surgery, consisting of 24 questions, each with a grading of 1–5 points, with a maximum score of 120. The questionnaire evaluates seven domains: pain, general self-image, function from back condition, activity level, postoperative self-image, postoperative function, and satisfaction (12, 13).
Surgical Technique
All patients were operated using posterior only approach. Bilateral segmental PSI with en bloc DVR (6.35 CD Legacy or Solera 6.0, Medtronics Spinal and Biologics, Memphis, TN, USA) was used to correct spinal deformity. Pedicle screws were inserted with free-hand technique. Ponte osteotomies were performed to facilitate correction of the sagittal imbalance. All structural curves according to the Lenke classification for JIS (curves crossing midline) were instrumented (2), and the fusion was extended to the stable vertebra in all JIS patients (i.e. central sacral vertical line (CSVL) between the pedicles of lowest instrumented vertebra). For the AIS patients, structural curves were instrumented, and the lowest instrumented vertebra was selected for the A and B type curves as the lowest vertebra touched and for the C type curves as the lowest vertebra bisected by the CSVL. Intraoperative neurophysiological monitoring was done with motor-evoked potentials (MEPs), somatosensory-evoked potential (SSEP), and electromyography (EMG) in all patients.
Radiographic Measurements
Standard standing posteroanterior and lateral radiographs were taken of the spine preoperatively, at 6-month and at 2-year FU and bending radiographs preoperatively. Data collected from radiographs included the proximal thoracic, main thoracic, and thoracolumbar/lumbar curves, coronal and sagittal balance, thoracic kyphosis (T5-T12), lumbar lordosis (T12-S1), and segmental kyphosis (T2-T5; T10-L2) or lordosis measured by Cobb technique (16). Lenke classification was used for both groups (2, 17). Distal adding-on was defined as an increase in the coronal Cobb angle of ⩾10° during FU (7, 9). Proximal junctional kyphosis was defined as proximal junction sagittal Cobb angle of 10° or more and at least 10° more than the preoperative measurement (18). Independent observer measured all radiographs.
Statistical Methods
Values are given as mean (SD). Since the distribution of all continuous variables did not follow normal distribution, non-parametric testing using the Mann–Whitney U test (19) was applied for between group and Wilcoxon signed rank sum test (20) for within group comparisons. The statistical significances of the unadjusted differences between frequency distributions were tested with Pearson’s chi-square test (21). p values of 0.05 or less were considered as significant.
Results
Clinical Characteristics
Clinical and radiographic FU rate was 100% at 2 years. Patients with JIS were operated at an earlier age (p < 0.001), and the juvenile cohort had significantly more girls than boys than AIS cohort (p = 0.027). JIS patients had also more fused levels (p = 0.012) and posterior column osteotomies (p = 0.014) than AIS patients, but operative time and intraoperative blood loss were similar in both groups (Table 1). The mean number of posterior column osteotomies performed was 1.9 (range of 1–5) in the juvenile and 2.6 (1–7) in the adolescent group.
Thoracic rib hump averaged 14° in both groups. It was corrected to 6° at 6 months in both groups, and to 8° in the juvenile group (p = 0.016) and 7° in adolescent group at 2-year FU (p < 0.001, preoperative vs 2-year FU) (Table 1).
Radiographic Outcomes
Fifteen (71%) of the juvenile patients had an open triradiate cartilage preoperatively (Fig. 1A to D). Patients with JIS had a significantly larger main curve than the adolescent group (58° vs 53°, p = 0.0032) (Table 2). The main curves were corrected to a mean of 13° in the juvenile and 12° in the adolescent group at 2-year FU. This represented 78% correction of the main coronal curve in the juvenile and 77% in the adolescent group, respectively (p = 0.90). Thoracic kyphosis averaged preoperatively 21° in both groups and were 17° in the JIS and 19° in the AIS at 2-year FU (p = 0.54). Distal adding on (>10°) was observed in one (4.8%) juvenile and three (3.6%) adolescent patients (p = 0.80). None of the patients needed re-operation for distal adding-on, and there were no signs of non-union at final FU. None of the patients in the juvenile and two (2.3%) in the adolescent group showed a proximal junctional kyphosis at final FU (p = 0.48).
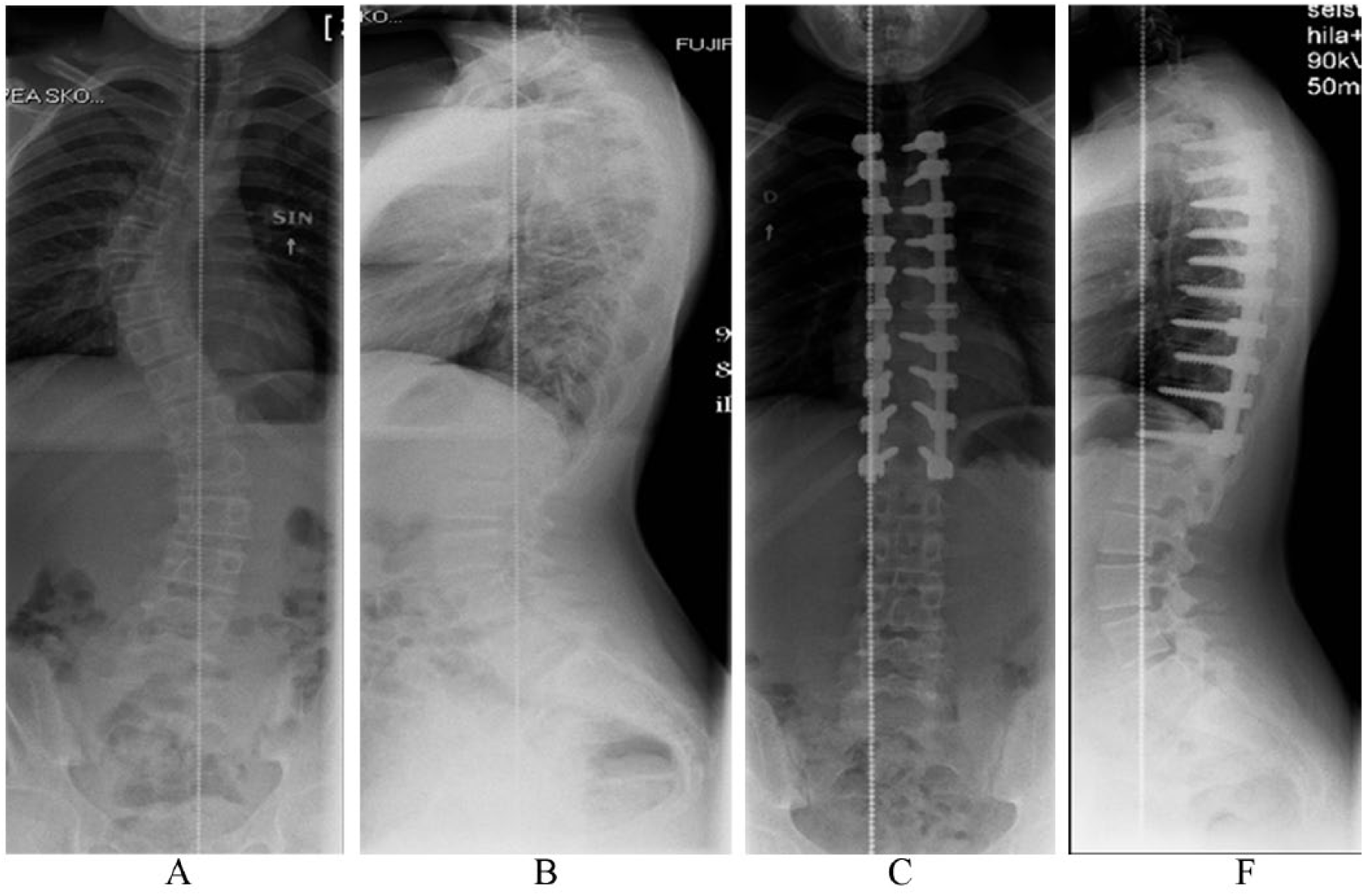
12-year-old girl with juvenile idiopathic scoliosis (Risser 0, open triradiate cartilage). Preoperative standing radiographs (A, B) demonstrate 52° thoracic scoliosis with normal kyphosis. Standing radiograph at 2-year FU (C, D) demonstrate bilateral segmental pedicle screw instrumentation without distal adding-on, proximal junctional kyphosis or flattening of the thoracic kyphosis.
Radiographic outcomes.
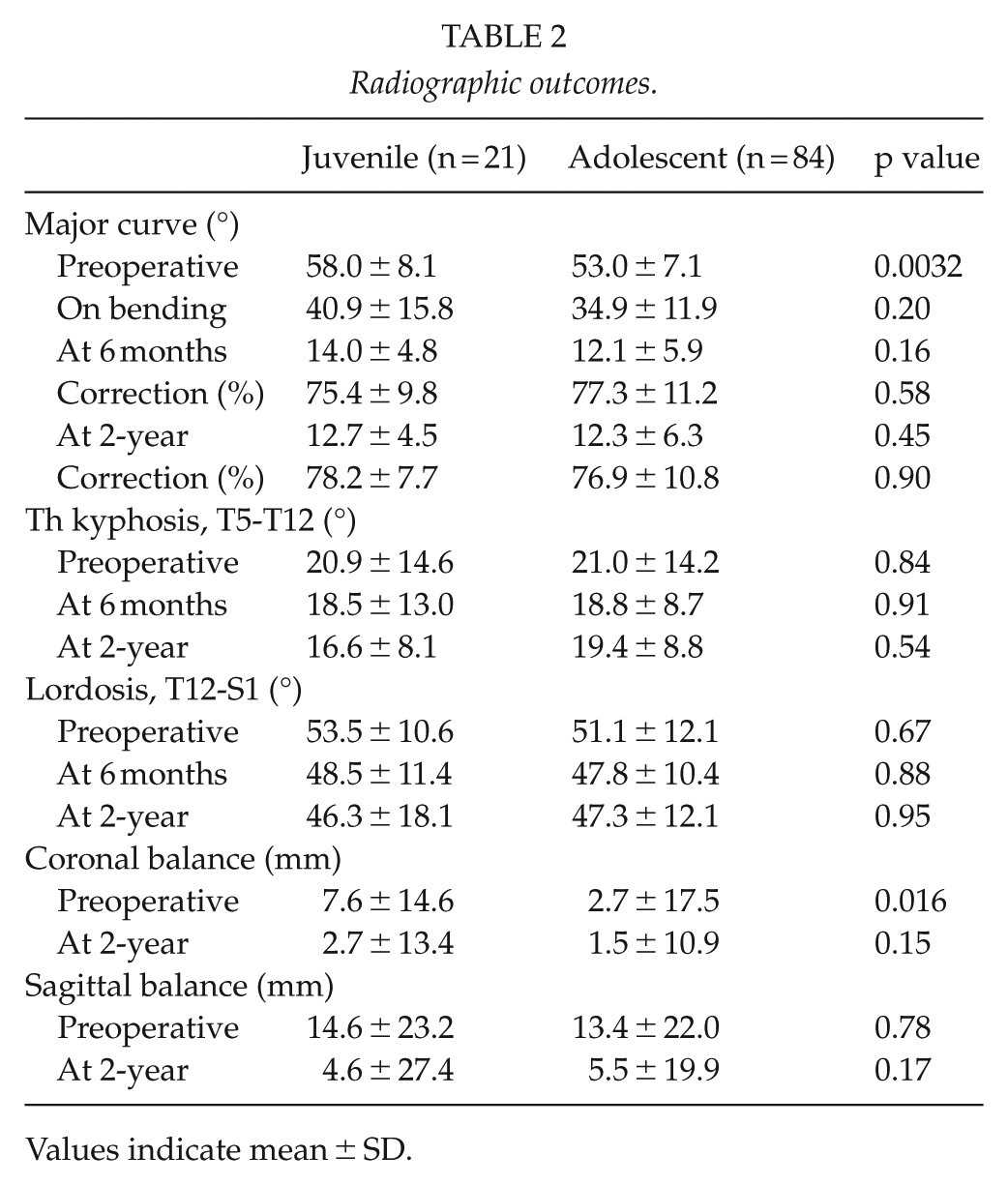
Values indicate mean ± SD.
Complications
There were two (9.5%) complications in the juvenile and four (4.8%) in the adolescent group (p = 0.80). To address these, a re-operation was required in one (4.8%) juvenile and in two (2.4%) adolescent patients (p = 0.56). Complications recorded in the juvenile group included one intraoperative dural lesion requiring suturing and one deep wound infection treated with irrigation and debridement while all complications in the adolescent group were screw related. These included one asymptomatic rod detachment from pedicle screw, while two adolescent patients suffered from transient right-sided motor deficits. The first due to malpositioned T9 screw inside the spinal canal requiring screw removal at a separate session and the other due to a spinal cord contusion caused by a pedicle probe entering spinal canal via fractured pedicle channel (treated with staged surgery). The first patient recovered immediately while the latter recovered fully from motor deficit within 6 weeks and sensory deficit within the 2-year FU. One patient was diagnosed of L4 root injury due to fractured pedicle. He had a sensory deficit but no motor deficit at 2-year FU.
The SRS-24 Outcome Questionnaire
SRS-24 questionnaire was available preoperatively in 95 patients (17 JIS and 78 AIS), in 98 patients (18 JIS and 80 AIS) at 6 months, and in 97 patients (18 JIS and 79 AIS) at the 2-year FU. Patients with JIS showed significantly better SRS-24 score for back pain (p = 0.040), function from back condition (p = 0.040), and satisfaction (p = 0.049) at 2-year FU as compared with the adolescent group (Table 3). The total score of SRS-24 at 2-year FU averaged 101 (4.2) points in the juvenile and 97 (4.0) in the adolescent group (p = 0.040). Both groups showed a statistically significant improvement in the back pain score from preoperative to 6 months (p < 0.001 in both groups) and from preoperative to 2-year FU (p = 0.0039 for JIS and p < 0.001 for AIS).
Outcomes of the Scoliosis Research Society (SRS) 24 questionnaire.
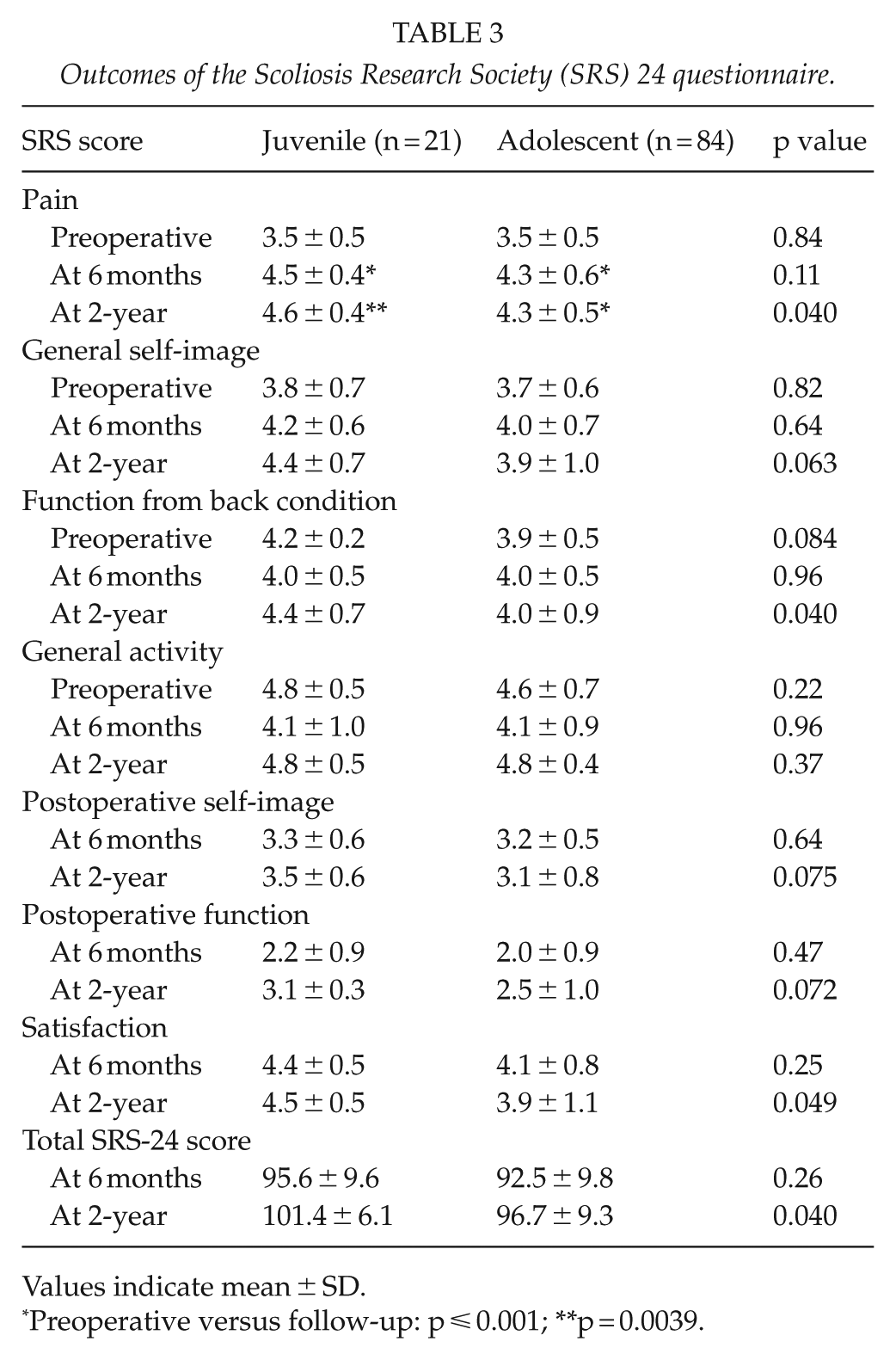
Values indicate mean ± SD.
Preoperative versus follow-up: p ⩽ 0.001; **p = 0.0039.
Discussion
The strengths of the study include the prospective data collection and standard surgical technique using bilateral segmental PSI with DVR to stabilize vertebra in patients with JIS. The same two orthopedic spine surgeons performed all the operations, and the postoperative FU was standardized. The study population included all consecutive juvenile patients operated for idiopathic scoliosis between 2009 and 2015 in a single center providing complete clinical and radiographic data collection. Consecutive AIS patients (⩾Risser 2) operated using similar surgical technique, but fused to the touched vertebra formed a control group. Due to the prospective data collection, we chose not to change the SRS-24 to a more modern version in order to increase the validity of our preoperative versus postoperative as well as between group comparisons. The SRS-24 total score has been reported to fulfill the properties of internal construct validity (22).
The limitations include the relatively small number of juvenile patients mainly due to the selection of growth friendly instrumentation in patients with an immature spine (Risser 0) instead of definitive spinal fusion. Due to the relatively small number of patients included in the JIS group comparisons across the two groups were not performed according to individual type of deformity (Lenke types). Lenke 5 group patients (main thoracolumbar curve) were not included in the present study, as this group of patients is treated using anterior spinal instrumentation at our unit. It is possible that distal adding-on was similar between the JIS and AIS groups, because the JIS patients were fused longer to the stable vertebra, which reduces such risk and not necessarily because the used DVR technique. The standard 2-year postoperative FU is considered adequate for the AIS patients who had mostly reached skeletal maturity by that stage. But this is not necessarily true for the JIS patients who at 2 years after surgery can still continue to grow. This remaining spinal growth can affect the results of surgery in regards to adding-on, proximal junctional kyphosis or recurrence of rib hump.
Comparison with Previous Data
Pawelek et al. (5) reported that JIS patients between 9 and 11 years of age benefit from definitive spinal fusion instead of traditional growing rods in terms of better correction of spinal deformity and less surgeries than patients undergoing growth-friendly instrumentation. Our decision to perform definitive spinal fusion for the juvenile patients when the estimated length of thoracic spine reaches at least 22 cm after spinal deformity correction is mainly based on findings of pulmonary function testing after thoracic spine fusion for early onset scoliosis (4).
In the study by Sponseller et al. (9), a relatively large proportion of JIS patients had distal adding-on after PSI (35%, 7/20), while patients undergoing a combined approach had a low risk (0%, 0/9). In their series fusing short of stable vertebra and posterior only approach were risk factors for distal adding-on. In our series, one of the juvenile patients showed distal adding-on, but without the need for revision surgery. All our juvenile patients were systematically fused to the stable vertebra. We hypothesize that by bringing the rotated thoracic and/or lumbar spine fully to the midline aiming at maximum correction in all three planes using DVR may actually decrease the risk of distal adding-on in immature patients with JIS. This hypothesis is in line with the historical recommendation of an anterior arthrodesis for immature scoliosis patients who have more than 2 years growth left, residual deformity of more than 30°, and rotation of more than 20° postoperatively (6). Thoracic kyphosis was reduced in both groups postoperatively, but no further progression of thoracic flattening occurred during FU suggesting that a three column fixation using maximum length thoracic pedicle screws can control the continued anterior growth of the spine in an effective manner.
Prospective studies evaluating the effects of spinal fusion on HRQoL are few in patients with JIS. Sponseller et al. (9) showed a similar improvement of SRS-22 scores in patients undergoing spinal fusion for JIS and AIS. In this study, though patients with JIS reported significantly better SRS-24 scores for back pain, function from back condition, satisfaction, and total score at 2-year FU as compared with the adolescent group, no correlation was found between the SRS-24 scores and the radiographic correction of scoliosis. Major curve correction averaged over 75% for both study groups being a relatively high level as compared with a previous systematic literature review (23).
Conclusion
This study shows significant improvement in clinical, radiographic, and HRQoL outcomes in both the JIS group with fusion to the stable vertebra and AIS group with fusion to the touched vertebra. Both groups showed over 75% stable radiographic coronal curve correction during 2-year FU. The correction of thoracic rib hump decreased from over 50% at 6 months to 39% at 2 years in the JIS group, but the risk of radiographic distal adding-on was low and none of the patients required revision for distal adding-on during the FU. HRQoL as measured using the SRS-24 questionnaire was significantly better for the juvenile than in the AIS group at 2-year FU.
Footnotes
Declaration of Conflicting Interests
I.H. is a consultant for Medtronic International, and received grants and research funding from Medtronic International and Baxter International. O.P. received grants and research funding from Medtronic International and Baxter International.
Ethical Approval
The ethics committee of our university hospital granted approval for the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by grants from University Hospital, Foundations, and Industry. The funding body did not play a role in the investigation. The funds were used only for financing research leaves and employment of a research nurse. This study was funded by the Medtronic International, Foundation for Pediatric Research, and Finska Läkaresällskapet.
Informed Consent
No additional patient contact was needed for this study, and therefore, written informed consent was not requested by the ethics committee.