
Abstract
Background and Aims:
Cardiac injuries are highly lethal lesions following trauma and most of the patients decease in pre-hospital settings. However, studies on cardiac trauma in Estonia are scarce. Thus, we set out to study cardiac injuries admitted to Estonian major trauma facilities during 23 years of Estonian independence.
Materials and Methods:
After the ethics review board approval, all consecutive patients with cardiac injuries per ICD-9 (861.0 and 861.1) and ICD-10 codes (S.26) admitted to the major trauma facilities between 1 January 1993 and 31 July 2016 were retrospectively reviewed. Cardiac contusions were excluded. Data collected included demographics, injury profile, and in-hospital outcomes. Primary outcome was mortality. Secondary outcomes were cardiac injury profile and hospital length of stay.
Results:
During the study period, 37 patients were included. Mean age was 33.1 ± 12.0 years and 92% were male. Penetrating and blunt trauma accounted for 89% and 11% of the cases, respectively. Thoracotomy and sternotomy rates for cardiac repair were 80% and 20%, respectively. Most frequently injured cardiac chamber was left ventricle at 49% followed by right ventricle, right atrium, and left atrium at 34%, 17%, and 3% of the patients, respectively. Multi-chamber injury was observed at 5% of the cases. Overall hospital length of stay was 13.5 ± 16.7 days. Overall mortality was 22% (n = 8) with uniformly fatal outcomes following left atrial and multi-chamber injuries.
Conclusion:
Overall, 37 patients with cardiac injuries were hospitalized to national major trauma facilities during the 23-year study period. The overall in-hospital mortality was 22% comparing favorably with previous reports. Risk factors for mortality were initial Glasgow Coma Scale < 9, pre-hospital cardiopulmonary resuscitation, and alcohol intoxication.
Background and Aims
Cardiac injuries (CI) are highly lethal lesions and most of these victims decease at the scene with only 6% of the patients reaching hospital alive (1). Recently published population-based autopsy study from Estonia noted that 11% of all trauma deaths were secondary to CI (2). Different trauma centers report their in-hospital mortality between 22% and 67% after CI in recent years (1, 3–12). However, there are no previous studies available on CI in Estonia despite the fact that injury-related deaths are significantly higher compared to European Union average (13–15). Thus, we set out to study CI admitted to Estonian major trauma facilities during 23 years of Estonian independence. We hypothesized that the outcomes of CI in Estonian major trauma facilities are comparable to previous reports.
Materials and Methods
Following the ethics review board approval, all patients admitted to the North Estonia Medical Centre and Tartu University Hospital with CI between
Data collected included demographics, American Association for the Surgery of Trauma Organ Injury Scale (AAST-OIS), Abbreviated Injury Scale (AIS) score, Injury Severity Score (ISS), Trauma and Injury Severity Score (TRISS), surgical interventions, CI profile, complications per Clavien-Dindo, hospital length of stay (HLOS), and in-hospital mortality (16–19).
Primary outcome was mortality. Secondary outcomes were CI profile and HLOS. Mortality and complications were compared between early (1993–2004) and late period (2005–2016) of the study.
Potential risk factors for mortality were analyzed including gender, age, initial systolic blood pressure (SBP) < 90 mmHg, Glasgow Coma Scale (GCS) < 9, pre-hospital cardiopulmonary resuscitation (CPR), emergency department thoracotomy (EDT), multi-chamber injury, cardiac tamponade, severe non-CI (with AIS ⩾ 3), and positive blood alcohol level similarly to other studies (1, 3, 8, 9).
During the study period, patients with suspected or confirmed CI were transferred to operating room for sternotomy or thoracotomy. Resuscitative Emergency Department Thoracotomy (EDT) was utilized in patients with imminent cardiac arrest or a witnessed cardiac arrest en route to hospital.
Statistical analysis was performed with R Studio 1.0.136 environment (Vienna, Austria). Continuous data are reported as mean ± standard deviation (SD) and categorical variables as percentage. To determine association between two variables, Fisher’s exact test was utilized for categorical and Wilcoxon–Mann–Whitney for continuous variables. A binary logistic regression analysis was deployed to determine independent risk factors for mortality. A p value < 0.05 was considered statistically significant.
Results
During the 23-year study period, a total of 37 patients were admitted to the major national trauma facilities in Estonia. Demographic and clinical injury characteristics are shown in Table 1. Most of the patients were young male. Mean ISS was 26.8 ± 14.8 and 62.1% of victims were critically injured (ISS > 25). Overall, almost every second patient had a positive blood alcohol level with an average of 2.45 g/L.
Demographic and clinical injury characteristics of all patients.
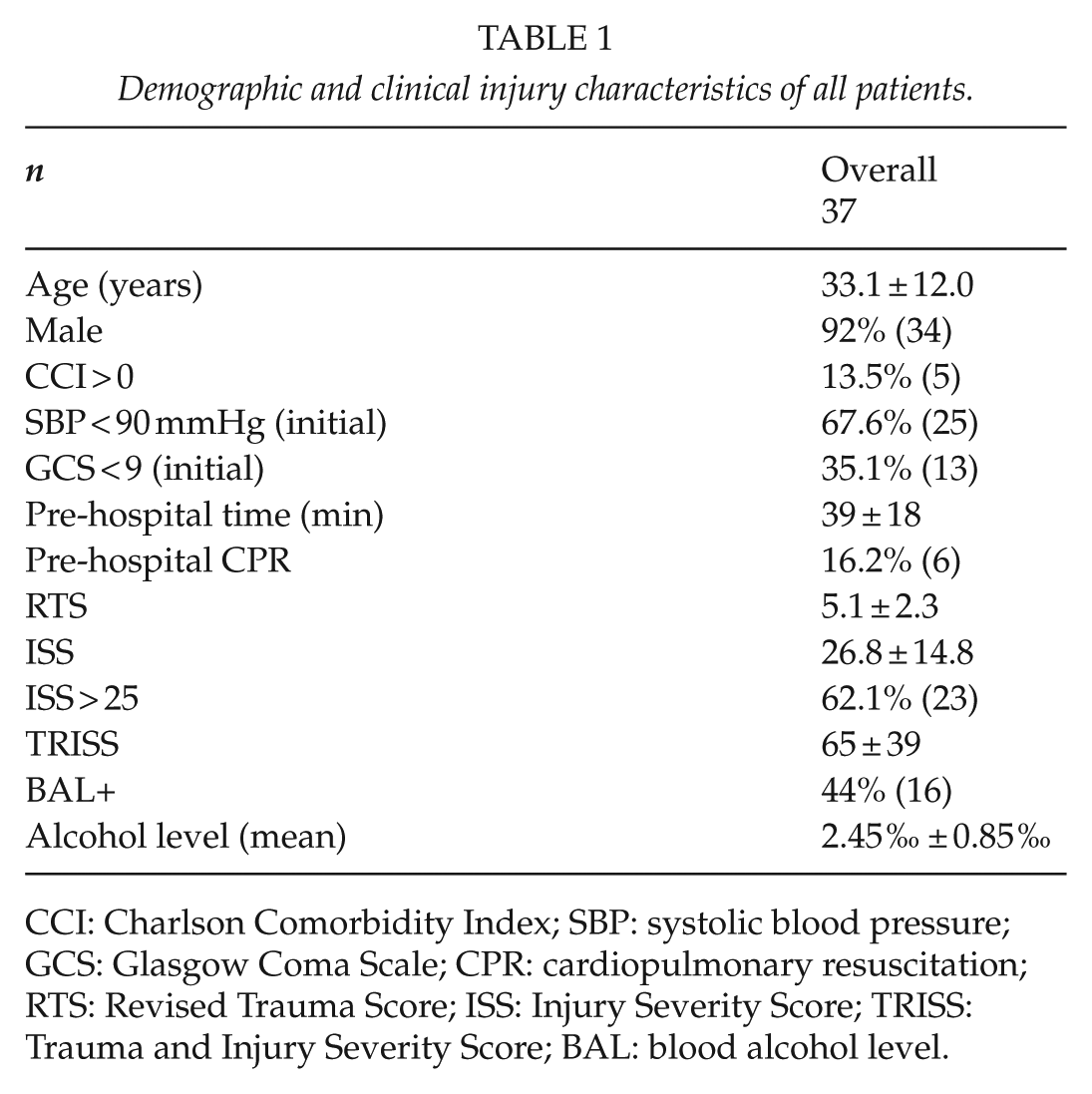
CCI: Charlson Comorbidity Index; SBP: systolic blood pressure; GCS: Glasgow Coma Scale; CPR: cardiopulmonary resuscitation; RTS: Revised Trauma Score; ISS: Injury Severity Score; TRISS: Trauma and Injury Severity Score; BAL: blood alcohol level.
Penetrating trauma accounted for 89% of the cases with stab wounds and gunshot wounds constituting 97% and 3%, respectively; 11% of cases were secondary to blunt trauma by a falling object and non-ground level falls constituting 50% of the cases. Homicides, suicides, and accidents accounted for 63%, 23%, and 14%, respectively. Focused assessment with sonography in trauma (FAST) scan was utilized in 54% (n = 20) of the cases resulting in a sensitivity and positive predictive value of 80% and 100% for pericardial effusion, respectively.
All the patients required surgery. Thoracotomy and sternotomy was performed in 80% and 20% of cases, respectively. EDT rate was 8% with 67% survival rate.
In total, 32% (n = 12) of patients with penetrating chest injury were stable on arrival to emergency department (ED). The decision for surgery in these patients was based on clinical findings, positive FAST, or a positive computed tomography (CT) finding for CI in one, four, and six cases, respectively. One patient was admitted from ED to intensive care unit (ICU) for observation; however, the patient became hemodynamically compromised in the ICU and was transferred to the operating room (OR) for surgery.
Most frequently injured cardiac chamber was left ventricle at 49% followed by right ventricle, right atrium, and left atrium at 34%, 17%, and 3% of the patients, respectively (Fig. 1). Multi-chamber injury was observed at 5% of the cases. Cardiac tamponade was diagnosed at 62% (n = 21) of the cases.
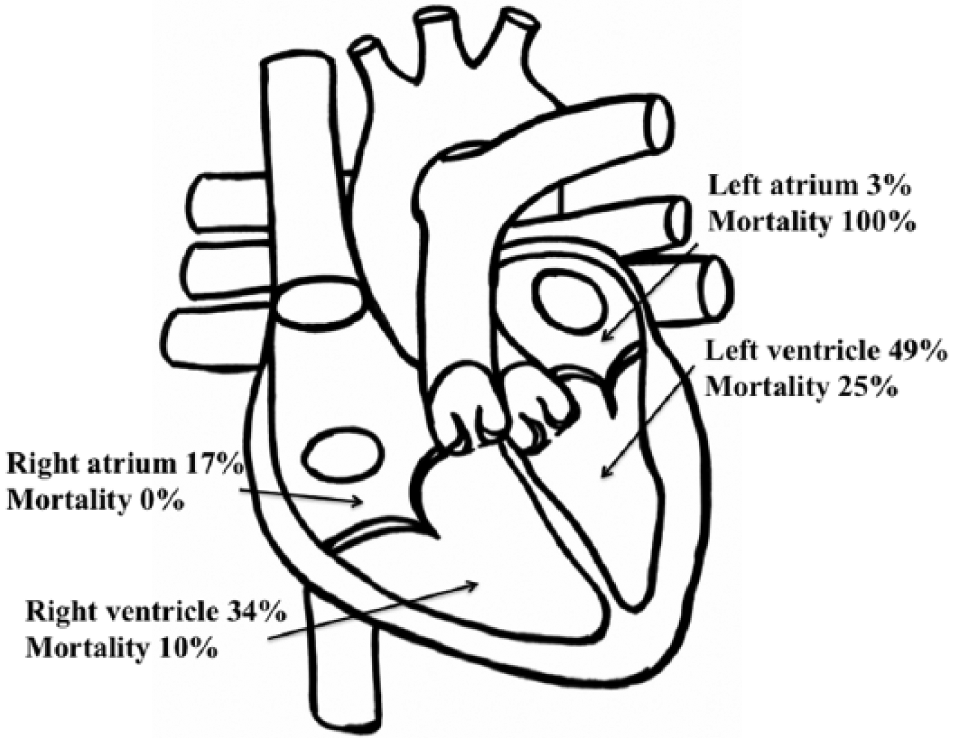
Distribution of cardiac injuries and mortality per the respective injured chamber.
AAST-OIS injury grade observed and the respective mortality was in grade I injuries (1 of 37) at 0%; in grade II injuries (5 of 37) at 0%; in grade III injuries (3 of 37) at 0%; in grade IV injuries (22 of 37) at 18% and in grade V injuries (6 of 37) at 67%. A detailed description of complications per Clavien–Dindo classification is presented in Table 2. The overall rate of complications was 37.8% with grade II and III complications predominated. Overall rate of complications did not differ between early and late period of the study (p = 0.87).
Overall rate of complications and complications per Clavien-Dindo classification.
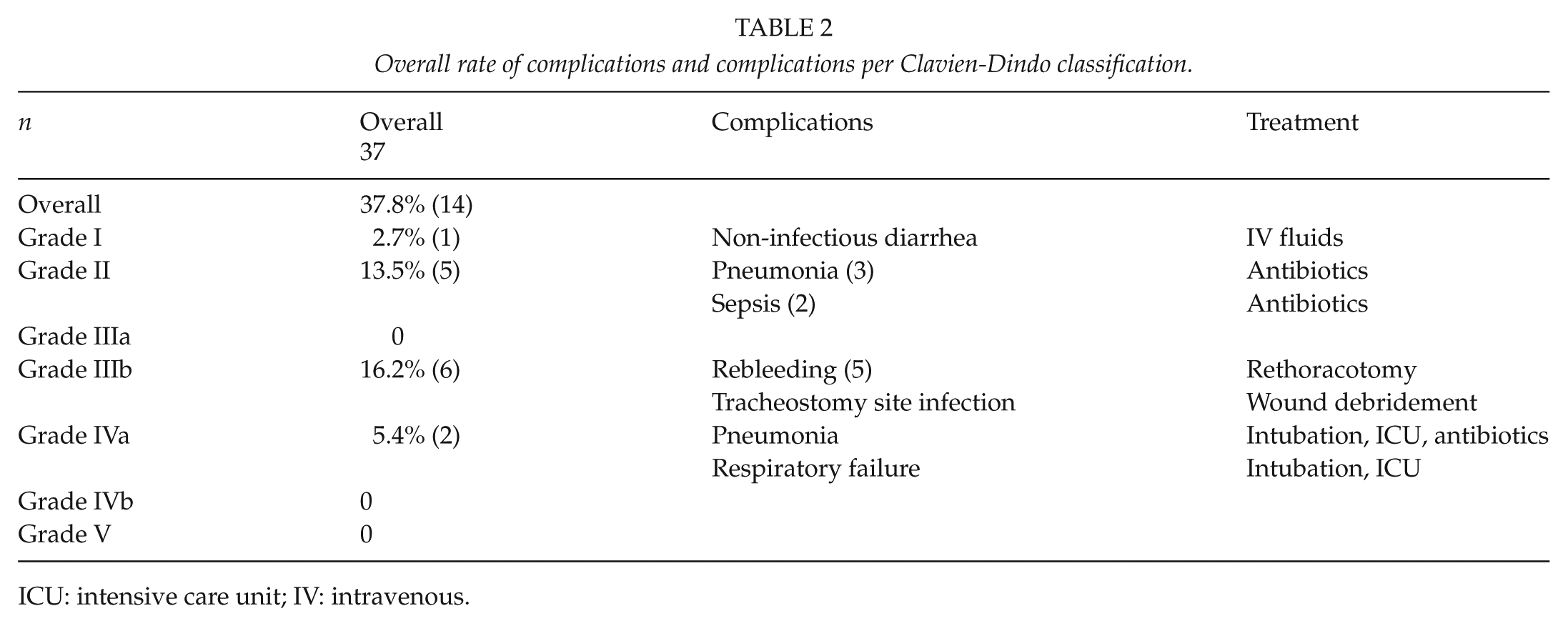
ICU: intensive care unit; IV: intravenous.
The average HLOS and intensive care unit length of stay (ICU-LOS) were 13.5 ± 16.7 and 6.4 ± 7.2 days, respectively. Overall in-hospital mortality was 22% with uniformly fatal outcomes following multi-chamber and left atrial injuries. All patients with right atrial injury survived. The most common cause of death was fatal hemorrhage secondary to CI at 75% followed by cardiogenic shock as a result of tamponade in one case and myocardial infarction in one case. All deaths were associated with CI. Mortality after penetrating and blunt CI was 21% and 25%, respectively. Mortality was similar between early and late period of the study (31% vs 17%, OR = 0.48, 95% CI: 0.07–3.24, p = 0.422).
Risk factors for mortality are shown in Table 3. Statistically significant predictors for mortality were pre-hospital CPR (p = 0.003), initial GCS < 9 (p = 0.001), and multi-chamber injury (p = 0.030). After logistic regression analysis, the significant predictors for mortality were pre-hospital CPR (p = 0.010), initial GCS < 9 (p = 0.002), and alcohol intoxication (p = 0.013).
Risk factors for mortality.
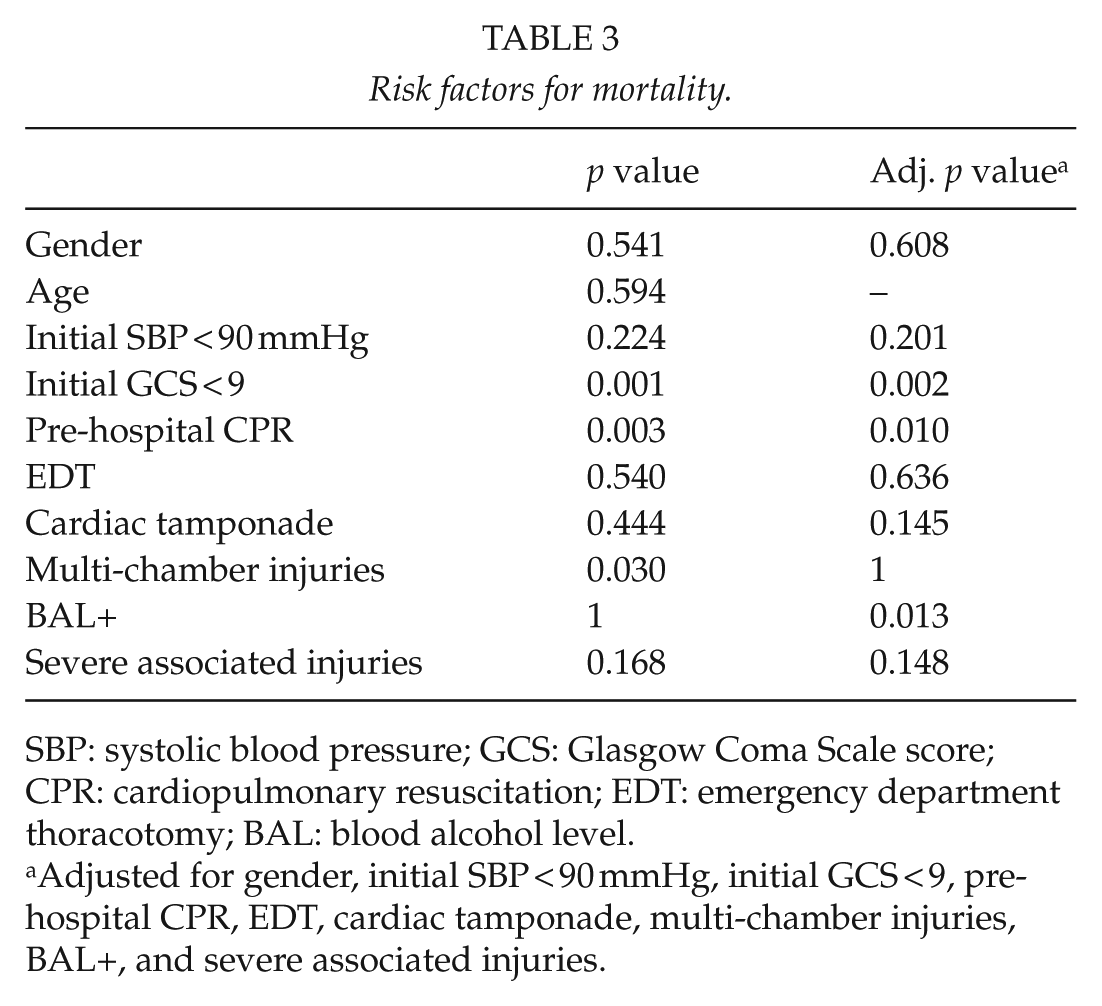
SBP: systolic blood pressure; GCS: Glasgow Coma Scale score; CPR: cardiopulmonary resuscitation; EDT: emergency department thoracotomy; BAL: blood alcohol level.
Adjusted for gender, initial SBP < 90 mmHg, initial GCS < 9, pre-hospital CPR, EDT, cardiac tamponade, multi-chamber injuries, BAL+, and severe associated injuries.
Discussion
During the 23-year period of Estonian independence, 37 patients with CI were hospitalized to the major national trauma facilities. The current study serves a population-based perspective as all major Estonian trauma facilities were involved and the vast majority of severe injuries are primarily or in a delayed fashion transferred to the involved trauma facilities. The Estonian pre-hospital emergency medical system has an access to almost an entire population within 30 min provided there are no competing priorities (20, 21).
Similar to other European countries, Estonia encounters a very low rate of penetrating trauma reflected in a small number of cases. The major trauma courses including Advanced Trauma Life Support®, Definitive Surgical Trauma Care™ and Advanced Surgical Skills for Exposure in Trauma™ have been recently introduced to Estonia to improve outcomes of the Estonian trauma system in patients suffering penetrating and blunt injuries (22–24). Most of the patients were young male similarly to other investigations (1, 3–12).
Our study showed in-hospital mortality of 22%, which is comparable to other investigations reporting mortality ranging from 22% to 67% (1, 3–12). However, many studies reporting higher mortality encounter significant number of CI secondary to gunshot wounds (GSW), which is a well-known risk factor for mortality (1, 3, 4, 8, 9). In our study, 89% of victims suffered penetrating trauma with only one GSW being typical for European region encountering very low rate of GSWs. A total of 11% of patients admitted to hospital had blunt cardiac laceration with survival rate of 75%. Most of the trauma victims with blunt cardiac laceration succumb at the scene and never reach hospital alive (25). Most frequently injured chamber of patients reaching hospital after blunt trauma was right atrium. Similarly, study by Brathwaite et al. (26) reported right atrial rupture as the most frequently injured chamber after blunt trauma in hospitalized patients. However, right ventricle has been observed as the predominantly injured chamber in patients succumbing at the scene (2).
Predictors for mortality were similar to many other studies (1, 3, 9). Regression analysis demonstrated that independent risk factors for mortality were pre-hospital CPR, initial GCS < 9, and alcohol intoxication. Multi-chamber injuries were uniformly fatal; however, as only two cases of multi-chamber injuries were observed, an adequate statistical analysis was not feasible.
In a study by Mina et al. (8), cardiac tamponade was found to be protective. In our study, however, cardiac tamponade did not show statistically significant protective effect. The number of repeat thoracotomies due to re-bleeding from cardiac wounds was high and may be explained by the low volume of the cases and limited experience in cardiac injuries.
A study by Nicol et al. (27) comparing subxiphoid window and pericardial drainage with sternotomy in stable patients with hemopericardium following penetrating thoracic trauma observed that subxiphoid window is an effective and safe method with no increase in mortality and with shorter ICU and overall hospital stay. In our study population, this method was not utilized. The subxiphoid window could be integrated into management algorithms in high volume sites; nevertheless, in low volume sites similar to ours, the gold standard of surgical exploration and repair of a suspected cardiac wound is the preferred strategy.
The low utilization rate of FAST in our study could be explained by the fact that availability of ultrasound was limited during the earlier period of the study. FAST in our study with a sensitivity of 80% with high rate of false negative results is concerning; however, similar results have been noted in some previous reports (28, 29). Also, a relatively high number of patients with CI receiving a CT scan is alarming and serves as a quality improvement initiative for the study sites. HLOS and ICU-LOS are comparable to other studies (6, 8).
Limitations of the current study are retrospective design, extended interval of case collection and a relatively small number of cases, which may have an effect on the accuracy of the statistical analysis. Likewise, some incidental CI not admitted to major trauma facilities were not included in the current study.
In conclusion, the number of CI hospitalized to the major trauma facilities in Estonia during the study period was 37. The overall in-hospital mortality was 22% comparing favorably with previous reports. Risk factors for mortality were initial GCS < 9, pre-hospital CPR, and alcohol intoxication.
Footnotes
Acknowledgements
Ingemar Almre MD, Department of Surgery, Division of Thoracic Surgery, North Estonia Medical Centre, Tallinn, Estonia.
Tanel Laisaar MD, PhD, Department of Pulmonology, Division of Thoracic Surgery, Tartu University Hospital, Tartu, Estonia.
Arno Ruusalepp MD, PhD, Department of Cardiology, Division of Cardiac Surgery, Tartu University Hospital, Tartu, Estonia.
Günter Taal MD, Department of Surgery, Division of Cardiac Surgery, North Estonia Medical Centre, Tallinn, Estonia.
Tõnu Vanakesa MD, Department of Surgery, Division of Thoracic Surgery, North Estonia Medical Centre, Tallinn, Estonia.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The abstract was presented as a poster at the 18th European Congress of Trauma and Emergency Surgery (ECTES), 7–9 May 2017 in Bucharest, Romania.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.